

Prostate-Specific Antigen as an Ultrasensitive Biomarker for Patients with Early Recurrent Prostate Cancer: How Low Shall We Go? A Systematic Review

Abstract
1. Introduction
2. Methods
2.1. Search for Studies and Analyses of the Studies
2.2. uPSA
2.3. Definitions
2.4. Statistical Analysis
3. Results
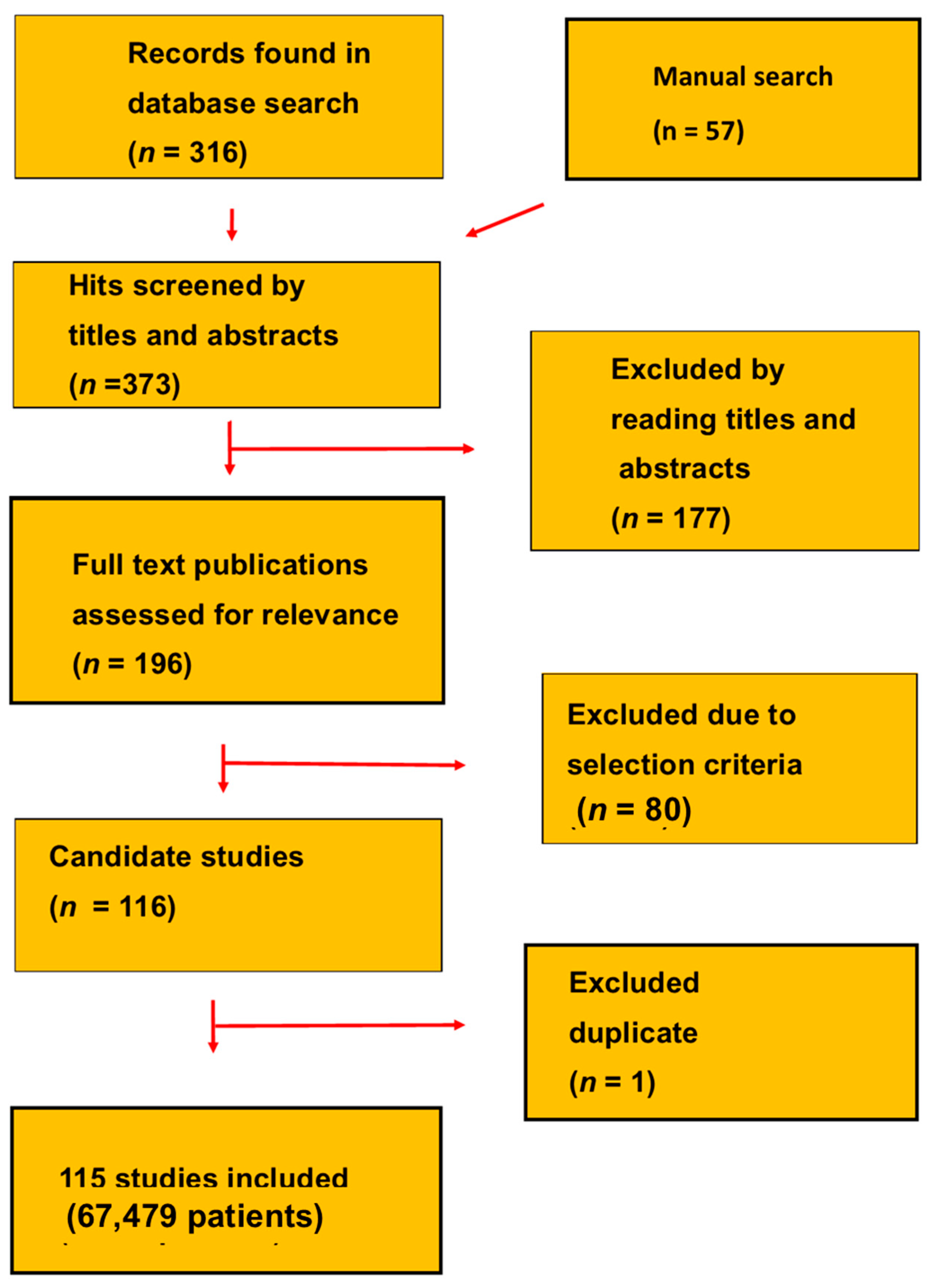
3.1. Selected Studies
3.2. uPSAs
3.3. Pre-PSAR Phase
3.4. High-Risk Nonmetastatic Castration-Resistant Prostate Cancer
4. Discussion
5. Conclusions
6. Perspectives
Supplementary Materials
Author Contributions
Funding
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Bottke, D.; Bartkowiak, D.; Schrader, M.; Wiegel, T. Radiotherapy after radical prostatectomy: Immediate or early delayed? Strahlenther. Onkol. 2012, 188, 1096–1101. [Google Scholar] [CrossRef] [PubMed]
- Pisansky, T.M.; Thompson, I.M.; Valicent, I.R.K.; D’Amico, A.V.; Selvarajah, S. Adjuvant and salvage radiotherapy after prostatectomy: ASTRO/AUA guideline amendment 2018–2019. J. Urol. 2019, 202, 533–538. [Google Scholar] [CrossRef] [PubMed]
- Daly, T.; Hickey, B.E.; Lehman, M.; Francis, D.P.; See, A.M. Adjuvant radiotherapy following radical prostatectomy for prostate cancer. Cochrane Database Syst. Rev. 2011, CD007234. [Google Scholar] [CrossRef] [PubMed]
- Cornford, P.; van den Bergh, R.C.N.; Briers, E.; Van den Broeck, T.; Cumberbatch, M.G.; De Santis, M.; Fanti, S.; Fossati, N.; Gandaglia, G.; Gillessen, S.; et al. EAU-EANM-ESTRO-ESUR-SIOG guidelines on prostate cancer. Part II-2020 Update: Treatment of relapsing and metastatic prostate cancer. Eur. Urol. 2021, 79, 263–282. [Google Scholar] [CrossRef] [PubMed]
- Vale, C.L.; Fisher, D.; Kneebone, A.; Parker, C.; Pearse, M.; Richaud, P.; Sargos, P.; Sydes, M.R.; Brawley, C.; Brihoum, M.; et al. Adjuvant or early salvage radiotherapy for the treatment of localised and locally advanced prostate cancer: A prospectively planned systematic review and meta-analysis of aggregate data. Lancet 2020, 396, 1422–1431. [Google Scholar] [CrossRef]
- Kneebone, A.; Fraser-Browne, C.; Duchesne, G.M.; Fisher, R.; Frydenberg, M.; Herschtal, A.; Williams, S.G.; Brown, C.; Delprado, W.; Haworth, A.; et al. Adjuvant radiotherapy versus early salvage radiotherapy following radical prostatectomy (TROG 08.03/ANZUP RAVES): A randomised, controlled, phase 3, non-inferiority trial. Lancet Oncol. 2020, 21, 1331–1340. [Google Scholar] [CrossRef]
- Mottet, N.; van den Bergh, R.C.N.; Briers, E.; Van den Broeck, T.; Cumberbatch, M.G.; De Santis, M.; Fanti, S.; Fossati, N.; Gandaglia, G.; Gillessen, S.; et al. EAU-EANM-ESTRO-ESUR-SIOG guidelines on prostate cancer-2020 Update. Part 1: Screening, diagnosis, and local treatment with curative intent. Eur. Urol. 2021, 79, 243–262. [Google Scholar] [CrossRef]
- D’Amico, A.V.; Whittington, R.; Malkowicz, S.B.; Schultz, D.; Blank, K.; Broderick, G.A.; Tomaszewski, J.E.; Renshaw, A.A.; Kaplan, I.; Beard, C.J.; et al. Biochemical outcome after radical prostatectomy, external beam radiation therapy, or interstitial radiation therapy for clinically localized prostate cancer. JAMA 1998, 280, 969–974. [Google Scholar] [CrossRef]
- Vickers, A.J.; Brewster, S.F. PSA velocity and doubling time in diagnosis and prognosis of prostate cancer. Br. J. Med. Surg. Urol. 2012, 5, 162–168. [Google Scholar] [CrossRef]
- Dowlatshahi, S.; Abdekhodaie, M.J. Electrochemical prostate-specific antigen biosensors based on electroconductive nanomaterials and polymers. Clin. Chim. Acta 2021, 516, 111–135. [Google Scholar] [CrossRef]
- Simon, N.I.; Parker, C.; Hope, T.A.; Paller, C.J. Best approaches and updates for prostate cancer biochemical recurrence. Am. Soc. Clin. Oncol. Educ. Book 2022, 42, 352–359. [Google Scholar] [CrossRef]
- Elgamal, A.A.; Van de Voorde, W.; Van Poppel, H.; Lauweryns, J.; Baert, L. Immunohistochemical localization of prostate-specific markers within the accessory male sex glands of Cowper, Littre, and Morgagni. Urology 1994, 44, 84–90. [Google Scholar] [CrossRef]
- Olsson, A.Y.; Bjartell, A.; Lilja, H.; Lundwall, A. Expression of prostate-specific antigen (PSA) and human glandular kallikrein 2 (hK2) in ileum and other extraprostatic tissues. Int. J. Cancer 2005, 113, 290–297. [Google Scholar] [CrossRef]
- Diamandis, E.P.; Yu, H. Nonprostatic sources of prostate-specific antigen. Urol. Clin. N. Am. 1997, 24, 275–282. [Google Scholar] [CrossRef]
- Merriel, S.W.D.; Pocock, L.; Gilbert, E.; Creavin, S.; Walter, F.M.; Spencer, A.; Hamilton, W. Systematic review and meta-analysis of the diagnostic accuracy of prostate-specific antigen (PSA) for the detection of prostate cancer in symptomatic patients. BMC Med. 2022, 20, 54. [Google Scholar] [CrossRef]
- Semjonow, A.; De Angelis, G. “Ultrasensitive “ methods for prostate specific antigen (PSA): How deep should we measure ? J. Lab. Med. 2003, 27, 16–19. (In German) [Google Scholar]
- Lilja, H.; Ulmert, D.; Vickers, A.J. Prostate-specific antigen and prostate cancer: Prediction, detection and monitoring. Nat. Rev. Cancer 2008, 8, 268–278. [Google Scholar] [CrossRef]
- Dash, P. Reconnoitring the status of prostate specific antigen and its role in women. Indian J. Clin. Biochem. 2015, 30, 124–133. [Google Scholar] [CrossRef]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. Rev. Esp. Cardiol. 2021, 74, 790–799. [Google Scholar] [CrossRef]
- Bogemann, M.; Shore, N.D.; Smith, M.R.; Tammela, T.L.J.; Ulys, A.; Vjaters, E.; Polyakov, S.; Jievaltas, M.; Luz, M.; Alekseev, B.; et al. Efficacy and safety of darolutamide in patients with nonmetastatic castration-resistant prostate cancer stratified by prostate-specific antigen doubling time: Planned subgroup analysis of the phase 3 ARAMIS trial. Eur. Urol. 2023, 83, 212–221. [Google Scholar] [CrossRef] [PubMed]
- Hussain, M.; Sternberg, C.N.; Efstathiou, E.; Fizazi, K.; Shen, Q.; Lin, X.; Sugg, J.; Steinberg, J.; Noerby, B.; De Giorgi, U.; et al. Nadir prostate-specific antigen as an Independent predictor of survival outcomes: A post hoc analysis of the PROSPER randomized clinical trial. J. Urol. 2023, 209, 532–539. [Google Scholar] [CrossRef]
- Lee, E.E.; Singh, T.; Hu, C.; Han, M.; Deville, C.J.; Halthore, A.; Greco, S.; Tran, P.; DeWeese, T.; Song, D.Y. The impact of salvage radiotherapy initiation at PSA </= 0.5 ng/ml on metastasis-free survival in patients with relapsed prostate cancer following prostatectomy. Prostate 2023, 83, 190–197. [Google Scholar]
- Ozyurt, C.; Uludag, I.; Sezginturk, M.K. An ultrasensitive and disposable electrochemical aptasensor for prostate-specific antigen (PSA) detection in real serum samples. Anal. Bioanal. Chem. 2023, 415, 1123–1136. [Google Scholar] [CrossRef]
- Sutil, R.S.; Varguz-Martal, D.; De Pablos-Rodriguez, P.; Altez-Fernandes, C.A.; Lozano, A.G.-F.; Backhaus, M.R.; Abal, V.C.; Antolin, A.R. European Association of Urology biochemical recurrence risk groups after radical prostatectomy: External validation and identification of independent risk factors. Actas Urol. Esp. 2023, 47, 422–429. [Google Scholar]
- Tilki, D.; Chen, M.H.; Wu, J.; Huland, H.; Graefen, M.; Mohamad, O.; Cowan, J.E.; Feng, F.Y.; Carroll, P.R.; D’Amico, A.V. Prostate-specific antigen level at the time of salvage therapy after radical prostatectomy for prostate cancer and the risk of death. J. Clin. Oncol. 2023, 41, 2428–2435. [Google Scholar] [CrossRef]
- Ueno, Y.; Fukumori, T.; Kusuhara, Y.; Fukawa, T.; Tsuda, M.; Daizumoto, K.; Sasaki, Y.; Tomida, R.; Yamamoto, Y.; Yamaguchi, K.; et al. Prostate-specific antigen levels following brachytherapy impact late biochemical recurrence in japanese patients with localized prostate cancer. In Vivo 2023, 37, 738–746. [Google Scholar] [CrossRef]
- Wu, K.; Lai, K.; Chen, J.; Yao, J.; Zeng, S.; Jiang, T.; Si, H.; Gu, C.; Jiang, J. Ag NC and Ag NP/PorC film-based surface-enhanced raman spectroscopy-type immunoassay for ultrasensitive prostate-specific antigen detection. ACS Omega 2023, 8, 18523–18529. [Google Scholar] [CrossRef]
- Cao, X.; Liu, M.; Zhao, M.; Li, J.; Xia, J.; Zou, T.; Wang, Z. Synergetic PtNP@Co3O4 hollow nanopolyhedrals as peroxidase-like nanozymes for the dual-channel homogeneous biosensing of prostate-specific antigen. Anal. Bioanal. Chem. 2022, 414, 1921–1932. [Google Scholar] [CrossRef]
- Orlov, A.V.; Burenin, A.G.; Skirda, A.M.; Nikitin, P.I. Kinetic analysis of prostate-specific antigen interaction with monoclonal antibodies for development of a magnetic immunoassay based on nontransparent fiber structures. Molecules 2022, 27, 8077. [Google Scholar] [CrossRef]
- Saad, F.; Small, E.J.; Feng, F.Y.; Graff, J.N.; Olmos, L.D.; Hadaschik, B.A.; Oudard, S.; Londhe, A.; Bhaumik, A.; Lopez-Gitlitz, A.; et al. Deep prostate-specific antigen response following addition of apalutamide to ongoing androgen deprivation therapy and long-term clinical benefit in SPARTAN. Eur. Urol. 2022, 81, 184–192. [Google Scholar] [CrossRef]
- Shen, J.; Situ, B.; Du, X.; Wang, Z.; Hu, R.; Li, B.; Qin, A.; Tang, B.Z. Aggregation-induced emission luminogen-based dual-mode enzyme-linked immunosorbent assay for ultrasensitive detection of cancer biomarkers in a broad concentration range. ACS Sens. 2022, 7, 766–774. [Google Scholar] [CrossRef]
- Von Eyben, R.; Hoffmann, M.A.; Kapp, D.S.; Soydal, C.; Uprimny, C.; Virgolini, I.; Tuncel, M.; Gauthe, M.; von Eyben, F.E. Quality goal for salvage treatment for patients with prostate cancer at prostate-specific antigen relapse. Eur. Urol. Oncol. 2022, 5, 732–733. [Google Scholar] [CrossRef]
- Von Eyben, R.; Kapp, D.S.; Hoffmann, M.A.; Soydal, C.; Uprimny, C.; Virgolini, I.; Tuncel, M.; Gauthe, M.; von Eyben, F.E. A risk model for patients with PSA-only recurrence (biochemical recurrence) based on PSA and PSMA PET/CT: An individual patient data meta-analysis. Cancers 2023, 15, 1035. [Google Scholar] [CrossRef]
- Chung, J.J.; Jeong, J.Y.; Lee, J.Y.; Song, W.; Kang, M.; Hwn, H.; Jeon, H.G.; Jeong, B.C.; Seo, S.I.; Lee, H.M.; et al. Biochemical recurrence after radical prostatectomy according to nadir prostate specific antigen value. PLoS ONE 2021, 16, e0249709. [Google Scholar] [CrossRef]
- Jansen, B.H.E.; van Leeuwen, P.J.; Wondergem, M.; van der Sluis, T.M.; Nieuwenhuijzen, J.A.; Knol, R.J.J.; van Moorselaar, R.J.A.; van der Poel, H.G.; Oprea-Lager, D.E.; Vis, A.N. Detection of recurrent prostate cancer using prostate-specific membrane antigen positron emission tomography in patients not meeting the Phoenix criteria for biochemical recurrence after curative radiotherapy. Eur. Urol. Oncol. 2021, 4, 821–825. [Google Scholar] [CrossRef]
- Zakaria, A.S.; Schwartz, R.N.; Hodhod, A.; Couture, F.; Tholomier, C.; Shahine, H.; Negrean, C.; Guyen, D.D.; Zanaty, M.; Stolzenbach, F.; et al. Detectable prostate-specific antigen value between 0.01 and 0.1 ng/ml following robotic-assisted radical prostatectomy (RARP): Does it correlate with future biochemical recurrence? World J. Urol. 2021, 39, 1853–1860. [Google Scholar] [CrossRef]
- Akl, M.A.; El-Gharkawy, E.R.; El-Mahdy, N.A.; El-Sheikh, S.M.; Sheta, S.M. A novel nano copper complex: Potentiometry, DFT and application as a cancer prostatic biomarker for the ultrasensitive detection of human PSA. Dalton Trans. 2020, 49, 15769–15778. [Google Scholar] [CrossRef]
- Cid-Barrio, L.; Ruiz Encinar, J.; Costa-Fernandez, J.M. Catalytic gold deposition for ultrasensitive optical immunosensing of prostate specific antigen. Sensors 2020, 20, 2587. [Google Scholar] [CrossRef]
- Dess, R.T.; Sun, Y.; Jackson, W.C.; Jairath, N.K.; Kishan, A.U.; Wallington, D.G.; Mahal, B.A.; Stish, B.J.; Zumsteg, Z.S.; Den, R.B.; et al. Association of presalavage radiotherapy PSA levels after prostatectomy with outcomes of long-term antiandrogen therapy in men with prostate cancer. JAMA Oncol. 2020, 6, 735–743. [Google Scholar] [CrossRef]
- Farschi, F.; Saadati, A.; Hasanzadeh, M. A novel immunosensor for the monitoring of PSA using binding of biotinylated antibody to the prostate specific antigen based on nano-ink modified flexible paper substrate: Efficient method for diagnosis of cancer using biosensing technology. Heliyon 2020, 6, e04327. [Google Scholar]
- Ren, A.H.; Soosaipillai, A.; Mathew, A.; Nikolenko, G.; Sardesai, L.; Stengelin, M.; Diamandis, E.P. Utility of a fifth-generation ultrasensitive prostate-specific antigen assay for monitoring prostate cancer patients after radical prostatectomy with 3 years of follow-up. Clin. Chem. 2020, 66, 1329–1338. [Google Scholar] [CrossRef]
- Wang, H.M.; Huang, X.Q.; Wang, A.J.; Luo, X.; Liu, W.D.; Yuan, P.X.; Feng, J.J. Construction of efficient “on-off-on” fluorescence aptasensor for ultrasensitive detection of prostate specific antigen via covalent energy transfer between g-C3N4 quantum dots and palladium triangular plates. Anal. Chim. Acta 2020, 104, 53–59. [Google Scholar] [CrossRef]
- Bottke, D.; Bartkowiak, D.; Siegmann, A.; Thamm, R.; Bohmer, D.; Budach, V.; Wiegel, T. Effect of early salvage radiotherapy at PSA < 0.5 ng/ml and impact of post-SRT PSA nadir in post-prostatectomy recurrent prostate cancer. Prostate Cancer Prostatic Dis. 2019, 22, 344–349. [Google Scholar]
- Bryant, A.K.; McKay, R.R.; Kader, A.K.; Parsons, J.K.; Einck, J.P.; Kane, C.J.; Mundt, A.J.; Murphy, J.D.; Rose, B.S. Subcastrate testosterone nadir and clinical outcomes in intermediate- or high-risk localized prostate cancer. Int. J. Radiat. Oncol. Biol. Phys. 2019, 103, 1068–1076. [Google Scholar] [CrossRef]
- Grivas, N.; de Bruin, D.; Barwari, K.; van Muilekom, E.; Tillier, C.; van Leeuwen, P.J.; Wit, E.; Kroese, W.; van der Poel, H. Ultrasensitive prostate-specific antigen level as a predictor of biochemical progression after robot-assisted radical prostatectomy: Towards risk adapted follow-up. J. Clin. Lab. Anal. 2019, 33, e22693. [Google Scholar] [CrossRef]
- Hahn, J.; Kim, E.; You, Y.; Choi, Y.J. Colorimetric switchable linker-based bioassay for ultrasensitive detection of prostate-specific antigen as a cancer biomarker. Analyst 2019, 144, 4439–4446. [Google Scholar] [CrossRef]
- Jalalvand, A.R. Fabrication of a novel and ultrasensitive label-free electrochemical aptasensor for detection of biomarker prostate specific antigen. Int. J. Biol. Macromol. 2019, 126, 1065–1073. [Google Scholar] [CrossRef]
- Pike, L.R.G.; Wu, J.; Chen, M.H.; Loffredo, M.; Renshaw, A.A.; Pfail, J.; Kantoff, P.W.; D’Amico, A.V. Time to prostate-specific antigen nadir and the risk of death from prostate cancer following radiation and androgen deprivation therapy. Urology 2019, 126, 145–151. [Google Scholar] [CrossRef]
- Schroeder, C.; Geiger, F.; Siebert, F.A.; Baumann, R.; Bockelmann, G.; Schultze, J.; Kimmig, B.; Dunst, J.; Galalae, R. Radical dose escalation by high-dose-rate brachytherapy for localized prostate cancer-significance of prostate-specific antigen nadir level within 18 months as correlation for long-term biochemical control. Brachytherapy 2019, 18, 8–12. [Google Scholar] [CrossRef]
- Sun, Y.; Wang, C.; Zhang, H.; Zhang, Y.; Zhang, G. A non-enzymatic and label-free fluorescence bioassay for ultrasensitive detection of PSA. Molecules 2019, 24, 831. [Google Scholar] [CrossRef]
- Tian, C.; Wang, L.; Luan, F.; Zhuang, X. An electrochemiluminescence sensor for the detection of prostate protein antigen based on the graphene quantum dots infilled TiO2 nanotube arrays. Talanta 2019, 191, 103–108. [Google Scholar] [CrossRef]
- Burkhardt, O.; Neuemschwander, J.; John, H.; Randazzo, M. Does seminal-vesicle-sparing robotic radical prostatectomy influence postoperative prostate-specific antigen measured with an ultrasensitive immunoassay? Swiss Med. Wkly. 2018, 148, 14685. [Google Scholar] [CrossRef]
- Kang, J.J.; Reiter, R.E.; Steinberg, M.L.M.; King, C.R. First postprostatectomy ultrasensitive prostate-specific antigen predicts survival in patients with high-risk prostate cancer pathology. Eur. Urol. Oncol. 2018, 1, 378–385. [Google Scholar] [CrossRef]
- Yang, Y.; Yan, Q.; Liu, Q.; Li, Y.; Liu, H.; Wang, P.; Chen, L.; Zhang, D.; Li, Y.; Dong, Y. An ultrasensitive sandwich-type electrochemical immunosensor based on the signal amplification strategy of echinoidea-shaped Au@Ag-Cu2O nanoparticles for prostate specific antigen detection. Biosens. Bioelectron. 2018, 99, 450–457. [Google Scholar] [CrossRef]
- Zhou, X.; Yang, L.; Tan, X.; Zhao, G.; Xie, X.; Du, G. A robust electrochemical immunosensor based on hydroxyl pillar [5]arene@AuNPs@g-C3N4 hybrid nanomaterial for ultrasensitive detection of prostate specific antigen. Biosens. Bioelectron. 2018, 112, 31–39. [Google Scholar] [CrossRef]
- Abugharib, A.; Jackson, W.C.; Tumati, V.; Dess, R.T.; Lee, J.Y.; Zhao, S.G.; Soliman, M.; Zumsteg, Z.S.; Mehra, R.; Feng, F.Y.; et al. Very early salvage radiotherapy improves distant metastasis-free survival. J. Urol. 2017, 197, 662–668. [Google Scholar] [CrossRef]
- Heydari-Bafrooei, E.; Shamszadeh, N.S. Electrochemical bioassay development for ultrasensitive aptasensing of prostate specific antigen. Biosens. Bioelectron. 2017, 91, 284–292. [Google Scholar] [CrossRef]
- Liu, Y.; Zhang, Z.; Yu, J.; Xie, J.; Li, C.M. A concentration-dependent multicolor conversion strategy for ultrasensitive colorimetric immunoassay with the naked eye. Anal. Chim. Acta 2017, 963, 129–135. [Google Scholar] [CrossRef]
- Royce, T.J.; Chen, M.H.; Wu, J.; Loffredo, M.; Renshaw, A.A.; Kantoff, P.W.; D’Amico, A.V. Surrogate end points for all-cause mortality in men with localized unfavorable-risk prostate cancer treated with radiation therapy vs. radiation therapy plus androgen deprivation therapy: A secondary analysis of a randomized clinical trial. JAMA Oncol. 2017, 3, 652–658. [Google Scholar] [CrossRef]
- Skove, S.L.; Howard, L.E.; Aronson, W.J.; Terris, M.K.; Kane, C.J.; Amling, C.L.; Cooperberg, M.R.; Moreira, D.M.; Freedland, S.J. Timing of prostate-specific antigen nadir after radical prostatectomy and risk of biochemical recurrence. Urology 2017, 108, 129–134. [Google Scholar] [CrossRef]
- Vesely, S.; Jarolim, L.; Schmidt, M.; Do Carmo Silva, J.; Duskova, K.; Babjuk, M. Stratification model based on early postprostatectomy prostate-specific antigen kinetics may help to reduce the risk of overtreatment in candidates for adjuvant radiotherapy. Scand. J. Urol. 2017, 51, 114–119. [Google Scholar] [CrossRef]
- Von Eyben, F.E.; Kiljunen, T.; Joensuu, T.; Kairemo, K.; Uprimny, C.; Virgolini, I. 177Lu-PSMA-617 radioligand therapy for a patient with lymph node metastatic prostate cancer. Oncotarget 2017, 8, 66112–66116. [Google Scholar] [CrossRef][Green Version]
- Boehm, K.; Schiffmann, J.; Tian, Z.; Lesmana, H.; Larcher, A.; Mandel, P.; Karakiewicz, P.I.; Graefen, M.; Schwarz, R.; Krull, A.; et al. Five-year biochemical recurrence-free and overall survival following high-dose-rate brachytherapy with additional external beam or radical prostatectomy in patients with clinically localized prostate cancer. Urol. Oncol. 2016, 34, 119.e11–119.e18. [Google Scholar] [CrossRef]
- Fossati, N.; Karnes, R.J.; Cozzarini, C.; Fiorino, C.; Gandaglia, G.; Joniau, S.; Boorjian, S.A.; Goldner, G.; Hinkelbein, W.; Haustermans, K.; et al. Assessing the optimal timing for early salvage radiation therapy in patients with prostate-specific antigen rise after radical prostatectomy. Eur. Urol. 2016, 69, 728–733. [Google Scholar] [CrossRef]
- Laajala, T.D.; Seikkula, H.; Seyednasrollah, F.; Mirtti, T.; Bostrom, P.J.; Elo, L.L. Longitudinal modeling of ultrasensitive and traditional prostate-specific antigen and prediction of biochemical recurrence after radical prostatectomy. Sci. Rep. 2016, 6, 36161. [Google Scholar] [CrossRef]
- Naik, M.; Reddy, C.A.; Stephans, K.L.; Ciezki, J.P.; Garcia, J.; Grivas, P.; Stephenson, A.J.; Klein, E.A.; Tendulkar, R.D. Posttreatment prostate-specific antigen 6 months after radiation with androgen deprivation therapy predicts for distant metastasis-free survival and prostate cancer-specific mortality. Int. J. Radiat. Oncol. Biol. Phys. 2016, 96, 617–623. [Google Scholar] [CrossRef]
- Sokoll, L.J.; Zhang, Z.; Chan, D.W.; Reese, A.C.; Bivalacqua, T.J.; Partin, A.W.; Sokoll, L.J.; Zhang, Z.; Chan, D.W.; Reese, A.C.; et al. Do ultrasensitive prostate specific antigen measurements have a role in predicting long-term biochemical recurrence-free survival in men after radical prostatectomy? J. Urol. 2016, 195, 330–336. [Google Scholar] [CrossRef]
- Stish, B.; Pisansky, T.M.; Harmsen, W.S.; Davis, B.J.; Tzou, K.S.; Choo, R.; Buskirk, S.J. Improved metastasis-free and survival outcomes with early salvage radiotherapy in men with detectable prostate-specific antigen after prostatectomy for prostate cancer. J. Clin. Oncol. 2016, 34, 3864–3871. [Google Scholar] [CrossRef]
- Kang, J.J.; Reiter, R.E.; Steinberg, M.L.; King, C.R. Ultrasensitive prostate specific antigen after prostatectomy reliably identifies patients requiring postoperative radiotherapy. J. Urol. 2015, 193, 1532–1538. [Google Scholar] [CrossRef]
- Kavosi, B.; Salimi, A.; Hallaj, R.; Moradi, F. Ultrasensitive electrochemical immunosensor for PSA biomarker detection in prostate cancer cells using gold nanoparticles/PAMAM dendrimer loaded with enzyme linked aptamer as integrated triple signal amplification strategy. Biosens. Bioelectron. 2015, 74, 915–923. [Google Scholar] [CrossRef]
- Liang, J.; Yao, C.; Li, X.; Wu, Z.; Huang, C.; Fu, Q.; Lan, C.; Cao, D.; Tang, Y. Silver nanoprism etching-based plasmonic ELISA for the high sensitive detection of prostate-specific antigen. Biosens. Bioelectron. 2015, 69, 128–134. [Google Scholar] [CrossRef]
- Seikkula, H.; Syvanen, K.T.; Kurki, S.; Mirtti, T.; Taimen, P.; Laato, M.; Bostrom, P.J. Role of ultrasensitive prostate-specific antigen in the follow-up of prostate cancer after radical prostatectomy. Urol. Oncol. 2015, 33, 16.e1–16.e7. [Google Scholar]
- Tang, L.; Li, S.; Xu, L.; Ma, W.; Kuang, H.; Wang, L.; Xu, C. Chirality-based Au@Ag nanorod dimers sensor for ultrasensitive PSA detection. ACS Appl. Mater. Interfaces 2015, 7, 12708–12712. [Google Scholar] [CrossRef]
- Tilki, D.; Mandel, P.; Schlomm, T.; Chun, F.K.M.; Tennstedt, P.; Pehrke, D.; Haese, A.; Huland, H.; Graefen, M.; Salomon, G.; et al. External validation of the CAPRA-S score to predict biochemical recurrence, metastasis and mortality after radical prostatectomy in a European cohort. J. Urol. 2015, 193, 1970–1975. [Google Scholar] [CrossRef]
- Briganti, A.; Karnes, R.J.; Joniau, S.; Boorjian, S.A.; Cozzarini, C.; Gandaglia, G.; Hinkelbein, W.; Haustermans, K.; Tombal, B.; Shariat, S.; et al. Prediction of outcome following early salvage radiotherapy among patients with biochemical recurrence after radical prostatectomy. Eur. Urol. 2014, 66, 479–486. [Google Scholar] [CrossRef]
- Chen, X.; Zhou, G.; Song, P.; Wang, J.; Gao, J.; Lu, J.; Fan, C.; Zuo, X. Ultrasensitive electrochemical detection of prostate-specific antigen by using antibodies anchored on a DNA nanostructural scaffold. Anal. Chem. 2014, 86, 7337–7342. [Google Scholar] [CrossRef]
- Furubayashi, N.; Negishi, T.; Kashiwagi, E.; Hirata, Y.; Taguchi, K.; Hasegawa, Y.; Nakamura, M. Usefulness of ultra-sensitive prostate-specific antigen following radical prostatectomy. Mol. Clin. Oncol. 2014, 2, 851–857. [Google Scholar] [CrossRef]
- Jackson, W.C.; Johnson, S.B.; Foster, B.; Foster, C.; Li, D.; Song, Y.; Vainshtein, J.; Zhou, J.; Hamstra, D.A.; Feng, F.Y. Combining prostate-specific antigen nadir and time to nadir allows for early identification of patients at highest risk for development of metastasis and death following salvage radiation therapy. Pract. Radiat. Oncol. 2014, 4, 99–107. [Google Scholar] [CrossRef]
- Keto, C.J.; Aronson, W.J.; Terris, M.K.; Presti, J.C.; Kane, C.J.; Amling, C.L.; Freedland, S.J. Detectable prostate-specific antigen nadir during androgen-deprivation therapy predicts adverse prostate cancer-specific outcomes: Results from the SEARCH database. Eur. Urol. 2014, 65, 620–627. [Google Scholar] [CrossRef]
- Mir, M.C.; Li, J.; Klink, J.C.; Kattan, M.W.; Klein, E.A.; Stephenson, A.J. Optimal definition of biochemical recurrence after radical prostatectomy depends on pathologic risk factors: Identifying candidates for early salvage therapy. Eur. Urol. 2014, 66, 204–210. [Google Scholar] [CrossRef]
- Vesely, S.; Jarolim, L.; Duskova, K.; Schmidt, M.; Dusek, P.; Babjuk, M. The use of early postoperative prostate-specific antigen to stratify risk in patients with positive surgical margins after radical prostatectomy. BMC Urol. 2014, 14, 79. [Google Scholar] [CrossRef]
- Vesely, S.; Jarolim, L.; Schmidt, M.; Minarik, I.M.; Dusek, P.; Babjuk, M. Parameters derived from the postoperative decline in ultrasensitive PSA improve the prediction of radical prostatectomy outcome. World J. Urol. 2013, 31, 299–304. [Google Scholar] [CrossRef]
- D’Amico, A.V.; Chen, M.H.; de Castro, M.; Loffredo, M.; Lamb, D.S.; Steigler, A.; Kantoff, P.W.; Denham, J.W. Surrogate endpoints for prostate cancer-specific mortality after radiotherapy and androgen suppression therapy in men with localised or locally advanced prostate cancer: An analysis of two randomised trials. Lancet Oncol. 2012, 13, 189–195. [Google Scholar] [CrossRef]
- Ho, T.; Gerber, L.; Aronson, W.J.; Terris, M.K.; Presti, J.C.; Kane, C.J.; Amling, C.L.; Freedland, S.J. Obesity, prostate-specific antigen nadir, and biochemical recurrence after radical prostatectomy: Biology or technique? Results from the SEARCH database. Eur. Urol. 2012, 62, 910–916. [Google Scholar] [CrossRef]
- Lepor, H.; Cheli, C.D.; Thiel, R.P.; Taneja, S.S.; Laze, J.; Chan, D.W.; Sokoll, L.J.; Mangold, L.; Partin, A.W. Clinical evaluation of a novel method for the measurement of prostate-specific antigen, AccuPSA(TM), as a predictor of 5-year biochemical recurrence-free survival after radical prostatectomy: Results of a pilot study. BJU Int. 2012, 109, 1770–1775. [Google Scholar] [CrossRef]
- McDermed, J.E.; Sanders, R.; Fait, S.; Klem, R.E.; Sarno, M.J.; Adams, T.H.; Diamandis, E.P. Nucleic acid detection immunoassay for prostate-specific antigen based on immuno-PCR methodology. Clin. Chem. 2012, 58, 732–740. [Google Scholar] [CrossRef]
- Siegmann, A.; Bottke, D.; Faehndrich, J.; Brachert, M.; Lohm, G.; Miller, K.; Bartkowiak, D.; Hinkelbein, W.; Wiegel, T. Salvage radiotherapy after prostatectomy—What is the best time to treat? Radiother. Oncol. 2012, 103, 239–243. [Google Scholar] [CrossRef]
- Yoshida, T.; Matsuzaki, K.; Kobayashi, Y.; Takeda, K.; Nakayama, M.; Arai, Y.; Kakimoto, K.; Nishimura, K. Usefulness of postoperative nadir prostate-specific antigen value by ultrasensitive assay as a predictor of prostate-specific antigen relapse for pathological T3 or positive surgical margins after radical prostatectomy for prostate cancer. Int. Urol. Nephrol. 2012, 44, 479–485. [Google Scholar] [CrossRef]
- Malik, R.D.; Goldberg, J.D.; Hochman, T.; Lepor, H. Three-year postoperative ultrasensitive prostate-specific antigen following open radical retropubic prostatectomy is a predictor for delayed biochemical recurrence. Eur. Urol. 2011, 60, 548–553. [Google Scholar] [CrossRef]
- Wilson, D.H.; Hanlon, D.W.; Provuncher, G.K.; Chang, L.; Song, L.; Patel, P.P.; Ferrell, E.P.; Lepor, H.; Partin, A.W.; Chan, D.W.; et al. Fifth-generation digital immunoassay for prostate-specific antigen by single molecule array technology. Clin. Chem. 2011, 57, 1712–1721. [Google Scholar] [CrossRef]
- Chang, S.L.; Freedland, S.J.; Terris, M.K.; Aronson, W.J.; Kane, C.J.; Amling, C.L.; Presti, J.C., Jr. Freedom from a detectable ultrasensitive prostate-specific antigen at two years after radical prostatectomy predicts a favorable clinical outcome: Analysis of the SEARCH database. Urology 2010, 75, 439–444. [Google Scholar] [CrossRef]
- Eisenberg, M.L.; Davies, B.J.; Cooperberg, M.R.; Cowan, J.E.; Carroll, P.R. Prognostic implications of an undetectable ultrasensitive prostate-specific antigen level after radical prostatectomy. Eur. Urol. 2010, 57, 622–629. [Google Scholar] [CrossRef]
- Hong, S.K.; Park, H.Z.; Lee, W.K.; Kim, D.S.; Lee, J.S.; Doo, S.H.; Jeong, S.J.; Yoon, C.Y.; Byun, S.S.; Lee, S.E. Prognostic significance of undetectable ultrasensitive prostate-specific antigen nadir after radical prostatectomy. Urology 2010, 76, 723–727. [Google Scholar] [CrossRef]
- Moreira, D.M.; Presti, J.C., Jr.; Aronson, W.J.; Terris, M.K.; Kane, C.J.; Amling, C.L.; Sun, L.L.; Moul, J.W.; Freedland, S.J. Postoperative prostate-specific antigen nadir improves accuracy for predicting biochemical recurrence after radical prostatectomy: Results from the Shared Equal Access Regional Cancer Hospital (SEARCH) and Duke Prostate Center databases. Int. J. Urol. 2010, 17, 914–922. [Google Scholar] [CrossRef]
- Lee, S.M.; Hwang, K.S.; Yoon, H.J.; Yoon, D.S.; Kim, S.K.; Lee, Y.S.; Kim, T.S. Sensitivity enhancement of a dynamic mode microcantilever by stress inducer and mass inducer to detect PSA at low picogram levels. Lab. Chip 2009, 9, 2683–2690. [Google Scholar] [CrossRef]
- Mani, V.; Chikkaveeraiah, B.V.; Patel, V.; Gutkind, J.S.; Rusling, J.F. Ultrasensitive immunosensor for cancer biomarker proteins using gold nanoparticle film electrodes and multienzyme-particle amplification. ACS Nano 2009, 3, 585–594. [Google Scholar] [CrossRef]
- Thaxton, C.S.; Elghanian, R.; Thomas, A.D.; Stoeva, S.I.; Lee, J.S.; Smith, N.D.; Schaeffer, A.J.; Klocker, H.; Horninger, W.; Bartsch, G.; et al. Nanoparticle-based bio-barcode assay redefines “undetectable” PSA and biochemical recurrence after radical prostatectomy. Proc. Natl. Acad. Sci. USA 2009, 106, 18437–18442. [Google Scholar] [CrossRef]
- Viney, R.; Gommersall, L.; Zeif, J.; Hayne, D.; Shah, Z.H.; Doherty, A. Ultrasensitive prostate specific antigen assay following laparoscopic radical prostatectomy—An outcome measure for defining the learning curve. Ann. R. Coll. Surg. Engl. 2009, 91, 399–403. [Google Scholar] [CrossRef]
- Wiegel, T.; Lohm, G.; Bottke, D.; Hocht, S.; Miller, K.; Siegmann, A.; Schostak, M.; Neumann, K.; Hinkelbein, W. Achieving an undetectable PSA after radiotherapy for biochemical progression after radical prostatectomy is an independent predictor of biochemical outcome—Results of a retrospective study. Int. J. Radiat. Oncol. Biol. Phys. 2009, 73, 1009–1016. [Google Scholar] [CrossRef]
- Zelefsky, M.J.; Shi, W.; Yamada, Y.; Kollmeier, M.A.; Cox, B.; Park, J.; Seshan, V.E. Postradiotherapy 2-year prostate-specific antigen nadir as a predictor of long-term prostate cancer mortality. Int. J. Radiat. Oncol. Biol. Phys. 2009, 75, 1350–1356. [Google Scholar] [CrossRef]
- Kinoshita, H.; Kamoto, T.; Nishiyama, H.; Nakamura, E.; Matsuda, T.; Ogawa, O. Prostate specific antigen nadir determined using ultra-sensitive prostate specific antigen as a predictor of biochemical progression after radical prostatectomy in Japanese males. Int. J. Urol. 2007, 14, 930–934. [Google Scholar] [CrossRef]
- Shimizu, F.; Tanaka, S.; Matsuyama, Y.; Tominaga, T.; Ohashi, Y.; Fujime, M. Efficiency of ultrasensitive prostate-specific antigen assay in diagnosing biochemical failure after radical prostatectomy. Jpn. J. Clin. Oncol. 2007, 37, 446–451. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Stephenson, A.J.; Scardino, P.T.; Kattan, M.W.; Pisansky, T.M.; Slawin, K.M.; Klein, E.A.; Anscher, M.S.; Michalski, J.M.; Sandler, H.M.; Lin, D.W.; et al. Predicting the outcome of salvage radiation therapy for recurrent prostate cancer after radical prostatectomy. J. Clin. Oncol. 2007, 25, 2035–2041. [Google Scholar] [CrossRef] [PubMed]
- Ray, M.E.; Thames, H.D.; Levy, L.B.; Horwitz, E.M.; Kupelian, P.A.; Martinez, A.A.; Michalski, J.M.; Pisansky, T.M.; Shipley, W.U.; Zelefsky, M.J.; et al. PSA nadir predicts biochemical and distant failures after external beam radiotherapy for prostate cancer: A multi-institutional analysis. Int. J. Radiat. Oncol. Biol. Phys. 2006, 64, 1140–1150. [Google Scholar] [CrossRef] [PubMed]
- Sakai, I.; Harada, K.; Kurahashi, T.; Muramaki, M.; Yamanaka, K.; Hara, I.; Inoue, T.A.; Miyake, H. Usefulness of the nadir value of serum prostate-specific antigen measured by an ultrasensitive assay as a predictor of biochemical recurrence after radical prostatectomy for clinically localized prostate cancer. Urol. Int. 2006, 76, 227–231. [Google Scholar] [CrossRef] [PubMed]
- Stephenson, A.J.; Kattan, M.W.; Eastham, J.A.; Dotan, Z.A.M.; Bianco, F.J., Jr.; Lilja, H.; Scardino, P.T. Defining biochemical recurrence of prostate cancer after radical prostatectomy: A proposal for a standardized definition. J. Clin. Oncol. 2006, 24, 3973–3978. [Google Scholar] [CrossRef] [PubMed]
- Taylor, J.A., 3rd; Koff, S.G.; Dauser, D.A.; McLeod, D.G. The relationship of ultrasensitive measurements of prostate-specific antigen levels to prostate cancer recurrence after radical prostatectomy. BJU Int. 2006, 98, 540–543. [Google Scholar] [CrossRef]
- Nakamura, M.; Hasumi, H.; Miyoshi, Y.; Sugiura, S.; Fujinami, K.; Yao, M.; Kubota, Y.; Uemura, H. Usefulness of ultrasensitive prostate-specific antigen assay for early detection of biochemical failure after radical prostatectomy. Int. J. Urol. 2005, 12, 1050–1054. [Google Scholar] [CrossRef]
- Shen, S.; Lepor, H.; Yaffee, R.; Taneja, S.S. Ultrasensitive serum prostate specific antigen nadir accurately predicts the risk of early relapse after radical prostatectomy. J. Urol. 2005, 173, 777–780. [Google Scholar] [CrossRef]
- Shinghal, R.; Yemoto, C.; McNeal, J.E.; Brooks, J.D. Biochemical recurrence without PSA progression characterizes a subset of patients after radical prostatectomy. Prostate-specific antigen. Urology 2003, 61, 380–385. [Google Scholar] [CrossRef]
- Doherty, A.P.; Bower, M.; Smith, G.L.; Miano, R.; Mannion, E.M.; Mitchell, H.; Christmas, T.J. Undetectable ultrasensitive PSA after radical prostatectomy for prostate cancer predicts relapse-free survival. Br. J. Cancer 2000, 83, 1432–1436. [Google Scholar] [CrossRef]
- Vassilikos, E.J.; Yu, H.; Trachtenberg, J.; Nam, R.K.; Narod, S.A.; Bromberg, I.L.; Diamandis, E.P. Relapse and cure rates of prostate cancer patients after radical prostatectomy and 5 years of follow-up. Clin. Biochem. 2000, 33, 115–123. [Google Scholar] [CrossRef] [PubMed]
- Allard, W.J.; Cheli, C.D.; Morris, D.L.; Goldblatt, J.; Pierre, Y.; Kish, L.; Chen, Y.; Dai, J.; Vessella, R.; Chan, D.W.; et al. Multicenter evaluation of the performance and clinical utility in longitudinal monitoring of the Bayer Immuno 1 complexed PSA assay. Int. J. Biol. Markers 1999, 14, 73–83. [Google Scholar] [CrossRef]
- Haese, A.; Huland, E.; Graefen, M.; Hammerer, P.; Noldus, J.; Huland, H. Ultrasensitive detection of prostate specific antigen in the followup of 422 patients after radical prostatectomy. J. Urol. 1999, 161, 1206–1211. [Google Scholar] [CrossRef]
- Pound, C.R.; Partin, A.W.; Eisenberger, M.A.; Chan, D.W.; Pearson, J.D.; Walsh, P.C. Natural history of progression after PSA elevation following radical prostatectomy. JAMA 1999, 281, 1591–1597. [Google Scholar] [CrossRef]
- Arai, Y.; Okubo, K.; Aoki, Y.; Maekawa, S.; Okada, T.; Maeda, H. Ultrasensitive assay of prostate-specific antigen for early detection of residual cancer after radical prostatectomy. Int. J. Urol. 1998, 5, 550–555. [Google Scholar] [CrossRef]
- Garg, M.K.; Tekyi-Mensah, S.; Bolton, S.; Velasco, J.; Pontes, E.; Wood, D.P., Jr.; Porter, A.T.; Forman, J.D. Impact of postprostatectomy prostate-specific antigen nadir on outcomes following salvage radiotherapy. Urology 1998, 51, 998–1002. [Google Scholar] [CrossRef] [PubMed]
- Morris, D.L.; Dillon, P.W.; Very, D.L.; Ng, P.; Kish, L.; Goldblatt, J.L.; Bruzek, D.J.; Chan, D.W.; Ahmed, M.S.; Witek, D.; et al. Bayer Immuno 1 PSA Assay: An automated, ultrasensitive method to quantitate total PSA in serum. J. Clin. Lab. Anal. 1998, 12, 65–74. [Google Scholar] [CrossRef]
- Ellis, L.W.J.; Vessella, R.L.; Noteboom, J.L.; Lange, P.H.; Wolfert, R.L.; Rittenhouse, H.G. Early detection of recurrent prostate cancer with an ultrasensitive chemiluminescent prostate-specific antigen assay. Urology 1997, 50, 573–579. [Google Scholar] [CrossRef] [PubMed]
- Pruthi, R.S.; Haese, A.; Huland, E.; Stamey, T.A. Use of serum concentration techniques to enhance early detection of recurrent prostate cancer after radical prostatectomy. Urology 1997, 49, 404–410. [Google Scholar] [CrossRef]
- Witherspoon, L.R.; Lapeyrolerie, T. Sensitive prostate specific antigen measurements identify men with long disease-free intervals and differentiate aggressive from indolent cancer recurrences within 2 years after radical prostatectomy. J. Urol. 1997, 157, 1322–1328. [Google Scholar] [CrossRef]
- Yu, H.; Diamandis, E.P.; Wong, P.Y.; Nam, R.; Trachtenberg, J. Detection of prostate cancer relapse with prostate specific antigen monitoring at levels of 0.001 to 0.1 microG./L. J. Urol. 1997, 157, 913–918. [Google Scholar] [CrossRef] [PubMed]
- Ferguson, R.A.; Yu, H.; Kalyva, S.M.; Zammit, S.; Diamandis, E.P. Ultrasensitive detection of prostate-specific antigen by a time-resolved immunofluorometric assay and the Immulite immunochemiluminescent third-generation assay: Potential applications in prostate and breast cancers. Clin. Chem. 1996, 42, 675–684. [Google Scholar] [CrossRef] [PubMed]
- Iersel, M.P.v.; Thomas, C.M.; Segers, M.F.; Witjes, W.P.; Debruyne, F.M.; Oosterhof, G.O. The use of ‘ultrasensitive’ prostate-specific antigen assays in the detection of biochemical recurrence after radical prostatectomy. Br. J. Urol. 1996, 77, 418–422. [Google Scholar] [CrossRef] [PubMed]
- Khosravi, M.J.; Papanastasiou-Diamandi, A.; Mistry, J. An ultrasensitive immunoassay for prostate-specific antigen based on conventional colorimetric detection. Clin. Biochem. 1995, 28, 407–414. [Google Scholar] [CrossRef] [PubMed]
- Mione, R.; Barichello, M.; Sartorello, P.; Leon, A.; Barioli, P.; Gion, M. Third-generation PSA: Ultrasensitive or ultraprecise assay? Int. J. Biol. Markers 1995, 10, 229–233. [Google Scholar] [CrossRef] [PubMed]
- Schambeck, C.M. Evaluation of the COBAS CORE Immunoassay for measuring prostate-specific antigen (PSA)—Multi-centre study results. The PSA Study Group. Eur. J. Clin. Chem. Clin. Biochem. 1995, 33, 541–547. [Google Scholar] [PubMed]
- Yu, H.; Diamandis, E.P.; Prestigiacomo, A.F.; Stamey, T.A. Ultrasensitive assay of prostate-specific antigen used for early detection of prostate cancer relapse and estimation of tumor-doubling time after radical prostatectomy. Clin. Chem. 1995, 41, 430–434. [Google Scholar] [CrossRef] [PubMed]
- Klee, G.G.; Preissner, C.M.; Oesterling, J.E. Development of a highly sensitive immunochemiluminometric assay for prostate-specific antigen. Urology 1994, 44, 76–82. [Google Scholar] [CrossRef] [PubMed]
- Arai, Y.; Onishi, H.; Oishi, K.; Takeuchi, H.; Yoshida, O. Use of a new hypersensitive assay for the detection of prostate specific antigen in prostate cancer. Jpn. J. Clin. Oncol. 1993, 23, 110–115. [Google Scholar]
- Liedtke, R.J.; Kroon, G.; Batjer, J.D. Modified assay of prostate-specific antigen with a detection limit < 0.01 microgram/L. Clin. Chem. 1993, 39, 2150–2154. [Google Scholar]
- Stamey, T.A.; Graves, H.C.; Wehner, N.; Ferrari, M.; Freiha, F.S. Early detection of residual prostate cancer after radical prostatectomy by an ultrasensitive assay for prostate specific antigen. J. Urol. 1993, 149, 787–792. [Google Scholar] [CrossRef] [PubMed]
- Yu, H.; Diamandis, E.P. Ultrasensitive time-resolved immunofluorometric assay of prostate-specific antigen in serum and preliminary clinical studies. Clin. Chem. 1993, 39, 2108–2114. [Google Scholar] [CrossRef] [PubMed]
- Vessella, R.L.; Noteboom, J.; Lange, P.H. Evaluation of the Abbott IMx automated immunoassay of prostate-specific antigen. Clin. Chem. 1992, 38, 2044–2054. [Google Scholar] [CrossRef] [PubMed]
- Whitby, L.G. The International System of Units (SI) and its application to clinical chemistry. Scott. Med. J. 1974, 19, 269–277. [Google Scholar] [CrossRef] [PubMed]
- Roach, M., 3rd; Hanks, G.; Thames, H., Jr.; Schellhammer, P.; Shipley, W.U.; Sokol, G.H.; Sandler, H. Defining biochemical failure following radiotherapy with or without hormonal therapy in men with clinically localized prostate cancer: Recommendations of the RTOG-ASTRO Phoenix Consensus Conference. Int. J. Radiat. Oncol. Biol. Phys. 2006, 65, 965–974. [Google Scholar] [CrossRef] [PubMed]
- Pfister, D.; Bolla, M.; Briganti, A.; Carroll, P.; Cozzarini, C.; Joniau, S.; van Poppel, H.; Roach, M.; Stephenson, A.; Wiegel, T.; et al. Early salvage radiotherapy following radical prostatectomy. Eur. Urol. 2014, 65, 1034–1043. [Google Scholar] [CrossRef] [PubMed]
- Nyaga, V.N.; Arbyn, M.; Aerts, M. Metaprop: A Stata command to perform meta-analysis of binomial data. Arch. Public Health 2014, 72, 39. [Google Scholar] [CrossRef] [PubMed]
- Tobias, A. Meta-analysis of p values. Stata Tech. Bull. 1999, 49, 15–17. [Google Scholar]
- Soletormos, G.; Semjonow, A.; Sibley, P.E.; Lamerz, R.; Petersen, P.H.; Albrecht, W.; Bialk, P.; Gion, M.; Junker, F.; Schmid, H.P.; et al. Biological variation of total prostate-specific antigen: A survey of published estimates and consequences for clinical practice. Clin. Chem. 2005, 51, 1342–1351. [Google Scholar] [CrossRef]
- Prestigiacomo, A.F.; Stamey, T.A. A comparison of 4 ultrasensitive prostate specific antigen assays for early detection of residual cancer after radical prostatectomy. J. Urol. 1994, 152, 1515–1519. [Google Scholar] [CrossRef]
- Forde, J.C.; Marignol, L.; Blake, O.; McDermott, T.; Grainger, R.; Crowley, V.E.; Lynch, T.H. Standardization of assay methods reduces variability of total PSA measurements: An Irish study. BJU Int. 2012, 110, 644–650. [Google Scholar] [CrossRef]
- Ferguson, J.; Patel, D.; Atkinson, E.; Rigsby, P.; Burns, C. Continued provision of WHO international standards for total and free PSA: Content and commutability of replacement preparations. Clin. Biochem. 2019, 71, 58–66. [Google Scholar] [CrossRef]
- Kort, S.A.; Martens, F.; Vanpoucke, H.; van Duijnhoven, H.L.; Blankenstein, M.A. Comparison of 6 automated assays for total and free prostate-specific antigen with special reference to their reactivity toward the WHO 96/670 reference preparation. Clin. Chem. 2006, 52, 1568–1574. [Google Scholar] [CrossRef]
- Garrido, M.M.; Marta, J.C.; Ribeiro, R.M.; Pinheiro, L.C.; Holdenrieder, S.; Guimaraes, J.T. Comparison of three assays for total and free PSA using hybritech and WHO calibrations. In Vivo 2021, 35, 3431–3439. [Google Scholar] [CrossRef] [PubMed]
- Foj, L.; Filella, X.; Alcover, J.; Auge, J.M.; Escudero, J.M.; Molina, R. Variability of assay methods for total and free PSA after WHO standardization. Tumour Biol. 2014, 35, 1867–1873. [Google Scholar] [CrossRef]
- Stephan, C.; Bangma, C.; Vignati, G.; Bartsch, G.; Lein, M.; Jung, K.; Philippe, M.; Semjonow, A.; Catalona, W.J. 20–25% lower concentrations of total and free prostate-specific antigen (PSA) after calibration of PSA assays to the WHO reference materials—Analysis of 1098 patients in four centers. Int. J. Biol. Markers 2009, 24, 65–69. [Google Scholar] [PubMed]
- Deng, L.; Yue, D.; Wang, X.; Li, H. Consistency and diagnostic accuracy of 4 assays in the detection of the total and free prostate-specific antigen. Transl. Androl. Urol. 2023, 12, 261–270. [Google Scholar] [CrossRef]
- Von Eyben, F.E.; Kangasmaki, A.; Kiljunen, T.; Joensuu, T. Volumetric-modulated arc therapy for a pelvic lymph-node metastasis from prostate cancer—A case report. Tumori 2013, 99, e120–e123. [Google Scholar] [CrossRef] [PubMed]
- Von Eyben, F.E.; Joensuu, T.; Kangasmaki, A.; Kairemo, K.; Kiljunen, T. Abiraterone and volumetric modulated arc therapy for second recurrence of node-positive prostate cancer—A case report. Diagn. Imaging Ther. 2014, 1, 73–80. [Google Scholar] [CrossRef][Green Version]
- Scher, H.I.; Morris, M.J.; Stadler, W.M.; Higano, C.; Basch, E.; Fizazi, K.; Antonarakis, E.S.; Beer, T.M.; Carducci, M.A.; Chi, K.N.; et al. Trial Design and Objectives for Castration-Resistant Prostate Cancer: Updated Recommendations From the Prostate Cancer Clinical Trials Working Group 3. J. Clin. Oncol. 2016, 34, 1402–1418. [Google Scholar] [CrossRef]
- King, C.R. The timing of salvage radiotherapy after radical prostatectomy: A systematic review. Int J Radiat. Oncol. Biol. Phys. 2012, 84, 104–111. [Google Scholar] [CrossRef] [PubMed]
- Kabasakal, L.; Demirci, E.; Nematyazar, J.; Akyel, R.; Razavi, B.; Ocak, M.; Aygun, A.; Obek, C.; Kural, A.R. The role of PSMA PET/CT imaging in restaging of prostate cancer patients with low prostate-specific antigen levels. Nucl. Med. Commun. 2017, 38, 149–155. [Google Scholar] [CrossRef] [PubMed]
- Vogel, M.M.E.; Dewes, S.; Sage, E.K.; Devecka, M.; Gschwend, J.E.; Eiber, M.; Combs, S.E.; Schiller, K. A survey among German-speaking radiation oncologists on PET-based radiotherapy of prostate cancer. Radiat. Oncol. 2021, 16, 82. [Google Scholar] [CrossRef] [PubMed]
- Vogel, M.M.E.; Dewes, S.; Sage, E.K.; Devecka, M.; Gschwend, J.E.; Schiller, K.; Combs, S.E. Patterns of care for prostate cancer radiotherapy-results from a survey among German-speaking radiation oncologists. Strahlenther. Onkol. 2021, 197, 962–970. [Google Scholar] [CrossRef]
- Burgard, C.; Hoffmann, M.A.; Frei, M.; Buchholz, H.G.; Khreish, F.; Marlowe, R.J.; Schreckenberger, M.; Ezziddin, S.; Rosar, F. Detection efficacy of (68)Ga-PSMA-11 PET/CT in biochemical recurrence of prostate cancer with very low PSA levels: A 7-year, two-center “real-world” experience. Cancers 2023, 15, 1376. [Google Scholar] [CrossRef] [PubMed]
- Renard-Penna, R.; Zhang-Yin, J.; Montagne, S.; Aupin, L.; Bruguiere, E.; Labidi, M.; Latorzeff, I.; Hennequin, C. Targeting local recurrence after surgery with MRI imaging for prostate cancer in the setting of salvage radiation therapy. Front. Oncol. 2022, 12, 775387. [Google Scholar] [CrossRef]
- Diamandis, E.P. Prostate-specific antigen: Its usefulness in clinical medicine. Trends Endocrinol. Metab. 1998, 9, 310–316. [Google Scholar] [CrossRef]
- McClelland, S., 3rd; Sandler, K.A.; Degnin, C.; Chen, Y.; Mitin, T. Adjuvant vs. salvage radiation therapy in men with high-risk features after radical prostatectomy: Survey of North American genitourinary expert radiation oncologists. Can. Urol. Assoc. J. 2019, 13, E132–E134. [Google Scholar] [CrossRef]
- Parker, C.; Sydes, M.R.; Catton, C.M.; Kynaston, H.; Logue, J.; Murphy, C.; Morgan, R.C.; Mellon, K.; Morash, C.; Parulekar, W.; et al. Radiotherapy and androgen deprivation in combination after local surgery (RADICALS): A new Medical Research Council/National Cancer Institute of Canada phase III trial of adjuvant treatment after radical prostatectomy. BJU Int. 2007, 99, 1376–1379. [Google Scholar] [CrossRef]
- Wegener, D.; Aebersold, D.M.; Grimm, M.O.; Hammerer, P.; Froehner, M.; Graefen, M.; Boehmer, D.; Zips, D.; Wiegel, T. Postoperative radiotherapy of prostate cancer: Adjuvant versus early salvage. Biomedicines 2022, 10, 2256. [Google Scholar] [CrossRef]
- Von Eyben, F.E.; Bauman, G. Re: Joaquin Mateo, Karim Fizazi, Silke Gillessen; et al. Managing nonmetastatic castration-resistant prostate cancer. Eur. Urol. 2019, 75, 285–293, Erratum in Eur. Urol. 2020, 77, e67–e68. [Google Scholar]
- Taskovska, M.; Frelih, M.; Smrkolj, T.; Volavsek, M. Basal cell carcinoma of the prostate misdiagnosed as high-grade urothelial cancer—A case report of a diagnostic pitfall. Res. Rep. Urol. 2023, 15, 187–192. [Google Scholar] [CrossRef] [PubMed]
- Grossman, J.E.; Wu, Y.; Ye, H.; Bhatt, R.S. Case of basal cell carcinoma of the prostate successfully treated before and after a BRCA2 reversion mutation. JCO Precis. Oncol. 2018, 2, 1–5. [Google Scholar] [CrossRef] [PubMed]
- Pak, S.; Suh, Y.S.; Lee, D.E.; Kim, S.H.; Joung, J.Y.; Park, W.S.; Lee, S.J.; Lee, K.H. Association between postoperative detection of circulating tumor cells and recurrence in patients with prostate cancer. J. Urol. 2020, 203, 128–134. [Google Scholar] [CrossRef]
- Prensner, J.R.; Iyer, M.K.; Sahu, A.; Asangani, I.A.; Cao, Q.; Patel, L.; Vergara, I.A.; Davicioni, E.; Erho, N.; Ghadessi, M.; et al. The long noncoding RNA SChLAP1 promotes aggressive prostate cancer and antagonizes the SWI/SNF complex. Nat. Genet. 2013, 45, 1392–1398. [Google Scholar] [CrossRef] [PubMed]
- Kidd, S.G.; Carm, K.T.; Bogaard, M.; Olsen, L.G.; Bakken, A.C.; Lovf, M.; Lothe, R.A.; Axcrona, K.; Axcrona, U.; Skotheim, R.I. High expression of SCHLAP1 in primary prostate cancer is an independent predictor of biochemical recurrence, despite substantial heterogeneity. Neoplasia 2021, 23, 634–641. [Google Scholar] [CrossRef]
- Berenguer, C.V.; Pereira, F.; Camara, J.S.; Pereira, J.A.M. Underlying features of prostate cancer-statistics, risk factors, and emerging methods for its diagnosis. Curr. Oncol. 2023, 30, 2300–2321. [Google Scholar] [CrossRef]
- Jairath, N.K.; Dal Pra, A.; Vince, R., Jr.; Dess, R.T.; Jackson, W.C.; Tosoian, J.J.; McBride, S.M.; Zhao, S.G.; Berlin, A.; Mahal, B.A.; et al. A Systematic Review of the Evidence for the Decipher Genomic Classifier in Prostate Cancer. Eur. Urol. 2021, 79, 374–383. [Google Scholar] [CrossRef]
- Feng, F.Y.; Huang, H.C.; Spratt, D.E.; Zhao, S.G.; Sandler, H.M.; Simko, J.P.; Davicioni, E.; Nguyen, P.L.; Pollack, A.; Efstathiou, J.A.; et al. Validation of a 22-gene genomic classifier in patients with recurrent prostate cancer: An ancillary study of the NRG/RTOG 9601 randomized clinical trial. JAMA Oncol. 2021, 7, 544–552. [Google Scholar] [CrossRef]
- Kwak, L.; Ravi, P.; Armstrong, J.G.; Beckendorf, V.; Chin, J.L.; D’Amico, A.V.; Dearnaley, D.P.; Di Stasi, S.M.; Gillessen, S.; Lukka, H.; et al. Prognostic Impact of Prostate-Specific Antigen at 6 Months After Radiotherapy in Localized Prostate Cancer: An Individual Patient Data Analysis of Randomized Trials. J. Clin. Oncol. 2024, JCO2300762. [Google Scholar] [CrossRef]












{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Year | Study | Reference | Method | LLD (ng/L) |
|---|---|---|---|---|
| 2023 | Ozyurt | [23] | ITO-PET | 0.0074 |
| Wu | [27] | Ag NP | 0.001 | |
| 2022 | Cao | [28] | PtNP@Co2O4 NP | 10 |
| Orlov | [29] | Enzyme-linked | 19 | |
| Shen | [31] | AIE-ELISA | 1.3 | |
| 2020 | Aki | [37] | Membrane biosensor | 5 |
| Cid-Barrio | [38] | Au NP | 1 | |
| Farsschi | [40] | Citrate-Ag NPs | 70 | |
| Ren | [41] | MesoScale | 0.0035 | |
| Wang | [42] | Pd TP | 4.2 | |
| 2019 | Hahn | [46] | Au NP | 0.1 |
| Jalalvand | [47] | Aptamer | 0.5 | |
| Sun | [50] | Fluorescence | 10 | |
| Tian | [51] | Electrochemilumiscence | 0.001 | |
| 2018 | Yang | [54] | Sandwich immunosensor | 0.003 |
| Zhou | [55] | Au NP | 0.12 | |
| 2017 | Heydari-Bafrooei | [57] | Au NP | 1 |
| Liu | [58] | Au BN sensor | 0.27 | |
| 2015 | Kavosi | [70] | Au NP | 10 |
| Liang | [71] | Ag NP | 0.004 | |
| Tang | [73] | Au NP | NR | |
| 2014 | Chen | [76] | Au NP | 1 |
| 2012 | McDermed | [86] | Immuno-PCR | 0.27 |
| 2011 | Wilson | [90] | Digital immunoassay | 0.65 |
| 2009 | Lee, | [95] | Polyclonal Ab | 1 |
| Mani | [96] | Au NP | 0.5 | |
| Thaxton | [97] | Au NP | 0.33 | |
| 1996 | Ferguson, | [123] | Bayer Immuno 1 PSA | 3 |
| 1995 | Khosravi | [125] | Polyclonal Ab | 12 |
| Mione | [126] | Polyclonal Ab | 9.8 | |
| Schambeck | [127] | Immunolite | 3.8 | |
| 1994 | Klee | [129] | Monoclonal Ab | 8 |
| 1993 | Arai | [130] | IMx PSA | 4 |
| Iiedtke | [131] | MARKIT-M PSA | 200 | |
| Yu | [133] | Tb fluorometry | 2 | |
| 1992 | Vessella | [134] | Abbot IMx PSA | 30 |
| Year | Study | Reference | Patients | p Values for Outcmes | Hazard Ratio | ||||
|---|---|---|---|---|---|---|---|---|---|
| Total Number | Median Age at Diagnosis (Years) | Outcomes (Numbers) | |||||||
| PSAR | Deaths | PSAR | OS | ||||||
| 2023 | Bokemann | [20] | 1509 | 74 | NR | 760 | NR | NR | NR |
| Hussain | [21] | 1409 | 74 | NR | 364 | NR | NR | NR | |
| Lee | [22] | 397 | 59 | 126 | NR | <0.00001 | NR | NR | |
| Sutil | [24] | 427 | 64 | NR | 72 | NR | NR | NR | |
| Tilki | [25] | 759 | 64 | NR | 127 | NR | 0.008 | 1.49 | |
| Ueno | [26] | 418 | 67 | 51 | NR | 0.001 | NR | NR | |
| 2022 | Saad | [30] | 1401 | 74 | NR | NR | NR | NR | NR |
| Von Eyben | [32,33] | 1216 | 68 | NR | 133 | NR | <0.0001 | NR | |
| 2021 | Chung | [34] | 1483 | 64 | 323 | NR | <0.001 | NR | NR |
| Jansen | [35] | 315 | 70 | NR | NR | NR | NR | NR | |
| Zakaria | [36] | 167 | 61 | 23 | NR | 0.013 | NR | 2.7 | |
| 2020 | Dess | [39] | 760 | 65 | 238 | 104 | NR | 0.004 | 1.59 |
| 2019 | Bottke | [43] | 301 | 66 | 92 | 17 | NR | 0.004 | 3 |
| Bryant | [44] | 764 | 66 | 95 | 25 | NR | NR | NR | |
| Grivas | [45] | 213 | 63 | 103 | NR | <0.01 | NR | NR | |
| Pike | [48] | 204 | NR | NR | 160 | NR | <0.001 | 5.07 | |
| Schroeder | [49] | 459 | NR | 75 | 24 | 0.01 | 0.006 | NR | |
| 2018 | Burkhardt | [52] | 102 | NR | 75 | 2 | NR | NR | NR |
| Kang | [53] | 269 | NR | 137 | 21 | <0.0001 | <0.001 | NR | |
| 2017 | Abugharib | [56] | 657 | NR | 198 | 135 | <0.0001 | 0.002 | NR |
| Royce | [59] | 157 | 72 | 85 | 110 | NR | <0.01 | NR | |
| Skove | [60] | 1790 | NR | 820 | NR | <0.001 | NR | NR | |
| Vessely | [61] | 205 | NR | 106 | NR | <0.01 | NR | NR | |
| Von Eyben | [62] | 1 | 50 | NR | NR | NR | NR | NR | |
| 2016 | Boehm | [63] | 5619 | 65 | 1014 | 181 | NF | NR | NR |
| Fossatti | [64] | 716 | 64 | 129 | NR | <0.001 | NR | NR | |
| Laajaala | [65] | 503 | NR | NR | NR | NR | NR | ||
| Naik | [66] | 532 | 64 | 354 | 185 | <0.0001 | >0.05 | NR | |
| Sokolls | [67] | 754 | 69 | 262 | NR | NR | NR | NR | |
| Stish | [68] | 1106 | 61 | 669 | 183 | <0.001 | NR | NR | |
| 2015 | Kang | [69] | 247 | 67 | 114 | NR | <0.0001 | NR | NR |
| Sikkula | [72] | 604 | NR | 365 | NR | <0.01 | NR | 1.12 | |
| Tilki | [74] | 14,532 | 64 | 2950 | NR | <0.0001 | NR | NR | |
| 2014 | Briganti | [75] | 472 | NR | 126 | NR | NR | NR | NR |
| Furubayashi | [77] | 200 | 66 | 17 | NR | <0.0001 | NR | NR | |
| Jackson | [78] | 409 | 65 | 261 | 49 | NR | NR | NR | |
| Keto | [79] | 294 | 65 | NR | 31 | NR | <0.0001 | NR | |
| Mir | [80] | 2348 | 67 | 177 | 31 | <0.0001 | 0.0098 | NR | |
| Vessely | [81] | 116 | 60 | 55 | NR | NR | NR | NR | |
| 2013 | Vesely | [82] | 319 | NR | 107 | 31 | NR | NR | NR |
| 2012 | D’Amico | [83] | 734 | 63 | NR | 201 | NR | NR | NR |
| Ho | [84] | 1038 | 69 | 262 | NR | <0.001 | NR | NR | |
| Lepor | [85] | 34 | 60 | 11 | NR | NR | NR | NR | |
| Siegmann | [87] | 301 | 61 | 82 | 3 | NR | NR | NR | |
| Yoshida | [88] | 102 | 66 | 22 | NR | >0.001 | NR | NR | |
| 2011 | Malik | [89] | 1197 | 59 | 32 | NR | 0.001 | NR | NR |
| 2010 | Chang | [91] | 115 | 58 | NR | NR | NR | NR | NR |
| Eisenberg | [92] | 525 | 65 | 87 | NR | <0.001 | NR | NR | |
| Hong | [93] | 384 | NR | 63 | NR | <0.001 | NR | NR | |
| Moreira | [94] | 2735 | 65 | 635 | NR | <0.01 | NR | NR | |
| 2009 | Viney | [98] | 300 | NR | 70 | NR | <0.001 | NR | NR |
| Wiegel | [99] | 162 | 62 | 75 | NR | NR | NR | NR | |
| Zelefsky | [100] | 844 | 66 | NR | 65 | NR | NR | NR | |
| 2007 | Kinoshita | [101] | 257 | 68 | 49 | NR | NR | NR | NR |
| Shimizu | [102] | 257 | 65 | 23 | NR | NR | NR | NR | |
| Stephenson | [103] | 1540 | NR | 1047 | NR | 0.003 | NR | NR | |
| 2006 | Ray | [104] | 4839 | NR | 2318 | NR | NR | NR | NR |
| Sakai | [105] | 177 | NR | 16 | NR | <0.0001 | NR | NR | |
| Stephenson | [106] | 3125 | NR | 458 | NR | NR | NR | NR | |
| Taylor | [107] | 225 | 690 | 21 | NR | NR | NR | NR | |
| 2005 | Nakamura | [108] | 46 | NR | 15 | 0 | <0.001 | NR | NR |
| Shen | [109] | 545 | 67 | 54 | NR | <0.05 | NR | NR | |
| 2003 | Shinhal | [110] | 14 | 60 | 0 | NR | NR | NR | NR |
| 2000 | Doherty | [111] | 134 | 64 | 49 | NR | <0.001 | NR | NR |
| Vassilikos | [112] | NR | 64 | NR | NR | NR | NR | NR | |
| 1999 | Allard | [113] | 384 | NR | 49 | 4 | <0.0005 | NR | NR |
| Hase | [114] | 442 | NR | 88 | NR | NR | NR | NR | |
| Pound | [115] | 1997 | NR | 315 | NR | NR | NR | NR | |
| 1998 | Arai | [116] | 34 | NR | NR | 16 | NR | NR | NR |
| Garg | [117] | 78 | NR | 21 | NR | <0.0001 | NR | NR | |
| Morris | [118] | 159 | NR | 2 | NR | NR | NR | NR | |
| 1997 | Ellis | [119] | 170 | NR | NR | 24 | NR | NR | NR |
| Pruthi | [120] | 31 | NR | 31 | NR | NR | NR | NR | |
| Whiterspoon | [121] | 127 | NR | 66 | NR | NR | NR | NR | |
| Yu | [122] | 148 | 65 | 51 | NR | NR | NR | NR | |
| 1996 | Van Irrsel | [124] | 137 | NR | NR | 12 | NR | NR | NR |
| 1995 | Yu | [128] | 15 | NR | 10 | NR | NR | NR | NR |
| 1993 | Stamey | [132] | 187 | NR | 22 | NR | NR | NR | NR |
| Total number | 67,489 | 14,865 | 2663 | ||||||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
von Eyben, F.E.; Kairemo, K.; Kapp, D.S. Prostate-Specific Antigen as an Ultrasensitive Biomarker for Patients with Early Recurrent Prostate Cancer: How Low Shall We Go? A Systematic Review. Biomedicines 2024, 12, 822. https://doi.org/10.3390/biomedicines12040822
von Eyben FE, Kairemo K, Kapp DS. Prostate-Specific Antigen as an Ultrasensitive Biomarker for Patients with Early Recurrent Prostate Cancer: How Low Shall We Go? A Systematic Review. Biomedicines. 2024; 12(4):822. https://doi.org/10.3390/biomedicines12040822
Chicago/Turabian Stylevon Eyben, Finn Edler, Kalevi Kairemo, and Daniel S. Kapp. 2024. "Prostate-Specific Antigen as an Ultrasensitive Biomarker for Patients with Early Recurrent Prostate Cancer: How Low Shall We Go? A Systematic Review" Biomedicines 12, no. 4: 822. https://doi.org/10.3390/biomedicines12040822
APA Stylevon Eyben, F. E., Kairemo, K., & Kapp, D. S. (2024). Prostate-Specific Antigen as an Ultrasensitive Biomarker for Patients with Early Recurrent Prostate Cancer: How Low Shall We Go? A Systematic Review. Biomedicines, 12(4), 822. https://doi.org/10.3390/biomedicines12040822