

Elevated FIB-4 Is Associated with Higher Rates of Cardiovascular Disease and Extrahepatic Cancer History in Patients with Type 2 Diabetes Mellitus
 ,
,
Abstract
1. Introduction
2. Material and Methods
2.1. Patients
2.2. Methods
2.3. Ethics
2.4. Statistical Analysis
3. Results
- —
- Differences between patients with FIB-4 > and ≤ 1.3 at the enrollment.
- —
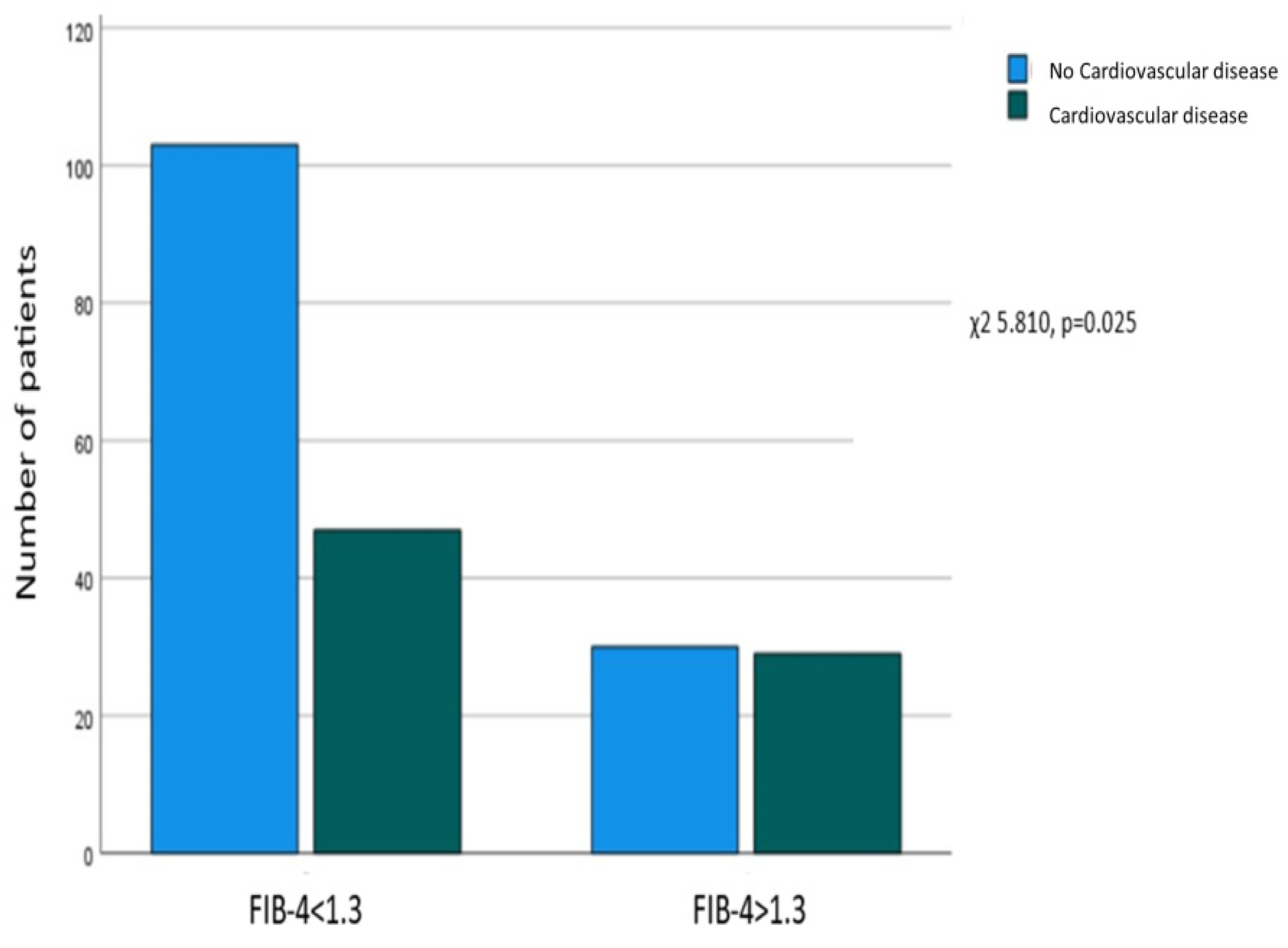
- Correlation between FIB-4 > 1.3 in enrollment and a history of CVD.
- —
- Patients over 65 years old.
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- IDF Diabetes Atlas 10th Edition 2021. Available online: www.diabetesatlas.org (accessed on 28 January 2024).
- Global Burden of Disease Collaborative Network. Global Burden of Disease Study 2019. Results. Institute for Health Metrics and Evaluation. 2020. Available online: https://vizhub.healthdata.org/gbd-results/ (accessed on 28 January 2024).
- Riazi, K.; Azhari, H.; Charette, J.H.; Underwood, F.E.; King, J.A.; Afshar, E.E.; Swain, M.G.; Congly, S.E.; Kaplan, G.G.; Shaheen, A.A. The Prevalence and Incidence of NAFLD Worldwide: A Systematic Review and Meta-Analysis. Lancet Gastroenterol. Hepatol. 2022, 7, 851–861. [Google Scholar] [CrossRef]
- Younossi, Z.M.; Koenig, A.B.; Abdelatif, D.; Fazel, Y.; Henry, L.; Wymer, M. Global Epidemiology of Nonalcoholic Fatty Liver Disease—Meta-analytic Assessment of Prevalence, Incidence, and Outcomes. Hepatology 2016, 64, 73–84. [Google Scholar] [CrossRef]
- Mc Glinchey, A.J.; Govaere, O.; Geng, D.; Ratziu, V.; Allison, M.; Bousier, J.; Petta, S.; de Oliviera, C.; Bugianesi, E.; Schattenberg, J.M.; et al. Metabolic signatures across the full spectrum of non-alcoholic fatty liver disease. JHEP Rep. 2022, 4, 100477. [Google Scholar] [CrossRef]
- Tsochatzis, E.A.; Bosch, J.; Burroughs, A.K. Liver cirrhosis. Lancet 2014, 383, 1749–1761. [Google Scholar] [CrossRef]
- Mantovani, A.; Morieri, M.L.; Aldigeri, R.; Palmisano, L.; Masulli, M.; Bonomo, K.; Baroni, M.G.; Cossu, E.; Cimini, F.A.; Cavallo, G.; et al. MASLD, hepatic steatosis, and fibrosis are associated with the prevalence of chronic kidney disease and retinopathy in adults with type 1 diabetes mellitus. Diabetes Metab. 2023, 50, 101497. [Google Scholar] [CrossRef] [PubMed]
- Mantovani, A.; Petracca, G.; Beatrice, G.; Csermely, A.; Tilg, H.; Byrne, C.D.; Targher, G. Non-alcoholic fatty liver disease and increased risk of incident extrahepatic cancers: A meta-analysis of observational cohort studies. Gut 2022, 71, 778–788. [Google Scholar] [CrossRef]
- Yan, Z.; Liu, Y.; Li, W.; Zhao, X.; Lin, W.; Zhang, J.; Yu, S.; Ma, J.; Wang, J.; Yu, P.; et al. Liver fibrosis scores and prognosis in patients with cardiovascular diseases: A systematic review and meta-analysis. Eur. J. Clin. Invest. 2022, 52, e13855. [Google Scholar] [CrossRef] [PubMed]
- Roca-Fernandez, A.; Banerjee, R.; Thomaides-Brears, H.; Telford, A.; Sanyal, A.; Neubauer, S.; Nichols, T.E.; Raman, B.; McCracken, C.; Petersen, S.E.; et al. Liver disease is a significant risk factor for cardiovascular outcomes—A UK Biobank study. J. Hepatol. 2023, 79, 1085–1095. [Google Scholar] [CrossRef] [PubMed]
- Castéra, L.; Nègre, I.; Samii, K.; Buffet, C. Pain experienced during percutaneous liver biopsy. Hepatology 1999, 30, 1529–1530. [Google Scholar] [CrossRef]
- Bedossa, P.; Dargère, D.; Paradis, V. Sampling variability of liver fibrosis in chronic hepatitis C. Hepatology 2003, 38, 1449–1457. [Google Scholar] [CrossRef]
- European Association for the Study of the Liver. EASL Clinical Practice Guidelines on non-invasive tests for evaluation of liver disease severity and prognosis—2021 update. J. Hepatol. 2021, 75, 659–689. [Google Scholar] [CrossRef] [PubMed]
- Crossan, C.; Majumdar, A.; Srivastava, A.; Thorburn, D.; Rosenberg, W.; Pinzani, M.; Longworth, L.; Tsochatzis, E.A. Referral pathways for patients with NAFLD based on non-invasive fibrosis tests: Diagnostic accuracy and cost analysis. Liver Int. 2019, 39, 2052–2060. [Google Scholar] [CrossRef] [PubMed]
- Abeysekera, K.W.M.; Valenti, L.; Younossi, Z.; Dillon, J.F.; Allen, A.M.; Nourredin, M.; Rinella, M.E.; Tacke, F.; Francque, S.; Ginès, P.; et al. Implementation of a Liver Health Check in People with Type 2 Diabetes. Lancet Gastroenterol. Hepatol. 2024, 9, 83–91. [Google Scholar] [CrossRef] [PubMed]
- Trivedi, H.D.; Tran, Q.; Fricker, Z.; Curry, M.P.; Li, J.X.; Lai, M. Type 2 diabetes complications are associated with liver fibrosis independent of hemoglobin A1c. Ann. Hepatol. 2023, 28, 101087. [Google Scholar] [CrossRef] [PubMed]
- Kim, R.G.; Deng, J.; Reaso, J.N.; Grenert, J.P.; Khalili, M. Noninvasive Fibrosis Screening in Fatty Liver Disease Among Vulnerable Populations: Impact of Diabetes and Obesity on FIB-4 Score Accuracy. Diabetes Care 2022, 45, 2449–2451. [Google Scholar] [CrossRef] [PubMed]
- Gracen, L.; Hayward, K.L.; Irvine, K.M.; Valery, P.C.; Powell, E.E. Low accuracy of FIB-4 test to identify people with diabetes at low risk of advanced fibrosis. J. Hepatol. 2022, 77, 1219–1221. [Google Scholar] [CrossRef] [PubMed]
- Ajmera, V.; Cepin, S.; Tesfai, K.; Hofflich, H.; Cadman, K.; Lopez, S.; Madamba, E.; Bettencourt, R.; Richards, L.; Behling, C.; et al. A prospective study on the prevalence of NAFLD, advanced fibrosis, cirrhosis and hepatocellular carcinoma in people with type 2 diabetes. J. Hepatol. 2023, 78, 471–478. [Google Scholar] [CrossRef] [PubMed]
- Kawata, N.; Takahashi, H.; Iwane, S.; Inoue, K.; Kojima, M.; Kohno, M.; Tanaka, K.; Mori, H.; Isoda, H.; Oeda, S.; et al. FIB-4 index-based surveillance for advanced liver fibrosis in diabetes patients. Diabetol. Int. 2020, 12, 118–125. [Google Scholar] [CrossRef] [PubMed]
- Ishiba, H.; Sumida, Y.; Tanaka, S.; Yoneda, M.; Hyogo, H.; Ono, M.; Fujii, H.; Eguchi, Y.; Suzuki, Y.; Yoneda, M.; et al. The novel cutoff points for the FIB4 index categorized by age increase the diagnostic accuracy in NAFLD: A multi-center study. J. Gastroenterol. 2018, 53, 1216–1224. [Google Scholar] [CrossRef]
- Mc Pherson, S.; Hardy, T.; Dufour, J.F.; Petta, S.; Romero-Gomez, M.; Allison, M.; Oliveira, C.P.; Francque, S.; Van Gaal, L.; Schattenberg, J.M.; et al. Age as a confounding factor for the accurate non-invasive diagnosis of advanced NAFLD fibrosis. Am. J. Gastroenterol. 2017, 112, 740–751. [Google Scholar] [CrossRef]
- Kim, B.K.; Kim, D.Y.; Park, J.Y.; Ahn, S.H.; Chon, C.Y.; Kim, J.K.; Paik, Y.H.; Lee, K.S.; Park, Y.N.; Han, K.H. Validation of FIB-4 and comparison with other simple noninvasive indices for predicting liver fibrosis and cirrhosis in hepatitis B virus-infected patients. Liver Int. 2010, 30, 546–553. [Google Scholar] [CrossRef] [PubMed]
- Lekakis, V.; Papatheodoridis, G.V. Natural history of metabolic dysfunction-associated steatotic liver disease. Eur. J. Intern. Med. 2024, 122, 3–10. [Google Scholar] [CrossRef] [PubMed]
- Cholongitas, E.; Tsilingiris, D.; Diamantopoulou, P.; Mastrogianni, E.; Tentolouris, A.; Karagiannakis, D.; Moyssakis, I.; Papatheodoridis, G.V.; Tentolouris, N. Association of cardiovascular factors in diabetic patients with non-alcoholic fatty liver disease. Hormones 2022, 21, 133–145. [Google Scholar] [CrossRef] [PubMed]
- Xiao, G.; Zhu, S.; Xiao, X.; Yan, L.; Yang, J.; Wu, G. Comparison of laboratory tests, ultrasound, or magnetic resonance elastography to detect fibrosis in patients with nonalcoholic fatty liver disease: A meta-analysis. Hepatology 2017, 66, 1486–1501. [Google Scholar] [CrossRef] [PubMed]
- Chadalavada, S.; Jensen, M.T.; Aung, N.; Cooper, J.; Lekadir, K.; Munroe, P.B.; Petersen, S.E. Women with Diabetes Are at Increased Relative Risk of Heart Failure Compared to Men: Insights from UK Biobank. Front. Cardiovasc. Med. 2021, 8, 658726. [Google Scholar] [CrossRef] [PubMed]
- Yoshida, Y.; Chen, Z.; Fonseca, V.A.; Mauvais-Jarvis, F. Sex Differences in Cardiovascular Risk Associated with Prediabetes and Undiagnosed Diabetes. Am. J. Prev. Med. 2023, 65, 854–862. [Google Scholar] [CrossRef] [PubMed]
- Yaow, C.Y.L.; Chong, B.; Chin, Y.H.; Kueh, M.T.W.; Ng, C.H.; Chan, K.E.; Tang, A.S.P.; Chung, C.; Goh, R.; Kong, G.; et al. Higher risk of adverse cardiovascular outcomes in females with type 2 diabetes Mellitus: An Umbrella review of systematic reviews. Eur. J. Prev. Cardiol. 2023, 30, 1227–1235. [Google Scholar] [CrossRef] [PubMed]
- Loosen, S.H.; Kostev, K.; Keitel, V.; Tacke, F.; Roderburg, C.; Luedde, T. An elevated FIB-4 score predicts liver cancer development: A longitudinal analysis from 29,999 patients with NAFLD. J. Hepatol. 2022, 76, 247–248. [Google Scholar] [CrossRef] [PubMed]
- Zhang, X.; Wong, V.W.; Yip, T.C.; Tse, Y.K.; Liang, L.Y.; Hui, V.W.; Li, G.L.; Chan, H.L.; Wong, G.L. Colonoscopy and Risk of Colorectal Cancer in Patients with Nonalcoholic Fatty Liver Disease: A Retrospective Territory-Wide Cohort Study. Hepatol. Commun. 2021, 5, 1212–1223. [Google Scholar] [CrossRef]
- Kautzky-Willer, A.; Leutner, M.; Harreiter, J. Sex differences in type 2 diabetes. Diabetologia 2023, 66, 986–1002. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Sex (M/F) | 152/57 (72.7%/27.3%) |
| Nationality (Greek/Other) | 187/22 (89.5%/10.5%) |
| Age (years) | 67 (15) |
| Weight (kg) | 85 (110) |
| BMI (kg/m2) | 29.2 98.4) |
| HbA1c (%) | 7.2 (2.6) |
| LDL (mg/dL) | 89 (61) |
| HDL (mg/dL) | 43.5 (16) |
| Tg (mg/dL) | 147 (100) |
| FIB-4 | 1.02 (0.5) |
| Metformin (Yes/No) | 153/56 (73.2%/26.8%) |
| DPP-4 inhibitors (Yes/No) | 47/162 (22.5%/77.5%) |
| SGLT-2 inhibitors (Yes/No) | 64/145 (30.6%/69.4%) |
| GLP-1 analogs (Yes/No) | 69/140 (33%/67%) |
| Sulfonylureas (Yes/No) | 22/187 (10.5%/89.5%) |
| Pioglitazone (Yes/No) | 7/202 (3.3%/96.7%) |
| Insulin (Yes/No) | 79/130 (37.8%/62.2%) |
| Hypertension (Yes/No) | 96/113 (45.9%/54.1%) |
| CKD (Yes/No) | 14/195 (6.7%/93.3%) |
| CVD (Yes/No) | 76/133 (36.4%/63.6%) |
| Extrahepatic cancer (Yes/No) | 39/160 (18.7%/81.3%) |
| FIB-4 > 1.3 (Yes/No) | 59/150 (28.2%/71.8%) |
| Variables | Patients with CVD (n = 76, 36.4%) | Patients without CVD (n = 133, 63.6%) | p Value |
|---|---|---|---|
| Sex (M/F) | 67/9 (88.2%/11.8%) | 85/48 (63.9%/36.1%) | <0.001 |
| Age (years) | 69 (12) 68.4 ± 8.5 | 63 (16) 63.2 ± 11.5 | 0.002 |
| Weight (Kg) | 90 (25) 93 ± 18 | 84 (26) 78 ± 20.7 | 0.018 |
| BMI (Kg/m2) | 29.4 (8.4) 30.7 ± 5.4 | 28.9 (8.3) 30.4 ± 6.1 | 0.475 |
| HbA1c (%) | 7.5 (38) 7.6 ± 1.6 | 7 (2.8) 7.8 ± 2.1 | 0.938 |
| LDL (mg/dL) | 76 (38) 78.1 ± 34.6 | 105 (56) 103.4 ± 43.5 | <0.001 |
| HDL (mg/dL) | 42 (15) 42.9 ± 12.1 | 44 (15) 44.8 ± 10.3 | 0.125 |
| Tg (mg/dL) | 120 (89) 161.1 ± 103.4 | 158 (106) 182.7 ± 127.9 | 0.215 |
| FIB-4 | 1.1 (0.67) 1.26 ± 0.54 | 0.97 (0.49) 1.08 ± 0.5 | 0.012 |
| Metformin | 48 (63.2%) | 105 (77.2%) | 0.015 |
| DPP-4 inhibitors | 17 (22.4%) | 30 (22.6%) | 0.975 |
| SGLT-2 inhibitors | 31 (40.8%) | 33 (24.8%) | 0.019 |
| GLP-1 analogs | 33 (43.4%) | 36 (27.1%) | 0.021 |
| Sulfonylureas | 7 (9.2%) | 15 (11.3%) | 0.815 |
| Pioglitazone | 4 (5.3%) | 3 (2.3%) | 0.259 |
| Insulin | 30 (39.5%) | 49 (36.8%) | 0.767 |
| Hypertension | 54 (71.1%) | 22 (16.5%) | <0.001 |
| FIB-4 > 1.3 | 29 (38.2%) | 30 (22.6%) | 0.025 |
| Variables | Patients with Extrahepatic Cancer (n = 39, 18.7%) | Patients without Extrahepatic Cancer (n = 170, 81.3%) | p Value |
|---|---|---|---|
| Sex (M/F) | 28/11 (71.8%/28.2%) | 124/46 (72.9%/27.1%) | 0.845 |
| Age (years) | 67.5 (15) 68.2 ± 9.5 | 66 (14) 64.4 ± 10.9 | 0.098 |
| Weight (Kg) | 85 (13) 84.4 ± 14.9 | 86.5 (30) 90.9 ± 20.7 | 0.206 |
| BMI (Kg/m2) | 27.3 (6.4) 29 ± 4.7 | 29.7 (8.5) 30.8 ± 6 | 0.152 |
| HbA1c (%) | 7.2 (2.6) 7.5 ± 1.5 | 7.2 (2.6) 7.8 ± 2 | 0.563 |
| LDL (mg/dL) | 86 (47) 83.5 ± 31.7 | 91 (62) 96.7 ± 44 | 0.13 |
| HDL (mg/dL) | 47 (16) 45.8 ± 10.9 | 42.5 (14) 43.7 ± 11 | 0.2 |
| Tg (mg/dL) | 119.5 (101) 157.9 ± 107.1 | 150 (97) 178.8 ± 122.5 | 0.114 |
| FIB-4 | 1.13 (0.64) 1.37 ± 0.6 | 0.96 (0.5) 1.1 ± 0.5 | 0.004 |
| Metformin | 27 (69.2%) | 126 (74.1%) | 0.551 |
| DPP-4 inhibitors | 10 (25.6%) | 37 (21.7%) | 0.671 |
| SGLT-2 inhibitors | 14 (35.9%) | 50 (29.4%) | 0.445 |
| GLP-1 analogs | 9 (23.1%) | 60 (35.3%) | 0.186 |
| Sulfonylureas | 4 (10.3%) | 18 (10.6%) | 0.951 |
| Pioglitazone | 2 (5.1%) | 5 (2.9%) | 0.617 |
| Insulin | 18 (46.1%) | 61 (35.9%) | 0.273 |
| Hypertension | 19 (61.5%) | 77 (45.3%) | 0.725 |
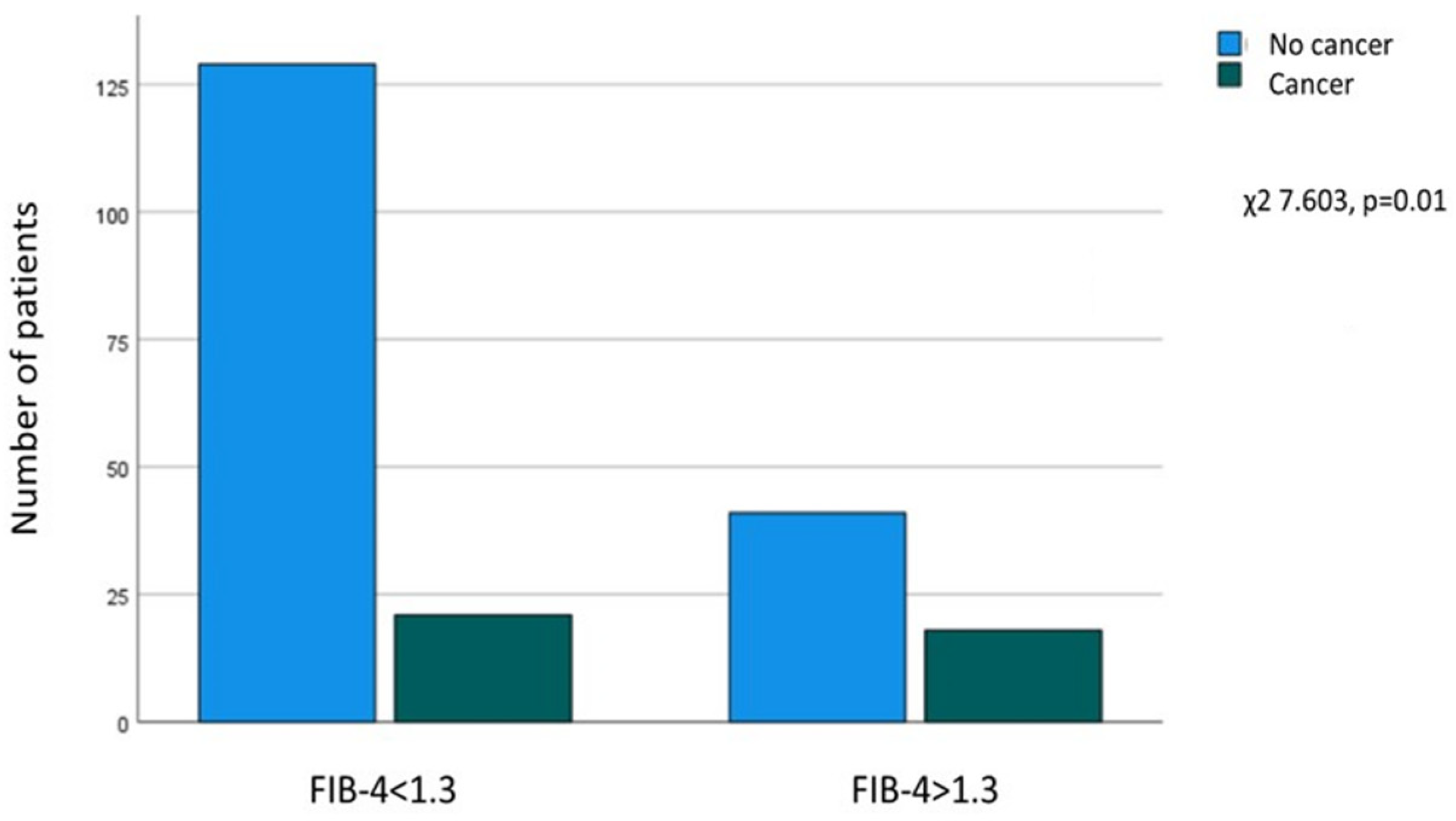
| FIB-4 > 1.3 | 18 (46.1%) | 41 (24.1%) | 0.01 |
| Variables | Patients with FIB-4 > 1.3 (n = 59, 28.2%) | Patients with FIB-4 ≤ 1.3 (n = 150, 71.8%) | p Value |
|---|---|---|---|
| Sex (M/F) | 49/10 (83%/17%) | 103/47 (68.7%/31.3%) | 0.039 |
| Age (years) | 71 (14) 70.2 ± 9.3 | 64 (14) 62.5 ± 10.9 | <0.001 |
| Weight (Kg) | 87 (16.5) 88.6 ± 13 | 85 (30) 90.5 ± 21.5 | 0.712 |
| BMI (Kg/m2) | 28.4 (8.60 30 ± 4.9 | 29.4 (8.4) 30.7 ± 6.1 | 0.683 |
| HbA1c (%) | 6.6 (1.6) 7 ± 1.3 | 7.4 (2.5) 8 ± 2.1 | <0.001 |
| LDL (mg/dL) | 71.5 (44.3) 81 ± 5 | 97 (55) 100.7 ± 40.7 | 0.003 |
| HDL (mg/dL) | 45 (14) 45.6 ± 10.3 | 43 (16) 44.2 ± 11.3 | 0.402 |
| Tg (mg/dL) | 119.5 (101) 157.9 ± 107.1 | 158 (102) 189.2 ± 131 | <0.001 |
| Metformin | 33 (55.9%) | 120 (80%) | <0.001 |
| DPP-4 inhibitors | 16 (27.1%) | 31 (20.7%) | 0.358 |
| SGLT-2 inhibitors | 25 (42.4%) | 39 (26%) | 0.03 |
| GLP-1 analogs | 18 (30.5%) | 51 (34%) | 0.744 |
| Sulfonylureas | 6 (10.2%) | 16 (10.7%) | 0.916 |
| Pioglitazone | 1 (1.7%) | 6 (4%) | 0.676 |
| Insulin | 24 (40.7%) | 55 (36.7%) | 0.636 |
| Hypertension | 31 (52.5%) | 65 (43.3%) | 0.281 |
| Univariate Analysis | Multivariate Analysis | |||||
|---|---|---|---|---|---|---|
| Variables | OR | 95%CI | p Value | OR | 95%CI | p Value |
| Age | 1.051 | 1.020–1.082 | <0.001 | |||
| Sex (male) | 0.238 | 0.109–0.519 | <0.001 | 0.266 | 0.114–0.619 | 0.002 |
| Duration of diabetes | 1.000 | 1.000–1.000 | 0.001 | 1.000 | 1.000–1.000 | 0.02 |
| Hypertension history | 5.318 | 2.872–9.846 | <0.001 | 4.685 | 2.443–8.986 | <0.001 |
| FIB-4 > 1.3 | 2.118 | 1.144–3.923 | 0.017 | 1.835 | 0.920–3.659 | 0.085 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Karagiannakis, D.S.; Stefanaki, K.; Petrea, F.; Zacharaki, P.; Giannou, A.; Michalopoulou, O.; Kazakou, P.; Psaltopoulou, T.; Vasileiou, V.; Paschou, S.A. Elevated FIB-4 Is Associated with Higher Rates of Cardiovascular Disease and Extrahepatic Cancer History in Patients with Type 2 Diabetes Mellitus. Biomedicines 2024, 12, 823. https://doi.org/10.3390/biomedicines12040823
Karagiannakis DS, Stefanaki K, Petrea F, Zacharaki P, Giannou A, Michalopoulou O, Kazakou P, Psaltopoulou T, Vasileiou V, Paschou SA. Elevated FIB-4 Is Associated with Higher Rates of Cardiovascular Disease and Extrahepatic Cancer History in Patients with Type 2 Diabetes Mellitus. Biomedicines. 2024; 12(4):823. https://doi.org/10.3390/biomedicines12040823
Chicago/Turabian StyleKaragiannakis, Dimitrios S., Katerina Stefanaki, Foteini Petrea, Panagiota Zacharaki, Alexandra Giannou, Olympia Michalopoulou, Paraskevi Kazakou, Theodora Psaltopoulou, Vasiliki Vasileiou, and Stavroula A. Paschou. 2024. "Elevated FIB-4 Is Associated with Higher Rates of Cardiovascular Disease and Extrahepatic Cancer History in Patients with Type 2 Diabetes Mellitus" Biomedicines 12, no. 4: 823. https://doi.org/10.3390/biomedicines12040823
APA StyleKaragiannakis, D. S., Stefanaki, K., Petrea, F., Zacharaki, P., Giannou, A., Michalopoulou, O., Kazakou, P., Psaltopoulou, T., Vasileiou, V., & Paschou, S. A. (2024). Elevated FIB-4 Is Associated with Higher Rates of Cardiovascular Disease and Extrahepatic Cancer History in Patients with Type 2 Diabetes Mellitus. Biomedicines, 12(4), 823. https://doi.org/10.3390/biomedicines12040823