
Metabolomic Investigation of Blood and Urinary Amino Acids and Derivatives in Patients with Type 2 Diabetes Mellitus and Early Diabetic Kidney Disease

 , , , and
, , , and
Abstract
:
1. Introduction
2. Materials and Methods
2.1. Patients and Compliance with Ethical Standards
2.2. Blood and Urine Collection and Processing
2.3. UHPLC-QTOF-ESI+-MS Analysis
2.4. Statistical Analysis
3. Results
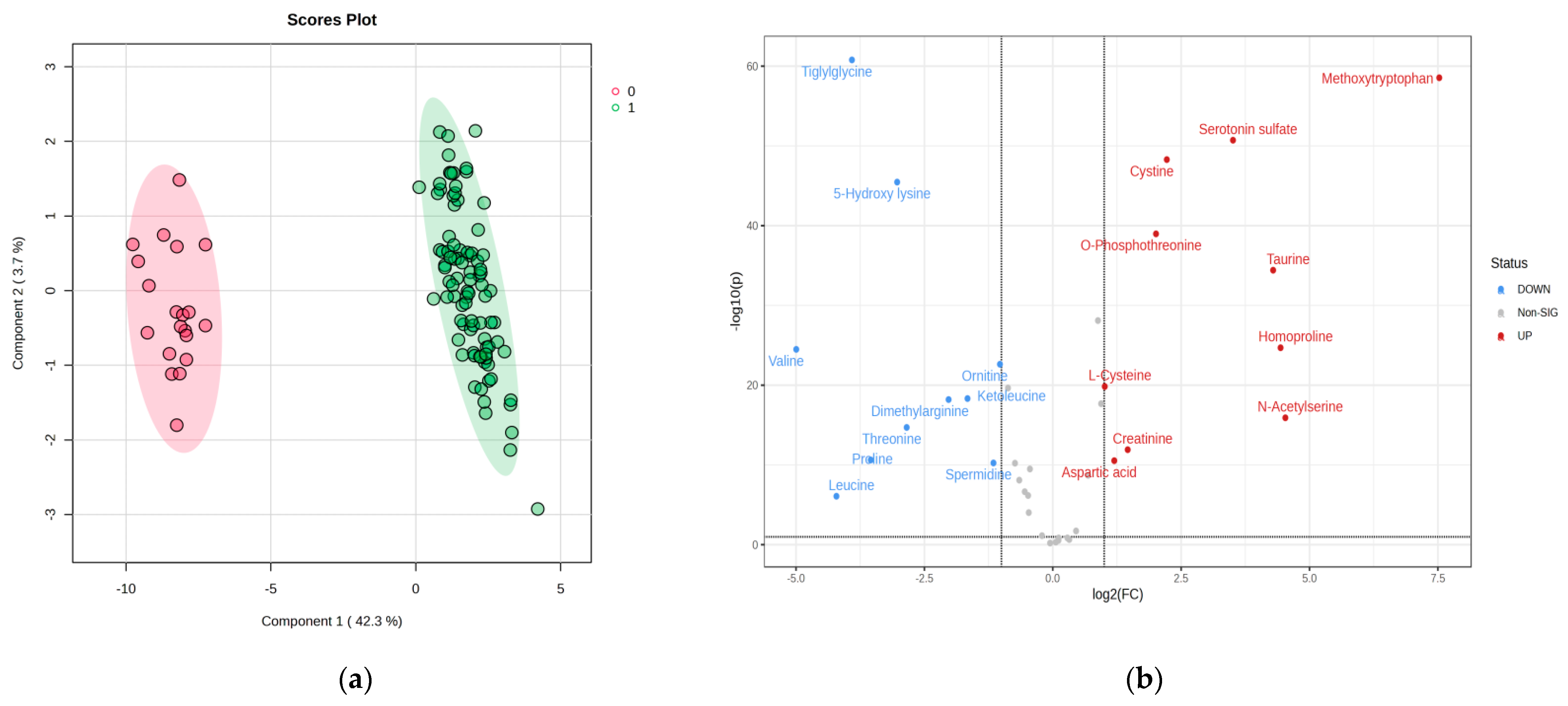
3.1. Multivariate Analysis of Blood Serum
3.1.1. PLSDA and Volcano Plot
3.1.2. Fold Change Values, VIP Scores, and Random Forest Data
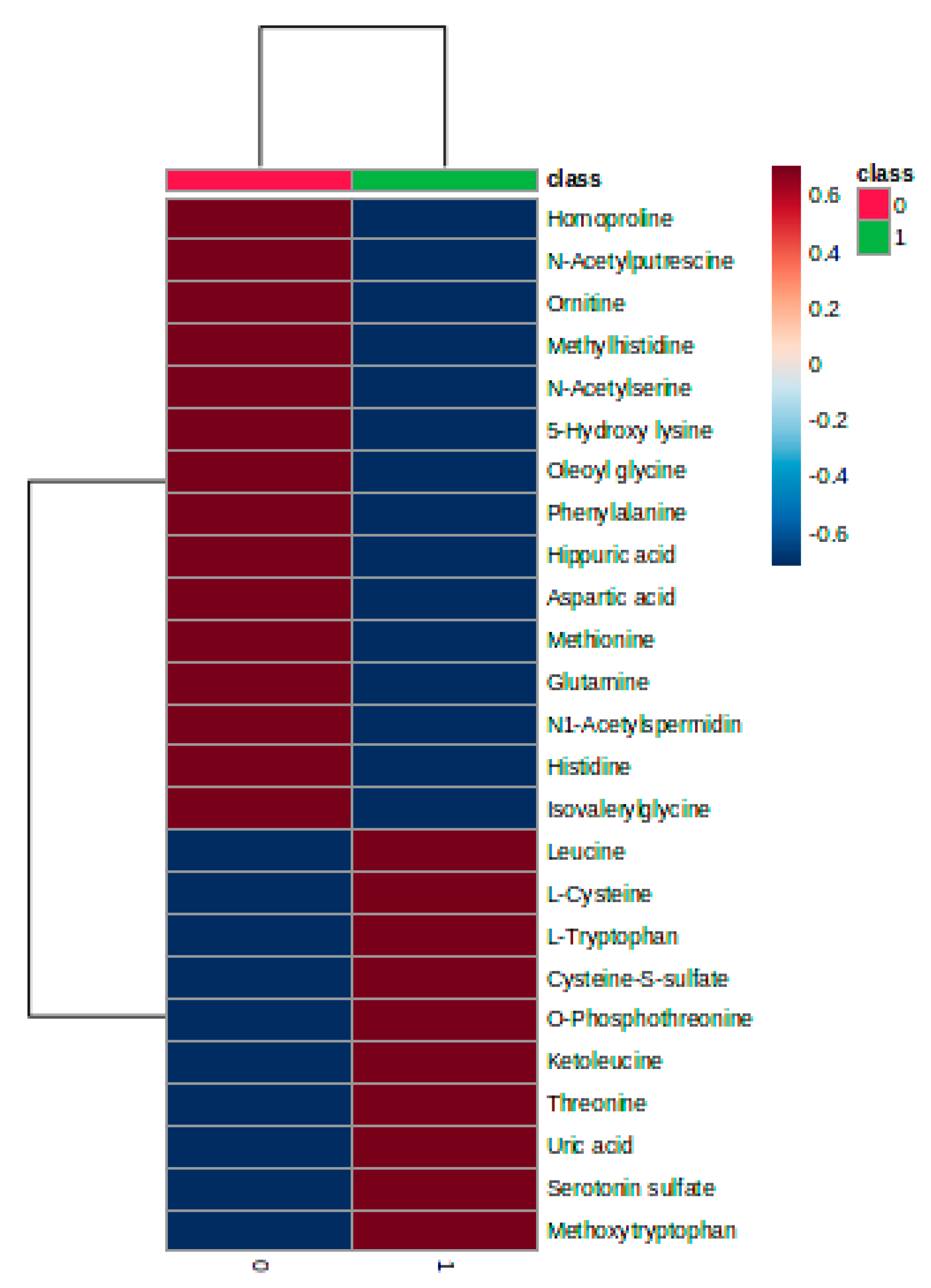
3.1.3. Heatmap
3.1.4. Biomarker Analysis
3.2. Univariate Analysis (One-Way ANOVA) to Evaluate the Relationship between Blood Metabolites and DKD/2DM Progression
3.2.1. ANOVA Parameters and Fisher’s LSD, VIP Scores, and MDA Values
3.2.2. PLSDA and Heatmap
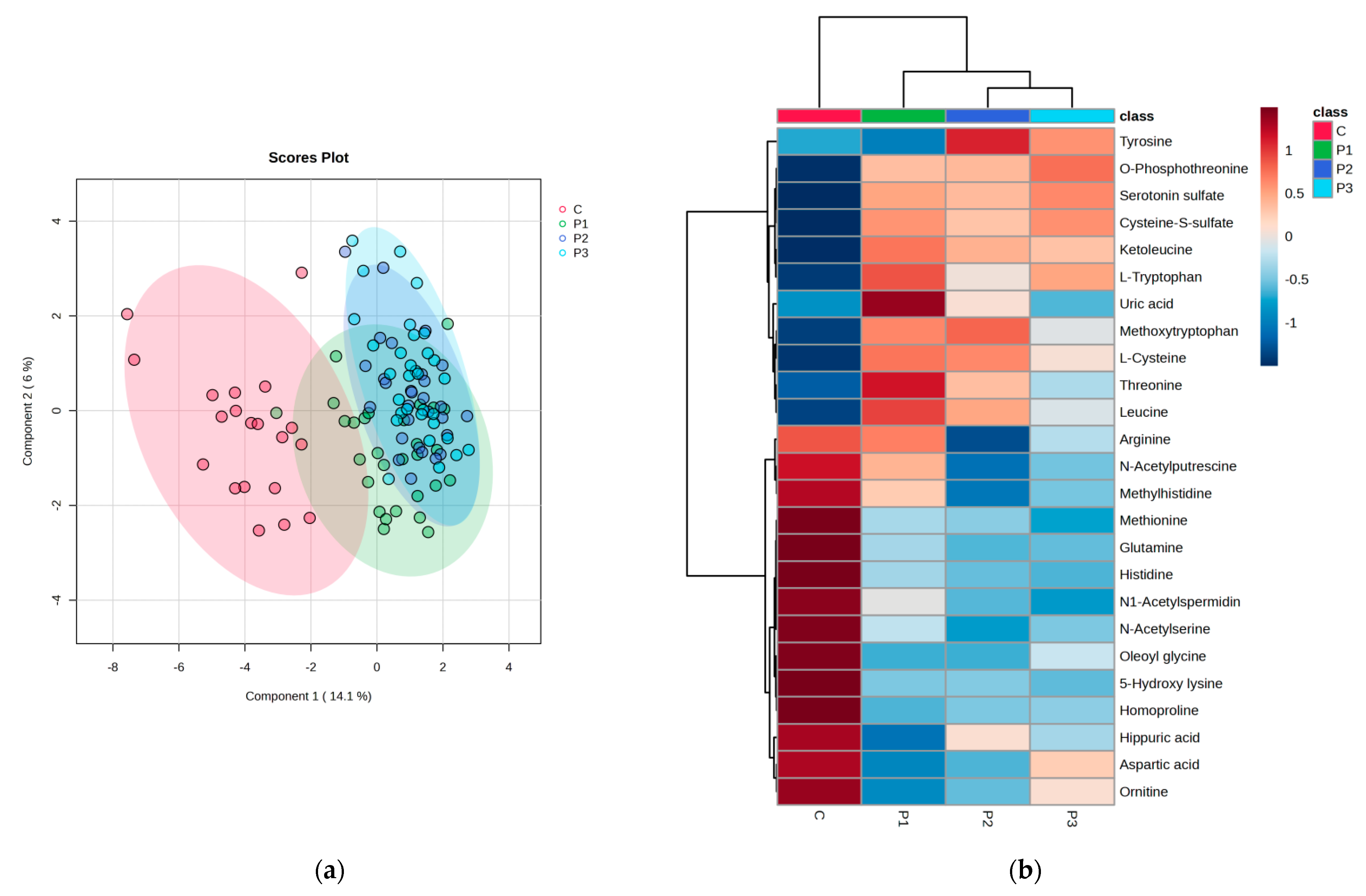
3.3. Multivariate Analysis of Urine
3.3.1. PLSDA and Volcano Plot
3.3.2. Fold Change Values, VIP Scores, and Random Forest Data
3.3.3. Heatmap
3.3.4. Biomarker Analysis
3.4. Univariate Analysis (One-Way ANOVA) to Evaluate the Relationship between Urine Metabolites and DKD/2DM Progression (from P1 to P3)
3.4.1. Analysis of Variance (ANOVA) Parameters and Fisher’s LSD, VIP Scores and MDA Values
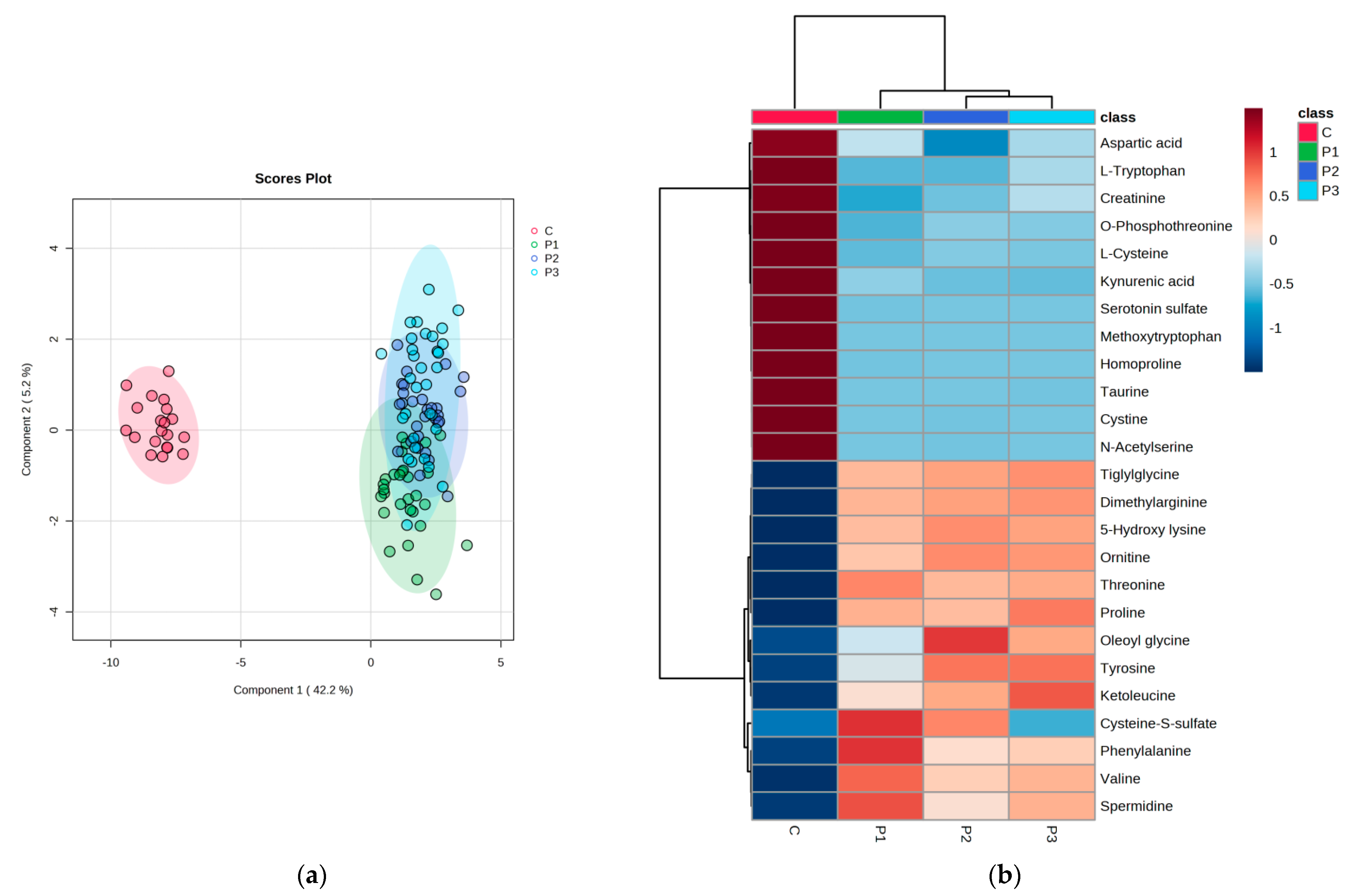
3.4.2. PLSDA and Heatmap
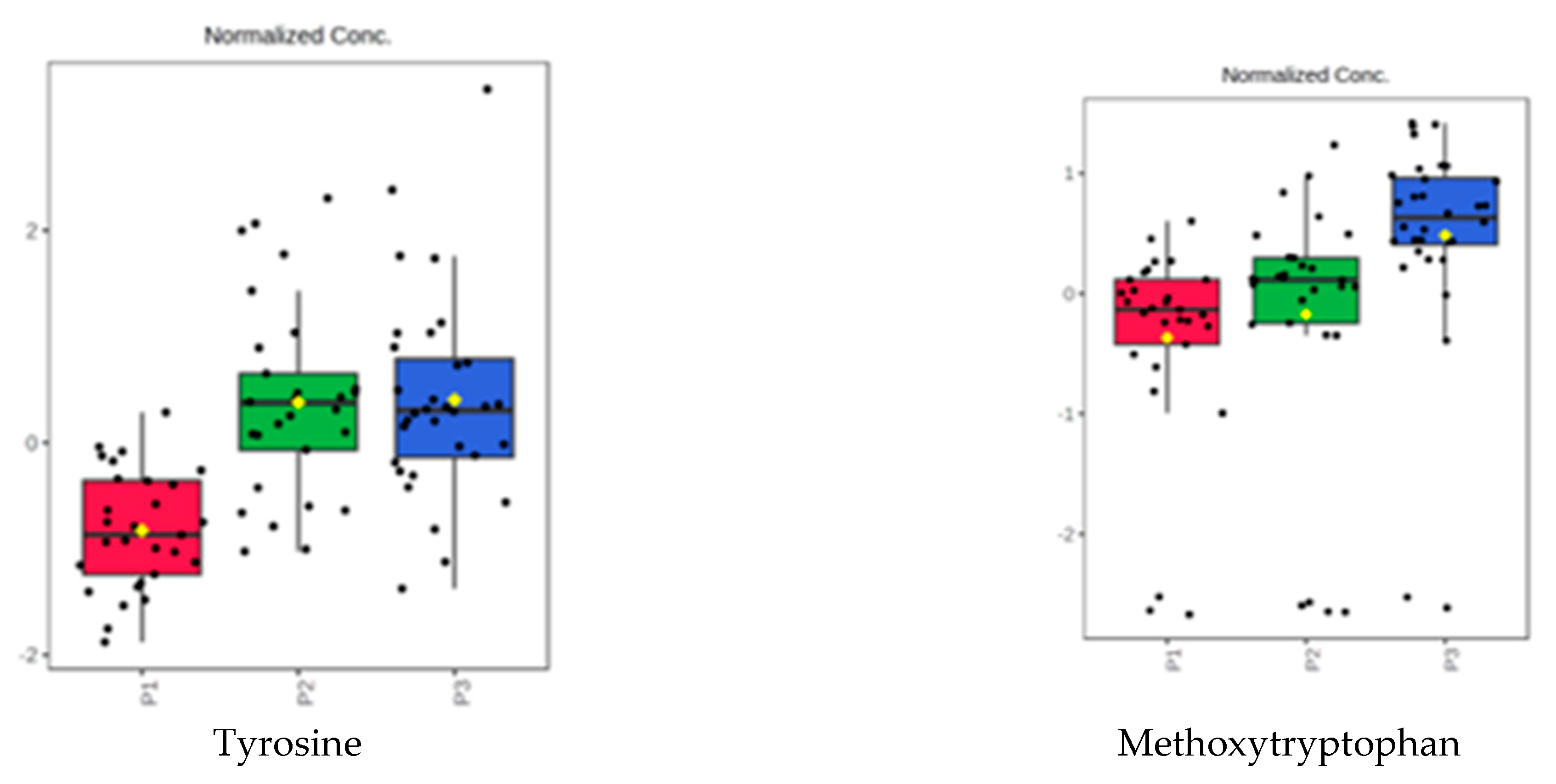
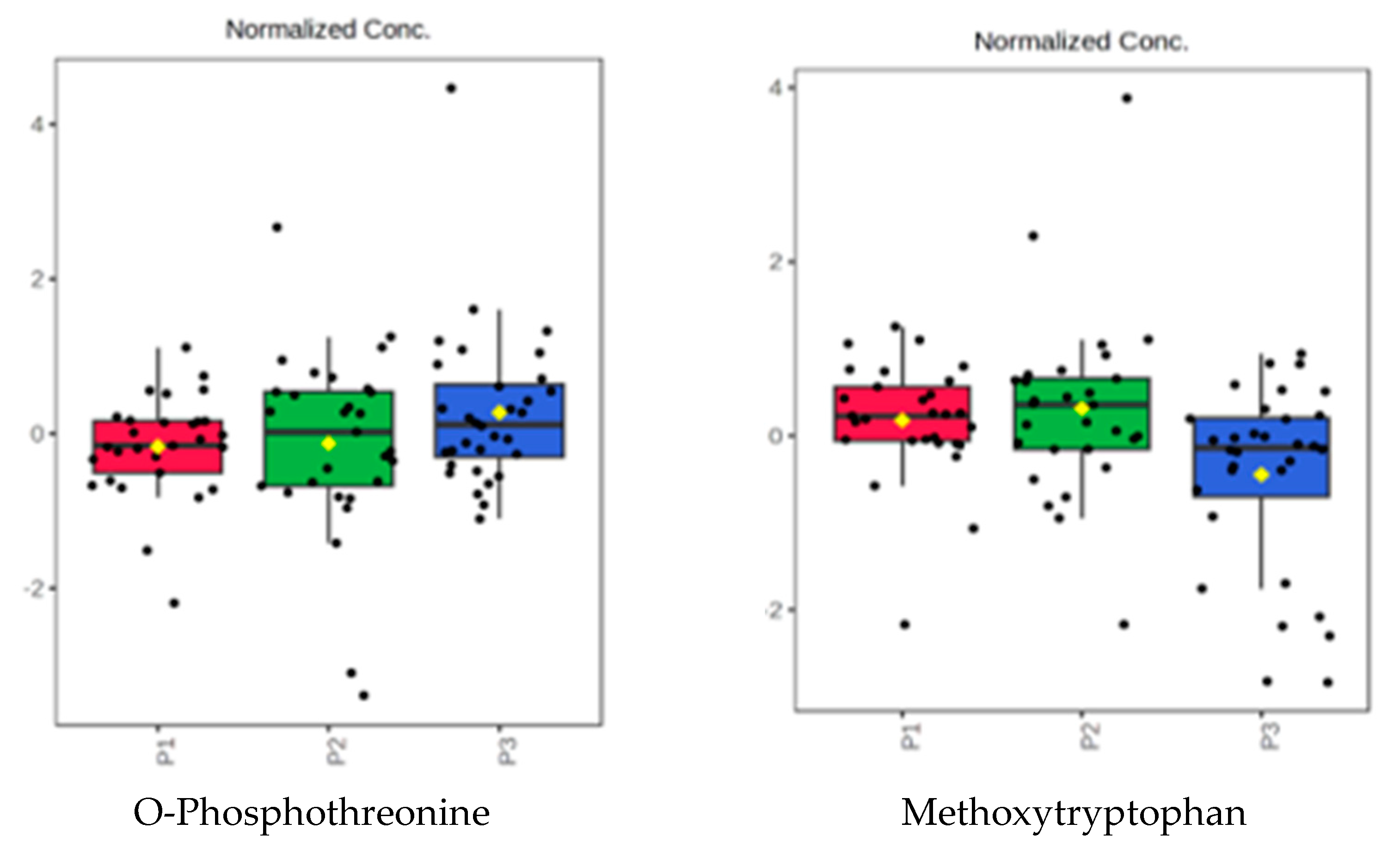
3.5. Variations of Significant Serum and Urine Metabolites at Different DKD Stages
4. Discussion
Impact of the Metabolites Studied at Glomerular and Tubular Level in Early DKD of Type 2 DM Patients
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- International Diabetes Federation. IDF Diabetes Atlas, 7th ed.; International Diabetes Federation: Brussels, Belgium, 2015. [Google Scholar]
- American Diabetes Association. 9. Microvascular Complications and Foot Care.Diabetes Care 2016, 39 (Suppl. S1), S72–S80.
- Lin, C.H.; Chang, Y.C.; Chuang, L.M. Early detection of diabetic kidney disease: Present limitations and future perspectives. World J. Diabetes 2016, 7, 290–301. [Google Scholar] [CrossRef]
- Vlad, A.; Vlad, M.; Petrica, L.; Ursoniu, S.; Gadalean, F.; Popescu, R.; Vlad, D.; Dumitrascu, V.; Gluhovschi, G.; Gluhovschi, C.; et al. Therapy with atorvastatin versus rosuvastatin reduces urinary podocytes, podocyte-associated molecules, and proximal tubule dysfunction biomarkers in patients with type 2 diabetes mellitus: A pilot study. Ren. Fail. 2017, 39, 112–119. [Google Scholar] [CrossRef] [PubMed]
- Hasegawa, S.; Jao, T.M.; Inagi, R. Dietary Metabolites and Chronic Kidney Disease. Nutrients 2017, 9, 358. [Google Scholar] [CrossRef] [PubMed]
- Sas, K.M.; Kayampilly, P.; Byun, J.; Nair, V.; Hinder, L.M.; Hur, J.; Zhang, H.; Lin, C.; Qi, N.R.; Michailidis, G.; et al. Tissue-specific metabolic reprogramming drives nutrient flux in diabetic complications. JCI Insight 2016, 1, e86976. [Google Scholar] [CrossRef] [PubMed]
- You, Y.H.; Quach, T.; Saito, R.; Pham, J.; Sharma, K. Metabolomics Reveals a Key Role for Fumarate in Mediating the Effects of NADPH Oxidase 4 in Diabetic Kidney Disease. J. Am. Soc. Nephrol. 2016, 27, 466–481. [Google Scholar] [CrossRef]
- Hasegawa, S.; Tanaka, T.; Saito, T.; Fukui, K.; Wakashima, T.; Susaki, E.A.; Ueda, H.R.; Nangaku, M. The oral hypoxia-inducible factor prolyl hydroxylase inhibitor enarodustat counteracts alterations in renal energy metabolism in the early stages of diabetic kidney disease. Kidney Int. 2020, 97, 934–950. [Google Scholar] [CrossRef]
- Rosenberger, C.; Khamaisi, M.; Abassi, Z.; Shilo, V.; Weksler-Zangen, S.; Goldfarb, M.; Shina, A.; Zibertrest, F.; Eckardt, K.U.; Rosen, S.; et al. Adaptation to hypoxia in the diabetic rat kidney. Kidney Int. 2008, 73, 34–42. [Google Scholar] [CrossRef]
- Yu, T.; Robotham, J.L.; Yoon, Y. Increased production of reactive oxygen species in hyperglycemic conditions requires dynamic change of mitochondrial morphology. Proc. Natl. Acad. Sci. USA 2006, 103, 2653–2658. [Google Scholar] [CrossRef]
- Inagi, R.; Ishimoto, Y.; Nangaku, M. Proteostasis in endoplasmic reticulum—New mechanisms in kidney disease. Nat. Rev. Nephrol. 2014, 10, 369–378. [Google Scholar] [CrossRef]
- Inagi, R.; Nangaku, M.; Onogi, H.; Ueyama, H.; Kitao, Y.; Nakazato, K.; Ogawa, S.; Kurokawa, K.; Couser, W.G.; Miyata, T. Involvement of endoplasmic reticulum (ER) stress in podocyte injury induced by excessive protein accumulation. Kidney Int. 2005, 68, 2639–2650. [Google Scholar] [CrossRef] [PubMed]
- Inagi, R.; Kumagai, T.; Nishi, H.; Kawakami, T.; Miyata, T.; Fujita, T.; Nangaku, M. Preconditioning with Endoplasmic Reticulum Stress Ameliorates Mesangioproliferative Glomerulonephritis. J. Am. Soc. Nephrol. 2008, 19, 915–922. [Google Scholar] [CrossRef] [PubMed]
- Darshi, M.; Van Espen, B.; Sharma, K. Metabolomics in Diabetic Kidney Disease: Unraveling the Biochemistry of a Silent Killer. Am. J. Nephrol. 2016, 44, 92–103. [Google Scholar] [CrossRef] [PubMed]
- Chen, D.Q.; Cao, G.; Chen, H.; Argyopoulos, C.P.; Yu, H.; Su, W.; Chen, L.; Samuels, D.C.; Zhuang, S.; Bayliss, G.P.; et al. Identification of serum metabolites associating with chronic kidney disease progression and anti-fibrotic effect of 5-methoxytryptophan. Nat. Commun. 2019, 10, 1476. [Google Scholar] [CrossRef]
- Wu, M.H.; Lin, C.N.; Chiu, D.T.; Chen, S.T. Kynurenine/Tryptophan Ratio Predicts Angiotensin Receptor Blocker Responsiveness in Patients with Diabetic Kidney Disease. Diagnostics 2020, 10, 207. [Google Scholar] [CrossRef]
- Chesney, R.W.; Han, X.; Patters, A.B. Taurine and the renal system. J. Biomed. Sci. 2010, 17 (Suppl. S1), S4. [Google Scholar] [CrossRef]
- Baliou, S.; Adamaki, M.; Ioannou, P.; Pappa, A.; Panayiotidis, M.I.; Christodoulou, I.; Spandidos, D.A.; Kyriakopoulos, A.M.; Zoumpourlis, V. Ameliorative effect of taurine against diabetes and renal-associated disorders (Review). Med. Int. 2021, 1, 3. [Google Scholar] [CrossRef]
- Fang, Q.; Liu, N.; Zheng, B.; Guo, F.; Zeng, X.; Huang, X.; Ouyang, D. Roles of Gut Microbial Metabolites in Diabetic Kidney Disease. Front. Endocrinol. 2021, 12, 636175. [Google Scholar] [CrossRef]
- Sharma, K.; Karl, B.; Mathew, A.; Gangoiti, J.; Wassel, C.; Saito, R.; Pu, M.; Sharma, S.; You, Y.H.; Wang, L.; et al. Metabolomics reveals signature of mitochondrial dysfunction in diabetic kidney disease. J. Am. Soc. Nephrol. 2013, 24, 1901–1912. [Google Scholar] [CrossRef]
- Zobel, E.H.; von Scholten, B.J.; Reinhard, H.; Persson, F.; Teerlink, T.; Hansen, T.W.; Parving, H.H.; Jacobsen, P.K.; Rossing, P. Symmetric and asymmetric dimethylarginine as risk markers of cardiovascular disease, all-cause mortality and deterioration in kidney function in persons with type 2 diabetes and microalbuminuria. Cardiovasc. Diabetol. 2017, 16, 88. [Google Scholar] [CrossRef]
- Balint, L.; Socaciu, C.; Socaciu, I.A.; Vlad, A.; Gadalean, F.; Bob, F.; Milas, O.; Cretu, O.M.; Simulescu-Suteanu, A.; Glavan, M.; et al. Metabolite Profiling of the Gut–Renal–Cerebral Axis Reveals a Particular Pattern in Early Diabetic Kidney Disease in T2DM Patients. IJMS 2023, 24, 6212. [Google Scholar] [CrossRef] [PubMed]
- Glavan, M.; Socaciu, C.; Socaciu, I.A.; Vlad, A.; Gadalean, F.; Cretu, O.M.; Vlad, A.; Muntean, D.M.; Bob, F.; Milas, O.; et al. Untargeted Metabolomics by Ultra-High-Performance Liquid Chromatography Coupled with Electrospray Ionization-Quadrupole-Time of Flight-Mass Spectrometry Analysis Identifies a Specific Metabolomic Profile in Patients with Early Chronic Kidney Disease. Biomedicines 2023, 11, 1057. [Google Scholar] [CrossRef] [PubMed]
- Mu, X.; Yang, M.; Ling, P.; Wu, A.; Zhou, H.; Jiang, J. Acylcarnitines: Can They Be Biomarkers of Diabetic Nephropathy? Diabetes Metab. Syndr. Obes. 2022, 15, 247–256. [Google Scholar] [CrossRef]
- Roointan, A.; Gheisari, Y.; Hudkins, K.L.; Gholaminejad, A. Non-invasive metabolic biomarkers for early diagnosis of diabetic nephropathy: Meta-analysis of profiling metabolomics studies. Nutr. Metab. Cardiovasc. Dis. 2021, 31, 2253–2272. [Google Scholar] [CrossRef] [PubMed]
- Hirakawa, Y.; Yoshioka, K.; Kojima, K.; Yamashita, Y.; Shibahara, T.; Wada, T.; Nangaku, M.; Inagi, R. Potential progression biomarkers of diabetic kidney disease determined using comprehensive machine learning analysis of non-targeted metabolomics. Sci. Rep. 2022, 12, 16287. [Google Scholar] [CrossRef] [PubMed]
- Lee, H.; Jang, B.H.; Yoo, M.G.; Park, S.I.; Lee, H.J. Amino Acid Metabolites Associated with Chronic Kidney Disease: An Eight-Year Follow-Up Korean Epidemiology Study. Biomedicines 2020, 8, 222. [Google Scholar] [CrossRef]
- Wu, T.; Qiao, S.; Shi, C.; Wang, S.; Ji, G. Metabolomics window into diabetic Complications. J. Diabetes Investig. 2018, 9, 244–255. [Google Scholar] [CrossRef]
- Jin, Q.; Ma, R.C.W. Metabolomics in Diabetes and Diabetic Complications: Insights from Epidemiological Studies. Cells 2021, 10, 2832. [Google Scholar] [CrossRef]
- Shao, M.; Lu, H.; Yang, M.; Liu, Y.; Yin, P.; Li, G.; Wang, Y.; Chen, L.; Chen, Q.; Zhao, C.; et al. Serum and urine metabolomics reveal potential biomarkers of T2DM patients with nephropathy. Ann. Transl. Med. 2020, 8, 199. [Google Scholar] [CrossRef]
- Cordero-Pérez, P.; Sánchez-Martínez, C.; García-Hernández, P.A.; Saucedo, A.L. Metabolomics of the diabetic nephropathy: Behind the fingerprint of development and progression indicators. Nefrología 2020, 40, 585–596. [Google Scholar] [CrossRef]
- Hsu, C.N.; Tain, Y.L. Developmental Programming and Reprogramming of Hypertension and Kidney Disease: Impact of Tryptophan Metabolism. Int. J. Mol. Sci. 2020, 21, 8705. [Google Scholar] [CrossRef]
- Zhu, H.; Bai, M.; Xie, X.; Wang, J.; Weng, C.; Dai, H.; Chen, J.; Han, F.; Lin, W. Impaired Amino Acid Metabolism and Its Correlation with Diabetic Kidney Disease Progression in Type 2 Diabetes Mellitus. Nutrients 2022, 14, 3345. [Google Scholar] [CrossRef] [PubMed]
- Peng, X.; Wang, X.; Shao, X.; Wang, Y.; Feng, S.; Wang, C.; Ye, C.; Chen, J.; Jiang, H. Serum Metabolomics Benefits Discrimination Kidney Disease Development in Type 2 Diabetes Patients. Front. Med. 2022, 9, 819311. [Google Scholar] [CrossRef] [PubMed]
- Zhou, C.; Zhang, Q.; Lu, L.; Wang, J.; Liu, D.; Liu, Z. Metabolomic Profiling of Amino Acids in Human Plasma Distinguishes Diabetic Kidney Disease from Type 2 Diabetes Mellitus. Front. Med. 2021, 8, 765873. [Google Scholar] [CrossRef]
- Luo, H.-H.; Li, J.; Feng, X.-F.; Sun, X.Y.; Li, J.; Yang, X.; Fang, Z.Z. Plasma phenylalanine and tyrosine and their interactions with diabetic nephropathy for risk of diabetic retinopathy in type 2 diabetes. BMJ Open Diabetes Res. Care 2020, 8, e000877. [Google Scholar] [CrossRef] [PubMed]
- Van der Kloet, F.M.; Tempels, F.W.A.; Ismail, N.; Van der Heijden, R.; Kasper, P.T.; Rojas-Cherto, M.; Van Doorn, R.; Spijksma, G.; Koek, M.; Van Der Greef, J. Discovery of early-stage biomarkers for diabetic kidney disease using ms-based metabolomics (FinnDiane study). Metabolomic 2012, 8, 109–119. [Google Scholar] [CrossRef]
- Debnath, S.; Velagapudi, C.; Redus, L.; Thameem, F.; Kasinath, B.; Hura, C.E.; Lorenzo, C.; Abboud, H.E.; O’Connor, J.C. Tryptophan Metabolism in Patients with Chronic Kidney Disease Secondary to Type 2 Diabetes: Relationship to Inflammatory Markers. Int. J. Tryptophan Res. 2017, 10, 1178646917694600. [Google Scholar] [CrossRef]
- Chou, C.A.; Lin, C.N.; Tsun-Yee Chiu, D.; Chen, I.W.; Chen, S.T. Tryptophan as a surrogate prognostic marker for diabetic nephropathy. J. Diabetes Investig. 2018, 9, 366–374. [Google Scholar] [CrossRef]
- Berg, A.H.; Drechsler, C.; Wenger, J.; Buccafusca, R.; Hod, T.; Kalim, S.; Ramma, W.; Parikh, S.M.; Steen, H.; Friedman, D.J.; et al. C arbamylation of serum albumin as a risk factor for mortality in patients with kidney failure. Sci. Transl. Med. 2013, 5, 175ra29. [Google Scholar] [CrossRef]
- Posada-Ayala, M.; Zubiri, I.; Martin-Lorenzo, M.; Sanz-Maroto, A.; Molero, D.; Gonzalez-Calero, L.; Fernandez-Fernandez, B.; de la Cuesta, F.; Laborde, C.M.; Barderas, M.G.; et al. Identification of a urine metabolomic signature in patients with advanced-stage chronic kidney disease. Kidney Int. 2014, 85, 103–111. [Google Scholar] [CrossRef]
- Goek, O.N.; Prehn, C.; Sekula, P.; Römisch-Margl, W.; Döring, A.; Gieger, C.; Heier, M.; Koenig, W.; Wang-Sattler, R.; Illig, T.; et al. Metabolites associate with kidney function decline and incidentchronic kidney disease in the general population. Nephrol. Dial. Transplant. 2013, 28, 2131–2138. [Google Scholar] [CrossRef] [PubMed]
- Rhee, E.P.; Clish, C.B.; Ghorbani, A.; Larson, M.G.; Elmariah, S.; McCabe, E.; Yang, Q.; Cheng, S.; Pierce, K.; Deik, A.; et al. A Combined Epidemiologic and Metabolomic Approach Improves CKD Prediction. J. Am. Soc. Nephrol. 2013, 24, 1330–1338. [Google Scholar] [CrossRef] [PubMed]
- Qi, S.; Ouyang, X.; Wang, L.; Peng, W.; Wen, J.; Dai, Y. A pilot metabolic profiling study in serum of patients with chronic kidney disease based on (1) H-NMR-spectroscopy. Clin. Transl. Sci. 2012, 5, 379–385. [Google Scholar] [CrossRef] [PubMed]
- Takashi, I.; Schaffer, S.W.; Azuma, J. The potential usefulness of taurine on diabetes mellitus and its complications. Amino Acids 2012, 42, 1529–1539. [Google Scholar] [CrossRef]
- Hayes, K.C.; Crey, R.E.; Schmidt, S.Y. Retinal degeneration associated with taurine deficiency in the cat. Science 1975, 188, 949–951. [Google Scholar] [CrossRef]
- Pion, P.D.; Kittleson, M.D.; Rogers, Q.R.; Morris, J.G. Myocardial failure in cats associated with low plasma taurine: A reversible cardiomyopathy. Science 1987, 237, 764–768. [Google Scholar] [CrossRef]
- Wang-Sattler, R.; Yu, Z.; Herder, C.; Messias, A.C.; Floegel, A.; He, Y.; Heim, K.; Campillos, M.; Holzapfel, C.; Thorand, B.; et al. Novel biomarkers for pre-diabetes identified by metabolomics. Mol. Syst. Biol. 2012, 8, 615. [Google Scholar] [CrossRef]
- Lee, S.Y.; Choi, M.E. Urinary biomarkers for early diabetic nephropathy: Beyond albuminuria. Pediatr. Nephrol. 2015, 30, 1063–1075. [Google Scholar] [CrossRef]
- Mor, A.; Kalaska, B.; Pawlak, D. Kynurenine Pathway in Chronic Kidney Disease: What’s Old, What’s New, and What’s Next? Int. J. Tryptophan Res. 2020, 13, 1178646920954882. [Google Scholar] [CrossRef]
- Oshima, M.; Shimizu, M.; Yamanouchi, M.; Toyama, T.; Hara, A.; Furuichi, K.; Wada, T. Trajectories of kidney function in diabetes: A clinicopathological update. Nat. Rev. Nephrol. 2021, 17, 740–750. [Google Scholar] [CrossRef]
- Fukuda, T.; Bouchi, R.; Asakawa, M.; Takeuchi, T.; Shiba, K.; Tsujimoto, K.; Komiya, C.; Yoshimoto, T.; Ogawa, Y.; Yamada, T. Sarcopenic obesity is associated with a faster decline in renal function in people with type 2 diabetes. Diabet. Med. 2020, 37, 105–113. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| P1 | P2 | P3 | C | |
|---|---|---|---|---|
| Number of participants | 30 | 30 | 30 | 20 |
| Age (y) | 68.41 ± 4.98 | 68.65 ± 4.91 | 68.84 ± 4.98 | 55.85 ± 7.25 |
| DM duration (y) | 9.6 ± 3.99 | 9.7 ± 3.99 | 12.78 ± 3.35 | 0 |
| Serum creatinine (mg/dL) | 0.82 ± 0.18 | 0.93 ± 0.21 | 1.07 ± 0.32 | 0.73 ± 0.08 |
| eGFR (mL/min/1.73 m2) | 90.42 ± 18.10 | 89.70 ± 18.19 | 77.85 ± 19.38 | 97.93 ± 11.71 |
| UACR (mg/g) | 7.38 ± 3.22 | 45.42 ± 57.08 | 319.86 ± 585.80 | 5 ± 0.23 |
| HbA1c (%) | 5 ± 0.23 | 6.42 ± 1.29 | 7.15 ± 1.60 | 4.98 ± 0.23 |
| Body weight (kg) | 79.06 ± 4.90 | 84.86 ± 3.9 | 86.06 ± 4.46 | 78.05 ± 5.47 |
| Male/female (number) | 17/13 | 16/14 | 20/10 | 12/8 |
| Molecules | Fold Change (FC) | log2(FC) | Significance P vs. C | VIP Scores | MDA |
|---|---|---|---|---|---|
| Methoxytryptophan | 184.460 | 7.527 | D | 1.492 | 0.02 |
| N-Acetylserine | 23.102 | 4.530 | D | 1.072 | 0.0002 |
| Homoproline | 21.654 | 4.437 | D | 1.245 | 0.002 |
| Taurine | 19.588 | 4.292 | D | 1.360 | 0.02 |
| Serotonin sulfate | 11.395 | 3.510 | D | 1.464 | 0.02 |
| Cystine | 4.663 | 2.221 | D | 1.453 | 0.03 |
| O-Phosphothreonine | 4.030 | 2.011 | D | 1.398 | 0.01 |
| L-Tryptophan | 3.030 | 1.011 | D | 1.114 | 0.001 |
| Creatinine | 2.750 | 1.460 | D | 0.955 | 0.002 |
| Aspartic acid | 2.294 | 1.198 | D | 0.907 | 5.41 × 10−5 |
| L-Cysteine | 2.018 | 1.013 | D | 1.160 | 0.0007 |
| Kynurenic acid | 0.675 | 0.87 | D | 1.292 | 0.02 |
| Ornitine | 0.490 | −1.028 | I | 1.212 | 0.001 |
| Spermidine | 0.449 | −1.155 | I | 0.896 | 0.001 |
| Ketoleucine | 0.316 | −1.660 | I | 1.129 | 0.002 |
| Dimethylarginine | 0.245 | −2.028 | I | 1.126 | 0.003 |
| Threonine | 0.139 | −2.845 | I | 1.040 | 0.0003 |
| 5-Hydroxy lysine | 0.122 | −3.030 | I | 1.439 | 0.01 |
| Proline | 0.086 | −3.544 | I | 0.910 | 0.02 |
| Tiglylglycine | 0.066 | −3.911 | I | 1.499 | 0.02 |
| Leucine | 0.054 | −4.213 | I | 0.989 | 0.002 |
| Tyrosine | 0.039 | −2.811 | I | 1.156 | 0.009 |
| Valine | 0.031 | −4.995 | I | 1.242 | 0.04 |
| Molecule | AUC | p-Value | Molecule | AUC | p-Value |
|---|---|---|---|---|---|
| Proline | 1 | 6.59 × 10−12 | Ornitine | 0.985 | 1.18 × 1025 |
| Valine | 1 | 1.50 × 10−24 | Ketoleucine | 0.978 | 3.71 × 10−26 |
| Taurine | 1 | 2.13 × 10−35 | Phenylalanine | 0.977 | 2.59 × 10−9 |
| Tiglylglycine | 1 | 2.22 × 10−73 | Spermidine | 0.964 | 3.77 × 10−11 |
| Tyrosine | 1 | 1.65 × 10−23 | Lysine | 0.954 | 5.87 × 10−10 |
| Kynurenic acid | 1 | 1.25 × 10−27 | Dimethylarginine | 0.951 | 3.71 × 10−18 |
| Methoxytryptophan | 1 | 1.61 × 10−64 | Creatinine | 0.938 | 9.96 × 10−13 |
| Cystine | 1 | 1.07 × 10−49 | Uric acid | 0.937 | 2.84 × 10−8 |
| Serotonin sulfate | 1 | 5.23 × 10−51 | Aspartic acid | 0.923 | 4.54 × 10−11 |
| L-Tryptophan | 0.993 | 3.72 × 10−19 | Homoproline | 0.918 | 7.90 × 10−26 |
| 5-Hydroxy lysine | 0.992 | 9.44 × 10−49 | Threonine | 0.9 | 1.30 × 10−14 |
| O-Phosphothreonine | 0.989 | 4.41 × 10−43 |
| Molecule | f-Value | p-Value | VIP Score | MDA | Fisher’s LSD |
|---|---|---|---|---|---|
| Tiglylglycine | 486.67 | 8.31 × 10−62 | 1.605 | 0.04 | P1–C; P2–C; P3–C; P2–P1; P3–P1 |
| Methoxytryptophan | 373.98 | 3.26 × 10−56 | 1.448 | 0.05 | C–P1; C–P2; C–P3 |
| Serotonin sulfate | 257.95 | 1.51 × 10−48 | 1.417 | 0.01 | C–P1; C–P2; C–P3 |
| Cystine | 229.12 | 3.60 × 10−46 | 1.416 | 0.01 | C–P1; C–P2; C–P3 |
| 5-Hydroxy lysine | 220.71 | 1.99 × 10−45 | 1.490 | 0.01 | P1–C; P2–C; P3–C; P2–P1 |
| O-Phosphothreonine | 149.86 | 5.52 × 10−38 | 1.257 | 0.01 | C–P1; C–P2; C–P3 |
| Taurine | 111.25 | 1.29 × 10−32 | 1.333 | 0.01 | C–P1; C–P2; C–P3 |
| Kynurenic acid | 78.191 | 9.39 × 10−27 | 1.342 | 0.01 | C–P1; C–P2; C–P3 |
| Tyrosine | 75.927 | 2.72 × 10−26 | 1.584 | 0.04 | P1–C; P2–C; P3–C; P2–P1; P3–P1 |
| Homoproline | 61.627 | 3.85 × 10−23 | 1.206 | 0.0003 | C–P1; C–P2; C–P3 |
| Molecule | Fold Change | log2(FC) | Significance P vs. C | VIP | MDA |
|---|---|---|---|---|---|
| Histidine | 2.335 | 1.224 | D | 0.849 | 0.0006 |
| N1-Acetylspermidine | 2.322 | 1.215 | D | 1.345 | 0.002 |
| Hippuric acid | 2.261 | 1.177 | D | 0.977 | 0.0005 |
| Glutamine | 2.230 | 1.157 | D | 1.472 | 0.004 |
| Aspartic acid | 2.059 | 1.042 | D | 1.011 | 0.0005 |
| 5-Hydroxy lysine | 2.020 | 1.014 | D | 1.906 | 0.03 |
| Oleoyl glycine | 1.005 | 0.924 | D | 1.537 | 0.03 |
| Methoxytryptophan | 0.460 | −1.120 | I | 1.613 | 0.008 |
| Serotonin sulfate | 0.460 | −1.121 | I | 2.170 | 0.05 |
| Threonine | 0.440 | −1.185 | I | 0.905 | 0.006 |
| O-Phosphothreonine | 0.405 | −1.303 | I | 1.968 | 0.03 |
| L-Tryptophan | 0.360 | −1.070 | I | 1.005 | 0.0003 |
| Dimethylarginine | 0.090 | −3.472 | I | 0.464 | 0.001 |
| Name | AUC | p-Value | Name | AUC | p-Value |
|---|---|---|---|---|---|
| Serotonin sulfate | 0.990 | 2.34 × 10−20 | L-Tryptophan | 0.778 | 9.30 × 10−5 |
| O-Phosphothreonine | 0.963 | 1.33 × 10−15 | N1-Acetylspermidine | 0.756 | 2.92 × 10−5 |
| Methoxytryptophan | 0.933 | 9.15 × 10−12 | Homoproline | 0.739 | 1.49 × 10−4 |
| Cysteine-S-sulfate | 0.912 | 8.55 × 10−6 | Hippuric acid | 0.728 | 0.0016 |
| Leucine | 0.911 | 0.036 | Isovalerylglycine | 0.704 | 0.3170 |
| Oleoyl glycine | 0.889 | 5.31 × 10−6 | L-Cysteine | 0.685 | 3.48 × 10−5 |
| Ketoleucine | 0.859 | 1.31 × 10−6 | N-Acetylserine | 0.683 | 0.0238 |
| 5-Hydroxy lysine | 0.839 | 1.04 × 10−12 | Aspartic acid | 0.675 | 0.0032 |
| Threonine | 0.780 | 0.0021 | Dimethylarginine | 0.667 | 0.1142 |
| f-Value | p-Value | VIP Score | MDA | Fisher’s LSD | |
|---|---|---|---|---|---|
| Serotonin sulfate | 37.141 | 1.74 × 10−16 | 2.243 | 0.03 | P1-C; P2-C; P3-C |
| O-Phosphothreonine | 27.236 | 3.88 × 10−13 | 2.269 | 0.03 | P1-C; P2-C; P3-C |
| 5-Hydroxy lysine | 22.646 | 2.09 × 10−11 | 1.927 | 0.02 | C-P1; C-P2; C-P3 |
| Methoxytryptophan | 18.767 | 7.75 × 10−10 | 0.987 | 0.01 | P1-C; P2-C; P3-C; P1-P3; P2-P3 |
| Oleoyl glycine | 13.243 | 2.08 × 10−7 | 1.141 | 0.03 | C-P1; C-P2; C-P3 |
| Glutamine | 10.961 | 2.50 × 10−6 | 1.767 | 0.002 | C-P1; C-P2; C-P3 |
| N1-Acetylspermidine | 10.160 | 6.14 × 10−6 | 1.767 | 0.002 | C-P1; C-P2; C-P3 |
| Methionine | 7.638 | 0.0001 | 1.573 | 0.003 | C-P1; C-P2; C-P3 |
| Uric acid | 7.587 | 0.0001 | 1.403 | 0.003 | P1-C; P1-P2; P1-P3 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mogos, M.; Socaciu, C.; Socaciu, A.I.; Vlad, A.; Gadalean, F.; Bob, F.; Milas, O.; Cretu, O.M.; Suteanu-Simulescu, A.; Glavan, M.; et al. Metabolomic Investigation of Blood and Urinary Amino Acids and Derivatives in Patients with Type 2 Diabetes Mellitus and Early Diabetic Kidney Disease. Biomedicines 2023, 11, 1527. https://doi.org/10.3390/biomedicines11061527
Mogos M, Socaciu C, Socaciu AI, Vlad A, Gadalean F, Bob F, Milas O, Cretu OM, Suteanu-Simulescu A, Glavan M, et al. Metabolomic Investigation of Blood and Urinary Amino Acids and Derivatives in Patients with Type 2 Diabetes Mellitus and Early Diabetic Kidney Disease. Biomedicines. 2023; 11(6):1527. https://doi.org/10.3390/biomedicines11061527
Chicago/Turabian StyleMogos, Maria, Carmen Socaciu, Andreea Iulia Socaciu, Adrian Vlad, Florica Gadalean, Flaviu Bob, Oana Milas, Octavian Marius Cretu, Anca Suteanu-Simulescu, Mihaela Glavan, and et al. 2023. "Metabolomic Investigation of Blood and Urinary Amino Acids and Derivatives in Patients with Type 2 Diabetes Mellitus and Early Diabetic Kidney Disease" Biomedicines 11, no. 6: 1527. https://doi.org/10.3390/biomedicines11061527