1. Introduction
Psoriasis (PS) is a chronic, inflammatory, autoimmune disease affecting 1–3% of the population worldwide [
1,
2]. The main characteristic is the production of skin lesions, but it is also associated with potentially disabling pathologies, such as erectile dysfunction in 35% of patients and arthropathy in 40% [
3,
4,
5,
6,
7,
8]. Consequently, psoriasis is considered a systemic entity that severely impacts the quality of life of patients [
9].
Etiology is not completely defined; however, it is believed that different factors are involved [
10,
11]. Regarding genetics, it has been observed that there are multiple chromosomal loci associated with susceptibility to psoriasis (PSORS), the most prominent being PSORS1, responsible for 50% of the heritability of the disease [
12]. In addition, the incidence of psoriasis is different according to ethnicity, and higher among relatives and even more so among monozygotic twins [
13]. The presence of the human leukocyte antigen HLA-Cw6 is particularly associated with phenotypic features, along with early development and course of the disease [
14,
15].
Genetic and environmental factors such as stress, infections, or unhealthy lifestyle habits predispose to the onset of the pathology, while abnormalities in cutaneous immune responses are responsible for the development and maintenance of psoriatic inflammation [
10,
14]. When plasmacytoid dendritic cells, keratinocytes, natural killer cells, and macrophages are activated they secrete various cytokines (tumor necrosis factor and Interleukin 1, respectively) that stimulate myeloid dendritic cells [
16]. The activated dendritic cells promote the production of a cytokine cascade that activates keratinocyte proliferation in the epidermis. Consequently, hyperproliferation of keratinocytes in the epidermis and vascular endothelium occurs, resulting in epidermal hyperplasia typical of psoriatic lesions [
11].
There are different types of psoriasis, but the most prevalent is “psoriasis vulgaris or plaque psoriasis” characterized by clinical manifestations in the form of erythematous plaques on the scalp, elbows, knees and back covered with whitish scales [
17,
18,
19]. The severity of the lesions is measured with the indicators of psoriasis area severity index (PASI), body surface area (BSA), and dermatologic quality-of-life index (DLQI). When these indicators are greater than 10, moderate–severe psoriasis is considered [
20]. The treatments employed are aimed at blocking the inflammatory response [
21]. Pharmacological treatment is chosen according to the severity, in mild psoriasis the treatment is mainly based on topical and symptomatic therapy [
22,
23]. However, in cases of moderate–severe psoriasis, treatment with systemic therapy (methotrexate, cyclosporine, acitretin, apremilast, fumaric acid esters), phototherapy, or photochemotherapy is indicated [
9,
24,
25]. In patients diagnosed with moderate–severe psoriasis who do not respond to systemic treatment or who are contraindicated, treatment with biologics is used [
20]. Generally, the drug most frequently used in the treatment of moderate-to-severe PS is methotrexate (MTX) at low doses, because of the benefits it shows (proven effectiveness, low cost, relatively simple administration, and its usefulness in combination with other treatments) [
26]. Furthermore, it can be administered orally or subcutaneously, the latter route being the more advantageous, with better absorption and greater bioavailability [
27,
28].
Methotrexate is an antimetabolite with antiproliferative, anti-inflammatory, and immunosuppressive activity. Although the mechanism of action at low doses is not clear, it is related to the ability to form intracellular polyglutamates and to increased adenosine formation due to inhibition of the ATIC (5-aminoimidazole-4-carboxamide ribonucleotide formyltransferase/IMP cyclohydrolase) enzyme, which leads to apoptosis in activated lymphocytes or to inhibition of the activation and expression of certain adhesion molecules in them [
29,
30,
31]. Consequently, the action of MTX may be conditioned at various points on the metabolic pathway [
32,
33,
34].
This drug has proved effective, reaching PASI75 and PASI90 after 16 and 24 weeks of treatment. However, it is frequently associated with reversible adverse effects (AEs) which entail temporary interruption of treatment or modification of the dose [
35]. Long-term studies show that AEs occur in around 61–95% of patients [
36]. The most common AEs are nausea, anorexia, and asthenia, depending on the dose and usually occurring at the start of therapy [
25].
Moreover, prolonged use of MTX is associated with hepatotoxicity and hematological, renal, pulmonary, and cutaneous toxicity, among others [
37]. Specifically, long-term treatment with MTX is associated with progressive and dose-dependent hepatotoxicity. Previous studies have observed that 23–33% of patients show an increase in liver enzyme levels; however, in the absence of excessive alcohol consumption, it rarely causes clinically significant liver damage [
38]. They have also observed that it may cause hematological toxicity through hematopoietic suppression of MTX, specifically pancytopenia, which is reversible with dose reduction or temporary withdrawal of MTX [
39,
40]. In 3% of the patients studied, renal toxicity occurred in prolonged treatment with MTX [
37,
40]. Pulmonary toxicity has also been described as a risk associated with MTX treatment; in particular, there are reports of pulmonary fibrosis and pneumonitis [
26]. Severe skin reactions were observed in patients with long-term MTX; in particular, 4% of the patients studied showed alopecia [
40,
41]. Finally, it is important to note the association of MTX treatment with a higher incidence of certain malignancies, such as lymphoma [
41].
Despite the risks involved in using MTX, it has been observed that AEs limit treatment in only 6.9% of patients treated with MTX for 6 months, and therefore the risk-benefit profile of MTX is acceptable [
42]. However, it is crucial to conduct exhaustive pharmacotherapeutic follow-ups of patients receiving treatment with MTX and to use folic acid supplementation [
43].
In conclusion, although low-dose MTX treatment in patients diagnosed with moderate-to-severe PS is safe and effective, certain patients do not attain an optimum response or they experience various degrees of toxicity [
44]. This variability in response and toxicity may be due to genetic factors. Interindividual variations in the genes implicated in the disease environment of the condition, pharmacokinetics, pharmacodynamics, metabolism, or in the mechanism of action of MTX may explain the emergence of adverse effects in certain patients treated with the same therapeutic conditions [
45]. Specifically, genetic polymorphisms in the membrane efflux transporters responsible for the intracellular entry of MTX (
ABCC1-4, ABCB1, and
ABCG2), as well as other genes involved in the physiopathogeny of the disease have proved to play a crucial role in interindividual variability in response to and toxicity from MTX [
46].
In particular, the
ABCC1 gene is located on chromosome 16 and encodes the ABCC1 protein, also known as multidrug-resistance-associated protein 1 (MRP1). It is found mainly in the basolateral plasma membranes of the enterocytes transporting endogenous substances, as well as xenobiotics and their metabolites [
46,
47,
48]. Genetic polymorphisms in
ABCC1 (rs35592 T>C; rs246240 A>G, rs2238476 G>A) have been associated with response to and toxicity from MTX in psoriasis patients [
49].
Similarly, the
ABCG2 gene, on chromosome 4, codes for a membrane transporter characterized by being essentially a xenobiotic transporter that plays an important part in resistance to numerous drugs, such as MTX. The ABCG2 protein transports MTX and its forms of polyglutamate, specifically polyglutamate 2 and 3, and therefore plays a key role in MTX’s mechanism of action [
50]. Previous studies have found an association between response to and toxicity from MTX treatment in patients diagnosed with PS and the po-lymorphism of this gene (
ABCG2 rs13120400, C>T) [
50]. Consequently, genetic alterations in
ABCC1 and
ABCG2 may modify the metabolism of MTX and lead to variability in the toxicity of this drug.
On the other hand, the
FOXP3 gene, located on the X chromosome, encodes a protein from the fork-winged helix family of transcription factors which plays an essential role in modulating regulatory T cells and can act as a transcriptional repressor or activator depending on its interactions with other transcription factors, histones, acetylases, and deacetylases [
51,
52]. Alterations in
FOXP3 (rs3761548; G>C/T/A) can potentiate the inflammatory cascade in psoriasis and consequently not respond to and/or provoke AEs due to MTX treatment [
53,
54].
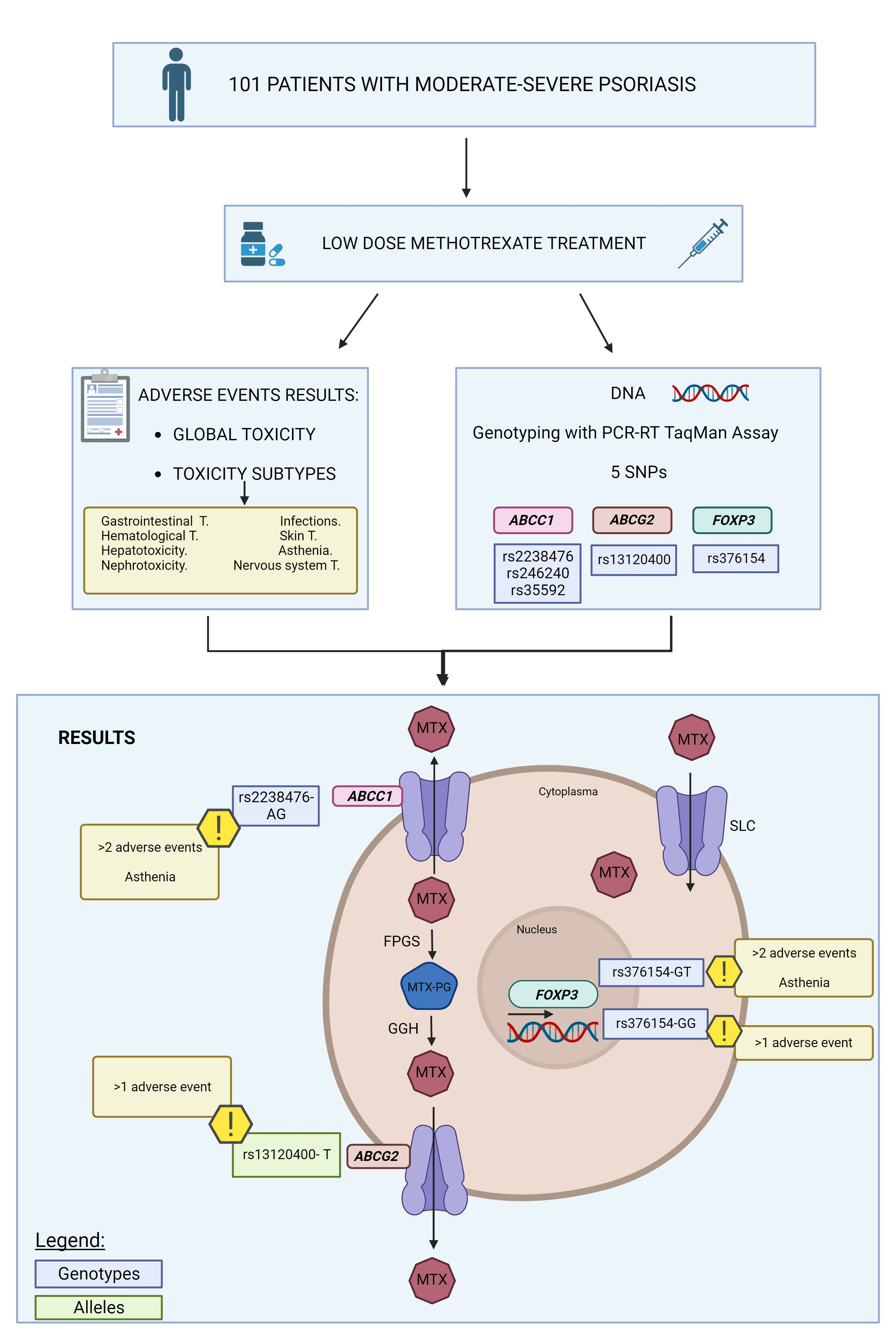
Based on all the foregoing, the object of this study was to evaluate the influence of polymorphisms of the ABCC1, ABCG2, and FOXP3 genes on the development of toxicity from treatment with MTX in moderate-to-severe psoriasis.
2. Materials and Methods
2.1. Study Design
Retrospective observational cohort study.
2.2. Study Subjects
The study included 101 Caucasian patients, over the age of 18, diagnosed with moderate-to-severe PS (BSA and PASI > 10), under treatment with MTX as monotherapy or in combination with biologic medications, for at least two months, from the Dermatology Department of the HUVN, during the period between January 2019 and November 2020. The starting dose of oral MTX was 15 mg/week, in combination with folic acid (5 mg/week, administered 24 h after the MTX), a dose approved in clinical practice guidelines [
55].
2.3. Sociodemographic and Clinical Variables
The sociodemographic variables collected were sex, age at the start of MTX therapy, family history, and smoking and drinking status. We also collected data on the clinical features of the PS, including the type of psoriasis (plaque, pustular, inverse, guttate, or a combination of different types of psoriasis: plaque and guttate, plaque and pustular, plaque and inverse, plaque, guttate and inverse) and the location of the lesions (scalp and face, nails, palmoplantar, torso, and upper and lower extremities or flexures). In addition, we studied the development of psoriatic arthritis, concomitant diseases, therapy adherence, duration of MTX treatment, route of administration of MTX, concomitant medication, and maximum dose of MTX (mg/week).
The adverse reactions collected were classified as gastrointestinal toxicity (nausea, vomiting, diarrhea, and stomatitis), hepatotoxicity (appearance of abnormalities in hepatic parameters [ALT/AST, GGT, total bilirubin, procollagen peptide], exacerbation or reactivation of hepatitis, fibrosis, or cirrhosis), hematological toxicity (anemia, leukopenia, thrombocytopenia, and/or pancytopenia), asthenia, infections, neurological toxicity (dizziness, headache disorders), skin toxicity (hair loss, skin rash), nephrotoxicity (appearance of abnormalities in renal parameters [creatinine, urea, uric acid] or renal disorders).
2.4. Sample Processing and Genotyping
2.4.1. DNA Isolation
DNA was obtained from saliva samples with buccal swabs (OCR-100 kit), after the inclusion of the patients and signing of the informed consent. Subsequently, DNA extraction was performed, using the QIAamp DNA Mini Kit (Qiagen GmbH, Hilden, Germany), following the manufacturer’s instructions for the purification of DNA from saliva, and stored at −20 °C. To check DNA concentration and purity values, a NanoDrop 2000 UV spectrophotometer was used with an absorbance ratio of 280/260 and 280/230.
2.4.2. Detection of Gene Polymorphisms
The ABCC1 rs35592 (TaqMan assay ID C___1003671_10), ABCC1 rs246240 (assay ID C___1003698_10), ABCC1 rs2238476 (assay ID C___16172578_10), ABCG2 rs13120400 (assay ID C___9510480_10), and FOXP3 rs3761548 (assay ID C___27476877_10) gene polymorphisms were determined by real-time polymerase chain reaction (PCR) using TaqMan® probes (ABI Applied Biosystems, 7300 Real-Time PCR System, Foster City, CA, USA).
2.5. Toxicity Variables
Toxicity was evaluated according to the common terminology criteria for adverse events (CTCAE) using version 5.0 (U.S. Department of Health and Human Services (HHS), Washington DC, USA). The severity of the adverse events was classified as presence (toxicity grade 1–4) or absence (no presence of toxicity). General toxicity was defined as present when there was at least one adverse event (grade 1–4). The occurrence of more than one and more than two adverse events was also analyzed.
2.6. Statistical Analysis
Statistical analysis was performed using the freely available software R 3.5.1 (R Foundation for Statistical Computing, Vienna, Austria). Normal quantitative variables were expressed as mean (±standard deviation) and as median (p50) and percentiles (25 and 75) for non-normal variables. Normality analysis was performed by applying the Kolmogorov–Smirnov test. Pearson’s chi-square test was used for bivariate analysis between toxicity and polymorphisms. Fisher’s exact test was applied for associations between toxicity and qualitative variables, while Student’s t-test was used for normal quantitative variables, and the Mann–Whitney test for non-normal variables. The association with SNPs was evaluated in multiple models (genotypic, dominant, and recessive), which were defined as follows: genotypic (DD vs. Dd vs. dd), dominant ((DD, Dd) vs. dd) and recessive (DD vs. (Dd, dd)), where D is the major allele (wild-type) and d the minor allele (variant).
The adjusted odds ratio (OR) and 95% confidence interval (95% CI) were obtained by logistic or linear regression from multivariate analysis. The Hosmer–Lemeshow test was applied to determine the goodness-of-fit of each model. In addition, the omnibus test and the Cox-Snell and Nagelkerke r2 coefficients were calculated. We considered a statistically significant probability with a value of 0.05 or less.
For the analysis of polymorphisms, haplotype frequencies were calculated, as well as Hardy-Weinberg equilibrium and linkage disequilibrium (Lewontin’s D (D’) and linkage disequilibrium coefficient (r2)). This genetic analysis was performed with the PLINK application for genome-wide association analysis and SNPstats, a web-based tool for association study analysis [
56,
57,
58,
59].
4. Discussion
Methotrexate is the most commonly used conventional systemic medication in patients diagnosed with moderate-to-severe psoriasis [
55]. Despite its widespread use, great interindividual variability has been observed regarding the appearance of adverse effects, and this, to a great extent, limits the effectiveness of the therapy in these patients [
60,
61]. Single-nucleotide polymorphisms (SNPs) in genes for enzymes involved in the metabolism and mechanism of action of MTX have been proposed as a potential cause of this variability [
62]. Particularly noteworthy among them are those involved in the transport of MTX across the cell membrane, which could determine the passage of MTX into and out of the cell, and thus its pharmacodynamics and pharmacokinetics [
63]. In this study, 101 patients diagnosed with moderate-to-severe PS and treated with MTX, as monotherapy or combined with biologic therapy, were evaluated to determine the influence of SNPs in the
ABCC1,
ABCG2, and
FOXP3 genes on the presence of toxicity due to MTX.
Various sociodemographic, clinical, and genetic factors may influence pharmacological response to and toxicity from MTX [
64,
65]. In our study, the appearance of possible grade 1–4 adverse effects was associated with the development of psoriatic arthritis, after the diagnosis of psoriasis. In line with these results, a study conducted on 235 Asian patients (China) diagnosed with the psoriatic disease (PS = 107; psoriatic arthritis = 128), under treatment with MTX, found a higher incidence of adverse events such as dizziness (9.4% vs. 0.9%,
p = 0.007), gastrointestinal symptoms (25.0% vs. 12.1%,
p = 0.01), and hepatotoxicity (26.6% vs. 15.0%,
p = 0.04) in patients with psoriatic arthritis than in those with PS [
66]. Furthermore, the route of administration of MTX was also associated with a higher prevalence of toxicity in our patients. Specifically, patients to whom MTX was administered subcutaneously or those in whom the route of administration had been changed showed a higher risk of adverse effects appearing (asthenia, gastrointestinal toxicity, and neurotoxicity) during MTX therapy, According to our results, a study conducted in 291 Caucasian patients (Netherlands) diagnosed with rheumatoid or psoriatic arthritis and under therapy with MTX at low doses showed a higher prevalence of intolerance in patients with parenteral administration of MTX (parenteral [20.6%] vs. oral [6.2%],
p < 0.001) [
67]. In contrast to these results, a study conducted in 28 Caucasian patients (Egypt) diagnosed with psoriasis and under treatment with oral (
n = 14) and subcutaneous (
n = 14) MTX showed a higher prevalence of gastrointestinal toxicity (71.4% vs. 14.3%) and hepatotoxicity (21.3% vs. 7.1%) in patients with oral administration of MTX [
68]. An investigation conducted in 55 Caucasian patients (Czech Republic) diagnosed with juvenile idiopathic arthritis and treated with MTX found no significant differences between the route of administration of MTX and the risk of adverse effects (parenteral vs. oral,
p = 0.236) [
69].
In our study, female sex was associated with a higher risk of undergoing adverse events, specifically gastrointestinal toxicity. A study carried out on 809 Caucasian patients diagnosed with psoriasis (
n = 690) and rheumatoid arthritis (
n = 119) and treated with MTX also found a higher risk of hepatotoxicity in women (hazard ratio [HR] = 1.46,
p < 0.001) [
70]. Similarly, smoking and drinking status were found to be associated with a higher risk of gastrointestinal toxicity. In line with this, previous studies have highlighted the influence of alcohol and tobacco consumption on the mechanism of action of MTX, since they could interfere with the mechanism of transporting the drug towards the cell interior, therefore modifying the pharmacological response and producing toxicity [
71].
Previous studies have revealed the influence of various SNPs on the toxicity of MTX in patients with autoimmune diseases, such as
MTHFR, MTR, ABCC1, ABCC2, and
ABCG2 [
72,
73,
74]. However, the existing evidence on the influence of genetics on MTX toxicity in patients with PS is limited. In our study, we found an association between the
ABCG2 rs13120400 SNP and the appearance of adverse effects after administration of MTX. Specifically, following the multivariate analysis, the
ABCG2 rs13120400-T allele was found to be associated with the risk of grade 1–4 toxicity, adjusted for the development of psoriatic arthritis. Similarly, patients carrying the
ABCG2 rs13120400-TT genotype showed a higher risk of hepatotoxicity from MTX. In line with our results, Warren et al. carried out a study in 374 Caucasian patients (United Kingdom) diagnosed with moderate-to-severe PS and treated with MTX, finding an association between the
ABCG2 rs13120400-TT genotype and lesser effectiveness of MTX (TT vs. CC/CT,
p = 0.03) [
49]. However, its association with toxicity from the drug was not evaluated [
49]. The transporter ABCG2 is composed of six transmembrane domains and is in hepatocytes, enterocytes, and renal cells, among others [
63,
75]. Previous research has suggested that ABCG2 is involved in the transport of MTX and its toxic metabolite, 7-hydroxymethotrexate (7OH-MTX), in the liver and kidney, finding that SNPs in these genes could cause variations in the activity of ABCG2, contributing to toxicity in patients treated with MTX [
76,
77,
78]. Specifically, the
ABCG2 rs13120400 SNP is encoded in intronic region 9 of the gene and its biological effect has not been studied to date [
79]. This SNP could influence the transcription and translation processes of the ABCG2 protein, giving rise to a non-functional molecule and affecting the cellular transport of MTX [
79].
Another of the SNPs evaluated in this study was
ABCC1 rs2238476, located in intron 23 of the
ABCC1 gene, which codes for the membrane transporter protein ABCC1, responsible for the transport of MTX, among other drugs [
49]. The main task of ABCC1 is to protect cells against toxic effects and contribute to the barrier function [
80]. In our study, patients carrying the
ABCC1 rs2238476-AG genotype showed a higher risk of grade 1–4 adverse effects of MTX. In addition, this genotype was associated with the development of asthenia, after the multivariate analysis, as well as the appearance of nephrotoxicity in our patients. In line with this, a study with 374 Caucasian patients (United Kingdom) diagnosed with PS and under treatment with MTX related to the
ABCC1 rs2238476-GG genotype with a higher risk of emergence of toxicity in general (OR = 2.49; IC95% = 1.1–6.0;
p = 0.01) [
49]. This SNP could affect the protective function of the ABCC1 protein, modifying the passage of MTX out of the cells and therefore causing an intracellular accumulation of the drug, giving rise to various adverse reactions [
79]. The association of these SNPs with mRNA/protein expression has been shown in some studies. A lower expression of ABCC1 could be the cause of greater toxicity due to the accumulation of MTX inside the cells [
79].
We also found a statistically significant association between the
FOXP3 rs376154 SNP and the risk of toxicity from MTX. In the multivariate analysis, it was observed that patients carrying the
FOXP3 rs376154-GT and GG genotypes showed a higher risk of developing adverse events after the administration of MTX, specifically asthenia. Although there are no previous studies that evaluate the association of this SNP with the development of toxicity due to MTX, its influence on the efficacy of MTX has been assessed. A study conducted in 132 Caucasian patients (India) diagnosed with moderate-to-severe PS receiving MRX therapy and 57 healthy controls associated the
FOXP3 rs376154-GG and GT polymorphism with a lesser response to the drug (OR = 3.21, 95% CI = 1.50–6.87,
p = 0.003) [
81]. On the other hand, Wu Zhuo et al. carried out a study in 114 Asian patients (China) who had undergone a kidney transplant and were being treated with tacrolimus, finding that those carrying the FOXP3 rs376154-GT and TT genotypes showed a higher risk of nephrotoxicity from the drug (GT/TT vs. GG: HR = 10.71, 95% CI = 2.219–51.72,
p = 0.036) [
82]. The
FOXP3 rs376154 SNP is in the promoter region of the gene, and therefore a base change may modify the place where the transcription factors bind to the promoter, leading to defective transcription of the FOXP3 protein [
83]. In addition, the
FOXP3 gene participates in the development and regulation of regulatory T cells and may contribute to the emergence of toxicity due to MTX via the inflammatory response suppression pathway mediated by IL-10 [
82,
84,
85,
86].
Regarding the
ABCC1 rs35592 and
ABCC1 rs246240 SNPs, no significant association was observed with the variables included in our study. These results are in line with those obtained in a study with 200 Caucasian patients (Australia) diagnosed with rheumatoid arthritis and treated with MTX at low doses, where no association was found between the
ABCC1 rs35592 SNP and the presence of toxicity (
p > 0.05) [
87]. Similarly, D’Cruz et al. studied the association between the
ABCC1 rs246240 SNP and plasma levels of MTX and its toxic metabolite 7OH-MTX in 100 Caucasian patients (United Kingdom) diagnosed with rheumatoid arthritis under treatment with MTX, without finding any significant association [
88]. Conversely, Warren et al. conducted a study in 374 Caucasian patients (United Kingdom) diagnosed with moderate-to-severe PS receiving MTX therapy at low doses, finding that the patients who carried the
ABCC1 rs246240-AA genotype showed a higher risk of hepatotoxicity and gastrointestinal toxicity (OR = 2.2, 95% CI = 1.3–3.6,
p = 0.001) [
49].
Among the main limitations of our study, we should highlight the limited sample size, which may be responsible for the fact that no statistical association was found between the ABCC1 rs35592 and ABCC1 rs246240 SNPs and toxicity. Despite this, we obtained important and representative results that show the influence that certain SNPs have on the emergence of toxicity during the use of MTX in patients with moderate-to-severe PS. Thus, our sample size has a statistical power to detect genetic association of 57.44%. It is also worth emphasizing that this study was conducted with patients from the same hospital, all diagnosed with moderate-to-severe PS, according to the same therapeutic protocols, by the same team of dermatologists. This allows a high degree of homogeneity in the cohort, as well as in the collection of variables.
Further studies with larger cohorts will be required to corroborate the prognostic value of biomarkers, in particular the ABCC1, ABCG2, and FOXP3 gene polymorphisms.
These results suggest that polymorphisms in the genes encoding the enzymes that participate in the cellular transport of MTX, particularly the ABCG2 rs13120400, ABCC1 rs2238476, and FOXP3 rs376154 polymorphisms, could act as risk biomarkers for the emergence of adverse effects in patients with moderate-to-severe PS treated with MTX at low doses.

 ,
, 

{kind=link}