

Effect of Semaglutide on Subclinical Atherosclerosis and Cardiometabolic Compensation: A Real-World Study in Patients with Type 2 Diabetes

 ,
,  ,
,  and
and 
Abstract
:1. Introduction
2. Patients and Methods
2.1. Study Design
2.2. Patients
2.3. Study Measures
2.4. Statistical Analysis
3. Results
3.1. Study Population and Clinical Characteristics
3.2. Effectiveness Parameters
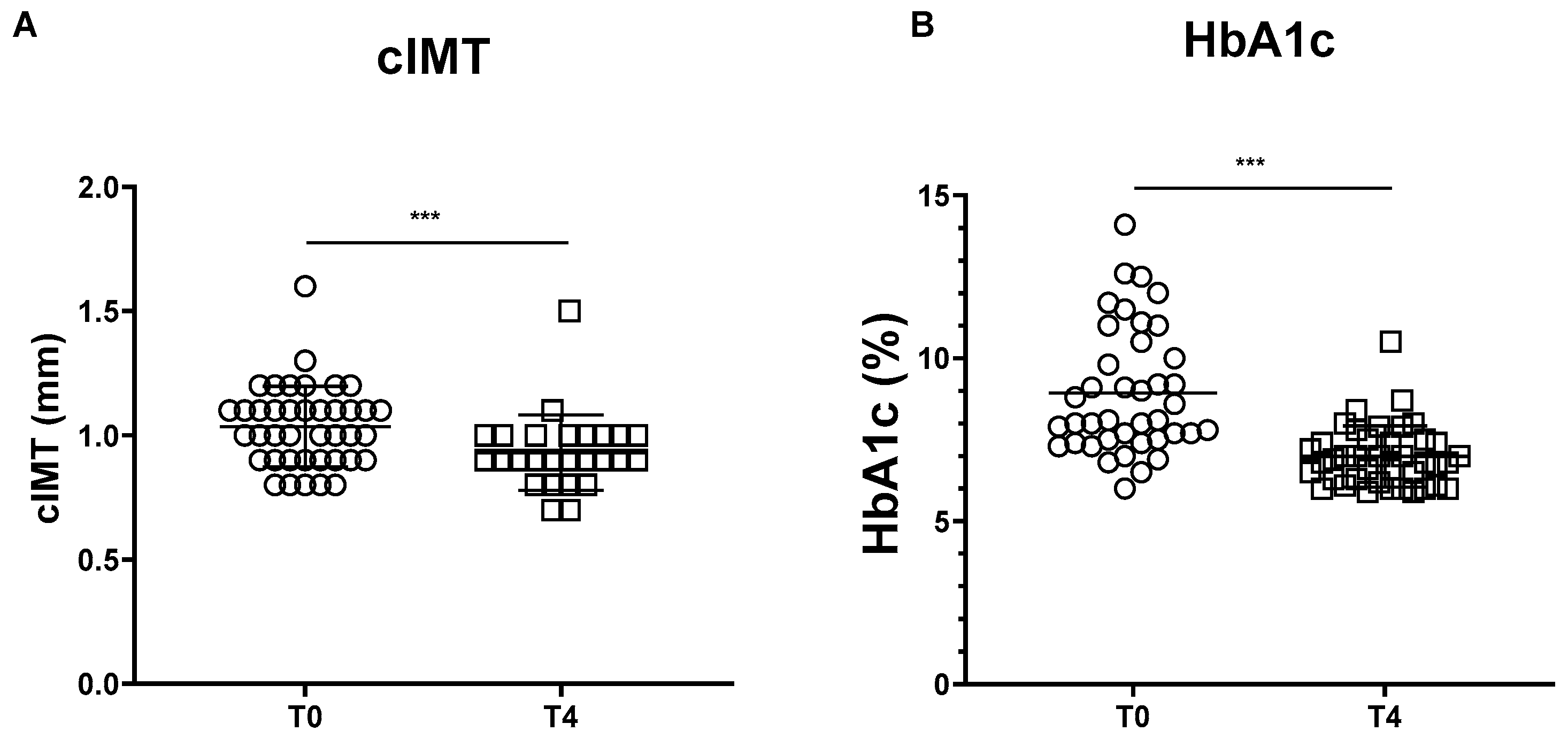
3.2.1. Carotid IMT
3.2.2. HbA1c Levels
3.3. Secondary Outcomes
3.4. Hepatic Steatosis and Fibrosis Markers and TyG Index
Correlation Analyses
3.5. Insulin Therapy during the Study Period
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Ma, C.X.; Ma, X.N.; Guan, C.H.; Li, Y.D.; Mauricio, D.; Fu, S.B. Cardiovascular disease in type 2 diabetes mellitus: Progress toward personalized management. Cardiovasc. Diabetol. 2022, 21, 74. [Google Scholar] [CrossRef] [PubMed]
- Rizzo, M.; Nauck, M.A.; Mantzoros, C.S. Incretin-based therapies in 2021—Current status and perspectives for the future. Metabolism 2021, 122, 154843. [Google Scholar] [CrossRef] [PubMed]
- Tashiro, Y.; Sato, K.; Watanabe, T.; Nohtomi, K.; Terasaki, M.; Nagashima, M.; Hirano, T. A glucagon-like peptide-1 analog liraglutide suppresses macrophage foam cell formation and atherosclerosis. Peptides 2014, 54, 19–26. [Google Scholar] [CrossRef] [PubMed]
- Tanaka, M.; Matsuo, Y.; Yamakage, H.; Masuda, S.; Terada, Y.; Muranaka, K.; Wada, H.; Hasegawa, K.; Shimatsu, A.; Satoh-Asahara, N. Differential effects of GLP-1 receptor agonist on foam cell formation in monocytes between non-obese and obese subjects. Metabolism 2016, 65, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Giglio, R.V.; Stoian, A.P.; Al-Rasadi, K.; Banach, M.; Patti, A.M.; Ciaccio, M.; Rizvi, A.A.; Rizzo, M. Novel therapeutical approaches to managing atherosclerotic risk. Int. J. Mol. Sci. 2021, 22, 4633. [Google Scholar] [CrossRef]
- Janez, A.; Muzurovic, E.; Stoian, A.P.; Haluzik, M.; Guja, C.; Czupryniak, L.; Duvnjak, L.; Lalic, N.; Tankova, T.; Bogdanski, P.; et al. Translating results from the cardiovascular outcomes trials with glucagon-like peptide-1 receptor agonists into clinical practice: Recommendations from a Eastern and Southern Europe diabetes expert group. Int. J. Cardiol. 2022, 365, 8–18. [Google Scholar] [CrossRef]
- Smits, M.M.; Van Raalte, D.H. Safety of semaglutide. Front. Endocrinol. 2021, 12, 645563. [Google Scholar] [CrossRef]
- Muzurović, E.M.; Volčanšek, Š.; Tomšić, K.Z.; Janež, A.; Mikhailidis, D.P.; Rizzo, M.; Mantzoros, C.S. Glucagon-like peptide-1 receptor agonists and dual glucose-dependent insulinotropic polypeptide/glucagon-like peptide-1 receptor agonists in the treatment of obesity/metabolic syndrome, prediabetes/diabetes and non-alcoholic fatty liver disease-current evidence. J. Cardiovasc. Pharmacol. Ther. 2022, 27, 10742484221146371. [Google Scholar]
- Lau, J.; Bloch, P.; Schäffer, L.; Pettersson, I.; Spetzler, J.; Kofoed, J.; Madsen, K.; Knudsen, L.B.; McGuire, J.; Steensgaard, D.B.; et al. Discovery of the once-weekly glucagon-like peptide-1 (GLP-1) analogue semaglutide. J. Med. Chem. 2015, 58, 7370–7380. [Google Scholar] [CrossRef]
- Mahapatra, M.K.; Karuppasamy, M.; Sahoo, B.M. Semaglutide, a glucagon like peptide-1 receptor agonist with cardiovascular benefits for management of type 2 diabetes. Rev. Endocr. Metab. Disord. 2022, 23, 521–539. [Google Scholar] [CrossRef]
- Tilinca, M.C.; Tiuca, R.A.; Niculas, C.; Varga, A.; Tilea, I. Future perspectives in diabesity treatment: Semaglutide, a glucagon-like peptide 1 receptor agonist (Review). Exp. Ther. Med. 2021, 22, 1167. [Google Scholar] [CrossRef] [PubMed]
- Aroda, V.R.; Capehorn, M.S.; Chaykin, L.; Frias, J.P.; Lausvig, N.L.; Macura, S.; Lüdemann, J.; Madsbad, S.; Rosenstock, J.; Tabak, O.; et al. Impact of baseline characteristics and beta-cell function on the efficacy and safety of subcutaneous once-weekly semaglutide: A patient-level, pooled analysis of the SUSTAIN 1-5 trials. Diabetes Obes. Metab. 2020, 22, 303–314. [Google Scholar] [CrossRef] [PubMed]
- Tan, X.; Cao, X.; Zhou, M.; Zou, P.; Hu, J. Efficacy and safety of once-weekly semaglutide for the treatment of type 2 diabetes. Expert Opin. Investig. Drugs 2017, 26, 1083–1089. [Google Scholar] [CrossRef] [PubMed]
- Marso, S.P.; Bain, S.C.; Consoli, A.; Eliaschewitz, F.G.; Jódar, E.; Leiter, L.A.; Lingvay, I.; Rosenstock, J.; Seufert, J.; Warren, M.L.; et al. Semaglutide and cardiovascular outcomes in patients with type 2 diabetes. N. Engl. J. Med. 2016, 375, 1834–1844. [Google Scholar] [CrossRef]
- Gardner, H.; Hamdy, O. Oral GLP1 analog: Where does the tide go? Clin. Med. Insights Endocrinol. Diabetes 2020, 13, 117955142098413. [Google Scholar] [CrossRef]
- Husain, M.; Bain, S.C.; Jeppesen, O.K.; Lingvay, I.; Sørrig, R.; Treppendahl, M.B.; Vilsbøll, T. Semaglutide (SUSTAIN and PIONEER) reduces cardiovascular events in type 2 diabetes across varying cardiovascular risk. Diabetes Obes. Metab. 2020, 22, 442–451. [Google Scholar] [CrossRef]
- Rakipovski, G.; Rolin, B.; Nøhr, J.; Klewe, I.; Frederiksen, K.S.; Augustin, R.; Hecksher-Sørensen, J.; Ingvorsen, C.; Polex-Wolf, J.; Knudsen, L.B. The GLP-1 analogs liraglutide and semaglutide reduce atherosclerosis in ApoE−/− and LDLr−/− mice by a mechanism that includes inflammatory pathways. JACC Basic Transl. Sci. 2018, 3, 844–857. [Google Scholar] [CrossRef]
- Vergès, B.; Charbonnel, B. After the LEADER trial and SUSTAIN-6, how do we explain the cardiovascular benefits of some GLP-1 receptor agonists? Diabetes Metab. 2017, 43 (Suppl. S1), 2S3–2S12. [Google Scholar] [CrossRef]
- Nikolic, D.; Patti, A.M.; Giglio, R.V.; Chianetta, R.; Castellino, G.; Magán-Fernández, A.; Citarrella, R.; Papanas, N.; Janez, A.; Stoian, A.P.; et al. Liraglutide improved cardiometabolic parameters more in obese than in non-obese patients with type 2 diabetes: A real-world 18-month prospective study. Diabetes Ther. 2022, 13, 453–464. [Google Scholar] [CrossRef]
- Kondo, T.; Miyakawa, N.; Kitano, S.; Watanabe, T.; Goto, R.; Suico, M.A.; Sato, M.; Takaki, Y.; Sakaguchi, M.; Igata, M.; et al. Activation of heat shock response improves biomarkers of NAFLD in patients with metabolic diseases. Endocr. Connect. 2021, 10, 521–533. [Google Scholar] [CrossRef]
- Harrison, S.A.; Oliver, D.; Arnold, H.L.; Gogia, S.; Neuschwander-Tetri, B.A. Development and validation of a simple NAFLD clinical scoring system for identifying patients without advanced disease. Gut 2008, 57, 1441–1447. [Google Scholar] [CrossRef] [PubMed]
- Citarrella, R.; Basile, G.; Mirarchi, L.; Amodeo, S.; Galletta, C.; Chianetta, R.; Nikolic, D.; Veronese, N.; Giannitrapani, L.; Soresi, M.; et al. Semaglutide e dulaglutide: Comparative effectiveness analysis e disparità nel Piano Terapeutico Regionale. J. AMD 2022, 25, 105–111. [Google Scholar] [CrossRef]
- Garber, A.J.; Abrahamson, M.J.; Barzilay, J.I.; Blonde, L.; Bloomgarden, Z.T.; Bush, M.A.; Dagogo-Jack, S.; DeFronzo, R.A.; Einhorn, D.; Fonseca, V.A.; et al. Consensus statement by the American Association of Clinical Endocrinologists and American College of Endocrinology on the comprehensive type 2 diabetes management algorithm—2017 executive summary. Endocr. Pract. 2017, 23, 207–238. [Google Scholar] [CrossRef] [PubMed]
- Goldenberg, R.M.; Steen, O. Semaglutide: Review and place in therapy for adults with type 2 diabetes. Can. J. Diabetes 2019, 43, 136–145. [Google Scholar] [CrossRef] [PubMed]
- Westerink, J.; Matthiessen, K.S.; Nuhoho, S.; Fainberg, U.; Lyng Wolden, M.; Østergaard, H.B.; Visseren, F.; Sattar, N. Estimated life-years gained free of new or recurrent major cardiovascular events with the addition of semaglutide to standard of care in people with type 2 diabetes and high cardiovascular risk. Diabetes Care 2022, 45, 1211–1218. [Google Scholar] [CrossRef]
- Verma, S.; Fainberg, U.; Husain, M.; Rasmussen, S.; Rydén, L.; Ripa, M.S.; Buse, J.B. Applying REWIND cardiovascular disease criteria to SUSTAIN 6 and PIONEER 6: An exploratory analysis of cardiovascular outcomes with semaglutide. Diabetes Obes. Metab. 2021, 23, 1677–1680. [Google Scholar] [CrossRef]
- Rizzo, M.; Chandalia, M.; Patti, A.M.; Di Bartolo, V.; Rizvi, A.A.; Montalto, G.; Abate, N. Liraglutide decreases carotid intima-media thickness in patients with type 2 diabetes: 8-month prospective pilot study. Cardiovasc. Diabetol. 2014, 13, 49. [Google Scholar] [CrossRef]
- Rizzo, M.; Rizvi, A.A.; Patti, A.M.; Nikolic, D.; Giglio, R.V.; Castellino, G.; Li Volti, G.; Caprio, M.; Montalto, G.; Provenzano, V.; et al. Liraglutide improves metabolic parameters and carotid intima-media thickness in diabetic patients with the metabolic syndrome: An 18-month prospective study. Cardiovasc. Diabetol. 2016, 15, 162. [Google Scholar] [CrossRef]
- Patti, A.M.; Nikolic, D.; Magan-Fernandez, A.; Giglio, R.V.; Castellino, G.; Chianetta, R.; Citarrella, R.; Corrado, E.; Provenzano, F.; Provenzano, V.; et al. Exenatide once-weekly improves metabolic parameters, endothelial dysfunction and carotid intima-media thickness in patients with type-2 diabetes: An 8-month prospective study. Diabetes Res. Clin. Pract. 2019, 149, 163–169. [Google Scholar] [CrossRef]
- Song, X.; Jia, H.; Jiang, Y.; Wang, L.; Zhang, Y.; Mu, Y.; Liu, Y. Anti-atherosclerotic effects of the glucagon-like peptide-1 (GLP-1) based therapies in patients with type 2 diabetes mellitus: A meta-analysis. Sci. Rep. 2015, 5, 10202. [Google Scholar] [CrossRef]
- Sonmez, A.; Yilmaz, M.I.; Saglam, M.; Unal, H.U.; Gok, M.; Cetinkaya, H.; Karaman, M.; Haymana, C.; Eyileten, T.; Oguz, Y.; et al. The role of plasma triglyceride/high-density lipoprotein cholesterol ratio to predict cardiovascular outcomes in chronic kidney disease. Lipids Health Dis. 2015, 14, 29. [Google Scholar] [CrossRef] [PubMed]
- Rizzo, M.; Rini, G.B.; Berneis, K. The clinical relevance of LDL size and subclasses modulation in patients with type-2 diabetes. Exp. Clin. Endocrinol. Diabetes 2007, 115, 477–482. [Google Scholar] [CrossRef] [PubMed]
- Rizzo, M.; Berneis, K. The clinical relevance of low-density-lipoproteins size modulation by statins. Cardiovasc. Drugs Ther. 2006, 20, 205–217. [Google Scholar] [CrossRef] [PubMed]
- Nikolic, D.; Giglio, R.V.; Rizvi, A.A.; Patti, A.M.; Montalto, G.; Maranta, F.; Cianflone, D.; Stoian, A.P.; Rizzo, M. Liraglutide reduces carotid intima-media thickness by reducing small dense low-density lipoproteins in a real-world setting of patients with type 2 diabetes: A novel anti-atherogenic effect. Diabetes Ther. 2021, 12, 261–274. [Google Scholar] [CrossRef]
- Rizzo, M.; Nikolic, D.; Patti, A.M.; Mannina, C.; Montalto, G.; McAdams, B.S.; Rizvi, A.A.; Cosentino, F. GLP-1 receptor agonists and reduction of cardiometabolic risk: Potential underlying mechanisms. Biochim. Biophys. Acta Mol. Basis Dis. 2018, 1864, 2814–2821. [Google Scholar] [CrossRef]
- Janić, M.; Rizzo, M.; Cosentino, F.; Pantea Stoian, A.; Lunder, M.; Šabović, M.; Janež, A. Effect of oral semaglutide on cardiovascular parameters and their mechanisms in patients with type 2 diabetes: Rationale and design of the Semaglutide Anti-Atherosclerotic Mechanisms of Action Study (SAMAS). Diabetes Ther. 2022, 13, 795–810. [Google Scholar] [CrossRef]
- Mountfort, K. ADA 2019 Oral Semaglutide—The PIONEER Program Trials. 2021. Available online: https://www.touchendocrinology.com/insight/ada-2019-oral-semaglutide-the-pioneer-program-trials/ (accessed on 9 March 2023).
- Ahmann, A.J.; Capehorn, M.; Charpentier, G.; Dotta, F.; Henkel, E.; Lingvay, I.; Holst, A.G.; Annett, M.P.; Aroda, V.R. Efficacy and safety of once-weekly semaglutide versus exenatide ER in subjects with type 2 diabetes (SUSTAIN 3): A 56-week, open-label, randomized clinical trial. Diabetes Care 2018, 41, 258–266. [Google Scholar] [CrossRef]
- Pratley, R.E.; Aroda, V.R.; Lingvay, I.; Lüdemann, J.; Andreassen, C.; Navarria, A.; Viljoen, A.; SUSTAIN 7 investigators. Semaglutide versus dulaglutide once weekly in patients with type 2 diabetes (SUSTAIN 7): A randomised, open-label, phase 3b trial. Lancet Diabetes Endocrinol. 2018, 6, 275–286. [Google Scholar] [CrossRef]
- Smith, N.K.; Hackett, T.A.; Galli, A.; Flynn, C.R. GLP-1: Molecular mechanisms and outcomes of a complex signaling system. Neurochem. Int. 2019, 128, 94–105. [Google Scholar] [CrossRef]
- Sachinidis, A.; Nikolic, D.; Stoian, A.P.; Papanas, N.; Tarar, O.; Rizvi, A.A.; Rizzo, M. Cardiovascular outcomes trials with incretin-based medications: A critical review of data available on GLP-1 receptor agonists and DPP-4 inhibitors. Metabolism 2020, 111, 154343. [Google Scholar] [CrossRef]
- Vekic, J.; Zeljkovic, A.; Cicero, A.F.G.; Janez, A.; Stoian, A.P.; Sonmez, A.; Rizzo, M. Atherosclerosis development and progression: The role of atherogenic small, dense LDL. Medicina 2022, 58, 299. [Google Scholar] [CrossRef] [PubMed]
- Jensen, J.K.; Binderup, T.; Grandjean, C.E.; Bentsen, S.; Ripa, R.S.; Kjaer, A. Semaglutide reduces vascular inflammation investigated by PET in a rabbit model of advanced atherosclerosis. Atherosclerosis 2022, 352, 88–95. [Google Scholar] [CrossRef] [PubMed]
- Buse, J.B.; Wexler, D.J.; Tsapas, A.; Rossing, P.; Mingrone, G.; Mathieu, C.; D’Alessio, D.A.; Davies, M.J. 2019 Update to: Management of Hyperglycemia in Type 2 Diabetes, 2018. A Consensus Report by the American Diabetes Association (ADA) and the European Association for the Study of Diabetes (EASD). Diabetes Care 2020, 43, 487–493. [Google Scholar] [CrossRef] [PubMed]
- Davies, M.J.; Aroda, V.R.; Collins, B.S.; Gabbay, R.A.; Green, J.; Maruthur, N.M.; Rosas, S.E.; Del Prato, S.; Mathieu, C.; Mingrone, G.; et al. Management of hyperglycemia in type 2 diabetes, 2022. A consensus report by the American Diabetes Association (ADA) and the European Association for the Study of Diabetes (EASD). Diabetes Care 2022, 45, 2753–2786. [Google Scholar] [CrossRef] [PubMed]
- Cosentino, F.; Grant, P.J.; Aboyans, V.; Bailey, C.J.; Ceriello, A.; Delgado, V.; Federici, M.; Filippatos, G.; Grobbee, D.E.; Hansen, T.B.; et al. 2019 ESC Guidelines on diabetes, pre-diabetes, and cardiovascular diseases developed in collaboration with the EASD. Eur. Heart J. 2020, 41, 255–323. [Google Scholar] [CrossRef] [PubMed]
- Sahin, Y.; Unluhizarci, K.; Yilmazsoy, A.; Yikilmaz, A.; Aygen, E.; Kelestimur, F. The effects of metformin on metabolic and cardiovascular risk factors in nonobese women with polycystic ovary syndrome. Clin. Endocrinol. 2007, 67, 904–908. [Google Scholar] [CrossRef]
- Katakami, N.; Yamasaki, Y.; Hayaishi-Okano, R.; Ohtoshi, K.; Kaneto, H.; Matsuhisa, M.; Kosugi, K.; Hori, M. Metformin or gliclazide, rather than glibenclamide, attenuate progression of carotid intima-media thickness in subjects with type 2 diabetes. Diabetologia 2004, 47, 1906–1913. [Google Scholar] [CrossRef] [PubMed]
- Lim, S.S.; Norman, R.J.; Clifton, P.M.; Noakes, M. The effect of comprehensive lifestyle intervention or metformin on obesity in young women. Nutr. Metab. Cardiovasc. Dis. 2011, 21, 261–268. [Google Scholar] [CrossRef]


{kind=link}
| Variables | Overall Population (n = 40) |
|---|---|
| Age (years) | 66 ± 10 |
| Male | 26 (65) |
| Weight (kg) | 88 ± 16 |
| BMI (kg/m2) | 32 ± 5 |
| cIMT (mm) | 1 ± 0.1 |
| Disease duration (years): | 14 ± 10 |
| ● Early diabetes | 12 (30) |
| ● Medium diabetes | 9 (22) |
| ● Late diabetes | 19 (47) |
| Smoking status: | |
| ● Yes | 13 (32) |
| ● Ex-smoker | 16 (40) |
| ● No | 11 (28) |
| Familiarity with CV diseases | 23 (57) |
| Comorbidities: | |
| ● Hypertension | 34 (85) |
| ● Dyslipidemia | 32 (80) |
| ● Obesity | 28 (70) |
| ● Diabetes complications | 11 (27) |
| Diabetes therapies: | |
| ● Metformin | 35 (87) |
| ● Gliptins | 3 (7) |
| ● SGLT-2 inhibitors | 7 (17) |
| ● SU | 9 (22) |
| ● Pioglitazone | 3 (7) |
| ● Glargine | 7 (17) |
| ● Degludec | 1 (2) |
| Concomitant therapies: | |
| ● Β-blockers | 18 (45) |
| ● ACE inhibitors | 13 (32) |
| ● Calcium antagonists | 11 (27) |
| ● Diuretics | 15 (37) |
| ● AT1R blockers | 20 (50) |
| Lipid-lowering drugs: | |
| ● Statins | 30 (75) |
| ● Fibrates | 2 (5) |
| ● Omega-3 | 6 (15) |
| ● Aspirin use | 25 (62) |
| Variables | Baseline (Mean ± SD) | 4 Months (Mean ± SD) | p-Value |
|---|---|---|---|
| Anthropometric parameters: | |||
| Weight (kg) | 88 ± 16 | 83 ± 14 | <0.001 |
| Waist (cm) | 101 ± 11 | 97 ± 10 | <0.001 |
| BMI (kg/m2) | 32 ± 5 | 30 ± 5 | <0.001 |
| Glycemic parameters: | |||
| Glycemia (mg/dL) | 176 ± 75 | 122 ± 22 | <0.001 |
| HbA1c (%) | 9 ± 2 | 7 ± 1 | <0.001 |
| Plasma lipids: | |||
| Total CHO (mg/dL) | 179 ± 42 | 155 ± 29 | <0.001 |
| TG (mg/dL) | 157 ± 90 | 131 ± 44 | 0.021 |
| LDL CHO (mg/dL) | 106 ± 40 | 88 ± 28 | <0.001 |
| HDL CHO (mg/dL) | 42 ± 11 | 42 ± 9 | 0.058 |
| Hepatic parameters: | |||
| Alkaline phosphatase (U/L) | 78 ± 45 | 66 ± 25 | 0.004 |
| GGT (UI/L) | 39 ± 24 | 34 ± 17 | 0.011 |
| AST (UI/L) | 22 ± 12 | 20 ± 7 | 0.067 |
| ALT (UI/L) | 29 ± 18 | 24 ± 11 | 0.002 |
| Carotid IMT | 1 ± 0.1 | 0.9 ± 0.1 | <0.001 |
| Variables | Baseline (Mean ± SD) | 4 Months (Mean ± SD) | p-Value |
|---|---|---|---|
| Steatosis markers: | |||
| ● FLI | 71.4 ± 21.3 | 61.6 ± 22.4 | <0.001 |
| ● HSI | 45.1 ± 6.0 | 42.3 ± 5.2 | <0.001 |
| Fibrosis markers: | |||
| ● AST/ALT ratio | 0.83 ± 0.26 | 0.88 ± 0.19 | 0.173 |
| ● BARD score | 2.8 ± 1.0 | 3.0 ± 1.0 | 0.115 |
| ● TyG index | 6.4 ± 0.7 | 6.0 ± 0.4 | <0.001 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Patti, A.M.; Giglio, R.V.; Allotta, A.; Bruno, A.; Di Bella, T.; Pantea Stoian, A.; Ciaccio, M.; Rizzo, M. Effect of Semaglutide on Subclinical Atherosclerosis and Cardiometabolic Compensation: A Real-World Study in Patients with Type 2 Diabetes. Biomedicines 2023, 11, 1362. https://doi.org/10.3390/biomedicines11051362
Patti AM, Giglio RV, Allotta A, Bruno A, Di Bella T, Pantea Stoian A, Ciaccio M, Rizzo M. Effect of Semaglutide on Subclinical Atherosclerosis and Cardiometabolic Compensation: A Real-World Study in Patients with Type 2 Diabetes. Biomedicines. 2023; 11(5):1362. https://doi.org/10.3390/biomedicines11051362
Chicago/Turabian StylePatti, Angelo Maria, Rosaria Vincenza Giglio, Alberto Allotta, Andreina Bruno, Tommaso Di Bella, Anca Pantea Stoian, Marcello Ciaccio, and Manfredi Rizzo. 2023. "Effect of Semaglutide on Subclinical Atherosclerosis and Cardiometabolic Compensation: A Real-World Study in Patients with Type 2 Diabetes" Biomedicines 11, no. 5: 1362. https://doi.org/10.3390/biomedicines11051362
APA StylePatti, A. M., Giglio, R. V., Allotta, A., Bruno, A., Di Bella, T., Pantea Stoian, A., Ciaccio, M., & Rizzo, M. (2023). Effect of Semaglutide on Subclinical Atherosclerosis and Cardiometabolic Compensation: A Real-World Study in Patients with Type 2 Diabetes. Biomedicines, 11(5), 1362. https://doi.org/10.3390/biomedicines11051362