
Early Diagnosis of Atrial Fibrillation and Stroke Incidence in Primary Care: Translating Measurements into Actions—A Retrospective Cohort Study
 , , , , and
, , , , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Study Scope
2.3. Data Collection and Information Sources
- 1.
- The “Health Plan of the “Terres de l’Ebre” region 2021–2025 [23]: a digital access platform used by the Department of Health.
- 2.
- The Institute of Statistics of Catalonia for each region of the territory: demographics, inhabitant density/km2, and aging index vs. Catalonia (100%).
- 3.
- The HCC3 Patient Episode Dataset for Catalonia (CatSalut, Health Department), which includes demographic and clinical data on all daily inpatient and outpatient admissions in Catalonian hospitals.
- 4.
- The 11 EAPs (Catalonian Health Institute, Governmental agency) share a clinical information database for all general practice (E-cap, HC3) and hospital (E-sap) interactions, including clinical data, symptoms, investigations, diagnoses, comorbidities, prescribed medications, referrals to secondary and tertiary care, and status (alive/dead). Pharmacological variables were collected from the SIRE (Catalan acronym for Integrated Electronic Prescription System).
2.4. Study Population
2.5. Inclusion and Exclusion Criteria
2.5.1. Inclusion Criteria
2.5.2. Exclusion Criteria
2.6. Variables
- (1)
- Cardiovascular risk factors and diagnostics using specific International Classification of Diseases (ICD–10) code prefixes for cerebrovascular disease (ischemic stroke or transient ischemic attack, I63, G45), heart failure (I50-51), ischemic heart disease (stable or unstable angina, percutaneous coronary intervention, coronary artery bypass grafting or myocardial infarction) (I20-I25), hypertension (I10–I15), hypercholesterolemia (E78), diabetes mellitus (E10–E14), body mass index (BMI), chronic kidney disease (CKD) (N18) and estimated glomerular filtration rate (eGFR ml/min/1.73 m2).
- (2)
- Clinical scores: AF risk index, CHADsVASc score, Pfeiffer Short Mental Status Questionnaire (SPMSQ) score, NIHSS score, and modified Rankin scale (mRS) in case of stroke as recommended by current guidelines. The model to stratify the risk of suffering AF at five years among individuals aged ≥65 years was published previously [24,25].
- (3)
- Antiplatelet and/oral anticoagulation (antivitaminK vs. NOACs).
- (4)
- Vital status (dead/alive) at the end of the study. All participants were followed from 1 January 2015 to 31 December 2021, loss tofollow-up, or date of death, whichever occurred first.
2.7. Statistical Analysis
3. Results
3.1. Baseline Characteristics
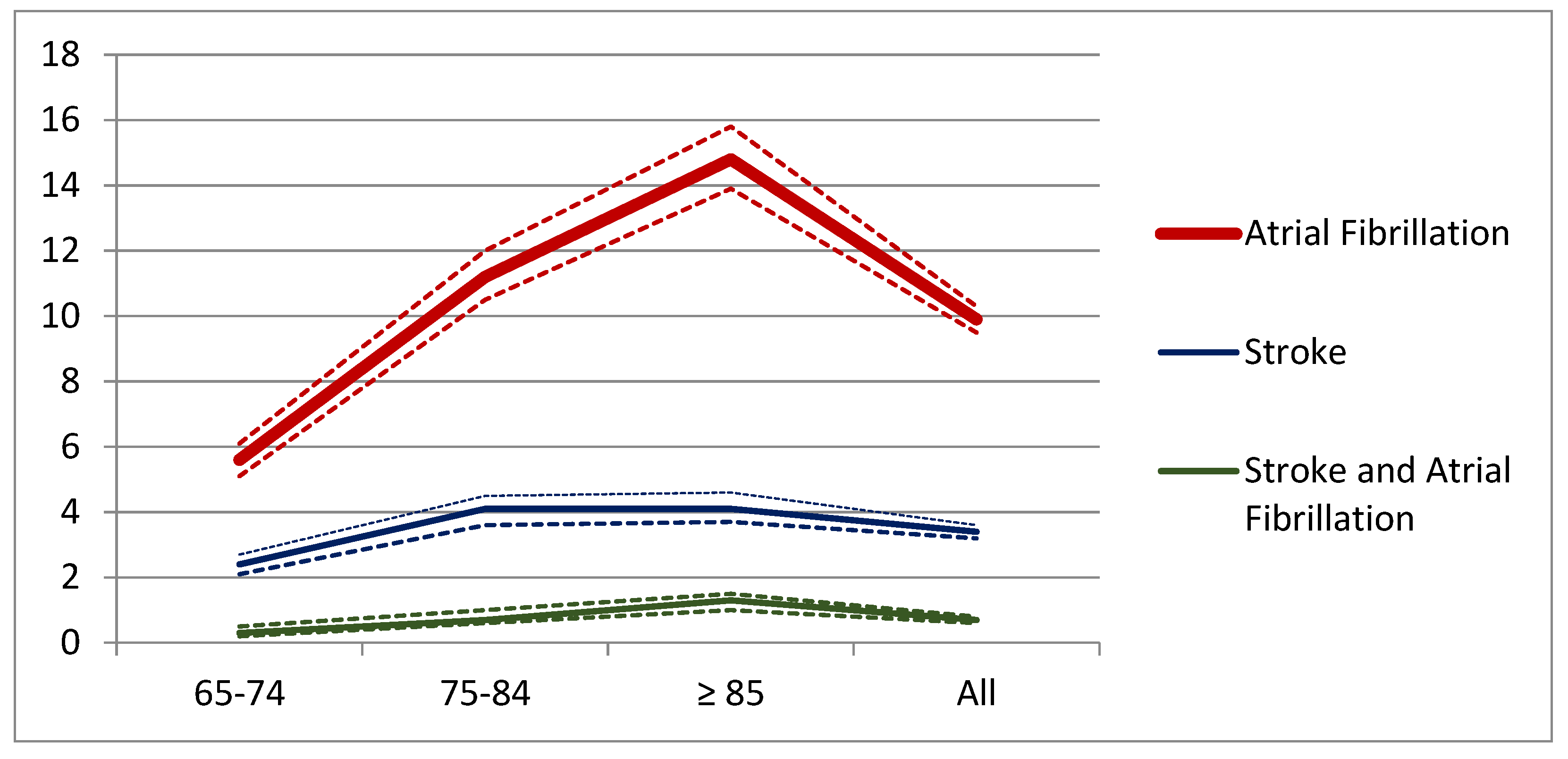
3.2. Atrial Fibrillation Incidence
3.3. Atrial Fibrillation and Stroke Incidence
3.4. Atrial Fibrillation and Cognitive Impairment
3.5. Atrial Fibrillation and Cardiovascular Comorbidities
4. Discussion
5. Conclusions
- 1.
- The individuals with the higher riskAF (Q4th) already had a similar risk to those with AF for ischemic heart disease, chronic kidney disease, or peripheral arteriopathy before their diagnosis of AF.
- 2.
- Unknown AF was diagnosed in 9.47% of patients at high risk of AF (Q4th) and among 21.1% of those with a new stroke. The NNS to detect one new case of AF was 15.
- 3.
- Individuals with prevalent AF had higher incidence of cardiovascular disease (MACE), four-fold higher risk of stroke, cognitive impairment (OR 1.34 (CI95% 1.1–1.5), and all-cause mortality (OR 1.14 (CI95% 1.0–1.2).
- 4.
- Stroke incidence increased progressively with AF risk levels. The 57.1% of simultaneous diagnoses of stroke and AF occurred in the Q4th risk level. The cardiovascular profile of individuals with AF and stroke was found to be different from those with atrial fibrillation alone.
- 5.
- The 41.7% of cases with cognitive impairment were concentrated in the Q4th risk level, were older (84.84 ± 6.70 vs. 81.22 ± 7.91, p < 0.001), and already had a higher incidence of cognitive impairment and mortality before diagnosing AF and displayed higher NIHSS (7.25 ± 8.62 vs. 4.55 ± 5.74, p = 0.002) scores than those without AF.
6. Patents
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A

References
- Cataluña. El Atlas Del Ictus. 2019. Available online: https://www.sen.es/images/2020/atlas/Informes_comunidad/Informe_ICTUS_Cataluna.pdf (accessed on 13 September 2022).
- Luengo-Fernandez, R.; Violato, M.; Candio, P.; Leal, J. Economic burden of stroke across Europe: A population-based cost analysis. Eur. Stroke J. 2020, 5, 17–25. [Google Scholar] [CrossRef]
- Rochmah, T.N.; Rahmawati, I.T.; Dahlui, M.; Budiarto, W.; Bilqis, N. Economic Burden of Stroke Disease: A Systematic Review. Int. J. Environ. Res. Public Health 2021, 18, 7552. [Google Scholar] [CrossRef]
- Tsao, C.W.; Aday, A.W.; Almarzooq, Z.I.; Anderson, C.A.M.; Arora, P.; Avery, C.L.; Baker-Smith, C.M.; Beaton, A.Z.; Boehme, A.K.; Buxton, A.E.; et al. American Heart Association Council on Epidemiology and Prevention Statistics Committee and Stroke Statistics Subcommittee. Heart Disease and Stroke Statistics-2023 Update: A Report from the American Heart Association. Circulation 2023, 8, e93–e621. [Google Scholar] [CrossRef]
- Salvatore, F.P.; Spada, A.; Fortunato, F.; Vrontis, D.; Fiore, M. Identification of Health Expenditures Determinants: A Model to Manage the Economic Burden of Cardiovascular Disease. Int. J. Environ. Res. Public Health 2021, 18, 4652. [Google Scholar] [CrossRef] [PubMed]
- European Stroke Organization, Stroke Alliance for Europe. Stroke Action Plan for Europe 2018–2030. Available online: https://www.safestroke.eu/wp-content/uploads/2019/05/SAFE-SAPE-ebook-correct-version_compressed-FINAL-FINAL.pdf (accessed on 10 July 2019).
- Yiin, G.S.; Howard, D.P.; Paul, N.L.; Li, L.; Luengo-Fernandez, R.; Bull, L.M.; Welch, S.J.; Gutnikov, S.A.; Mehta, Z.; Rothwell, P.M. Oxford Vascular Study. Age-specific incidence, outcome, cost, and projected future burden of atrial fibrillation-related embolic vascular events: A population-based study. Circulation 2014, 130, 1236–1244. [Google Scholar] [CrossRef] [Green Version]
- The World Health Organization. Global Burden of Stroke. Available online: https://www.who.int/cardiovascular_diseases/en/cvd_atlas_15_burden_stroke.pdf (accessed on 30 July 2022).
- Rivard, L.; Friberg, L.; Conen, D.; Healey, J.S.; Berge, T.; Boriani, G.; Brandes, A.; Calkins, H.; Camm, A.J.; Yee Chen, L.; et al. Atrial Fibrillation and Dementia: A Report From the AF-SCREEN International Collaboration. Circulation 2022, 145, 392–409. [Google Scholar] [CrossRef]
- Bosco, E.; Hsueh, L.; McConeghy, K.W.; Gravenstein, S.; Saade, E. Major adverse cardiovascular event definitions used in observational analysis of administrative databases: A systematic review. BMC Med. Res. Methodol. 2021, 21, 241. [Google Scholar] [CrossRef] [PubMed]
- Cotté, F.E.; Chaize, G.; Gaudin, A.F.; Samson, A.; Vainchtock, A.; Fauchier, L. Burden of stroke and other cardiovascular complications in patients with atrial fibrillation hospitalized in France. EP Eur. 2016, 18, 501–507. [Google Scholar] [CrossRef] [PubMed]
- Li, X.; Tse, V.C.; Au-Doung, L.W.; Wong, I.C.K.; Chan, E.W. The impact of ischaemic stroke on atrial fibrillation-related healthcare cost: A systematic review. EP Eur. 2017, 19, 937–947. [Google Scholar] [CrossRef] [PubMed]
- Sussman, M.; Menzin, J.; Lin, I.; Kwong, W.J.; Munsell, M.; Friedman, M.; Selim, M. Impact of atrial fibrillation on stroke-related healthcare costs. J. Am. Heart Assoc. 2013, 2, e000479. [Google Scholar] [CrossRef] [Green Version]
- de Andrés-Nogales, F.; Vivancos Mora, J.; Barriga Hernández, F.J.; Díaz Otero, F.; Izquierdo Esteban, L.; Ortega-Casarrubios, M.Á.; Castillo Moreno, L.; Ximénez-Carrillo Rico, Á.; Martín Torres, M.P.; Gómez-Escalonilla Escobar, C.I.; et al. Use of healthcare resources and costs of acute cardioembolic stroke management in the Region of Madrid: The CODICE Study. Neurología 2015, 30, 536–544, (In English and Spanish). [Google Scholar] [CrossRef] [PubMed]
- Queralt-Tomas, L.; Clua-Espuny, J.L.; Fernández-Saez, J.; Lleixà-Fortuño, M.M.; Albiol-Zaragoza, I.; Gil-Guillen, V.; Carratala-Munuera, C. Risk of Dependency: A Challenge for Health and Social Care Planning-Observational Stroke Cohort. Value in Health 2019, 22, 1083–1091. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Donkor, E.S. Stroke in the 21st Century: A Snapshot of the Burden, Epidemiology, and Quality of Life. Stroke Res. Treat. 2018, 2018, 3238165. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Health Information and Quality. Health Technology Assessment (HTA) of a National Screening Programme for Atrial Fibrillation in Primary Care. Available online: https://www.hiqa.ie/reports-and-publications/health-technology-assessments/hta-atrial-fibrillation-screening (accessed on 20 November 2022).
- Petryszyn, P.; Niewinski, P.; Staniak, A.; Piotrowski, P.; Well, A.; Well, M.; Jeskowiak, I.; Lip, G.; Ponikowski, P. Effectiveness of screening for atrial fibrillation and its determinants. A meta-analysis. PLoS ONE 2019, 14, e0213198. [Google Scholar] [CrossRef] [Green Version]
- Chan, N.Y. Systematic Screening for Atrial Fibrillation in the Community: Evidence and Obstacles. Arrhythm. Electrophysiol. Rev. 2018, 7, 39–42. [Google Scholar] [CrossRef]
- Institut d’Estadística de Catalunya. Idescat. Indicadors Demogràfics i de Territori. Estructura Per Edats, Envelliment i Dependència. Comarques i Aran. Available online: http://www.idescat.cat/pub/?id=inddt&n=915&by=com (accessed on 5 December 2022).
- Generalitat de Catalunya. Projeccions de Població Principals Resultats 2013–2051. Available online: https://www.idescat.cat/serveis/biblioteca/docs/cat/pp2021-2041pr.pdf (accessed on 5 December 2022).
- Idescat. Anuario Estadístico de Cataluña. Renda Familiar Disponible Bruta. Índex. Comarques i Aran, i Àmbits. Available online: http://www.idescat.cat/pub/?id=aec&n=941 (accessed on 5 December 2022).
- Pla de salut de la Regió Sanitària Terres de l’Ebre 2021-2025. Tortosa: Direcció General de Planificació i Recerca en Salut. 2022. Available online: https://scientiasalut.gencat.cat/handle/11351/7964 (accessed on 5 December 2022).
- Muria-Subirats, E.; Clua-Espuny, J.L.; Ballesta-Ors, J.; Lorman-Carbó, B.; Lechuga-Durán, I.; Fernández-Sáez, J.; Pla-Farnós, R. Incidence and Risk Assessment for Atrial Fibrillation at 5 Years: Hypertensive Diabetic Retrospective Cohort. Int. J. Environ. Res. 2020, 17, 3491. [Google Scholar] [CrossRef]
- Abellana, R.; Gonzalez-Loyola, F.; Verdu-Rotellar, J.M.; Bustamante, A.; Palà, E.; Clua-Espuny, J.L.; Montaner, J.; Pedrote, A.; Del Val-Garcia, J.L.; Ribas Segui, D.; et al. Predictive model for atrial fibrillation in hypertensive diabetic patients. Eur. J. Clin. Investig. 2021, 51, e13633. [Google Scholar] [CrossRef]
- Palà, E.; Bustamante, A.; Clúa-Espuny, J.L.; Acosta, J.; González-Loyola, F.; Santos, S.D.; Ribas-Segui, D.; Ballesta-Ors, J.; Penalba, A.; Giralt, M.; et al. Blood-biomarkers and devices for atrial fibrillation screening: Lessons learned from the AFRICAT (Atrial Fibrillation Research in CATalonia) study. PLoS ONE 2022, 17, e0273571. [Google Scholar] [CrossRef]
- Romiti, G.F.; Proietti, M.; Bonini, N.; Ding, W.Y.; Boriani, G.; Huisman, M.V.; Lip, G.Y.H.; GLORIA-AF Investigators. Adherence to the Atrial Fibrillation Better Care (ABC) pathway and the risk of major outcomes in patients with atrial fibrillation: A post-hoc analysis from the prospective GLORIA-AF Registry. EClinicalMedicine 2022, 55, 101757. [Google Scholar] [CrossRef]
- Ding, W.Y.; Proietti, M.; Romiti, G.F.; Vitolo, M.; Fawzy, A.M.; Boriani, G.; Marin, F.; Blomström-Lundqvist, C.; Potpara, T.S.; Fauchier, L.; et al. A EORP-AF Long-Term General Registry Investigators. Impact of ABC (Atrial Fibrillation Better Care) pathway adherence in high-risk subgroups with atrial fibrillation: A report from the ESC-EHRA EORP-AF long-term general registry. Eur. J. Intern. Med. 2023, 107, 60–65. [Google Scholar] [CrossRef]
- Hsieh, C.Y.; Lee, C.H.; Sung, S.F. Stroke occurrence while on antiplatelet therapy may predict atrial fibrillation detected after stroke. Atherosclerosis 2019, 283, 13–18. [Google Scholar] [CrossRef] [PubMed]
- Reverté-Villarroya, S.; Suñer-Soler, R.; Zaragoza-Brunet, J.; Martín-Ozaeta, G.; Esteve-Belloch, P.; Payo-Froiz, I.; Sauras-Colón, E.; Lopez-Espuela, F. Vascular Risk Factors in Ischemic Stroke Survivors: A Retrospective Study in Catalonia, Spain. Healthcare 2022, 10, 2219. [Google Scholar] [CrossRef] [PubMed]
- Liu, Y.; Wang, H.; Bai, B.; Liu, F.; Chen, Y.; Wang, Y.; Liang, Y.; Shi, X.; Yu, X.; Wu, C.; et al. Trends in Unhealthy Lifestyle Factors among Adults with Stroke in the United States between 1999 and 2018. J. Clin. Med. 2023, 12, 1223. [Google Scholar] [CrossRef] [PubMed]
- Clua-Espuny, J.L.; Lechuga-Duran, I.; Bosch-Princep, R.; Roso-Llorach, A.; Panisello-Tafalla, A.; Lucas-Noll, J.; López-Pablo, C.; Queralt-Tomas, L.; Giménez-Garcia, E.; González-Rojas, N.; et al. Prevalence of undiagnosed atrial fibrillation and of that not being treated with anticoagulant drugs: The AFABE study. Rev. Esp. Cardiol. 2013, 66, 545–552. [Google Scholar] [CrossRef]
- Freedman, B.; Schnabel, R.B. Atrial fibrillation screening perspectives after STROKESTOP and LOOP. Nat. Rev. Cardiol. 2023, 20, 1–2. [Google Scholar] [CrossRef]
- Freedman, B. Screening for Atrial Fibrillation A Report of the AF-SCREEN International Collaboration. Circulation 2017, 135, 1851–1867. [Google Scholar] [CrossRef]
- Hindricks, G.; Potpara, T.; Dagres, N.; Arbelo, E.; Bax, J.J.; Blomström-Lundqvist, C.; Boriani, G.; Castella, M.; Dan, G.A.; Dilaveris, P.E.; et al. ESC Scientific Document Group. 2020 ESC Guidelines for the diagnosis and management of atrial fibrillation developed in collaboration with the European Association for Cardio-Thoracic Surgery (EACTS): The Task Force for the diagnosis and management of atrial fibrillation of the European Society of Cardiology (ESC) Developed with the special contribution of the European Heart Rhythm Association (EHRA) of the ESC. Eur. Heart J. 2021, 42, 373–498. [Google Scholar] [CrossRef]
- Ballesta-Ors, J.; Clua-Espuny, J.L.; Gentille-Lorente, D.I.; Lechuga-Duran, I.; Fernández-Saez, J.; Muria-Subirats, E.; Blasco-Mulet, M.; Lorman-Carbo, B.; Alegret, J.M. Results, barriers and enablers in atrial fibrillation case finding: Barriers in opportunistic atrial fibrillation case finding-a cross-sectional study. Fam. Pract. 2020, 37, 486–492. [Google Scholar] [CrossRef]
- Proietti, M.; Mairesse, G.H.; Goethals, P.; Scavee, C.; Vijgen, J.; Blankoff, I.; Vandekerckhove, Y.; Lip, G.Y.; Belgian Heart Rhythm Week Investigators. A population screening programme for atrial fibrillation: A report from the Belgian Heart Rhythm Week screening programme. EP Eur. 2016, 18, 1779–1786. [Google Scholar] [CrossRef]
- Kearney, M.; Fay, M.; Fitzmaurice, D.A. Stroke prevention in atrial fibrillation: We can do better. Br. J. Gen. Pract. 2016, 66, 62–63. [Google Scholar] [CrossRef] [Green Version]
- Jatau, A.I.; Bereznicki, L.R.; Wimmer, B.C.; Bezabhe, W.M.; Peterson, G.M. Improving Knowledge and Early Detection of Atrial Fibrillation through a Community-Based Opportunistic Screening Program: What’s Your Beat? Int. J. Environ. Res. Public Health 2022, 19, 6860. [Google Scholar] [CrossRef] [PubMed]
- Panisello-Tafalla, A.; Clua-Espuny, J.L.; Gil-Guillen, V.F.; González-Henares, A.; Queralt-Tomas, M.L.; López-Pablo, C.; Lucas-Noll, J.; Lechuga-Duran, I.; Ripolles-Vicente, R.; Carot-Domenech, J.; et al. Results from the Registry of Atrial Fibrillation (AFABE): Gap between Undiagnosed and Registered Atrial Fibrillation in Adults—Ineffectiveness of Oral Anticoagulation Treatment with VKA. BioMed. Res. Int. 2015, 2015, 134756. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sociedad Española de Cardiología. Atlas del Mal Control de la Anticoagulación en Pacientes con Fibrilación Auricular no Valvular. Available online: https://secardiologia.es/images/secciones/clinica/atlas-mal-control-anticoagulacion-INFOGRAFIA.pdf (accessed on 23 June 2022).
- Oldgren, J.; Åsberg, S.; Hijazi, Z.; Wester, P.; Bertilsson, M.; Norrving, B. National TIMING Collaborators. Early Versus Delayed Non-Vitamin K Antagonist Oral Anticoagulant Therapy after Acute Ischemic Stroke in Atrial Fibrillation (TIMING): A Registry-Based Randomized Controlled Noninferiority Study. Circulation 2022, 146, 1056–1066. [Google Scholar] [CrossRef]
- López-López, J.A.; Sterne, J.A.C.; Thom, H.H.Z.; Higgins, J.P.T.; Hingorani, A.D.; Okoli, G.N.; Davies, P.A.; Bodalia, P.N.; Bryden, P.A.; Welton, N.J.; et al. Oral anticoagulants for prevention of stroke in atrial fibrillation: Systematic review, network meta-analysis, and cost effectiveness analysis. BMJ 2017, 359, j5058. [Google Scholar] [CrossRef] [Green Version]
- Jiang, C.; Li, S.; Wang, Y.; Lai, Y.; Bai, Y.; Zhao, M.; He, L.; Kong, Y.; Guo, X.; Li, S.; et al. Diastolic Blood Pressure and Intensive Blood Pressure Control on Cognitive Outcomes: Insights from the SPRINT MIND Trial. Hypertension 2023, 80, 580–589. [Google Scholar] [CrossRef] [PubMed]
- Giner-Soriano, M.; Casajuana, M.; Roso-Llorach, A.; Vedia, C.; Morros, R. Effectiveness, safety and costs of stroke prevention in non-valvular auricular fibrillation. Study of cohorts matched by Propensity score. Aten. Primaria 2020, 52, 176–184. [Google Scholar] [CrossRef]
- Gumprecht, J.; Lip, G.Y.H.; Sokal, A.; Średniawa, B.; Mitręga, K.; Stokwiszewski, J.; Wierucki, Ł.; Rajca, A.; Rutkowski, M.; Zdrojewski, T.; et al. Relationship between diabetes mellitus and atrial fibrillation prevalence in the Polish population: A report from the Non-invasive Monitoring for Early Detection of Atrial Fibrillation (NOMED-AF) prospective cross-sectional observational study. Cardiovasc. Diabetol. 2021, 20, 128. [Google Scholar] [CrossRef]
- Boehme, C.; Toell, T.; Mayer-Suess, L.; Domig, L.; Pechlaner, R.; Willeit, K.; Tschiderer, L.; Seekircher, L.; Willeit, P.; Griesmacher, A.; et al. The dimension of preventable stroke in a large representative patient cohort. Neurology 2019, 93, e2121–e2132. [Google Scholar] [CrossRef]
- Erkent, I.; Topcuoglu, M.A.; Sorgun, M.H.; Batur Caglayan, H.Z.; Togay Isikay, C.; Nazliel, B.; Arsava, E.M. Determinants of preventable stroke-Ankara ACROSS stroke preventability study. J. Stroke Cerebrovasc. Dis. 2020, 29, 104825. [Google Scholar] [CrossRef]
- Kahwati, L.; Asher, G.N.; Kadro, Z.O.; Keen, S.; Ali, R.; Coker-Schwimmer, E.; Jonas, D.E. Screening for Atrial Fibrillation: An Evidence Review for the US Preventive Services Task Force. Evid. Synth. 2022, 327, 368–383. [Google Scholar]
- Gillis, C.; Mirzaei, F.; Potashman, M.; Ikram, M.A.; Maserejian, N. The incidence of mild cognitive impairment: A systematic review and data synthesis. Alzheimers Dement. 2019, 11, 248–256. [Google Scholar] [CrossRef] [PubMed]
- Johansen, M.C.; Wang, W.; Zhang, M.; Knopman, D.S.; Ndumele, C.; Mosley, T.H.; Selvin, E.; Shah, A.M.; Solomon, S.D.; Gottesman, R.F.; et al. Risk of Dementia Associated with Atrial Cardiopathy: The ARIC Study. J. Am. Heart Assoc. 2022, 11, e025646. [Google Scholar] [CrossRef]
- Wang, W.; Zhang, M.J.; Inciardi, R.M.; Norby, F.L.; Johansen, M.C.; Parikh, R.; Van’t Hof, J.R.; Alonso, A.; Soliman, E.Z.; Mosley, T.H.; et al. Association of Echocardiographic Measures of Left Atrial Function and Size with Incident Dementia. JAMA Netw. Open 2022, 327, 1138–1148. [Google Scholar] [CrossRef]
- Maheshwari, A.; Norby, F.L.; Inciardi, R.M.; Wang, W.; Zhang, M.J.; Soliman, E.Z.; Alonso, A.; Johansen, M.C.; Gottesman, R.F.; Solomon, S.D.; et al. Left Atrial Mechanical Dysfunction and the Risk for Ischemic Stroke in People Without Prevalent Atrial Fibrillation or Stroke: A Prospective Cohort Study. Ann. Intern. Med. 2022, 176, 39–48. [Google Scholar] [CrossRef] [PubMed]
- Vera, A.; Cecconi, A.; Ximénez-Carrillo, Á.; Ramos, C.; Martínez-Vives, P.; Lopez-Melgar, B.; Sanz-García, A.; Ortega, G.; Aguirre, C.; Vivancos, J.; et al. DECRYTORING Study Investigators. Advanced Echocardiography with Left Atrial Strain and Indexed Left Atrial Three-Dimensional Volume for Predicting Underlying Atrial Fibrillation After Cryptogenic Stroke. Am. J. Cardiol. 2022, 185, 87–93. [Google Scholar] [CrossRef] [PubMed]
- Kim, D.; Yang, P.S.; Yu, H.T.; Kim, T.H.; Jang, E.; Sung, J.H.; Pak, H.N.; Lee, M.Y.; Lee, M.H.; Lip, G.Y.H.; et al. Risk of dementia in stroke-free patients diagnosed with atrial fibrillation: Data from a population-based cohort. Eur. Heart J. 2019, 40, 2313–2323. [Google Scholar] [CrossRef] [Green Version]
- Dagres, N.; Chao, T.F.; Fenelon, G.; Aguinaga, L.; Benhayon, D.; Benjamin, E.J.; Bunch, T.J.; Chen, L.Y.; Chen, S.A.; Darrieux, F.; et al. European Heart Rhythm Association (EHRA)/Heart Rhythm Society (HRS)/Asia Pacific Heart Rhythm Society (APHRS)/Latin American Heart Rhythm Society (LAHRS) expert consensus on arrhythmias and cognitive function: What is the best practice? Heart Rhythm. 2018, 15, e37–e60. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lip, G.Y.H. The ABC pathway: An integrated approach to improve AF management. Nat. Rev. Cardiol. 2017, 14, 627–628. [Google Scholar] [CrossRef]
- Chunyan, L.; Qionghua, D.; Haijiang, L.; Lianmei, Z. Association Between Silent Brain Infarcts and Cognitive Function: A Systematic Review and Meta-Analysis. J. Stroke Cerebrovasc. Dis. 2019, 28, 2376–2387. [Google Scholar] [CrossRef]
- Palà, E.; Escudero-Martínez, I.; Penalba, A.; Bustamante, A.; Lamana-Vallverdú, M.; Mancha, F.; Ocete, R.F.; Piñero, P.; Galvao-Carmona, A.; Gómez-Herranz, M.; et al. Association of blood-based biomarkers with radiologic markers and cognitive decline in atrial fibrillation patients. J. Stroke Cerebrovasc. Dis. 2022, 31, 106833. [Google Scholar] [CrossRef]
- Zungsontiporn, N.; Link, M.S. Newer technologies for detection of atrial fibrillation. BMJ 2018, 363, k3946. [Google Scholar] [CrossRef]
- Svennberg, E.; Tjong, F.; Goette, A.; Akoum, N.; Di Biaise, L.; Bordachar, P.; Boriani, G.; Burri, H.; Conte, G.; Deharo, J.C.; et al. How to use digital devices to detect and manage arrhythmias: An EHRA practical guide. EP Eur. 2022, 24, euac038. [Google Scholar] [CrossRef] [PubMed]
- Lubitz, S.A.; Faranesh, A.Z.; Selvaggi, C.; Atlas, S.J.; McManus, D.D.; Singer, D.E.; Pagoto, S.; McConnell, M.V.; Pantelopoulos, A.; Foulkes, A.S. Detection of Atrial Fibrillation in a Large Population Using Wearable Devices: The Fitbit Heart Study. Circulation 2022, 146, 1415–1424. [Google Scholar] [CrossRef] [PubMed]
- Turakhia, M.P.; Desai, M.; Hedlin, H.; Rajmane, A.; Talati, N.; Ferris, T.; Desai, S.; Nag, D.; Patel, M.; Kowey, P.; et al. Rationale and design of a large-scale, app-based study to identify cardiac arrhythmias using a smartwatch: The Apple Heart Study. Am. Heart J. 2019, 207, 66–75. [Google Scholar] [CrossRef] [PubMed]
- Dritsas, E.; Trigka, M. Stroke Risk Prediction with Machine Learning Techniques. Sensors 2022, 22, 4670. [Google Scholar] [CrossRef]
- Haq, I.U.; Chhatwal, K.; Sanaka, K.; Xu, B. Artificial Intelligence in Cardiovascular Medicine: Current Insights and Future Prospects. Vasc. Health Risk Manag. 2022, 18, 517–528. [Google Scholar] [CrossRef]
- Sposato, L.A.; Cipriano, L.E.; Saposnik, G.; Ruíz Vargas, E.; Riccio, P.M.; Hachinski, V. Diagnosis of atrial fibrillation after stroke and transient ischaemic attack: A systematic review and meta-analysis. Lancet Neurol. 2015, 14, 377–387. [Google Scholar] [CrossRef]
- Andrade, J.G.; Deyell, M.W.; Macle, L.; Wells, G.A.; Bennett, M.; Essebag, V.; Champagne, J.; Roux, J.F.; Yung, D.; Skanes, A.; et al. EARLY-AF Investigators. Progression of Atrial Fibrillation after Cryoablation or Drug Therapy. N. Engl. J. Med. 2023, 388, 105–116. [Google Scholar] [CrossRef]
- Kany, S.; Cardoso, V.R.; Bravo, L.; Williams, J.A.; Schnabel, R.; Fabritz, L.; Gkoutos, G.V.; Kirchhof, P. Eligibility for early rhythm control in patients with atrial fibrillation in the UK Biobank. Heart 2022, 108, 1873–1880. [Google Scholar] [CrossRef]
- Reiffel, J.A.; Verma, A.; Kowey, P.R.; Halperin, J.L.; Gersh, B.J.; Wachter, R.; Pouliot, E.; Ziegler, P.D.; REVEAL AF Investigators. Incidence of Previously Undiagnosed Atrial Fibrillation Using Insertable Cardiac Monitors in a High-Risk Population: The REVEAL AF Study. JAMA Cardiol 2017, 2, 1120–1127. [Google Scholar] [CrossRef]
- Clua-Espuny, J.L.; Muria-Subirats, E.; Ballesta-Ors, J.; Lorman-Carbo, B.; Clua-Queralt, J.; Palà, E.; Lechuga-Duran, I.; Gentille-Lorente, D.; Bustamante, A.; Muñoz, M.Á.; et al. Risk of Atrial Fibrillation, Ischemic Stroke and Cognitive Impairment: Study of a Population Cohort ≥65 Years of Age. Vasc. Health Risk. Manag. 2020, 16, 445–454. [Google Scholar] [CrossRef] [PubMed]
- Guo, Y.; Lane, D.A.; Wang, L.; Zhang, H.; Wang, H.; Zhang, W.; Wen, J.; Xing, Y.; Wu, F.; Xia, Y.; et al. mAF-App II Trial Investigators. Mobile Health Technology to Improve Care for Patients with Atrial Fibrillation. J. Am. Coll. Cardiol. 2020, 75, 1523–1534. [Google Scholar] [CrossRef] [PubMed]
- Hong, C.; Pencina, M.J.; Wojdyla, D.M.; Hall, J.L.; Judd, S.E.; Cary, M.; Engelhard, M.M.; Berchuck, S.; Xian, Y.; D’Agostino, R., Sr.; et al. Predictive Accuracy of Stroke Risk Prediction Models Across Black and White Race, Sex, and Age Groups. JAMA Netw. Open 2023, 329, 306–317. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
| Variables | All | No AF | AF | p |
|---|---|---|---|---|
| All (n) | 40,297 | 37,723 | 2574 | |
| Female | 18,878 | 17,535 | 1343 | <0.001 |
| Age average | 77.88 ± 8.47 | 77.65 ± 8.46 | 81.22 ± 7.91 | <0.001 |
| Arterial hypertension | 25,555 | 23,610 | 1945 | <0.001 |
| Diabetes mellitus | 10,458 | 9689 | 769 | <0.001 |
| BMI (kg/m2) | 28.71 ± 5.16 | 28.66 ± 5.14 | 29.5 ± 5.38 | <0.001 |
| Dyslipidemia | 19,129 | 17,913 | 1216 | 0.822 |
| Active Smoking | 838 | 809 | 29 | 0.854 |
| Risky Alcohol | 506 | 487 | 19 | 0.395 |
| Ischemic cardiomyopathy | 2915 | 2558 | 357 | <0.001 |
| Heart failure | 2772 | 2096 | 676 | <0.001 |
| Stroke | 885 | 698 | 187 | <0.001 |
| Peripheral vascular disease | 2776 | 2431 | 345 | <0.001 |
| Dementia/cognitive impairment | 3781 | 3471 | 310 | <0.001 |
| Antiplatelet therapy | 6251 | 6110 | 141 | <0,001 |
| CHA2DS2-VASc | 3.24 ± 1.16 | 3.20 ± 1.15 | 3.83 ± 1.2 | <0.001 |
| Anticoagulation | 2981 | 987 | 1994 | <0.001 |
| AntivitaminK | 1698 | 754 | 944 | <0.001 |
| NACO | 1288 | 235 | 1053 | <0.001 |
| Death—all causes | 7317 | 6799 | 518 | 0.008 |
| Variables | All | AF and Stroke | AF without Stroke | p |
|---|---|---|---|---|
| All (N) | 2574 | 187 | 2387 | <0.001 |
| Women (n) | 1343 | 112 | 1231 | 0.565 |
| Men (n) | 1231 | 97 | 1134 | |
| Average age (years ± SD) | 81.95 ± 8.46 | 82.91 | 81.87 | 0.899 |
| Arterial hypertension (n) | 2035 | 152 | 1883 | 0.667 |
| Diabetes mellitus (n) | 788 | 57 | 731 | 0.935 |
| BMI (kg/m2 average ± SD) | 28.71 ± 5.16 | 28.62 ± 5.21 | 29.40 ± 5.37 | 0.052 |
| Glomerular filtration rate (mL/min/1.73 m2) | 72.17 ± 18.89 | 65.92 ± 20.13 | 62.84 ± 20.43 | 0.069 |
| Dyslipidemia (n) | 1263 | 86 | 1177 | 0.374 |
| Ischemic cardiomyopathy (n) | 370 | 24 | 346 | 0.591 |
| Heart failure | 716 | 50 | 666 | 0.738 |
| Peripheral vascular disease(n) | 360 | 26 | 334 | 1.000 |
| MACE (n) | 1162 | 209 | 953 | <0.001 |
| CHA2DS2-VASc (average ± SD) | 3.83 ± 1.19 | 4.76 ± 1.1 | 3.74 ± 1.17 | <0.001 |
| Anticoagulation (n) | 2026 | 134 | 1892 | 0.016 |
| Pfeiffer score (average ± SD) | 3.02 ± 3.07 | 3.38 ± 2.91 | 2.98 ± 3.09 | 0.332 |
| Dementia/cognitive impairment (n) | 342 | 41 | 301 | <0.001 |
| Charlson score (average ± SD) | 1.81 ± 1.43 | 2.60 ± 1.36 | 1.75 ± 1.42 | <0.001 |
| Statins treatment (n) | 957 | 91 | 866 | =0.001 |
| Death—allcauses (n) | 2574 | 137 | 2437 | 0.008 |
| High AF Risk (Q4th) | New AF | No AF | OR AF/Q4 (CI95%) | OR AF/NoAF (CI95%) | |
|---|---|---|---|---|---|
| N | 10,072 | 2574 | 37,718 | ||
| AF all Incidence/1000 people per year (CI95%) | 1148 17.3 (16.3–18.3) | 2574 9.9 (9.5–10.3) | - | ||
| Women n (%) Incidence/1000 people per year (CI95%) | 2876 22.8 (20.7–25.1) | 1231 8.9 (8.4–9.4) | - | ||
| Men n (%) Incidence/1000 people per year (CI95%) | 7196 15.0 (13.9–16.1) | 1343 11.0 (10.4–11.6) | - | ||
| Stroke/Transient ischemic attack Incidence/1000 people per year (CI95%) | 456 6.9 (6.2–7.5) | 187 3.4 (3.2–3.6) | 698 2.7 (2.5–3.0) | 1.62 (1.37–1.92) p < 0.001 | 4.03 (3.43–4.74) p < 0.001 |
| Heart Failure Incidence/1000 people per year (CI95%) | 1.844 27.5 (26.3–28.8) | 676 40.1 (37.1–43.2) | 2.096 8.3 (7.9–8.6) | 1.45 (1.33–1.6) p < 0.001 | 4.85 (4.5–5.3) p < 0.001 |
| Ischemic Heart Disease Incidence/1000 people per year (CI95%) | 1468 22.0 (20.8–23.1) | 367 21.8 (19.6–24.1) | 2558 10.1 (9.7–10.5) | 0.99 (0.88–1.11) p = 0.908 | 2.16 (1.93–2.41) p < 0.001 |
| Major Cardiovascular Events Incidence/1000 people per year (CI95%) | 3791 56.3 (54.5–58.1) | 1230 73.0 (68.9–77.1) | 5352 21.1 (20.5–21.6) | 1.29 (1.21–1.38) p < 0.001 | 3.52 (3.31–3.75) p < 0.001 |
| Cognitive Impairment Incidence/1000 people per year (CI95%) | 1553 23.3 (22.1–24.5) | 310 18.4 (16.4–20.6) | 3471 13.7 (13.2–14.1) | 0.78 (0.69–0.89) p = 0.002 | 1.34 (1.19–1.51) p < 0.001 |
| Chronic Kidney Disease Incidence/1000 people per year (CI95%) | 2731 40.8 (39.3–42.3) | 676 40.1 (37.1–43.2) | 5158 20.3 (19.8–20.9) | 0.98 (0.90–1.06) p = 0.706 | 1.97 (1.82–2.13) p < 0.001 |
| Peripheral Arteriopathy Incidence/1000 people per year (CI95%) | 1.337 20.0 (18.9–21.1) | 345 20.5 (18.4–22.7) | 2.431 9.6 (9.2–10.0) | 1.02 (0.90–1.15) p = 0,724 | 2.13 (1.90–2.4) p < 0,001 |
| Death—allcauses Incidence/1000 people per year (CI95%) | 2822 42.5 (40.9–44.0) | 518 30.7 (28.1–33.5) | 6799 26.8 (26.1–27.4) | 0.72 (0.65–0.79) p < 0.001 | 1.14 (1.04–1.25) p = 0.027 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Clua-Espuny, J.-L.; Molto-Balado, P.; Lucas-Noll, J.; Panisello-Tafalla, A.; Muria-Subirats, E.; Clua-Queralt, J.; Queralt-Tomas, L.; Reverté-Villarroya, S.; Investigators EBRICTUS Research. Early Diagnosis of Atrial Fibrillation and Stroke Incidence in Primary Care: Translating Measurements into Actions—A Retrospective Cohort Study. Biomedicines 2023, 11, 1116. https://doi.org/10.3390/biomedicines11041116
Clua-Espuny J-L, Molto-Balado P, Lucas-Noll J, Panisello-Tafalla A, Muria-Subirats E, Clua-Queralt J, Queralt-Tomas L, Reverté-Villarroya S, Investigators EBRICTUS Research. Early Diagnosis of Atrial Fibrillation and Stroke Incidence in Primary Care: Translating Measurements into Actions—A Retrospective Cohort Study. Biomedicines. 2023; 11(4):1116. https://doi.org/10.3390/biomedicines11041116
Chicago/Turabian StyleClua-Espuny, Josep-Lluis, Pedro Molto-Balado, Jorgina Lucas-Noll, Anna Panisello-Tafalla, Eulalia Muria-Subirats, Josep Clua-Queralt, Lluïsa Queralt-Tomas, Silvia Reverté-Villarroya, and Investigators EBRICTUS Research. 2023. "Early Diagnosis of Atrial Fibrillation and Stroke Incidence in Primary Care: Translating Measurements into Actions—A Retrospective Cohort Study" Biomedicines 11, no. 4: 1116. https://doi.org/10.3390/biomedicines11041116