
Continuous Glucose Monitoring as an Additional Tool in Early Cystic Fibrosis-Related Diabetes Monitoring and in Evaluation of Short-Term Sitagliptin Response

 , , and
, , and
Abstract
1. Introduction
2. Materials and Methods
2.1. Oral Glucose Tolerance Test
2.2. Continuous Subcutaneous Glucose Monitoring
2.3. Sitagliptin Therapy
2.4. Statistical Analysis
2.5. Ethics
3. Results
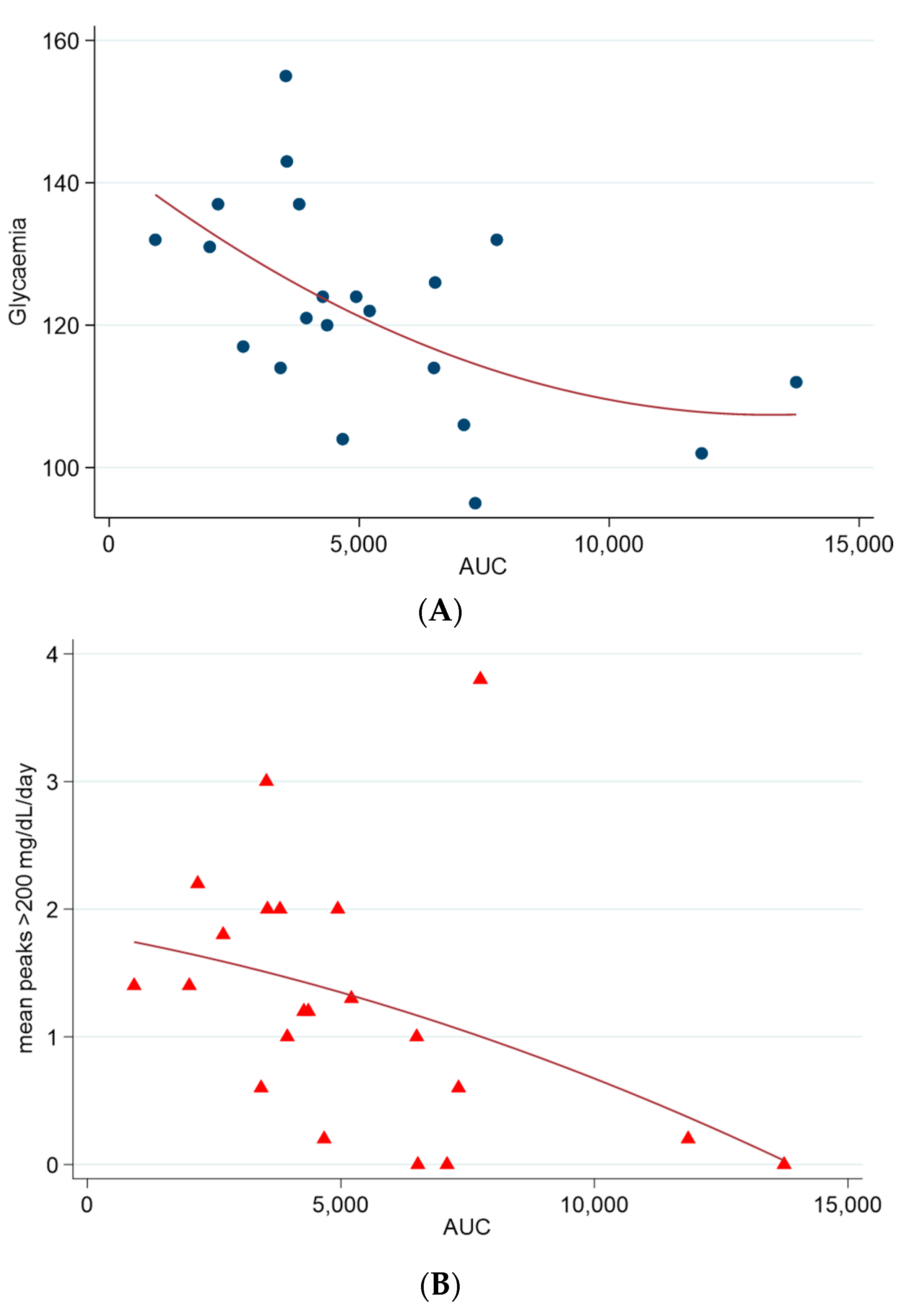
3.1. Basal CGM Results
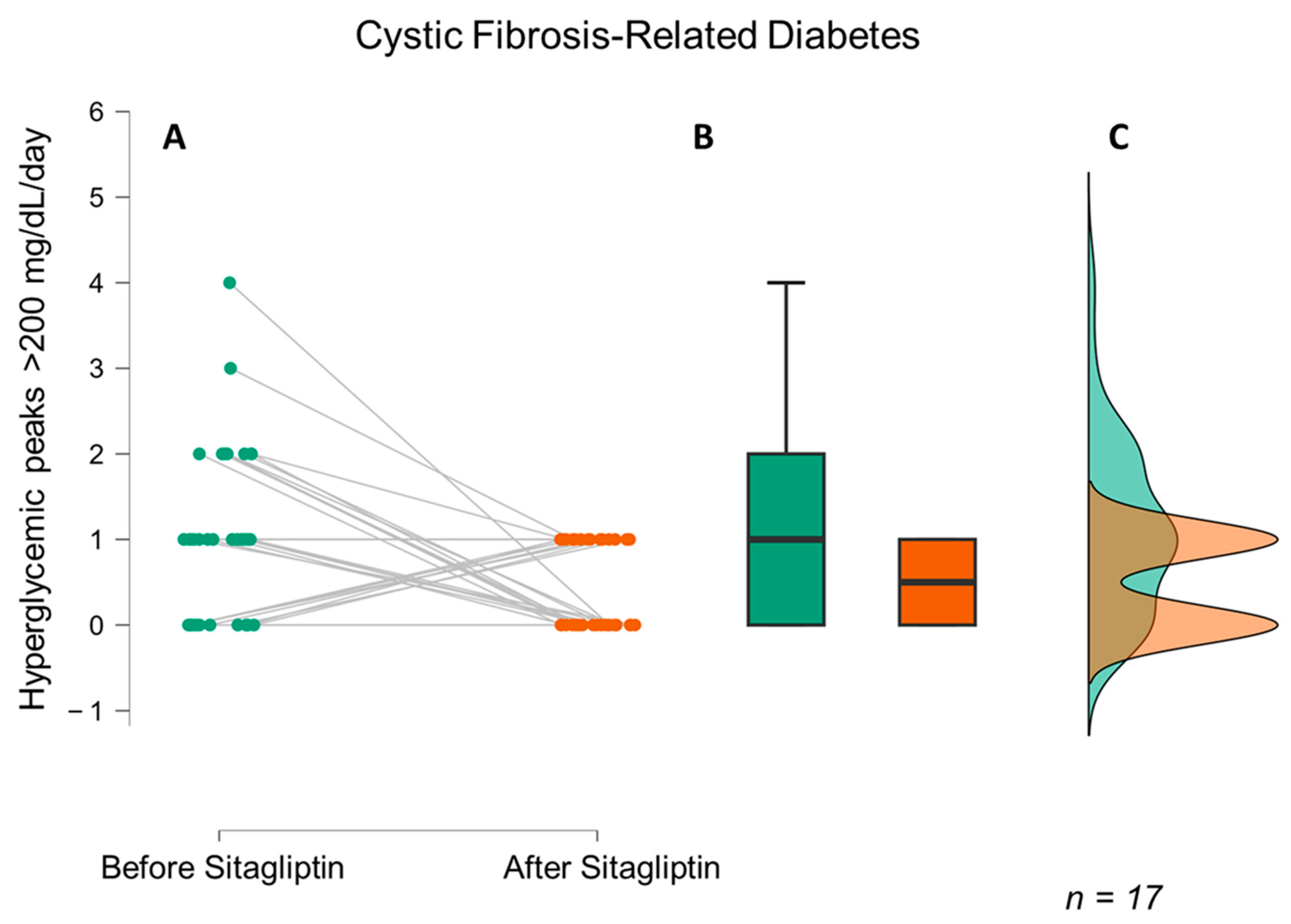
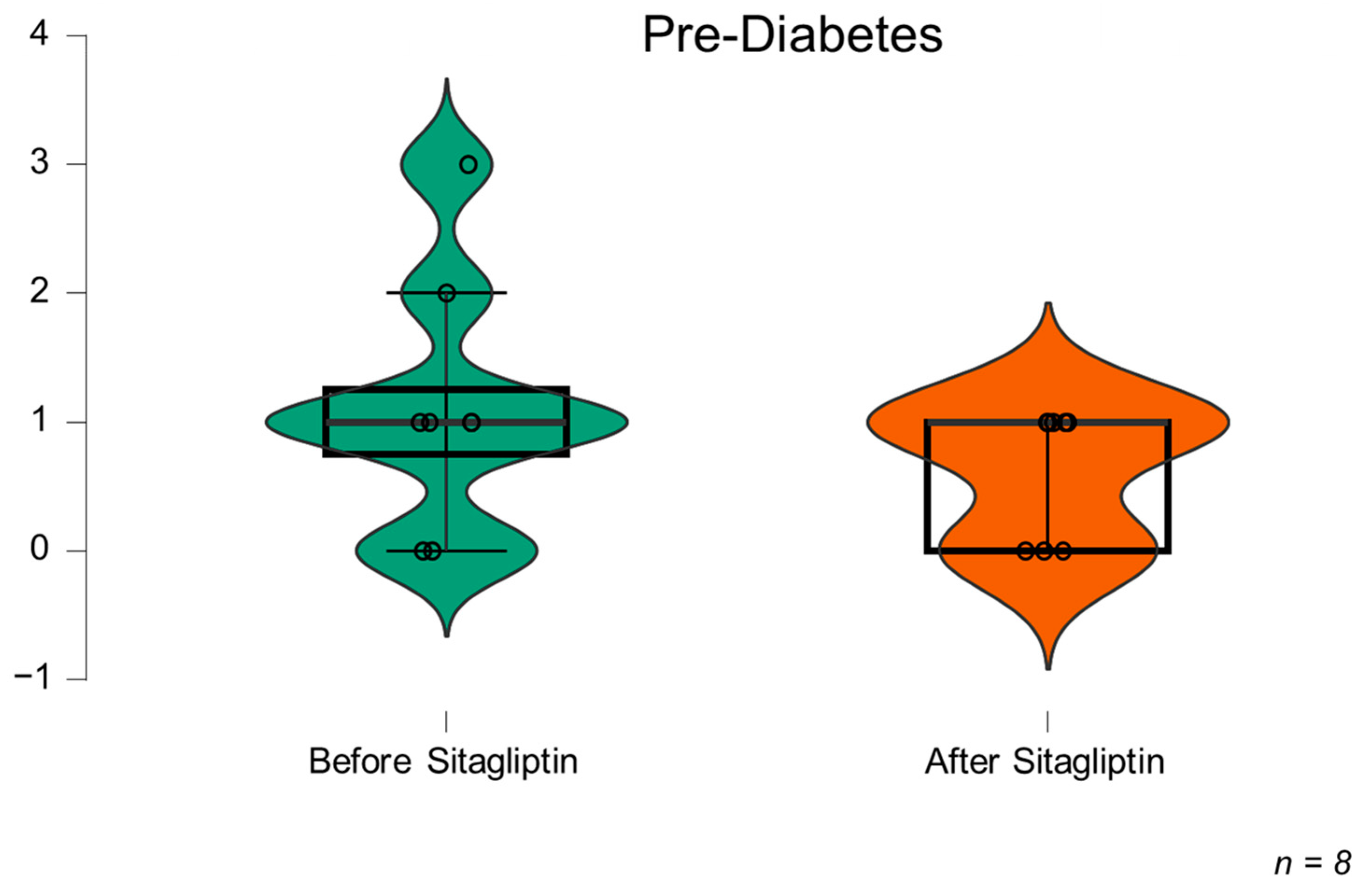
3.2. Results of CGM during Sitagliptin Therapy
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- FitzSimmons, S.C. The changing epidemiology of cystic fibrosis. J. Pediatr. 1993, 122, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Moran, A.; Pillay, K.; Becker, D.; Granados, A.; Hameed, S.; Acerini, C.L. ISPAD Clinical Practice Consensus Guidelines 2018: Management of cystic fibrosis-related diabetes in children and adolescents. Pediatr. Diabetes 2018, 19, 64–74. [Google Scholar] [CrossRef] [PubMed]
- Weiss, L.; Reix, P.; Mosnier-Pudar, H.; Ronsin, O.; Beltrand, J.; Reynaud, Q.; Mely, L.; Burgel, P.-R.; Stremler, N.; Rakotoarisoa, L.; et al. Screening strategies for glucose tolerance abnormalities and diabetes in people with cystic fibrosis. Diabetes Metab. 2023, 49, 101444. [Google Scholar] [CrossRef] [PubMed]
- Moran, A.; Brunzell, C.; Cohen, R.C.; Katz, M.; Marshall, B.C.; Onady, G.; Robinson, K.A.; Sabadosa, K.A.; Stecenko, A.; Slovis, B.; et al. Clinical Care Guidelines for Cystic Fibrosis–Related Diabetes. Diabetes Care 2010, 33, 2697–2708. [Google Scholar] [CrossRef]
- Tanner, K.T.; Daniel, R.M.; Bilton, D.; Simmonds, N.J.; Sharples, L.D.; Keogh, R.H. Mediation of the total effect of cystic fibrosis-related diabetes on mortality: A UK Cystic Fibrosis Registry cohort study. Diabetes Med. 2022, 39, e14958. [Google Scholar] [CrossRef]
- Ode, K.L.; Frohnert, B.; Laguna, T.; Phillips, J.; Holme, B.; Regelmann, W.; Thomas, W.; Moran, A. Oral glucose tolerance testing in children with cystic fibrosis. Pediatr. Diabetes 2010, 11, 487–492. [Google Scholar] [CrossRef]
- Lanng, S.; Thorsteinsson, B.; Nerup, J.; Koch, C. Influence of the development of diabetes mellitus on clinical status in patients with cystic fibrosis. Eur. J. Pediatr. 1992, 151, 684–687. [Google Scholar] [CrossRef]
- Rolon, M.; Benali, K.; Munck, A.; Navarro, J.; Clement, A.; Tubiana-Rufi, N.; Czernichow, P.; Polak, M. Cystic fibrosis-related diabetes mellitus: Clinical impact of prediabetes and effects of insulin therapy. Acta Paediatr. 2001, 90, 860–867. [Google Scholar]
- Potter, K.J.; Boudreau, V.; Shohoudi, A.; Mailhot, M.; Tremblay, F.; Lavoie, A.; Carricart, M.; Senior, P.A.; Rabasa-Lhoret, R. Influence of pre-diabetic and pancreatic exocrine states on pulmonary and nutritional status in adults with Cystic Fibrosis. J. Cyst. Fibros. 2021, 20, 803–809. [Google Scholar] [CrossRef]
- Milla, C.E.; Warwick, W.J.; Moran, A. Trends in Pulmonary Function in Patients with Cystic Fibrosis Correlate with the Degree of Glucose Intolerance at Baseline. Am. J. Respir. Crit. Care Med. 2000, 162, 891–895. [Google Scholar] [CrossRef]
- American Diabetes Association Professional Practice Committee. 2. Classification and Diagnosis of Diabetes: Standards of Medical Care in Diabetes—2022. Diabetes Care 2021, 45, S17–S38. [Google Scholar]
- Scheuing, N.; Holl, R.W.; Dockter, G.; Hermann, J.M.; Junge, S.; Koerner-Rettberg, C.; Naehrlich, L.; Smaczny, C.; Staab, D.; Thalhammer, G.; et al. High Variability in Oral Glucose Tolerance among 1128 Patients with Cystic Fibrosis: A Multicenter Screening Study. PLoS ONE 2014, 9, e112578. [Google Scholar] [CrossRef]
- Gilmour, J.A.; Sykes, J.; Etchells, E.; Tullis, E. Cystic Fibrosis-Related Diabetes Screening in Adults: A Gap Analysis and Evaluation of Accuracy of Glycated Hemoglobin Levels. Can. J. Diabetes 2018, 43, 13–18. [Google Scholar] [CrossRef]
- Darukhanavala, A.; Van Dessel, F.; Ho, J.; Hansen, M.; Kremer, T.; Alfego, D. Use of hemoglobin A1c to identify dysglycemia in cystic fibrosis. PLoS ONE 2021, 16, e0250036. [Google Scholar] [CrossRef]
- Chan, C.L.; Vigers, T.; Pyle, L.; Zeitler, P.S.; Sagel, S.D.; Nadeau, K.J. Continuous glucose monitoring abnormalities in cystic fibrosis youth correlate with pulmonary function decline. J. Cyst. Fibros. 2018, 17, 783–790. [Google Scholar] [CrossRef]
- Gojsina, B.; Minic, P.; Todorovic, S.; Soldatovic, I.; Sovtic, A. Continuous Glucose Monitoring as a Valuable Tool in the Early Detection of Diabetes Related to Cystic Fibrosis. Front. Pediatr. 2021, 9, 659728. [Google Scholar] [CrossRef]
- Frost, F.; Jones, G.H.; Dyce, P.; Jackson, V.; Nazareth, D.; Walshaw, M.J. Loss of incretin effect contributes to postprandial hyperglycaemia in cystic fibrosis-related diabetes. Diabet. Med. 2019, 36, 1367–1374. [Google Scholar] [CrossRef]
- Ismail, H.M. Potential Role for the Use of Gliptins in Cystic Fibrosis-related Diabetes. J. Clin. Endocrinol. Metab. 2021, 106, e4786–e4788. [Google Scholar] [CrossRef]
- Dobson, L.; Sheldon, C.D.; Hattersley, A.T. Validation of Interstitial Fluid Continuous Glucose Monitoring in Cystic Fibrosis. Diabetes Care 2003, 26, 1940–1941. [Google Scholar] [CrossRef]
- O’Riordan, S.M.P.; Hindmarsh, P.; Hill, N.R.; Matthews, D.R.; George, S.; Greally, P.; Canny, G.; Slattery, D.; Murphy, N.; Roche, E.; et al. Validation of Continuous Glucose Monitoring in Children and Adolescents with Cystic Fibrosis: A prospective cohort study. Diabetes Care 2009, 32, 1020–1022. [Google Scholar] [CrossRef]
- Hameed, S.; Morton, J.R.; Jaffé, A.; Field, P.I.; Belessis, Y.; Yoong, T.; Katz, T.; Verge, C.F. Early Glucose Abnormalities in Cystic Fibrosis Are Preceded by Poor Weight Gain. Diabetes Care 2009, 33, 221–226. [Google Scholar] [CrossRef] [PubMed]
- Leclercq, A.; Gauthier, B.; Rosner, V.; Weiss, L.; Moreau, F.; Constantinescu, A.A.; Kessler, R. Early assessment of glucose abnormalities during continuous glucose monitoring associated with lung function impairment in cystic fibrosis patients. J. Cyst. Fibros. 2014, 13, 478–484. [Google Scholar] [CrossRef]
- Schiaffini, R.; Brufani, C.; Russo, B.; Fintini, D.; Migliaccio, A.; Pecorelli, L.; Bizzarri, C.; Lucidi, V.; Cappa, M. Abnormal glucose tolerance in children with cystic fibrosis: The predictive role of continuous glucose monitoring system. Eur. J. Endocrinol. 2010, 162, 705–710. [Google Scholar] [CrossRef] [PubMed]
- Frost, F.; Dyce, P.; Nazareth, D.; Malone, V.; Walshaw, M.J. Continuous glucose monitoring guided insulin therapy is associated with improved clinical outcomes in cystic fibrosis-related diabetes. J. Cyst. Fibros. 2018, 17, 798–803. [Google Scholar] [CrossRef]
- Taylor-Cousar, J.L.; Janssen, J.S.; Wilson, A.; Clair, C.G.S.t.; Pickard, K.M.; Jones, M.C.; Brayshaw, S.J.; Chacon, C.S.; Barboa, C.M.; Sontag, M.K.; et al. Glucose > 200 mg/dL during Continuous Glucose Monitoring Identifies Adult Patients at Risk for Development of Cystic Fibrosis Related Diabetes. J. Diabetes Res. 2016, 2016, 1527932. [Google Scholar] [CrossRef] [PubMed]
- Marshall, B.C.; Butler, S.M.; Stoddard, M.; Moran, A.M.; Liou, T.G.; Morgan, W.J. Epidemiology of cystic fibrosis-related diabetes. J. Pediatr. 2005, 146, 681–687. [Google Scholar] [CrossRef]
- Moran, A.; Pekow, P.; Grover, P.; Zorn, M.; Slovis, B.; Pilewski, J.; Tullis, E.; Liou, T.G.; Allen, H.; Cystic Fibrosis Related Diabetes Therapy Study Group. Insulin Therapy to Improve BMI in Cystic Fibrosis–Related Diabetes without Fasting Hyperglycemia: Results of the Cystic Fibrosis Related Diabetes Therapy Trial. Diabetes Care 2009, 32, 1783–1788. [Google Scholar] [CrossRef]
- Battelino, T.; Danne, T.; Bergenstal, R.M.; Amiel, S.A.; Beck, R.; Biester, T.; Bosi, E.; Buckingham, B.A.; Cefalu, W.T.; Close, K.L.; et al. Clinical Targets for Continuous Glucose Monitoring Data Interpretation: Recommendations From the International Consensus on Time in Range. Diabetes Care 2019, 42, 1593–1603. [Google Scholar] [CrossRef]
- Mozzillo, E.; Franzese, A.; Valerio, G.; Sepe, A.; De Simone, I.; Mazzarella, G.; Ferri, P.; Raia, V. One-year glargine treatment can improve the course of lung disease in children and adolescents with cystic fibrosis and early glucose derangements. Pediatr. Diabetes 2009, 10, 162–167. [Google Scholar] [CrossRef]
- Nousia-Arvanitakis, S.; Galli-Tsinopoulou, A.; Karamouzis, M. Insulin improves clinical status of patients with cystic-fibrosis-related diabetes mellitus. Acta Paediatr. 2001, 90, 515–519. [Google Scholar] [CrossRef]
- Bizzarri, C.; Lucidi, V.; Ciampalini, P.; Bella, S.; Russo, B.; Cappa, M. Clinical effects of early treatment with insulin glargine in patients with cystic fibrosis and impaired glucose tolerance. J. Endocrinol. Investig. 2006, 29, RC1–RC4. [Google Scholar] [CrossRef]
- Papazafiropoulou, A.K.; Papanas, N.; Trikkalinou, A.; Fousteris, E.; Melidonis, A. The Oral Dipeptidyl-Peptidase-4 Inhibitor Sitagliptin Increases Circulating Levels Of Stromal-Derived Factor-1 Alpha. Exp. Clin. Endocrinol. Diabetes 2017, 126, 367–370. [Google Scholar] [CrossRef]
- Zhou, X.J.; Ding, L.; Liu, J.X.; Su, L.Q.; Dong, J.J.; Liao, L. Efficacy and short-term side effects of sitagliptin, vildagliptin and saxagliptin in Chinese diabetes: A randomized clinical trial. Endocr. Connect. 2019, 8, 318–325. [Google Scholar] [CrossRef]
- Genestreti, P.R.R.; Furtado, R.H.M.; Salsoso, R.; Dalçóquio, T.F.; Franci, A.; Menezes, F.R.; Caporrino, C.; Ferrari, A.G.; Nakashima, C.A.K.; Filho, M.A.S.; et al. Effects of DPP4 Inhibitor in Platelet Reactivity and Other Cardiac Risk Markers in Patients with Type 2 Diabetes and Acute Myocardial Infarction. J. Clin. Med. 2022, 11, 5776. [Google Scholar] [CrossRef]
- Zhou, Y.; Guo, Z.; Yan, W.; Wang, W. Cardiovascular effects of sitagliptin—An anti-diabetes medicine. Clin. Exp. Pharmacol. Physiol. 2018, 45, 628–635. [Google Scholar] [CrossRef]
- Bogdanov, P.; Ramos, H.; Valeri, M.; Deàs-Just, A.; Huerta, J.; Simó, R.; Hernández, C. Minimum Effective Dose of DPP-4 Inhibitors for Treating Early Stages of Diabetic Retinopathy in an Experimental Model. Biomedicines 2022, 10, 465. [Google Scholar] [CrossRef]
- Ramos, H.; Bogdanov, P.; Sabater, D.; Huerta, J.; Valeri, M.; Hernández, C.; Simó, R. Neuromodulation Induced by Sitagliptin: A New Strategy for Treating Diabetic Retinopathy. Biomedicines 2021, 9, 1772. [Google Scholar] [CrossRef]
- Ramos, H.; Bogdanov, P.; Simó, R.; Deàs-Just, A.; Hernández, C. Transcriptomic Analysis Reveals That Retinal Neuromodulation Is a Relevant Mechanism in the Neuroprotective Effect of Sitagliptin in an Experimental Model of Diabetic Retinopathy. Int. J. Mol. Sci. 2022, 24, 571. [Google Scholar] [CrossRef]
- AL-Qabbaa, S.M.; Qaboli, S.I.; Alshammari, T.K.; Alamin, M.A.; Alrajeh, H.M.; Almuthnabi, L.A.; Alotaibi, R.R.; Alonazi, A.S.; Bin Dayel, A.F.; Alrasheed, N.M.; et al. Sitagliptin Mitigates Diabetic Nephropathy in a Rat Model of Streptozotocin-Induced Type 2 Diabetes: Possible Role of PTP1B/JAK-STAT Pathway. Int. J. Mol. Sci. 2023, 24, 6532. [Google Scholar] [CrossRef]
- Solerte, S.B.; D’Addio, F.; Trevisan, R.; Lovati, E.; Rossi, A.; Pastore, I.; Dell’acqua, M.; Ippolito, E.; Scaranna, C.; Bellante, R.; et al. Sitagliptin Treatment at the Time of Hospitalization Was Associated with Reduced Mortality in Patients with Type 2 Diabetes and COVID-19: A Multicenter, Case-Control, Retrospective, Observational Study. Diabetes Care 2020, 43, 2999–3006. [Google Scholar] [CrossRef]
- Yoshikawa, K.; Tsuchiya, A.; Kido, T.; Ota, T.; Ikeda, K.; Iwakura, M.; Maeda, Y.; Maekawa, S. Long-Term Safety and Efficacy of Sitagliptin for Type 2 Diabetes Mellitus in Japan: Results of a Multicentre, Open-Label, Observational Post-Marketing Surveillance Study. Adv. Ther. 2020, 37, 2442–2459. [Google Scholar] [CrossRef] [PubMed]
- Ballmann, M.; Hubert, D.; Assael, B.M.; Staab, D.; Hebestreit, A.; Naehrlich, L.; Nickolay, T.; Prinz, N.; Holl, R.W.; CFRD Study Group. Repaglinide versus insulin for newly diagnosed diabetes in patients with cystic fibrosis: A multicentre, open-label, randomised trial. Lancet Diabetes Endocrinol. 2018, 6, 114–121. [Google Scholar] [CrossRef]
- Onady, G.M.; Stolfi, A. Drug treatments for managing cystic fibrosis-related diabetes. Cochrane Database Syst. Rev. 2020, 2020, CD004730. [Google Scholar] [CrossRef]
- Kelly, A.; Sheikh, S.; Stefanovski, D.; Peleckis, A.J.; Nyirjesy, S.C.; Eiel, J.N.; Sidhaye, A.; Localio, R.; Gallop, R.; De Leon, D.D.; et al. Effect of Sitagliptin on Islet Function in Pancreatic Insufficient Cystic Fibrosis with Abnormal Glucose Tolerance. J. Clin. Endocrinol. Metab. 2021, 106, 2617–2634. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Characteristic | |
|---|---|
| Age | 26 (18) |
| Men/Women | 17/8 (68%/32%) |
| HbA1c %(mmol/mol) | 5.9% (0.4) |
| HOMA-IR | 2.04 (0.48–5.33) |
| Homozygosis F508 mutation | 11 (44%) |
| Heterozygosis F508 mutation | 10 (40%) |
| Other mutations | 4 (16%) |
| FEV1% | 72 (31) |
| FVC% | 87 (19) |
| FEV1/FVC | 70 (10) |
| Impaired fasting glucose | 0 |
| Impaired glucose tolerance | 3 (12%) |
| Indeterminate glycaemia | 5 (20%) |
| Diabetes mellitus | 17 (68%) |
| Pancreatic enzymes u/kg/day | 3584 (2975) |
| Fasting glucose, mg/dL | 101 (20) |
| 1 h OGTT glucose, mg/dL | 258 (83) |
| 2 h OGTT glucose, mg/dL | 214 (102) |
| Result | OFF-STG | ON-STG | p-Value |
|---|---|---|---|
| Glycaemia average (mg/dL) | 124.2 ± 14.9 | 117.2 ± 13.8 | p = 0.002 95% CI [2.9–11.1] |
| SD | 33.1 ± 9.1 | 27.5 ± 8.3 | p < 0.001 95% CI [3.2–8.1] |
| Number of hyperglycaemic peaks > 200 mg/dL/day | 1.4 (0.6–2) | 0.6 (0.3–1) | p = 0.021 95% CI [0.1–1.3] |
| TIR (70–180 mg/dL)% | 88.7 ± 6.1 | 92.2 ± 5.2 | p = 0.036 95% CI [6.7–0.3] |
| >180 mg/dL % | 10.1 ± 6.8 | 6.0 ± 4.6 | p = 0.006 95% CI [1.4–6.8] |
| >250 mg/dL % | 1.3 ± 2.2 | 0.5 ± 1.1 | p = 0.011 95% CI [0.1–2.2] |
| <70 mg/dL % | 1.2 ± 2.3 | 1.7 ± 3.4 | p > 0.05 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sebastian-Valles, F.; Arranz Martín, J.A.; Girón, R.M.; Knott-Torcal, C.; Sampedro-Nuñez, M.A.; Martin-Adan, J.C.; Jiménez-Díaz, J.; Marazuela, M. Continuous Glucose Monitoring as an Additional Tool in Early Cystic Fibrosis-Related Diabetes Monitoring and in Evaluation of Short-Term Sitagliptin Response. Biomedicines 2023, 11, 1754. https://doi.org/10.3390/biomedicines11061754
Sebastian-Valles F, Arranz Martín JA, Girón RM, Knott-Torcal C, Sampedro-Nuñez MA, Martin-Adan JC, Jiménez-Díaz J, Marazuela M. Continuous Glucose Monitoring as an Additional Tool in Early Cystic Fibrosis-Related Diabetes Monitoring and in Evaluation of Short-Term Sitagliptin Response. Biomedicines. 2023; 11(6):1754. https://doi.org/10.3390/biomedicines11061754
Chicago/Turabian StyleSebastian-Valles, Fernando, José Alfonso Arranz Martín, Rosa María Girón, Carolina Knott-Torcal, Miguel Antonio Sampedro-Nuñez, Jose Carlos Martin-Adan, Jessica Jiménez-Díaz, and Mónica Marazuela. 2023. "Continuous Glucose Monitoring as an Additional Tool in Early Cystic Fibrosis-Related Diabetes Monitoring and in Evaluation of Short-Term Sitagliptin Response" Biomedicines 11, no. 6: 1754. https://doi.org/10.3390/biomedicines11061754
APA StyleSebastian-Valles, F., Arranz Martín, J. A., Girón, R. M., Knott-Torcal, C., Sampedro-Nuñez, M. A., Martin-Adan, J. C., Jiménez-Díaz, J., & Marazuela, M. (2023). Continuous Glucose Monitoring as an Additional Tool in Early Cystic Fibrosis-Related Diabetes Monitoring and in Evaluation of Short-Term Sitagliptin Response. Biomedicines, 11(6), 1754. https://doi.org/10.3390/biomedicines11061754