
Racial Disparity in Anthracycline-induced Cardiotoxicity in Breast Cancer Patients

 , and
, and 
Abstract
:1. Introduction
2. Clinical Manifestations of Anthracycline-Induced Cardiotoxicity
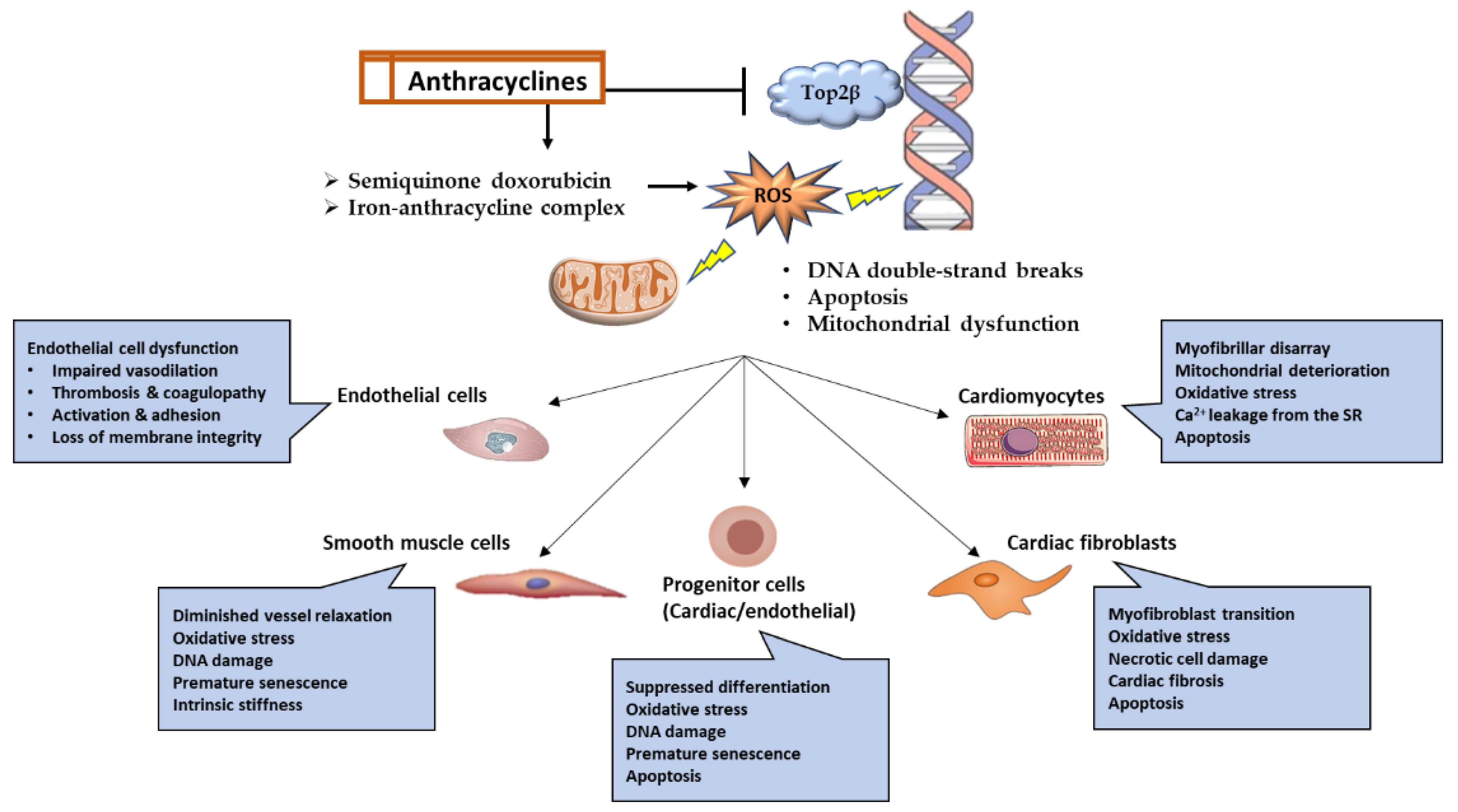
3. Molecular Mechanisms of Anthracycline-Induced Cardiotoxicity
3.1. Topoisomerase-2 (Top2)
3.2. Reactive Oxygen Species
3.3. Iron Metabolism
3.4. Guanylate Cyclase Activity
4. Factors That May Contribute to Disparities in Anthracycline-Induced Cardiotoxicity
4.1. Preexisting Morbidities
4.1.1. Obesity
4.1.2. Type 2 Diabetes
4.1.3. Hypertension
4.1.4. Hyperlipidemia
4.1.5. Cardiovascular Diseases
4.2. Genetic Factors
4.3. Socioeconomic Determinants
4.3.1. Education and Socioeconomic Status
4.3.2. Unequal Healthcare Access
4.3.3. Underrepresentation in Clinical Trials
4.3.4. Housing and Food Insecurities
4.3.5. Environmental Safety
4.3.6. Structural Racism and Violence
4.3.7. Patient Advocacy and Community Interventions
5. Lifestyle Factors
6. Conclusions and Recommendations
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- American Cancer Society. Cancer Facts and Figures; American Cancer Society: Atlanta, GA, USA, 2022; Available online: https://www.cancer.org/cancer/breast-cancer/about/how-common-is-breast-cancer.html (accessed on 30 November 2022).
- Yedjou, C.G.; Tchounwou, P.B.; Payton, M.; Miele, L.; Fonseca, D.D.; Lowe, L.; Alo, R.A. Assessing the Racial and Ethnic Disparities in Breast Cancer Mortality in the United States. Int. J. Environ. Res. Public Health 2017, 14, 486. [Google Scholar] [CrossRef] [PubMed]
- Waks, A.G.; Winer, E.P. Breast Cancer Treatment: A Review. JAMA 2019, 321, 288–300. [Google Scholar] [CrossRef] [PubMed]
- Burstein, H.J.; Curigliano, G.; Thurlimann, B.; Weber, W.P.; Poortmans, P.; Regan, M.M.; Senn, H.J.; Winer, E.P.; Gnant, M. Panelists of the St Gallen Consensus Conference. Customizing local and systemic therapies for women with early breast cancer: The St. Gallen International Consensus Guidelines for treatment of early breast cancer 2021. Ann. Oncol. 2021, 32, 1216–1235. [Google Scholar] [CrossRef]
- Venkatesh, P.; Kasi, A. Anthracyclines; StatPearls: Treasure Island, FL, USA, 2022. [Google Scholar]
- Nicolazzi, M.A.; Carnicelli, A.; Fuorlo, M.; Scaldaferri, A.; Masetti, R.; Landolfi, R.; Favuzzi, A.M.R. Anthracycline and trastuzumab-induced cardiotoxicity in breast cancer. Eur. Rev. Med. Pharmacol. Sci. 2018, 22, 2175–2185. [Google Scholar] [CrossRef] [PubMed]
- Sobczuk, P.; Czerwinska, M.; Kleibert, M.; Cudnoch-Jedrzejewska, A. Anthracycline-induced cardiotoxicity and renin-angiotensin-aldosterone system-from molecular mechanisms to therapeutic applications. Heart Fail. Rev. 2022, 27, 295–319. [Google Scholar] [CrossRef] [PubMed]
- Hundley, W.G.; Jordan, J.H. When Left Ventricular Extracellular Volume Fraction Changes After Anthracyclines: Is it Due to a Change in the Numerator, Denominator, or Both? JACC Cardiovasc. Imaging 2018, 11, 1056–1058. [Google Scholar] [CrossRef] [PubMed]
- Gulati, M.; Mulvagh, S.L. The connection between the breast and heart in a woman: Breast cancer and cardiovascular disease. Clin. Cardiol. 2018, 41, 253–257. [Google Scholar] [CrossRef]
- Cousin, L.; Roper, N.; Nolan, T.S. Cardio-Oncology Health Disparities: Social Determinants of Health and Care for Black Breast Cancer Survivors. Clin. J. Oncol. Nurs. 2021, 25, 36–41. [Google Scholar] [CrossRef]
- Bradshaw, P.T.; Stevens, J.; Khankari, N.; Teitelbaum, S.L.; Neugut, A.I.; Gammon, M.D. Cardiovascular Disease Mortality Among Breast Cancer Survivors. Epidemiology 2016, 27, 6–13. [Google Scholar] [CrossRef]
- Dhir, A.A.; Sawant, S.P. Cardiac morbidity & mortality in patients with breast cancer: A review. Indian J. Med. Res. 2021, 154, 199–209. [Google Scholar] [CrossRef]
- Lyon, A.R.; Lopez-Fernandez, T.; Couch, L.S.; Asteggiano, R.; Aznar, M.C.; Bergler-Klein, J.; Boriani, G.; Cardinale, D.; Cordoba, R.; Cosyns, B.; et al. 2022 ESC Guidelines on cardio-oncology developed in collaboration with the European Hematology Association (EHA), the European Society for Therapeutic Radiology and Oncology (ESTRO) and the International Cardio-Oncology Society (IC-OS). Eur. Heart J. 2022, 43, 4229–4361. [Google Scholar] [CrossRef] [PubMed]
- Cardinale, D.; Iacopo, F.; Cipolla, C.M. Cardiotoxicity of Anthracyclines. Front. Cardiovasc. Med. 2020, 7, 26. [Google Scholar] [CrossRef] [PubMed]
- Zhang, L.; Song, J.; Clark, R.; Mangoni, A.; Goldberg, Y.; Slipczuk, L.; Garcia, M.J.; Bansal, N.; Sadler, D.B.; Neilan, T.; et al. Abstract 13090: Racial and Ethnic Differences in Anthracycline Cardiotoxicity. Circulation 2021, 144, A13090. [Google Scholar] [CrossRef]
- Kalinowski, J.; Taylor, J.Y.; Spruill, T.M. Why Are Young Black Women at High Risk for Cardiovascular Disease? Circulation 2019, 139, 1003–1004. [Google Scholar] [CrossRef] [PubMed]
- Zavala, V.A.; Bracci, P.M.; Carethers, J.M.; Carvajal-Carmona, L.; Coggins, N.B.; Cruz-Correa, M.R.; Davis, M.; de Smith, A.J.; Dutil, J.; Figueiredo, J.C.; et al. Cancer health disparities in racial/ethnic minorities in the United States. Br. J. Cancer 2021, 124, 315–332. [Google Scholar] [CrossRef] [PubMed]
- Coughlin, S.S. Social determinants of breast cancer risk, stage, and survival. Breast Cancer Res. Treat. 2019, 177, 537–548. [Google Scholar] [CrossRef] [PubMed]
- Qiu, S.; Zhou, T.; Qiu, B.; Zhang, Y.; Zhou, Y.; Yu, H.; Zhang, J.; Liu, L.; Yuan, L.; Yang, G.; et al. Risk Factors for Anthracycline-Induced Cardiotoxicity. Front. Cardiovasc. Med. 2021, 8, 736854. [Google Scholar] [CrossRef] [PubMed]
- Swain, S.M.; Whaley, F.S.; Ewer, M.S. Congestive heart failure in patients treated with doxorubicin: A retrospective analysis of three trials. Cancer 2003, 97, 2869–2879. [Google Scholar] [CrossRef] [PubMed]
- Babaei, H.; Razmaraii, N.; Assadnassab, G.; Mohajjel Nayebi, A.; Azarmi, Y.; Mohammadnejad, D.; Azami, A. Ultrastructural and Echocardiographic Assessment of Chronic Doxorubicin-Induced Cardiotoxicity in Rats. Arch. Razi Inst. 2020, 75, 55–62. [Google Scholar] [CrossRef] [PubMed]
- Boyd, A.; Stoodley, P.; Richards, D.; Hui, R.; Harnett, P.; Vo, K.; Marwick, T.; Thomas, L. Anthracyclines induce early changes in left ventricular systolic and diastolic function: A single centre study. PLoS ONE 2017, 12, e0175544. [Google Scholar] [CrossRef] [PubMed]
- Araujo-Gutierrez, R.; Chitturi, K.R.; Xu, J.; Wang, Y.; Kinder, E.; Senapati, A.; Chebrolu, L.B.; Kassi, M.; Trachtenberg, B.H. Baseline global longitudinal strain predictive of anthracycline-induced cardiotoxicity. Cardiooncology 2021, 7, 4. [Google Scholar] [CrossRef] [PubMed]
- Al-Sadawi, M.; Singh, K.; Capric, V.; Mohiuddin, A.; Haddadin, M.; Nunez, A.; Shaikh, S.; Bukharovich, I.; McFarlane, S.I. Incidence and Associated Risk Factors of Chemotherapy-Induced Cardiomyopathy in the African American and Afro-Caribbean Populations. Int. J. Clin. Res. Trials 2020, 5, 154. [Google Scholar] [CrossRef]
- Al-Sadawi, M.; Hussain, Y.; Copeland-Halperin, R.S.; Tobin, J.N.; Moskowitz, C.S.; Dang, C.T.; Liu, J.E.; Steingart, R.M.; Johnson, M.N.; Yu, A.F. Racial and Socioeconomic Disparities in Cardiotoxicity Among Women With HER2-Positive Breast Cancer. Am. J. Cardiol. 2021, 147, 116–121. [Google Scholar] [CrossRef] [PubMed]
- Hasan, S.; Dinh, K.; Lombardo, F.; Kark, J. Doxorubicin cardiotoxicity in African Americans. J. Natl. Med. Assoc. 2004, 96, 196–199. [Google Scholar] [PubMed]
- Braithwaite, D.; Tammemagi, C.M.; Moore, D.H.; Ozanne, E.M.; Hiatt, R.A.; Belkora, J.; West, D.W.; Satariano, W.A.; Liebman, M.; Esserman, L. Hypertension is an independent predictor of survival disparity between African-American and white breast cancer patients. Int. J. Cancer 2009, 124, 1213–1219. [Google Scholar] [CrossRef]
- Troeschel, A.N.; Liu, Y.; Collin, L.J.; Bradshaw, P.T.; Ward, K.C.; Gogineni, K.; McCullough, L.E. Race differences in cardiovascular disease and breast cancer mortality among US women diagnosed with invasive breast cancer. Int. J. Epidemiol. 2019, 48, 1897–1905. [Google Scholar] [CrossRef]
- Hu, Q.; Chang, C.P.; Rowe, K.; Snyder, J.; Deshmukh, V.; Newman, M.; Fraser, A.; Smith, K.; Gren, L.H.; Porucznik, C.; et al. Disparities in Cardiovascular Disease Risk Among Hispanic Breast Cancer Survivors in a Population-Based Cohort. JNCI Cancer Spectr. 2021, 5, pkab016. [Google Scholar] [CrossRef]
- Bloom, M.W.; Hamo, C.E.; Cardinale, D.; Ky, B.; Nohria, A.; Baer, L.; Skopicki, H.; Lenihan, D.J.; Gheorghiade, M.; Lyon, A.R.; et al. Cancer Therapy-Related Cardiac Dysfunction and Heart Failure: Part 1: Definitions, Pathophysiology, Risk Factors, and Imaging. Circ. Heart Fail. 2016, 9, e002661. [Google Scholar] [CrossRef]
- Liu, J.E. Anthracycline-Induced Cardiotoxicity: Remembering the Forgotten Ventricle. JACC CardioOncol. 2020, 2, 23–25. [Google Scholar] [CrossRef]
- Kamphuis, J.A.M.; Linschoten, M.; Cramer, M.J.; Doevendans, P.A.; Asselbergs, F.W.; Teske, A.J. Early- and late anthracycline-induced cardiac dysfunction: Echocardiographic characterization and response to heart failure therapy. Cardiooncology 2020, 6, 23. [Google Scholar] [CrossRef]
- Doroshow, J.H. Doxorubicin-induced cardiac toxicity. N. Engl. J. Med. 1991, 324, 843–845. [Google Scholar] [CrossRef]
- Singal, P.K.; Iliskovic, N. Doxorubicin-induced cardiomyopathy. N. Engl. J. Med. 1998, 339, 900–905. [Google Scholar] [CrossRef]
- Cardinale, D.; Sandri, M.T.; Martinoni, A.; Tricca, A.; Civelli, M.; Lamantia, G.; Cinieri, S.; Martinelli, G.; Cipolla, C.M.; Fiorentini, C. Left ventricular dysfunction predicted by early troponin I release after high-dose chemotherapy. J. Am. Coll. Cardiol. 2000, 36, 517–522. [Google Scholar] [CrossRef] [PubMed]
- Cardinale, D.; Colombo, A.; Bacchiani, G.; Tedeschi, I.; Meroni, C.A.; Veglia, F.; Civelli, M.; Lamantia, G.; Colombo, N.; Curigliano, G.; et al. Early detection of anthracycline cardiotoxicity and improvement with heart failure therapy. Circulation 2015, 131, 1981–1988. [Google Scholar] [CrossRef]
- Marwick, T.H. Global Longitudinal Strain Monitoring to Guide Cardioprotective Medications During Anthracycline Treatment. Curr. Oncol. Rep. 2022, 24, 687–694. [Google Scholar] [CrossRef]
- Abou, R.; van der Bijl, P.; Bax, J.J.; Delgado, V. Global longitudinal strain: Clinical use and prognostic implications in contemporary practice. Heart 2020, 106, 1438–1444. [Google Scholar] [CrossRef]
- Shi, J.; Guo, Y.; Cheng, L.; Song, F.; Shu, X. Early change in left atrial function in patients treated with anthracyclines assessed by real-time three-dimensional echocardiography. Sci. Rep. 2016, 6, 25512. [Google Scholar] [CrossRef] [PubMed]
- Laufer-Perl, M.; Perelman-Gvili, M.; Sirota Dorfman, S.; Baruch, G.; Rothschild, E.; Beer, G.; Arbel, Y.; Arnold, J.H.; Rozenbaum, Z.; Banai, S.; et al. Prevalence of Right Ventricle Strain Changes following Anthracycline Therapy. Life 2022, 12, 291. [Google Scholar] [CrossRef] [PubMed]
- Zhao, R.; Shu, F.; Zhang, C.; Song, F.; Xu, Y.; Guo, Y.; Xue, K.; Lin, J.; Shu, X.; Hsi, D.H.; et al. Early Detection and Prediction of Anthracycline-Induced Right Ventricular Cardiotoxicity by 3-Dimensional Echocardiography. JACC CardioOncol. 2020, 2, 13–22. [Google Scholar] [CrossRef]
- Surkova, E.; Muraru, D.; Iliceto, S.; Badano, L.P. The use of multimodality cardiovascular imaging to assess right ventricular size and function. Int. J. Cardiol. 2016, 214, 54–69. [Google Scholar] [CrossRef] [PubMed]
- Liu, J.E.; Barac, A.; Thavendiranathan, P.; Scherrer-Crosbie, M. Strain Imaging in Cardio-Oncology. JACC CardioOncol. 2020, 2, 677–689. [Google Scholar] [CrossRef] [PubMed]
- Dobson, R.; Ghosh, A.K.; Ky, B.; Marwick, T.; Stout, M.; Harkness, A.; Steeds, R.; Robinson, S.; Oxborough, D.; Adlam, D.; et al. BSE and BCOS Guideline for Transthoracic Echocardiographic Assessment of Adult Cancer Patients Receiving Anthracyclines and/or Trastuzumab. JACC CardioOncol. 2021, 3, 1–16. [Google Scholar] [CrossRef] [PubMed]
- Carrasco, R.; Castillo, R.L.; Gormaz, J.G.; Carrillo, M.; Thavendiranathan, P. Role of Oxidative Stress in the Mechanisms of Anthracycline-Induced Cardiotoxicity: Effects of Preventive Strategies. Oxid. Med. Cell Longev. 2021, 2021, 8863789. [Google Scholar] [CrossRef]
- Narezkina, A.; Narayan, H.K.; Zemljic-Harpf, A.E. Molecular mechanisms of anthracycline cardiovascular toxicity. Clin. Sci. 2021, 135, 1311–1332. [Google Scholar] [CrossRef]
- Henriksen, P.A. Anthracycline cardiotoxicity: An update on mechanisms, monitoring and prevention. Heart 2018, 104, 971–977. [Google Scholar] [CrossRef] [PubMed]
- Geisberg, C.A.; Sawyer, D.B. Mechanisms of anthracycline cardiotoxicity and strategies to decrease cardiac damage. Curr. Hypertens. Rep. 2010, 12, 404–410. [Google Scholar] [CrossRef]
- Eom, Y.W.; Kim, M.A.; Park, S.S.; Goo, M.J.; Kwon, H.J.; Sohn, S.; Kim, W.H.; Yoon, G.; Choi, K.S. Two distinct modes of cell death induced by doxorubicin: Apoptosis and cell death through mitotic catastrophe accompanied by senescence-like phenotype. Oncogene 2005, 24, 4765–4777. [Google Scholar] [CrossRef]
- Huang, J.; Wu, R.; Chen, L.; Yang, Z.; Yan, D.; Li, M. Understanding Anthracycline Cardiotoxicity From Mitochondrial Aspect. Front. Pharmacol. 2022, 13, 811406. [Google Scholar] [CrossRef]
- Stasch, J.P.; Pacher, P.; Evgenov, O.V. Soluble guanylate cyclase as an emerging therapeutic target in cardiopulmonary disease. Circulation 2011, 123, 2263–2273. [Google Scholar] [CrossRef]
- Lehotay, D.C.; Levey, B.A.; Rogerson, B.J.; Levey, G.S. Inhibition of cardiac guanylate cyclase by doxorubicin and some of its analogs: Possible relationship to cardiotoxicity. Cancer Treat Rep. 1982, 66, 311–316. [Google Scholar]
- Vandenwijngaert, S.; Swinnen, M.; Walravens, A.S.; Beerens, M.; Gillijns, H.; Caluwe, E.; Tainsh, R.E.; Nathan, D.I.; Allen, K.; Brouckaert, P.; et al. Decreased Soluble Guanylate Cyclase Contributes to Cardiac Dysfunction Induced by Chronic Doxorubicin Treatment in Mice. Antioxid Redox Signal 2017, 26, 153–164. [Google Scholar] [CrossRef] [PubMed]
- Zhu, C.; Shi, T.; Jiang, C.; Liu, B.; Baldassarre, L.A.; Zarich, S. Racial and Ethnic Disparities in All-Cause and Cardiovascular Mortality Among Cancer Patients in the U.S. JACC CardioOncol. 2023, 5, 55–66. [Google Scholar] [CrossRef] [PubMed]
- Ohman, R.E.; Yang, E.H.; Abel, M.L. Inequity in Cardio-Oncology: Identifying Disparities in Cardiotoxicity and Links to Cardiac and Cancer Outcomes. J. Am. Heart Assoc. 2021, 10, e023852. [Google Scholar] [CrossRef]
- Howard, G.; Safford, M.M.; Moy, C.S.; Howard, V.J.; Kleindorfer, D.O.; Unverzagt, F.W.; Soliman, E.Z.; Flaherty, M.L.; McClure, L.A.; Lackland, D.T.; et al. Racial Differences in the Incidence of Cardiovascular Risk Factors in Older Black and White Adults. J. Am. Geriatr. Soc. 2017, 65, 83–90. [Google Scholar] [CrossRef] [PubMed]
- Toure, A.; Luan, D.; Wu, Y.; Christos, P.J.; Leonard, J.P.; Martin, P. An Assessment of Race as a Risk Factor for Doxorubicin-Related Cardiotoxicity in Diffuse Large B-Cell Lymphoma. Clin. Lymphoma Myeloma Leuk. 2022, 22, e57–e64. [Google Scholar] [CrossRef]
- Collin, L.J.; Troeschel, A.N.; Liu, Y.; Gogineni, K.; Borger, K.; Ward, K.C.; McCullough, L.E. A balancing act: Racial disparities in cardiovascular disease mortality among women diagnosed with breast cancer. Ann. Cancer Epidemiol. 2020, 4, 4. [Google Scholar] [CrossRef]
- Berkman, A.; F Cole, B.; Ades, P.A.; Dickey, S.; Higgins, S.T.; Trentham-Dietz, A.; Sprague, B.L.; Lakoski, S.G. Racial differences in breast cancer, cardiovascular disease, and all-cause mortality among women with ductal carcinoma in situ of the breast. Breast Cancer Res. Treat. 2014, 148, 407–413. [Google Scholar] [CrossRef]
- Bays, H.E.; Taub, P.R.; Epstein, E.; Michos, E.D.; Ferraro, R.A.; Bailey, A.L.; Kelli, H.M.; Ferdinand, K.C.; Echols, M.R.; Weintraub, H.; et al. Ten things to know about ten cardiovascular disease risk factors. Am. J. Prev. Cardiol. 2021, 5, 100149. [Google Scholar] [CrossRef]
- Williams, M.S.; Beech, B.M.; Griffith, D.M.; Thorpe, R.J., Jr. The Association between Hypertension and Race/Ethnicity among Breast Cancer Survivors. J. Racial. Ethn. Health Disparities 2020, 7, 1172–1177. [Google Scholar] [CrossRef]
- Lopez-Neyman, S.M.; Davis, K.; Zohoori, N.; Broughton, K.S.; Moore, C.E.; Miketinas, D. Racial disparities and prevalence of cardiovascular disease risk factors, cardiometabolic risk factors, and cardiovascular health metrics among US adults: NHANES 2011–2018. Sci. Rep. 2022, 12, 19475. [Google Scholar] [CrossRef]
- Cai, F.; Luis, M.A.F.; Lin, X.; Wang, M.; Cai, L.; Cen, C.; Biskup, E. Anthracycline-induced cardiotoxicity in the chemotherapy treatment of breast cancer: Preventive strategies and treatment. Mol. Clin. Oncol. 2019, 11, 15–23. [Google Scholar] [CrossRef]
- Thotamgari, S.R.; Sheth, A.R.; Grewal, U.S. Racial Disparities in Cardiovascular Disease Among Patients with Cancer in the United States: The Elephant in the Room. EClinicalMedicine 2022, 44, 101297. [Google Scholar] [CrossRef] [PubMed]
- Carnethon, M.R.; Pu, J.; Howard, G.; Albert, M.A.; Anderson, C.A.M.; Bertoni, A.G.; Mujahid, M.S.; Palaniappan, L.; Taylor, H.A., Jr.; Willis, M.; et al. Cardiovascular Health in African Americans: A Scientific Statement From the American Heart Association. Circulation 2017, 136, e393–e423. [Google Scholar] [CrossRef] [PubMed]
- Ferdinand, K.C.; Yadav, K.; Nasser, S.A.; Clayton-Jeter, H.D.; Lewin, J.; Cryer, D.R.; Senatore, F.F. Disparities in hypertension and cardiovascular disease in blacks: The critical role of medication adherence. J. Clin. Hypertens. 2017, 19, 1015–1024. [Google Scholar] [CrossRef] [PubMed]
- Kenchaiah, S.; Evans, J.C.; Levy, D.; Wilson, P.W.; Benjamin, E.J.; Larson, M.G.; Kannel, W.B.; Vasan, R.S. Obesity and the risk of heart failure. N. Engl. J. Med. 2002, 347, 305–313. [Google Scholar] [CrossRef] [PubMed]
- Mitra, M.S.; Donthamsetty, S.; White, B.; Mehendale, H.M. High fat diet-fed obese rats are highly sensitive to doxorubicin-induced cardiotoxicity. Toxicol. Appl. Pharmacol. 2008, 231, 413–422. [Google Scholar] [CrossRef] [PubMed]
- Benjamin, E.J.; Blaha, M.J.; Chiuve, S.E.; Cushman, M.; Das, S.R.; Deo, R.; de Ferranti, S.D.; Floyd, J.; Fornage, M.; Gillespie, C.; et al. Heart Disease and Stroke Statistics-2017 Update: A Report From the American Heart Association. Circulation 2017, 135, e146–e603. [Google Scholar] [CrossRef]
- Gomez, S.; Blumer, V.; Rodriguez, F. Unique Cardiovascular Disease Risk Factors in Hispanic Individuals. Curr. Cardiovasc. Risk Rep. 2022, 16, 53–61. [Google Scholar] [CrossRef]
- Aguayo-Mazzucato, C.; Diaque, P.; Hernandez, S.; Rosas, S.; Kostic, A.; Caballero, A.E. Understanding the growing epidemic of type 2 diabetes in the Hispanic population living in the United States. Diabetes Metab. Res. Rev. 2019, 35, e3097. [Google Scholar] [CrossRef]
- Foy, C.G.; Hsu, F.C.; Haffner, S.M.; Norris, J.M.; Rotter, J.I.; Henkin, L.F.; Bryer-Ash, M.; Chen, Y.D.; Wagenknecht, L.E. Visceral fat and prevalence of hypertension among African Americans and Hispanic Americans: Findings from the IRAS family study. Am. J. Hypertens. 2008, 21, 910–916. [Google Scholar] [CrossRef]
- de Azambuja, E.; McCaskill-Stevens, W.; Francis, P.; Quinaux, E.; Crown, J.P.; Vicente, M.; Giuliani, R.; Nordenskjold, B.; Gutierez, J.; Andersson, M.; et al. The effect of body mass index on overall and disease-free survival in node-positive breast cancer patients treated with docetaxel and doxorubicin-containing adjuvant chemotherapy: The experience of the BIG 02-98 trial. Breast Cancer Res. Treat. 2010, 119, 145–153. [Google Scholar] [CrossRef] [PubMed]
- Ladoire, S.; Dalban, C.; Roche, H.; Spielmann, M.; Fumoleau, P.; Levy, C.; Martin, A.L.; Ecarnot, F.; Bonnetain, F.; Ghiringhelli, F. Effect of obesity on disease-free and overall survival in node-positive breast cancer patients in a large French population: A pooled analysis of two randomised trials. Eur. J. Cancer 2014, 50, 506–516. [Google Scholar] [CrossRef]
- Herman, D.R.; Ganz, P.A.; Petersen, L.; Greendale, G.A. Obesity and cardiovascular risk factors in younger breast cancer survivors: The Cancer and Menopause Study (CAMS). Breast Cancer Res. Treat. 2005, 93, 13–23. [Google Scholar] [CrossRef] [PubMed]
- Sun, H.; Zou, J.; Chen, L.; Zu, X.; Wen, G.; Zhong, J. Triple-negative breast cancer and its association with obesity. Mol. Clin. Oncol. 2017, 7, 935–942. [Google Scholar] [CrossRef] [PubMed]
- Guenancia, C.; Lefebvre, A.; Cardinale, D.; Yu, A.F.; Ladoire, S.; Ghiringhelli, F.; Zeller, M.; Rochette, L.; Cottin, Y.; Vergely, C. Obesity As a Risk Factor for Anthracyclines and Trastuzumab Cardiotoxicity in Breast Cancer: A Systematic Review and Meta-Analysis. J. Clin. Oncol. 2016, 34, 3157–3165. [Google Scholar] [CrossRef]
- Kabore, E.G.; Guenancia, C.; Vaz-Luis, I.; Di Meglio, A.; Pistilli, B.; Coutant, C.; Cottu, P.; Lesur, A.; Petit, T.; Dalenc, F.; et al. Association of body mass index and cardiotoxicity related to anthracyclines and trastuzumab in early breast cancer: French CANTO cohort study. PLoS Med. 2019, 16, e1002989. [Google Scholar] [CrossRef]
- Selvin, E.; Parrinello, C.M.; Sacks, D.B.; Coresh, J. Trends in prevalence and control of diabetes in the United States, 1988–1994 and 1999–2010. Ann. Intern. Med. 2014, 160, 517–525. [Google Scholar] [CrossRef]
- Tan, Y.; Zhang, Z.; Zheng, C.; Wintergerst, K.A.; Keller, B.B.; Cai, L. Mechanisms of diabetic cardiomyopathy and potential therapeutic strategies: Preclinical and clinical evidence. Nat. Rev. Cardiol. 2020, 17, 585–607. [Google Scholar] [CrossRef]
- Zhang, M.; Yang, H.; Xu, C.; Jin, F.; Zheng, A. Risk Factors for Anthracycline-Induced Cardiotoxicity in Breast Cancer Treatment: A Meta-Analysis. Front. Oncol. 2022, 12, 899782. [Google Scholar] [CrossRef]
- Elhussein, A.; Anderson, A.; Bancks, M.P.; Coday, M.; Knowler, W.C.; Peters, A.; Vaughan, E.M.; Maruthur, N.M.; Clark, J.M.; Pilla, S.; et al. Racial/ethnic and socioeconomic disparities in the use of newer diabetes medications in the Look AHEAD study. Lancet Reg. Health Am. 2022, 6, 100111. [Google Scholar] [CrossRef]
- Sachinidis, A.; Nikolic, D.; Stoian, A.P.; Papanas, N.; Tarar, O.; Rizvi, A.A.; Rizzo, M. Cardiovascular outcomes trials with incretin-based medications: A critical review of data available on GLP-1 receptor agonists and DPP-4 inhibitors. Metabolism 2020, 111, 154343. [Google Scholar] [CrossRef] [PubMed]
- Russo, M.; Della Sala, A.; Tocchetti, C.G.; Porporato, P.E.; Ghigo, A. Metabolic Aspects of Anthracycline Cardiotoxicity. Curr. Treat. Options Oncol. 2021, 22, 18. [Google Scholar] [CrossRef] [PubMed]
- Xia, P.; Chen, J.; Liu, Y.; Fletcher, M.; Jensen, B.C.; Cheng, Z. Doxorubicin induces cardiomyocyte apoptosis and atrophy through cyclin-dependent kinase 2-mediated activation of forkhead box O1. J. Biol. Chem. 2020, 295, 4265–4276. [Google Scholar] [CrossRef] [PubMed]
- Gallagher, E.J.; Fei, K.; Feldman, S.M.; Port, E.; Friedman, N.B.; Boolbol, S.K.; Killelea, B.; Pilewskie, M.; Choi, L.; King, T.; et al. Insulin resistance contributes to racial disparities in breast cancer prognosis in US women. Breast Cancer Res. 2020, 22, 40. [Google Scholar] [CrossRef]
- Han, H.; Guo, W.; Shi, W.; Yu, Y.; Zhang, Y.; Ye, X.; He, J. Hypertension and breast cancer risk: A systematic review and meta-analysis. Sci. Rep. 2017, 7, 44877. [Google Scholar] [CrossRef] [PubMed]
- Gu, A.; Yue, Y.; Desai, R.P.; Argulian, E. Racial and Ethnic Differences in Antihypertensive Medication Use and Blood Pressure Control Among US Adults With Hypertension: The National Health and Nutrition Examination Survey, 2003 to 2012. Circ. Cardiovasc. Qual. Outcomes 2017, 10, e003166. [Google Scholar] [CrossRef]
- Kotwinski, P.; Smith, G.; Cooper, J.; Sanders, J.; Ma, L.; Teis, A.; Kotwinski, D.; Mythen, M.; Pennell, D.J.; Jones, A.; et al. Body Surface Area and Baseline Blood Pressure Predict Subclinical Anthracycline Cardiotoxicity in Women Treated for Early Breast Cancer. PLoS ONE 2016, 11, e0165262. [Google Scholar] [CrossRef]
- Fogarassy, G.; Vathy-Fogarassy, A.; Kenessey, I.; Kasler, M.; Forster, T. Risk prediction model for long-term heart failure incidence after epirubicin chemotherapy for breast cancer—A real-world data-based, nationwide classification analysis. Int. J. Cardiol. 2019, 285, 47–52. [Google Scholar] [CrossRef]
- Vaitiekus, D.; Muckiene, G.; Vaitiekiene, A.; Maciuliene, D.; Vaiciuliene, D.; Ambrazeviciute, G.; Sereikaite, L.; Verikas, D.; Jurkevicius, R.; Juozaityte, E. Impact of Arterial Hypertension on Doxorubicin-Based Chemotherapy-Induced Subclinical Cardiac Damage in Breast Cancer Patients. Cardiovasc. Toxicol. 2020, 20, 321–327. [Google Scholar] [CrossRef]
- Agarwala, A.; Bekele, N.; Deych, E.; Rich, M.W.; Hussain, A.; Jones, L.K.; Sturm, A.C.; Aspry, K.; Nowak, E.; Ahmad, Z.; et al. Racial Disparities in Modifiable Risk Factors and Statin Usage in Black Patients With Familial Hypercholesterolemia. J. Am. Heart Assoc. 2021, 10, e020890. [Google Scholar] [CrossRef]
- Kalra, D.K. Bridging the Racial Disparity Gap in Lipid-Lowering Therapy. J. Am. Heart Assoc. 2021, 10, e019533. [Google Scholar] [CrossRef] [PubMed]
- Yun, U.J.; Lee, J.H.; Shim, J.; Yoon, K.; Goh, S.H.; Yi, E.H.; Ye, S.K.; Lee, J.S.; Lee, H.; Park, J.; et al. Anti-cancer effect of doxorubicin is mediated by downregulation of HMG-Co A reductase via inhibition of EGFR/Src pathway. Lab. Investig. 2019, 99, 1157–1172. [Google Scholar] [CrossRef] [PubMed]
- Mensah, G.A. Cardiovascular Diseases in African Americans: Fostering Community Partnerships to Stem the Tide. Am. J. Kidney Dis. 2018, 72, S37–S42. [Google Scholar] [CrossRef] [PubMed]
- Limdi, N.A.; Howard, V.J.; Higginbotham, J.; Parton, J.; Safford, M.M.; Howard, G. US Mortality: Influence of Race, Geography and Cardiovascular Risk Among Participants in the Population-Based REGARDS Cohort. J. Racial. Ethn. Health Disparities 2016, 3, 599–607. [Google Scholar] [CrossRef]
- Mensah, G.A.; Goff, D.C.; Gibbons, G.H. Cardiovascular Mortality Differences-Place Matters. JAMA 2017, 317, 1955–1957. [Google Scholar] [CrossRef]
- LaVeist, T.; Pollack, K.; Thorpe, R., Jr.; Fesahazion, R.; Gaskin, D. Place, not race: Disparities dissipate in southwest Baltimore when blacks and whites live under similar conditions. Health Aff. 2011, 30, 1880–1887. [Google Scholar] [CrossRef]
- Williams, R.A. Cardiovascular disease in African American women: A health care disparities issue. J. Natl. Med. Assoc. 2009, 101, 536–540. [Google Scholar] [CrossRef]
- Connor, A.E.; Dibble, K.E.; Visvanathan, K. Lifestyle factors in Black female breast cancer survivors-Descriptive results from an online pilot study. Front. Public Health 2023, 11, 1072741. [Google Scholar] [CrossRef]
- Rodriguez, C.J.; Allison, M.; Daviglus, M.L.; Isasi, C.R.; Keller, C.; Leira, E.C.; Palaniappan, L.; Pina, I.L.; Ramirez, S.M.; Rodriguez, B.; et al. Status of cardiovascular disease and stroke in Hispanics/Latinos in the United States: A science advisory from the American Heart Association. Circulation 2014, 130, 593–625. [Google Scholar] [CrossRef]
- Armenian, S.H.; Yang, D.; Teh, J.B.; Atencio, L.C.; Gonzales, A.; Wong, F.L.; Leisenring, W.M.; Forman, S.J.; Nakamura, R.; Chow, E.J. Prediction of cardiovascular disease among hematopoietic cell transplantation survivors. Blood Adv. 2018, 2, 1756–1764. [Google Scholar] [CrossRef]
- Chow, E.J.; Chen, Y.; Kremer, L.C.; Breslow, N.E.; Hudson, M.M.; Armstrong, G.T.; Border, W.L.; Feijen, E.A.; Green, D.M.; Meacham, L.R.; et al. Individual prediction of heart failure among childhood cancer survivors. J. Clin. Oncol. 2015, 33, 394–402. [Google Scholar] [CrossRef]
- Altena, R.; Bajalica-Lagercrantz, S.; Papakonstantinou, A. Pharmacogenomics for Prediction of Cardiovascular Toxicity: Landscape of Emerging Data in Breast Cancer Therapies. Cancers 2022, 14, 4665. [Google Scholar] [CrossRef]
- Visscher, H.; Ross, C.J.; Rassekh, S.R.; Sandor, G.S.; Caron, H.N.; van Dalen, E.C.; Kremer, L.C.; van der Pal, H.J.; Rogers, P.C.; Rieder, M.J.; et al. Validation of variants in SLC28A3 and UGT1A6 as genetic markers predictive of anthracycline-induced cardiotoxicity in children. Pediatr. Blood Cancer 2013, 60, 1375–1381. [Google Scholar] [CrossRef]
- Kabore, E.G.; Macdonald, C.; Kabore, A.; Didier, R.; Arveux, P.; Meda, N.; Boutron-Ruault, M.C.; Guenancia, C. Risk Prediction Models for Cardiotoxicity of Chemotherapy Among Patients With Breast Cancer: A Systematic Review. JAMA Netw. Open 2023, 6, e230569. [Google Scholar] [CrossRef]
- Bhatia, S. Genetics of Anthracycline Cardiomyopathy in Cancer Survivors: JACC: CardioOncology State-of-the-Art Review. JACC CardioOncol. 2020, 2, 539–552. [Google Scholar] [CrossRef]
- Barzaman, K.; Karami, J.; Zarei, Z.; Hosseinzadeh, A.; Kazemi, M.H.; Moradi-Kalbolandi, S.; Safari, E.; Farahmand, L. Breast cancer: Biology, biomarkers, and treatments. Int. Immunopharmacol. 2020, 84, 106535. [Google Scholar] [CrossRef] [PubMed]
- Kohler, B.A.; Sherman, R.L.; Howlader, N.; Jemal, A.; Ryerson, A.B.; Henry, K.A.; Boscoe, F.P.; Cronin, K.A.; Lake, A.; Noone, A.M.; et al. Annual Report to the Nation on the Status of Cancer, 1975–2011, Featuring Incidence of Breast Cancer Subtypes by Race/Ethnicity, Poverty, and State. J. Natl. Cancer Inst. 2015, 107, djv048. [Google Scholar] [CrossRef] [PubMed]
- Gapstur, S.M.; Dupuis, J.; Gann, P.; Collila, S.; Winchester, D.P. Hormone receptor status of breast tumors in black, Hispanic, and non-Hispanic white women. An analysis of 13,239 cases. Cancer 1996, 77, 1465–1471. [Google Scholar] [CrossRef]
- Hayanga, A.J.; Newman, L.A. Investigating the phenotypes and genotypes of breast cancer in women with African ancestry: The need for more genetic epidemiology. Surg. Clin. N. Am. 2007, 87, 551–568. [Google Scholar] [CrossRef]
- Newman, L.A. Disparities in breast cancer and african ancestry: A global perspective. Breast J. 2015, 21, 133–139. [Google Scholar] [CrossRef]
- Linnenbringer, E.; Gehlert, S.; Geronimus, A.T. Black-White Disparities in Breast Cancer Subtype: The Intersection of Socially Patterned Stress and Genetic Expression. AIMS Public Health 2017, 4, 526–556. [Google Scholar] [CrossRef] [PubMed]
- Nachman, M.W.; Bauer, V.L.; Crowell, S.L.; Aquadro, C.F. DNA variability and recombination rates at X-linked loci in humans. Genetics 1998, 150, 1133–1141. [Google Scholar] [CrossRef] [PubMed]
- Mihalcea, D.J.; Florescu, M.; Vinereanu, D. Mechanisms and Genetic Susceptibility of Chemotherapy-Induced Cardiotoxicity in Patients With Breast Cancer. Am. J. Ther. 2017, 24, e3–e11. [Google Scholar] [CrossRef] [PubMed]
- Lunardi, M.; Al-Habbaa, A.; Abdelshafy, M.; Davey, M.G.; Elkoumy, A.; Ganly, S.; Elzomor, H.; Cawley, C.; Sharif, F.; Crowley, J.; et al. Genetic and RNA-related molecular markers of trastuzumab-chemotherapy-associated cardiotoxicity in HER2 positive breast cancer: A systematic review. BMC Cancer 2022, 22, 396. [Google Scholar] [CrossRef]
- Visscher, H.; Ross, C.J.; Rassekh, S.R.; Barhdadi, A.; Dube, M.P.; Al-Saloos, H.; Sandor, G.S.; Caron, H.N.; van Dalen, E.C.; Kremer, L.C.; et al. Pharmacogenomic prediction of anthracycline-induced cardiotoxicity in children. J. Clin. Oncol. 2012, 30, 1422–1428. [Google Scholar] [CrossRef] [PubMed]
- Vulsteke, C.; Pfeil, A.M.; Maggen, C.; Schwenkglenks, M.; Pettengell, R.; Szucs, T.D.; Lambrechts, D.; Dieudonne, A.S.; Hatse, S.; Neven, P.; et al. Clinical and genetic risk factors for epirubicin-induced cardiac toxicity in early breast cancer patients. Breast Cancer Res. Treat. 2015, 152, 67–76. [Google Scholar] [CrossRef] [PubMed]
- Ruiz-Pinto, S.; Pita, G.; Martin, M.; Alonso-Gordoa, T.; Barnes, D.R.; Alonso, M.R.; Herraez, B.; Garcia-Miguel, P.; Alonso, J.; Perez-Martinez, A.; et al. Exome array analysis identifies ETFB as a novel susceptibility gene for anthracycline-induced cardiotoxicity in cancer patients. Breast Cancer Res. Treat. 2018, 167, 249–256. [Google Scholar] [CrossRef] [PubMed]
- Vaitiekus, D.; Muckiene, G.; Vaitiekiene, A.; Sereikaite, L.; Inciuraite, R.; Insodaite, R.; Cepuliene, D.; Kupcinskas, J.; Ugenskiene, R.; Jurkevicius, R.; et al. HFE Gene Variants’Impact on Anthracycline-Based Chemotherapy-Induced Subclinical Cardiotoxicity. Cardiovasc. Toxicol. 2021, 21, 59–66. [Google Scholar] [CrossRef]
- Serie, D.J.; Crook, J.E.; Necela, B.M.; Dockter, T.J.; Wang, X.; Asmann, Y.W.; Fairweather, D.; Bruno, K.A.; Colon-Otero, G.; Perez, E.A.; et al. Genome-wide association study of cardiotoxicity in the NCCTG N9831 (Alliance) adjuvant trastuzumab trial. Pharmacogenet. Genom. 2017, 27, 378–385. [Google Scholar] [CrossRef]
- Wells, Q.S.; Veatch, O.J.; Fessel, J.P.; Joon, A.Y.; Levinson, R.T.; Mosley, J.D.; Held, E.P.; Lindsay, C.S.; Shaffer, C.M.; Weeke, P.E.; et al. Genome-wide association and pathway analysis of left ventricular function after anthracycline exposure in adults. Pharmacogenet. Genom. 2017, 27, 247–254. [Google Scholar] [CrossRef]
- Loizidou, M.A.; Michael, T.; Neuhausen, S.L.; Newbold, R.F.; Marcou, Y.; Kakouri, E.; Daniel, M.; Papadopoulos, P.; Malas, S.; Kyriacou, K.; et al. Genetic polymorphisms in the DNA repair genes XRCC1, XRCC2 and XRCC3 and risk of breast cancer in Cyprus. Breast Cancer Res. Treat. 2008, 112, 575–579. [Google Scholar] [CrossRef] [PubMed]
- Kim, K.; Kang, S.B.; Chung, H.H.; Kim, J.W.; Park, N.H.; Song, Y.S. XRCC1 Arginine194Tryptophan and GGH-401Cytosine/Thymine polymorphisms are associated with response to platinum-based neoadjuvant chemotherapy in cervical cancer. Gynecol. Oncol. 2008, 111, 509–515. [Google Scholar] [CrossRef] [PubMed]
- Bewick, M.A.; Conlon, M.S.; Lafrenie, R.M. Polymorphisms in XRCC1, XRCC3, and CCND1 and survival after treatment for metastatic breast cancer. J. Clin. Oncol. 2006, 24, 5645–5651. [Google Scholar] [CrossRef] [PubMed]
- Apetoh, L.; Ghiringhelli, F.; Tesniere, A.; Obeid, M.; Ortiz, C.; Criollo, A.; Mignot, G.; Maiuri, M.C.; Ullrich, E.; Saulnier, P.; et al. Toll-like receptor 4-dependent contribution of the immune system to anticancer chemotherapy and radiotherapy. Nat. Med. 2007, 13, 1050–1059. [Google Scholar] [CrossRef] [PubMed]
- DeMichele, A.; Gray, R.; Horn, M.; Chen, J.; Aplenc, R.; Vaughan, W.P.; Tallman, M.S. Host genetic variants in the interleukin-6 promoter predict poor outcome in patients with estrogen receptor-positive, node-positive breast cancer. Cancer Res. 2009, 69, 4184–4191. [Google Scholar] [CrossRef]
- Xu, Y.; Yao, L.; Ouyang, T.; Li, J.; Wang, T.; Fan, Z.; Lin, B.; Lu, Y.; Xie, Y. p53 Codon 72 polymorphism predicts the pathologic response to neoadjuvant chemotherapy in patients with breast cancer. Clin. Cancer Res. 2005, 11, 7328–7333. [Google Scholar] [CrossRef]
- Fagerholm, R.; Hofstetter, B.; Tommiska, J.; Aaltonen, K.; Vrtel, R.; Syrjakoski, K.; Kallioniemi, A.; Kilpivaara, O.; Mannermaa, A.; Kosma, V.M.; et al. NAD(P)H:quinone oxidoreductase 1 NQO1*2 genotype (P187S) is a strong prognostic and predictive factor in breast cancer. Nat. Genet. 2008, 40, 844–853. [Google Scholar] [CrossRef]
- Thomas, M.; Kalita, A.; Labrecque, S.; Pim, D.; Banks, L.; Matlashewski, G. Two polymorphic variants of wild-type p53 differ biochemically and biologically. Mol. Cell. Biol. 1999, 19, 1092–1100. [Google Scholar] [CrossRef]
- Katkoori, V.R.; Jia, X.; Shanmugam, C.; Wan, W.; Meleth, S.; Bumpers, H.; Grizzle, W.E.; Manne, U. Prognostic significance of p53 codon 72 polymorphism differs with race in colorectal adenocarcinoma. Clin. Cancer Res. 2009, 15, 2406–2416. [Google Scholar] [CrossRef]
- Siegel, D.; Anwar, A.; Winski, S.L.; Kepa, J.K.; Zolman, K.L.; Ross, D. Rapid polyubiquitination and proteasomal degradation of a mutant form of NAD(P)H:quinone oxidoreductase 1. Mol. Pharmacol. 2001, 59, 263–268. [Google Scholar] [CrossRef]
- Taylor, B.D.; Darville, T.; Ferrell, R.E.; Ness, R.B.; Haggerty, C.L. Racial variation in toll-like receptor variants among women with pelvic inflammatory disease. J. Infect. Dis. 2013, 207, 940–946. [Google Scholar] [CrossRef]
- Giannitrapani, L.; Soresi, M.; Giacalone, A.; Campagna, M.E.; Marasa, M.; Cervello, M.; Marasa, S.; Montalto, G. IL-6-174G/C polymorphism and IL-6 serum levels in patients with liver cirrhosis and hepatocellular carcinoma. OMICS 2011, 15, 183–186. [Google Scholar] [CrossRef]
- Hoffmann, S.C.; Stanley, E.M.; Cox, E.D.; DiMercurio, B.S.; Koziol, D.E.; Harlan, D.M.; Kirk, A.D.; Blair, P.J. Ethnicity greatly influences cytokine gene polymorphism distribution. Am. J. Transpl. 2002, 2, 560–567. [Google Scholar] [CrossRef] [PubMed]
- Bu, T.; Liu, L.; Sun, Y.; Zhao, L.; Peng, Y.; Zhou, S.; Li, L.; Chen, S.; Gao, Y. XRCC1 Arg399Gln polymorphism confers risk of breast cancer in American population: A meta-analysis of 10846 cases and 11723 controls. PLoS ONE 2014, 9, e86086. [Google Scholar] [CrossRef] [PubMed]
- Deshmukh, S.K.; Azim, S.; Ahmad, A.; Zubair, H.; Tyagi, N.; Srivastava, S.K.; Bhardwaj, A.; Singh, S.; Rocconi, R.P.; Singh, A.P. Biological basis of cancer health disparities: Resources and challenges for research. Am. J. Cancer Res. 2017, 7, 1–12. [Google Scholar] [PubMed]
- Kim, G.; Pastoriza, J.M.; Condeelis, J.S.; Sparano, J.A.; Filippou, P.S.; Karagiannis, G.S.; Oktay, M.H. The Contribution of Race to Breast Tumor Microenvironment Composition and Disease Progression. Front. Oncol. 2020, 10, 1022. [Google Scholar] [CrossRef]
- Webb Hooper, M.; Napoles, A.M.; Perez-Stable, E.J. COVID-19 and Racial/Ethnic Disparities. JAMA 2020, 323, 2466–2467. [Google Scholar] [CrossRef]
- Bibbins-Domingo, K. This Time Must Be Different: Disparities During the COVID-19 Pandemic. Ann. Intern. Med. 2020, 173, 233–234. [Google Scholar] [CrossRef]
- Singh, G.K.; Jemal, A. Socioeconomic and Racial/Ethnic Disparities in Cancer Mortality, Incidence, and Survival in the United States, 1950–2014: Over Six Decades of Changing Patterns and Widening Inequalities. J. Environ. Public Health 2017, 2017, 2819372. [Google Scholar] [CrossRef]
- Singh GK, M.B.; Hankey, B.F.; Edwards, B.K. Area Socioeconomic Variations in U.S. Cancer Incidence, Mortality, Stage, Treatment, and Survival, 1975–1999; NCI Cancer Surveillance Monograph Series, Number 4; National Cancer Institute: Bethesda, MD, USA, 2003. [Google Scholar]
- Keegan, T.H.M.; Kushi, L.H.; Li, Q.; Brunson, A.; Chawla, X.; Chew, H.K.; Malogolowkin, M.; Wun, T. Cardiovascular disease incidence in adolescent and young adult cancer survivors: A retrospective cohort study. J. Cancer Surviv. 2018, 12, 388–397. [Google Scholar] [CrossRef]
- Singh, G.K.; Williams, S.D.; Siahpush, M.; Mulhollen, A. Socioeconomic, Rural-Urban, and Racial Inequalities in US Cancer Mortality: Part I-All Cancers and Lung Cancer and Part II-Colorectal, Prostate, Breast, and Cervical Cancers. J. Cancer Epidemiol. 2011, 2011, 107497. [Google Scholar] [CrossRef] [PubMed]
- Angier, H.E.; Marino, M.; Springer, R.J.; Schmidt, T.D.; Huguet, N.; DeVoe, J.E. The Affordable Care Act improved health insurance coverage and cardiovascular-related screening rates for cancer survivors seen in community health centers. Cancer 2020, 126, 3303–3311. [Google Scholar] [CrossRef] [PubMed]
- Harris, L.; Batist, G.; Belt, R.; Rovira, D.; Navari, R.; Azarnia, N.; Welles, L.; Winer, E.; Group, T.D.S. Liposome-encapsulated doxorubicin compared with conventional doxorubicin in a randomized multicenter trial as first-line therapy of metastatic breast carcinoma. Cancer 2002, 94, 25–36. [Google Scholar] [CrossRef]
- Smith, L.A.; Cornelius, V.R.; Plummer, C.J.; Levitt, G.; Verrill, M.; Canney, P.; Jones, A. Cardiotoxicity of anthracycline agents for the treatment of cancer: Systematic review and meta-analysis of randomised controlled trials. BMC Cancer 2010, 10, 337. [Google Scholar] [CrossRef] [PubMed]
- Wallace, J.; Lollo, A.; Duchowny, K.A.; Lavallee, M.; Ndumele, C.D. Disparities in Health Care Spending and Utilization Among Black and White Medicaid Enrollees. JAMA Health Forum. 2022, 3, e221398. [Google Scholar] [CrossRef]
- Mahajan, S.; Caraballo, C.; Lu, Y.; Valero-Elizondo, J.; Massey, D.; Annapureddy, A.R.; Roy, B.; Riley, C.; Murugiah, K.; Onuma, O.; et al. Trends in Differences in Health Status and Health Care Access and Affordability by Race and Ethnicity in the United States, 1999–2018. JAMA 2021, 326, 637–648. [Google Scholar] [CrossRef]
- Grette, K.V.; White, A.L.; Awad, E.K.; Scalici, J.M.; Young-Pierce, J.; Rocconi, R.P.; Jones, N.L. Not immune to inequity: Minority under-representation in immunotherapy trials for breast and gynecologic cancers. Int. J. Gynecol. Cancer 2021, 31, 1403–1407. [Google Scholar] [CrossRef]
- Loree, J.M.; Anand, S.; Dasari, A.; Unger, J.M.; Gothwal, A.; Ellis, L.M.; Varadhachary, G.; Kopetz, S.; Overman, M.J.; Raghav, K. Disparity of Race Reporting and Representation in Clinical Trials Leading to Cancer Drug Approvals From 2008 to 2018. JAMA Oncol. 2019, 5, e191870. [Google Scholar] [CrossRef]
- Geller, S.E.; Adams, M.G.; Carnes, M. Adherence to federal guidelines for reporting of sex and race/ethnicity in clinical trials. J. Womens Health 2006, 15, 1123–1131. [Google Scholar] [CrossRef]
- Geller, S.E.; Koch, A.; Pellettieri, B.; Carnes, M. Inclusion, analysis, and reporting of sex and race/ethnicity in clinical trials: Have we made progress? J. Womens Health 2011, 20, 315–320. [Google Scholar] [CrossRef]
- Ma, M.A.; Gutierrez, D.E.; Frausto, J.M.; Al-Delaimy, W.K. Minority Representation in Clinical Trials in the United States: Trends Over the Past 25 Years. Mayo Clin. Proc. 2021, 96, 264–266. [Google Scholar] [CrossRef] [PubMed]
- Gany, F.; Melnic, I.; Ramirez, J.; Wu, M.; Li, Y.; Paolantonio, L.; Roberts-Eversley, N.; Blinder, V.; Leng, J. The association between housing and food insecurity among medically underserved cancer patients. Support. Care Cancer 2021, 29, 7765–7774. [Google Scholar] [CrossRef]
- Phillips, S.; Raskin, S.E.; Harrington, C.B.; Brazinskaite, R.; Gany, F.M. “You Have to Keep a Roof Over Your Head”: A Qualitative Study of Housing Needs Among Patients With Cancer in New York City. J. Oncol. Pract. 2019, 15, e677–e689. [Google Scholar] [CrossRef] [PubMed]
- Mendoza, J.A.; Miller, C.A.; Martin, K.J.; Resnicow, K.; Iachan, R.; Faseru, B.; McDaniels-Davidson, C.; Deng, Y.; Martinez, M.E.; Demark-Wahnefried, W.; et al. Examining the Association of Food Insecurity and Being Up-to-Date for Breast and Colorectal Cancer Screenings. Cancer Epidemiol. Biomarkers Prev. 2022, 31, 1017–1025. [Google Scholar] [CrossRef] [PubMed]
- Patel, K.G.; Borno, H.T.; Seligman, H.K. Food insecurity screening: A missing piece in cancer management. Cancer 2019, 125, 3494–3501. [Google Scholar] [CrossRef]
- Gucciardi, E.; Vahabi, M.; Norris, N.; Del Monte, J.P.; Farnum, C. The Intersection between Food Insecurity and Diabetes: A Review. Curr. Nutr. Rep. 2014, 3, 324–332. [Google Scholar] [CrossRef]
- Seligman, H.K.; Jacobs, E.A.; Lopez, A.; Tschann, J.; Fernandez, A. Food insecurity and glycemic control among low-income patients with type 2 diabetes. Diabetes Care 2012, 35, 233–238. [Google Scholar] [CrossRef]
- Simkhovich, B.Z.; Kleinman, M.T.; Kloner, R.A. Particulate air pollution and coronary heart disease. Curr. Opin. Cardiol. 2009, 24, 604–609. [Google Scholar] [CrossRef]
- Lamas, G.A.; Ujueta, F.; Navas-Acien, A. Lead and Cadmium as Cardiovascular Risk Factors: The Burden of Proof Has Been Met. J. Am. Heart Assoc. 2021, 10, e018692. [Google Scholar] [CrossRef]
- Alamolhodaei, N.S.; Shirani, K.; Karimi, G. Arsenic cardiotoxicity: An overview. Environ. Toxicol. Pharmacol. 2015, 40, 1005–1014. [Google Scholar] [CrossRef]
- Cykert, S.; Eng, E.; Manning, M.A.; Robertson, L.B.; Heron, D.E.; Jones, N.S.; Schaal, J.C.; Lightfoot, A.; Zhou, H.; Yongue, C.; et al. A Multi-faceted Intervention Aimed at Black-White Disparities in the Treatment of Early Stage Cancers: The ACCURE Pragmatic Quality Improvement trial. J. Natl. Med. Assoc. 2020, 112, 468–477. [Google Scholar] [CrossRef]
- Loehrer, A.P.; Cevallos, P.C.; Jimenez, R.T.; Wong, S.L. Reporting on Race and Racial Disparities in Breast Cancer: The Neglect of Racism as a Driver of Inequitable Care. Ann. Surg. 2023, 277, 329–334. [Google Scholar] [CrossRef] [PubMed]
- Johnson, W.A.; Pieters, H.C. Intimate Partner Violence Among Women Diagnosed With Cancer. Cancer Nurs. 2016, 39, 87–96. [Google Scholar] [CrossRef] [PubMed]
- Flaherty, R.L.; Falcinelli, M.; Flint, M.S. Stress and drug resistance in cancer. Cancer Drug Resist. 2019, 2, 773–786. [Google Scholar] [CrossRef] [PubMed]
- Goodman, C.R.; Sato, T.; Peck, A.R.; Girondo, M.A.; Yang, N.; Liu, C.; Yanac, A.F.; Kovatich, A.J.; Hooke, J.A.; Shriver, C.D.; et al. Steroid induction of therapy-resistant cytokeratin-5-positive cells in estrogen receptor-positive breast cancer through a BCL6-dependent mechanism. Oncogene 2016, 35, 1373–1385. [Google Scholar] [CrossRef]
- Vignjevic Petrinovic, S.; Milosevic, M.S.; Markovic, D.; Momcilovic, S. Interplay between stress and cancer-A focus on inflammation. Front. Physiol. 2023, 14, 1119095. [Google Scholar] [CrossRef] [PubMed]
- Eldridge, L.; Berrigan, D. Structural Racism and Triple-Negative Breast Cancer Among Black and White Women in the United States. Health Equity 2022, 6, 116–123. [Google Scholar] [CrossRef]
- Williams, D.R.; Rucker, T.D. Understanding and addressing racial disparities in health care. Health Care Financ. Rev. 2000, 21, 75–90. [Google Scholar]
- Cene, C.W.; Viswanathan, M.; Fichtenberg, C.M.; Sathe, N.A.; Kennedy, S.M.; Gottlieb, L.M.; Cartier, Y.; Peek, M.E. Racial Health Equity and Social Needs Interventions: A Review of a Scoping Review. JAMA Netw. Open 2023, 6, e2250654. [Google Scholar] [CrossRef]
- Bauer, G.R.; Churchill, S.M.; Mahendran, M.; Walwyn, C.; Lizotte, D.; Villa-Rueda, A.A. Intersectionality in quantitative research: A systematic review of its emergence and applications of theory and methods. SSM Popul. Health 2021, 14, 100798. [Google Scholar] [CrossRef]
- Homan, P.; Brown, T.H.; King, B. Structural Intersectionality as a New Direction for Health Disparities Research. J. Health Soc. Behav. 2021, 62, 350–370. [Google Scholar] [CrossRef] [PubMed]
- Boen, C.; Keister, L.; Aronson, B. Beyond Net Worth: Racial Differences in Wealth Portfolios and Black-White Health Inequality across the Life Course. J. Health Soc. Behav. 2020, 61, 153–169. [Google Scholar] [CrossRef]
- Farhud, D.D. Impact of Lifestyle on Health. Iran J. Public Health 2015, 44, 1442–1444. [Google Scholar] [PubMed]
- Patel, N.A.; Kianoush, S.; Jia, X.; Nambi, V.; Koh, S.; Patel, J.; Saeed, A.; Ahmed, A.I.; Al-Mallah, M.; Agarwala, A.; et al. Racial/Ethnic Disparities and Determinants of Sufficient Physical Activity Levels. Kans J. Med. 2022, 15, 267–272. [Google Scholar] [CrossRef]
- Ford, M.C.; Gordon, N.P.; Howell, A.; Green, C.E.; Greenspan, L.C.; Chandra, M.; Mellor, R.G.; Lo, J.C. Obesity Severity, Dietary Behaviors, and Lifestyle Risks Vary by Race/Ethnicity and Age in a Northern California Cohort of Children with Obesity. J. Obes. 2016, 2016, 4287976. [Google Scholar] [CrossRef]
- Guo, H.; Wu, H.; Sajid, A.; Li, Z. Whole grain cereals: The potential roles of functional components in human health. Crit. Rev. Food Sci. Nutr. 2022, 62, 8388–8402. [Google Scholar] [CrossRef]
- Hoy, M.K.; Goldman, J.D. Fiber intake of the U.S. population: What We Eat in America, NHANES 2009–2010. In FSRG Dietary Data Briefs; United States Department of Agriculture (USDA): Beltsville, MD, USA, 2010. [Google Scholar]
- Lin, B.H.; Guthrie, J.; Smith, T. Dietary Quality by Food Source and Demographics in the United States, 1977–2018; USDA, Economic Research Service: Beltsville, MD, USA, 2023. [Google Scholar]
- Dunn, C.G.; Gao, K.J.; Soto, M.J.; Bleich, S.N. Disparities in Adult Fast-Food Consumption in the U.S. by Race and Ethnicity, National Health and Nutrition Examination Survey 2017–2018. Am. J. Prev. Med. 2021, 61, e197–e201. [Google Scholar] [CrossRef] [PubMed]
- Smit, E.; Nieto, F.J.; Crespo, C.J.; Mitchell, P. Estimates of animal and plant protein intake in US adults: Results from the Third National Health and Nutrition Examination Survey, 1988–1991. J. Am. Diet. Assoc. 1999, 99, 813–820. [Google Scholar] [CrossRef] [PubMed]
- Dubowitz, T.; Heron, M.; Bird, C.E.; Lurie, N.; Finch, B.K.; Basurto-Dávila, R.; Hale, L.; Escarce, J.J. Neighborhood socioeconomic status and fruit and vegetable intake among whites, blacks, and Mexican Americans in the United States. Am. J. Clin. Nutr. 2008, 87, 1883–1891. [Google Scholar] [CrossRef]
- Zhang, X.Y.; Yang, K.L.; Li, Y.; Zhao, Y.; Jiang, K.W.; Wang, Q.; Liu, X.N. Can Dietary Nutrients Prevent Cancer Chemotherapy-Induced Cardiotoxicity? An Evidence Mapping of Human Studies and Animal Models. Front. Cardiovasc. Med. 2022, 9, 921609. [Google Scholar] [CrossRef] [PubMed]
- Dent, S.F.; Kikuchi, R.; Kondapalli, L.; Ismail-Khan, R.; Brezden-Masley, C.; Barac, A.; Fradley, M. Optimizing Cardiovascular Health in Patients With Cancer: A Practical Review of Risk Assessment, Monitoring, and Prevention of Cancer Treatment-Related Cardiovascular Toxicity. Am. Soc. Clin. Oncol. Educ. Book 2020, 40, 501–515. [Google Scholar] [CrossRef]
- Byrd, D.A.; Agurs-Collins, T.; Berrigan, D.; Lee, R.; Thompson, F.E. Racial and Ethnic Differences in Dietary Intake, Physical Activity, and Body Mass Index (BMI) Among Cancer Survivors: 2005 and 2010 National Health Interview Surveys (NHIS). J. Racial Ethn. Health Disparities 2017, 4, 1138–1146. [Google Scholar] [CrossRef]
- Smith, A.W.; Alfano, C.M.; Reeve, B.B.; Irwin, M.L.; Bernstein, L.; Baumgartner, K.; Bowen, D.; McTiernan, A.; Ballard-Barbash, R. Race/ethnicity, physical activity, and quality of life in breast cancer survivors. Cancer Epidemiol. Biomarkers Prev. 2009, 18, 656–663. [Google Scholar] [CrossRef] [PubMed]
- August, K.J.; Sorkin, D.H. Racial/ethnic disparities in exercise and dietary behaviors of middle-aged and older adults. J. Gen. Intern. Med. 2011, 26, 245–250. [Google Scholar] [CrossRef]
- Powell, L.M. Slater, S.; Chaloupka, F.J. The relationship between community physical activity settings and race, ethnicity and socioeconomic status. Evid. Based Prev. Med. 2004, 1, 135–144. [Google Scholar]
- Ahmed, A.A.; Patel, K.; Nyaku, M.A.; Kheirbek, R.E.; Bittner, V.; Fonarow, G.C.; Filippatos, G.S.; Morgan, C.J.; Aban, I.B.; Mujib, M.; et al. Risk of Heart Failure and Death After Prolonged Smoking Cessation: Role of Amount and Duration of Prior Smoking. Circ. Heart Fail. 2015, 8, 694–701. [Google Scholar] [CrossRef]
- Nguyen-Grozavu, F.T.; Pierce, J.P.; Sakuma, K.K.; Leas, E.C.; McMenamin, S.B.; Kealey, S.; Benmarhnia, T.; Emery, S.L.; White, M.M.; Fagan, P.; et al. Widening disparities in cigarette smoking by race/ethnicity across education level in the United States. Prev. Med. 2020, 139, 106220. [Google Scholar] [CrossRef]
- Zeinomar, N.; Qin, B.; Amin, S.; Lin, Y.; Xu, B.; Chanumolu, D.; Omene, C.O.; Pawlish, K.S.; Demissie, K.; Ambrosone, C.B.; et al. Association of Cigarette Smoking and Alcohol Consumption With Subsequent Mortality Among Black Breast Cancer Survivors in New Jersey. JAMA Netw. Open 2023, 6, e2252371. [Google Scholar] [CrossRef]
- John, E.M.; McGuire, V.; Kurian, A.W.; Koo, J.; Shariff-Marco, S.; Gomez, S.L.; Cheng, I.; Keegan, T.H.M.; Kwan, M.L.; Bernstein, L.; et al. Racial/Ethnic Disparities in Survival after Breast Cancer Diagnosis by Estrogen and Progesterone Receptor Status: A Pooled Analysis. Cancer Epidemiol. Biomarkers Prev. 2021, 30, 351–363. [Google Scholar] [CrossRef]
- Parada, H., Jr.; Sun, X.; Tse, C.K.; Olshan, A.F.; Troester, M.A.; Conway, K. Active smoking and survival following breast cancer among African American and non-African American women in the Carolina Breast Cancer Study. Cancer Causes Control 2017, 28, 929–938. [Google Scholar] [CrossRef]
- Padron-Monedero, A.; Tannenbaum, S.L.; Koru-Sengul, T.; Miao, F.; Hansra, D.; Lee, D.J.; Byrne, M.M. Smoking and survival in female breast cancer patients. Breast Cancer Res. Treat. 2015, 150, 395–403. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
{kind=link}
| Study | Design | Population | Treatment Dose | Cardiotoxicity Outcomes | Conclusion |
|---|---|---|---|---|---|
| Toure et al., 2022 [57] | Retrospective observational study | 8604 (274 African American and 8330 White participants) | Doxorubicin (dose ranged from 400 mg/m2 to 700 mg/m2) | Congestive heart failure (CHF) was detected in 27.8% of White participants and 32.5% of African Americans. | Significant differences between African Americans and White patients in hazard of incident CHF and cumulative incidence of incident CHF. |
| Collin et al., 2020 [58] | Prospective observational study | 8503 (3580 African American and 4923 non-Hispanic White (NHW) participants) | Not specified | Anthracyclines were associated with a greater hazard ratio in African Americans (HR, 1.45) than in White breast cancer survivors (HR, 0.86); data were not statistically significant. | Disparity in chemotherapy-induced cardiotoxicity between African American and White breast cancer survivors contributed to the racial disparity in overall survival between these groups. |
| Troeschel et al., 2019 [28] | Retrospective observational study | 407,587 (36,458 NHW) and 43,562 African American) | Not specified | The 20-year cumulative incidence of CVD-related mortality was 13.3% in African American women and 8.9% in NHW. Higher hazard ratio of cardiovascular mortality in African American breast cancer survivors compared with White breast cancer survivors (HR = 2.73 for those less than 50 and 1.72 for those aged 55 to 68 years). | CVD-related mortality was significantly higher among African American than NHW breast cancer survivors, especially the young. |
| Berkman et al., 2014 [59] | Retrospective observational study | 67,514 (54,518 White and 6113 African American participants) | Not specified | Higher hazard ratio of cardiovascular mortality in African American t cancer survivors compared with White breast cancer survivors (HR = 14.99 for the age group 40–49, HR = 6.43 for the age group 50–59, and HR = 2.26 for the age group 60–69). | Cardiovascular mortality was significantly higher in African American breast cancer survivors, especially among the young. |
| Braithwaite et al., 2009 [27] | Retrospective observational study | 1254 (416 African American and 838 White participants) | Not specified | All-cause mortality was 39.7% in African Americans vs. 33.3% in White patients. The association between hypertension and all-cause survival accounted for 30% of the racial disparity in this outcome. | Hypertension is an independent predictor of the disparity between African American and White breast cancer survivors in cardiovascular outcomes and survival. |
| Hasan et al., 2004 [26] | Retrospective observational study | 499 (100 African Americans and 399 White patients) | The median of cumulative doxorubicin dose infused over 48 h is 374 mg/m2; the range is between 264 and 580 mg/m2 | Higher incidence of doxorubicin-induced cardiotoxicity (LVEF less than 45%) among African American patients (7%) compared to White patients (2.5%). | Doxorubicin-induced cardiotoxicity is more in African American than in White patients. |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Balaji, S.; Antony, A.K.; Tonchev, H.; Scichilone, G.; Morsy, M.; Deen, H.; Mirza, I.; Ali, M.M.; Mahmoud, A.M. Racial Disparity in Anthracycline-induced Cardiotoxicity in Breast Cancer Patients. Biomedicines 2023, 11, 2286. https://doi.org/10.3390/biomedicines11082286
Balaji S, Antony AK, Tonchev H, Scichilone G, Morsy M, Deen H, Mirza I, Ali MM, Mahmoud AM. Racial Disparity in Anthracycline-induced Cardiotoxicity in Breast Cancer Patients. Biomedicines. 2023; 11(8):2286. https://doi.org/10.3390/biomedicines11082286
Chicago/Turabian StyleBalaji, Swetha, Antu K. Antony, Harry Tonchev, Giorgia Scichilone, Mohammed Morsy, Hania Deen, Imaduddin Mirza, Mohamed M. Ali, and Abeer M. Mahmoud. 2023. "Racial Disparity in Anthracycline-induced Cardiotoxicity in Breast Cancer Patients" Biomedicines 11, no. 8: 2286. https://doi.org/10.3390/biomedicines11082286
APA StyleBalaji, S., Antony, A. K., Tonchev, H., Scichilone, G., Morsy, M., Deen, H., Mirza, I., Ali, M. M., & Mahmoud, A. M. (2023). Racial Disparity in Anthracycline-induced Cardiotoxicity in Breast Cancer Patients. Biomedicines, 11(8), 2286. https://doi.org/10.3390/biomedicines11082286