Abstract
Introduction: Several days to months after diagnosis of SARS-CoV-2, 35% of patients have persistent symptoms in high incidence. This is referred to as post-COVID-19 Syndrome. There is a pressing need to find a way to help patients with the manifested symptoms. Objective: To show the different therapies that exist for post-COVID Syndrome and their efficacy. Methodology: A systematic review of the scientific literature was carried out. The data search was carried out in Scopus, PubMed, Cinahl, and Web of Science. Of the 106 articles found, 12 articles were obtained after applying the following eligibility criteria. Results: Interventions related to respiratory musculature and moderate intensity exercise both in supervised face-to-face sessions and in supervised home sessions led patients to a significant improvement in the symptoms presented. Conclusion: Physical therapies significantly reduce fatigue and dyspnea as well as other symptoms related to quality of life.
1. Introduction
As is well known, in March 2020, due to the SARS-CoV-2 coronavirus, a pandemic called COVID-19 was declared. It is known that almost 50% of SARS-CoV-2 patients with COVID-19 pneumonia can recover spontaneously from a functional point of view at 3 months [1]; however, it has been possible to observe the persistence of symptoms (11.5 ± 5.7 days), and sometimes up to 10–35% of patients have persistent symptoms after several days or months. In the same way it can happen with people who have been mildly ill, undiagnosed, or who may have late or persistent symptoms [2,3].
This syndrome, which is appearing, attracts attention because it refers to the sum of very diverse symptoms that last until after the confirmation of SARS-CoV-2 infection. When we speak of a syndrome in health, we refer to a “coexistence of several symptoms” [4,5,6]. Therefore, this syndrome will continue to exist even after the acute phase has ended and several symptoms are still present.
Several names have been coined for this syndrome among patients, such as persistent COVID or long COVID [6], but the one recommended by the WHO [7] for use is the term post-COVID-19, since it does not allude to any kind of durability or causality [3].
The symptomatology of this syndrome can be very heterogeneous. The prevalent post-COVID symptoms encompass fatigue, difficulty breathing, impaired sense of smell and taste, chest pain, muscle aches, as well as sleep and psychological disturbances [5]. This leads to a poor quality of life [2,3].
Studies, such as Simani et al. [8], have determined a prevalence rate of 5.8% to 43%. The symptoms of this syndrome related to physical and respiratory deterioration can affect the psychological health and, as a consequence, can condition the performance of physical activity [2]. All this affects the ability of individuals to achieve a full recovery, affecting the basic activities of daily living and even the return to work [9].
In order to find a correct approach to this syndrome, it is recommended to have a first consultation 4 weeks after the acute phase [10]. The assessment of each patient can be performed telematically or in person depending on the patient’s data. The use of scales and/or questionnaires will also help us for the subsequent comparison of the state of health and the follow-up of the evaluation, and will also allow us to unify criteria with the health professionals.
There is a study, in particular, that talks about the symptoms associated with post-COVID syndrome. It shows that there is a high incidence of the syndrome in question, exposing the imperative need to find a way to effectively and efficiently help patients with the aforementioned symptoms [11].
For this reason, a review of the literature is proposed to show the different therapies that exist for patients with post-COVID syndrome and to evaluate their efficacy.
2. Materials and Methods
2.1. Review Protocol
The methodology used for this report was a systematic review of the scientific literature published on physical therapies for the treatment of post-COVID syndrome, following the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) [12] review protocol, which consists of a 27-point checklist of the most representative parts of an original article, as well as the process of elaboration of these sections.
2.2. Eligibility Criteria
Articles with randomised clinical trial (RCT) methodology and articles with case study methodology were selected. The articles should be written after the COVID-19 pandemic was declared, January 2020, and should provide information on the modalities of therapies for the recovery of post-COVID syndrome in patients older than 18 years, without restriction in reference to the language of publication.
2.3. Sources of Information
This search was performed in the Scopus, PubMed, Cinahl, and Web of Science databases. In addition, a manual search was performed using reference lists of studies to find other relevant studies.
The structured language used was obtained by means of MeSH terms and health science descriptors (DeCS). The DeCs used were Post-Acute COVID-19 Syndrome and Physical Therapy Modalities, and the Boolean operators used were “OR” and “AND”.
2.4. Search Strategy
The following table (Table 1) shows the search strategy used for this work, the source, filters, and the date on which the search was performed.

Table 1.
Search strategy details: source, filters, and search date.
2.5. Data Extraction Process
After carrying out the search strategy, the articles found were transferred to the Mendeley web application using the Mendeley web importer tool. They were then structured by folders, according to the databases through which they had been obtained, and duplicates were later eliminated.
The included studies were randomised clinical trials (RCTs) and cohort studies with the objective of showing therapies in post-COVID syndrome patients and evaluating their efficacy. The studies were published between 2020 and 2023. The title, abstract and keywords of each study were examined, and the inclusion and exclusion criteria were applied.
2.6. Data Collection Process and Data Collected
The following data were extracted from each article: men and women over 18 years of age who have had the disease, number of participants, type of physical exercise performed, duration of exercise, intensity, and whether it was supervised by professionals.
Section 3 shows the selection process of the articles in more detail.
2.7. Risk of Bias in Individual Studies
To carry out the methodological evaluation of the articles selected for this study, we proceeded to analyse the design, methodology and type of study of each article, with the aim of selecting the most specific methodological evaluation scale for each case.
Of the 13 articles, 4 were case studies, 1 was a cohort study, 7 were RCTs, and 1 was a quasi-experimental study.
The articles whose design was a case study were evaluated using the Single-Case Experimental Design (SCED) [13]. The SCED was constructed including 11 items, of which 10 are used to evaluate methodological quality and one for the use of statistical analysis.
The following table (Table 2) shows the results obtained after the methodological evaluation using the SCED scale [13].
Table 2.
Methodological evaluation results using SCED scale.
For the articles whose methodology corresponded to a clinical trial, the scientific quality was evaluated using the PEDro scale [18]. This scale provides information on the clinical scientific evidence and scores it based on certain indicators, adding 1 point to each one if they are present and 0 points if they are not, giving a total score of 10 points. If the trial obtains a score between 9 and 10, it indicates that it is of very good quality; if it obtains between 6 and 8, it indicates good quality; if it is between 4 and 5, it indicates fair quality; and if it is less than 4, it indicates poor quality. In the case of the articles chosen for this systematic review, the values range between 6 and 9, receiving an average score of 8.30, which indicates that the average scientific quality is considered to be “good quality”.
The following table (Table 3) shows the results obtained after carrying out the methodological evaluation using the PEDro scale [18].
Table 3.
Assessment of methodology using the PEDro scale.
3. Results
After applying the search strategy for articles in the different databases and applying the inclusion and exclusion criteria set out in the methodology, we identified 12 studies that we included in our review. Figure 1 shows the flow chart of the identified articles.
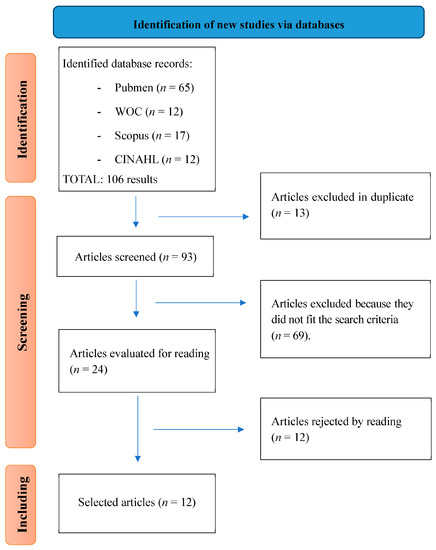
Figure 1.
Flow diagram.
Taken together, the studies obtained highlight the efficacy of various therapeutic interventions to address the symptoms of prolonged COVID, encompassing physical and psychological well-being.
Overall, there were notable increases in physical function, with improvements in balance, muscle strength, and functional capacity, among others. Symptoms, such as fatigue and dyspnoea, decreased substantially in the intervention group compared to the control group. In addition, improvements in mental health and cardiovascular and pulmonary capacity were recorded. These results support the efficacy of exercise and rehabilitation strategies in the overall recovery of patients.
A summary of the results can be found in Table 4.
Table 4.
Summary of the conclusions of the results obtained.
4. Discussion
The objective of this systematic review was to show the therapies that exist in patients with long-COVID and to evaluate their efficacy, and for this reason the study of the articles has been carried out.
This topic is closely related to the assessment of the systemic consequences of COVID-19, which is a broad field of research in which the assessment of respiratory function plays a key role. This was presented in the report by Pini et al. [26], where respiratory function was analysed 4–6 months after hospital discharge in these patients to study the negative consequences of COVID-19 pneumonia.
The results of this systematic review demonstrated that the exercise and rehabilitation strategies had a positive impact on multiple aspects of patients’ health, from physical function to mental health. These findings support the efficacy of the interventions implemented and suggest a pathway to improved recovery and well-being in people facing similar health challenges.
Most of the articles selected in the elaboration have been published in the year 2022, since we are dealing with a recent disease, namely COVID-19, and, above all, our objective concerns therapies against post-COVID syndrome. After analysing them, we can conclude that the selected articles have a generally good methodological level. We have been able to answer the main objective, since we have found different therapies for persistent COVID, such as exercises of moderate intensity [19,21], exercises for the respiratory musculature [15,20,22,23,24,25], electromagnetic field therapy [15,20,22,23,24,25], application of cutaneous electromagnetic nerve stimulation [9], and trigger point injections [17].
In the clinical guideline for long-COVID care, they recommend for fatigue a type of progressive exercise therapy tailored to the individual patient [27], information that we have been finding offers good results after completion [19,21]. In relation to dyspnoea, the guideline recommends respiratory exercise [20]. However, we cannot determine the efficacy of all studies as these have been based on a single case [9,14,17].
Several studies mention the improvement in the 6MWT test. Thanks to the controlled exercise, it was observed that men run a shorter distance when compared to women, with a significant increase for both [15,22,23].
Another improvement observed with controlled exercise was dyspnoea, which was shown to decrease significantly, with a decrease of approximately 80% in the control groups [15,21,22,24].
Depression and anxiety are a more subjective issue, since some studies show that there is a significant improvement in the control groups [24,25] but there is another that does not show a significant difference [16]. Despite that, it is observed that controlled exercise improves depression and anxiety.
Regarding articles that discuss electromagnetic field therapy [14], namely the application of electromagnetic nerve stimulation [11], it is shown that both women improved the sensation of fatigue, pain disappeared completely, and quality of life improved. On the other hand, the patient who received the trigger injections only manifested a complete disappearance of the pain [17]. It is necessary to qualify this aspect, as it is interesting to relate dry and wet needling with evident improvements in pain control in patients with post-COVID symptomatology. As shown in the case of Zha et al. [17]. It is true that this relationship can only be seen in this specific patient, so it is proposed as a new line of research derived from this study to substantiate this possible new treatment pathway.
One of the limitations that have been found is the poor adherence of study participants to the interventions [15,19,21,22,24] and the very small samples used [9,14,17].
Although there are several studies that demonstrate the efficacy of physical therapies, it remains to be determined whether other types of therapies or treatment would be effective against physical and psychological symptoms. And, above all, it is necessary to provide psychological and emotional help to these patients.
In terms of the limitations observed, more studies are needed, as the limitations are evident and may compromise the validity and reliability of the results. These limitations stem from sample sizes, the potential for bias, inadequate control of confounding variables and even the cross-sectional approach. Therefore, it is crucial to take these limitations into account when interpreting and applying the results of such studies to ensure accurate interpretation and appropriate use of their results in relation to physical therapies and prolonged COVID.
5. Conclusions
After searching the literature, we have found that moderate exercise and respiratory muscle exercises are beneficial for recovery from the most common symptoms of persistent COVID, namely fatigue and dyspnoea.
It can be concluded that, in cases where there was exercise control, patients have a considerable improvement in fatigue, depression and dyspnoea, among others.
However, there are still too few studies to be able to speak of the efficacy of certain therapies for the symptoms of long-COVID-19.
Author Contributions
Conceptualisation, J.C.-M., R.R.-B. and J.C.S.-G.; data curation, M.R.M., E.M.-G., R.R.-B. and J.C.S.-G.; formal analysis, J.C.-M., M.R.M., B.P.-S., A.L.-G. and R.R.-B.; investigation, R.R.-B. and E.M.-G.; methodology, R.R.-B., J.C.S.-G. and J.C.-M.; project administration, R.R.-B. and E.M.-G.; resources, R.R.-B. and A.L.-G.; supervision, J.C.S.-G.; validation, R.R.-B., J.C.-M., E.M.-G. and B.P.-S.; visualisation, R.R.-B. and J.C.-M.; writing—original draft, M.R.M., E.M.-G., J.C.-M., R.R.-B. and J.C.S.-G.; writing—review and editing, R.R.-B., M.R.M., B.P.-S., J.C.-M. and J.C.S.-G. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
This systematic review was carried out following a protocol, available on the web: http://www.crd.york.ac.uk/PROSPERO/ (accessed on 16 January 2023) and whose registration number is CRD42023391811.
Informed Consent Statement
Not applicable.
Data Availability Statement
Not applicable.
Acknowledgments
We are grateful to the Official College of Nursing of Granada (CODEGRA) for their help in the research support programme, and to the Chair of Research in Nursing Care of the University of Granada and the Official College of Nursing of Granada.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Orzes, N.; Pini, L.; Levi, G.; Uccelli, S.; Cettolo, F.; Tantucci, C. A prospective evaluation of lung function at three and six months in patients with previous SARS-COV-2 pneumonia. Respir. Med. 2021, 186, 106541. [Google Scholar] [CrossRef] [PubMed]
- Gómez Conesa, A. ¿Cómo abordar desde la fisioterapia la salud mental en el COVID persistente? Fisioterapia 2022, 44, 1–5. [Google Scholar] [CrossRef]
- López-Sampalo, A.; Bernal-López, M.R.; Gómez-Huelgas, R. Síndrome de COVID-19 persistente. Una revisión narrativa. Rev. Clín. Esp. 2022, 222, 241–250. [Google Scholar] [CrossRef] [PubMed]
- Timewar, R.R.; Sumar, A.I.; Nitin, B.; Kohale; Suraj, B.; Rathod; Guarav, G. Manwar Post Acute Corona Virus (COVID-19) Syndrome. Int. J. Adv. Res. Sci. Commun. Technol. 2023, 3, 385–391. [Google Scholar] [CrossRef]
- Maltezou, H.C.; Pavli, A.; Tsakris, A. Post-COVID Syndrome: An Insight on Its Pathogenesis. Vaccines 2021, 9, 497. [Google Scholar] [CrossRef] [PubMed]
- Fernández-de-las-Peñas, C.; Palacios-Ceña, D.; Gómez-Mayordomo, V.; Cuadrado, M.L.; Florencio, L.L. Defining Post-COVID Symptoms (Post-Acute COVID, Long COVID, Persistent Post-COVID): An Integrative Classification. Int. J. Environ. Res. Public Health 2021, 18, 2621. [Google Scholar] [CrossRef]
- World Health Organization. Post COVID-19 Condition (Long COVID). Available online: https://www.who.int/europe/news-room/fact-sheets/item/post-covid-19-condition (accessed on 8 August 2023).
- Simani, L.; Ramezani, M.; Darazam, I.A.; Sagharichi, M.; Aalipour, M.A.; Ghorbani, F.; Pakdaman, H. Prevalence and correlates of chronic fatigue syndrome and post-traumatic stress disorder after the outbreak of the COVID-19. J. Neurovirol. 2021, 27, 154–159. [Google Scholar] [CrossRef] [PubMed]
- Santos, S.; Flores, J.A. Musculoskeletal physiotherapy in physical sequelae of SARS-CoV-2 infection: A case report. Physiother. Res. Int. 2022, 27, e1938. [Google Scholar] [CrossRef]
- Centre for Disease Control and Prevention. CDC Post-COVID Conditions: Information for Healthcare Providers. Available online: https://www.cdc.gov/coronavirus/2019-ncov/hcp/clinical-care/post-covid-conditions.html#print (accessed on 8 August 2023).
- Donnachie, E.; Hapfelmeier, A.; Linde, K.; Tauscher, M.; Gerlach, R.; Greissel, A.; Schneider, A. Incidence of post-COVID syndrome and associated symptoms in outpatient care in Bavaria, Germany: A retrospective cohort study using routinely collected claims data. BMJ Open 2022, 12, e064979. [Google Scholar] [CrossRef]
- Welch, V.; Petticrew, M.; Tugwell, P.; Moher, D.; O’Neill, J.; Waters, E.; White, H. Extensión PRISMA-Equidad 2012: Guías para la escritura y la publicación de revisiones sistemáticas enfocadas en la equidad en salud. Rev. Panam. Salud Publica/Pan Am. J. Public Health 2013, 34, 60–67. [Google Scholar] [CrossRef]
- Psycbite SCED Scale. Available online: http://www.psycbite.com/docs/The_SCED_Scale.pdf (accessed on 27 March 2021).
- Wagner, B.; Steiner, M.; Markovic, L.; Crevenna, R. Successful application of pulsed electromagnetic fields in a patient with post-COVID-19 fatigue: A case report. Wien. Med. Wochenschr. 2022, 172, 227–232. [Google Scholar] [CrossRef]
- Rausch, L.; Puchner, B.; Fuchshuber, J.; Seebacher, B.; Löffler-Ragg, J.; Pramsohler, S.; Netzer, N.; Faulhaber, M. The Effects of Exercise Therapy Moderated by Sex in Rehabilitation of COVID-19. Int. J. Sports Med. 2022, 43, 1043–1051. [Google Scholar] [CrossRef]
- Daynes, E.; Gerlis, C.; Chaplin, E.; Gardiner, N.; Singh, S.J. Early experiences of rehabilitation for individuals post-COVID to improve fatigue, breathlessness exercise capacity and cognition—A cohort study. Chron. Respir. Dis. 2021, 18, 147997312110156. [Google Scholar] [CrossRef] [PubMed]
- Zha, M.; Chaffee, K.; Alsarraj, J. Trigger point injections and dry needling can be effective in treating long COVID syndrome-related myalgia: A case report. J. Med. Case Rep. 2022, 16, 31. [Google Scholar] [CrossRef] [PubMed]
- Gómez Conesa, A. Escala PEDro. Available online: https://pedro.org.au/spanish/resources/pedro-scale/ (accessed on 27 March 2021).
- Estebanez-Pérez, M.-J.; Pastora-Bernal, J.-M.; Martín-Valero, R. The Effectiveness of a Four-Week Digital Physiotherapy Intervention to Improve Functional Capacity and Adherence to Intervention in Patients with Long COVID-19. Int. J. Environ. Res. Public Health 2022, 19, 9566. [Google Scholar] [CrossRef] [PubMed]
- Sharma, P.; Goswami, S.K. Pulmonary Tele-Rehabilitation in Patients (Post Covid-19) With Respiratory Complications: A Randomized Controlled Trial. Indian J. Physiother. Occup. Ther. 2022, 16, 182–189. [Google Scholar] [CrossRef]
- Jimeno-Almazán, A.; Franco-López, F.; Buendía-Romero, Á.; Martínez-Cava, A.; Sánchez-Agar, J.A.; Sánchez-Alcaraz Martínez, B.J.; Courel-Ibáñez, J.; Pallarés, J.G. Rehabilitation for post-COVID-19 condition through a supervised exercise intervention: A randomized controlled trial. Scand. J. Med. Sci. Sports 2022, 32, 1791–1801. [Google Scholar] [CrossRef] [PubMed]
- Sari, F.; Bayram, S.; Pala, G.G.; Çömçe, F.; Küçük, H.; Oskay, D. Effects of Inspiratory Muscle Training in Patients with post-COVID-19. Harran Üniversitesi. Tıp Fakültesi. Derg. 2022, 19, 581–588. [Google Scholar] [CrossRef]
- Okan, F.; Okan, S.; Duran Yücesoy, F. Evaluating the Efficiency of Breathing Exercises via Telemedicine in Post-Covid-19 Patients: Randomized Controlled Study. Clin. Nurs. Res. 2022, 31, 771–781. [Google Scholar] [CrossRef]
- McNarry, M.A.; Berg, R.M.G.; Shelley, J.; Hudson, J.; Saynor, Z.L.; Duckers, J.; Lewis, K.; Davies, G.A.; Mackintosh, K.A. Inspiratory muscle training enhances recovery post-COVID-19: A randomised controlled trial. Eur. Respir. J. 2022, 60, 2103101. [Google Scholar] [CrossRef]
- Palau, P.; Domínguez, E.; Gonzalez, C.; Bondía, E.; Albiach, C.; Sastre, C.; Martínez, M.L.; Núñez, J.; López, L. Effect of a home-based inspiratory muscle training programme on functional capacity in postdischarged patients with long COVID: The InsCOVID trial. BMJ Open Respir. Res. 2022, 9, e001439. [Google Scholar] [CrossRef] [PubMed]
- Pini, L.; Montori, R.; Giordani, J.; Guerini, M.; Orzes, N.; Ciarfaglia, M.; Arici, M.; Cappelli, C.; Piva, S.; Latronico, N.; et al. Assessment of respiratory function and exercise tolerance at 4–6 months after COVID-19 infection in patients with pneumonia of different severity. Intern. Med. J. 2023, 53, 202–208. [Google Scholar] [CrossRef] [PubMed]
- Sociedad Española de Médicos Generales y de Familia. Guía Clínica Para la Atención al Paciente Long COVID/COVID Persistente; ERGON: Madrid, Spain, 2021. [Google Scholar]

Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).