
No Impact of Enteral Nutrition on Fecal Short-Chain Fatty Acids in Children with Cerebral Palsy

 , ,
, ,  and
and
Abstract
1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Procedures
2.3. Fecal Sample Collection
2.4. Isolation and Measurement of SCFAs Using Gas Chromatography
2.5. Statistical Analysis
3. Results
3.1. Levels of SCFAs in Fecal Samples
3.2. Molar Ratios between SCFA
4. Discussion
Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Piccioni, A.; Rosa, F.; Manca, F.; Pignataro, G.; Zanza, C.; Savioli, G.; Covino, M.; Ojetti, V.; Gasbarrini, A.; Franceschi, F.; et al. Gut Microbiota and Clostridium difficile: What We Know and the New Frontiers. Int. J. Mol. Sci. 2022, 23, 13323. [Google Scholar] [CrossRef]
- Kuźniar, A.; Szawica, D.; Wąsiewicz, E.; Fularska, K.; Oleszko, M. Human Gut Microbiome—How intestinal bacteria influence our health. J. Educ. Health Sport 2023, 22, 30–35. [Google Scholar] [CrossRef]
- Dupont, H.L.; Jiang, Z.-D.; Dupont, A.W.; Utay, N.S. The intestinal microbiome in human health and disease. Trans. Am. Clin. Climatol. Assoc. 2020, 131, 178–197. [Google Scholar] [PubMed]
- Cani, P.D.; Everard, A.; Duparc, T. Gut microbiota, enteroendocrine functions and metabolism. Curr. Opin. Pharmacol. 2013, 13, 935–940. [Google Scholar] [CrossRef]
- Shaw, A.G.; Black, N.; Rushd, A.; Sim, K.; Randell, P.; Kroll, J.S.; Epstein, J. Assessing the Colonic Microbiota in Children: Effects of Sample Site and Bowel Preparation. J. Pediatr. Gastroenterol. Nutr. 2017, 64, 230–237. [Google Scholar] [CrossRef]
- Liu, X.F.; Shao, J.H.; Liao, Y.T.; Wang, L.N.; Jia, Y.; Dong, P.J.; Liu, Z.Z.; He, D.D.; Li, C.; Zhang, X. Regulation of short fatty acids in the immune system. Front. Immunol. 2023, 14, 1186892. [Google Scholar] [CrossRef] [PubMed]
- Panthee, B.; Gyawali, S.; Panthee, P.; Techato, K. Environmental and human microbiome for health. Life 2022, 12, 456. [Google Scholar] [CrossRef]
- Gilbert, J.; Blaser, M.J.; Caporaso, J.G.; Jansson, J.K.; Lynch, S.V.; Knight, R. Current understanding of the human microbiome. Nat. Med. 2018, 10, 24. [Google Scholar] [CrossRef] [PubMed]
- Łoniewska, B.; Fraszczyk-Tousty, M.; Tousty, P.; Skonieczna-Żydecka, K.; Maciejewska-Markiewicz, D.; Łoniewski, I. Analysis of fecal short-chain fatty acids (SCFAs) in healthy children during the first two years of life: An observational prospective cohort study. Nutrients 2023, 15, 367. [Google Scholar] [CrossRef]
- Deleu, S.; Machiels, K.; Raes, J.; Verbeke, K.; Vermeire, S. Short chain fatty acids and its producing organisms: An overlooked therapy for IBD? eBioMedicine 2021, 66, 103293. [Google Scholar] [CrossRef]
- Spiljar, M.; Merkler, D.; Trajkovski, M. The Immune System Bridges the gut microbiota with systemic energy homeostasis: Focus on TLRs. Mucosal Barrier, and SCFAs. Front. Immunol. 2017, 8, 1353. [Google Scholar] [CrossRef] [PubMed]
- Rahman, S.; O’Connor, A.L.; Becker, S.L.; Patel, R.K.; Martindale, R.G.; Tsikitis, V.L. Gut microbial metabolites and its impact on human health. Ann. Gastroenterol. 2023, 36, 360–368. [Google Scholar] [CrossRef] [PubMed]
- Louis, P.; Flint, H.J. Formation of propionate and butyrate by the human colonic microbiota. Environ. Microbiol. 2017, 19, 29–41. [Google Scholar] [CrossRef] [PubMed]
- Gao, G.; Zhou, J.; Wang, H.; Ding, Y.; Zhou, J.; Chong, P.H.; Zhu, L.; Ke, L.; Wang, X.; Rao, P.; et al. Effects of valerate on intestinal barrier in cultured Caco-2 epithelial cell monolayers. Mol. Biol. Rep. 2022, 49, 1817–1825. [Google Scholar] [CrossRef] [PubMed]
- Graham, D.; Paget, S.P.; Wimalasundera, N. Current thinking in the health care management of children with cerebral palsy. Med. J. Aust. 2019, 210, 129–135. [Google Scholar] [CrossRef]
- Surveillance of Cerebral Palsy in Europe. Surveillance of cerebral palsy in Europe: A collaboration of cerebral palsy surveys and registers. Surveillance of Cerebral Palsy in Europe (SCPE). Dev. Med. Child Neurol. 2000, 42, 816–824. [Google Scholar] [CrossRef]
- Coq, J.; Delcour, M.; Massicotte, V.S.; Baud, O.; Barbe, M.F. Prenatal ischemia deteriorates white matter, brain organization, and function: Implications for prematurity and cerebral palsy. Dev. Med. Child Neurol. 2016, 58, 7–11. [Google Scholar] [CrossRef]
- Marret, S.; Vanhulle, C.; Laquerriere, A. Pathophysiology of cerebral palsy. Handb. Clin. Neurol. 2013, 111, 169–176. [Google Scholar] [CrossRef] [PubMed]
- Hillesund, E.; Skranes, J.; Trygg, K.U.; Bøhmer, T. Micronutrient status in children with cerebral palsy. Acta Paediatr. 2007, 96, 1195–1198. [Google Scholar] [CrossRef]
- Dziechciarz, P. Ocena Stanu odżywienia (in Żywienie i leczenie żywieniowe dzieci i młodzieży. In Nutrition and Nutritional Treatment in Children and Adolescents; Szajewska, H., Horvath, A., Eds.; Medycyna Praktyczna: Kraków, Poland, 2017; Volume 1, pp. 7–14. [Google Scholar]
- Nawarycz, L.O.; Krzyżaniak, A.; Nawarycz, T. Normy rozwojowe dla dzieci i młodzieży w wieku 6–18 lat opracowane na podstawie 4 województw (Developmental Standards for Children and Adolescents Aged 6–18 Developed on the Basis of 4 Voivodeships). In Żywienie i Leczenie Żywieniowe Dzieci i Młodzieży; Szajewska, H., Horvath, A., Eds.; Medycyna Praktyczna: Kraków, Polska, 2017; Volume 1, pp. 474–479. [Google Scholar]
- Kułaga, Z. Normy Rozwojowe OLA/OLAF in Żywienie i Leczenie Żywieniowe Dzieci i Młodzieży (OLA/OLAF Developmental Standards in Nutrition and Nutritional Treatment of Children and Adolescents); Szajewska, H., Horvath, A., Eds.; Medycyna Praktyczna: Kraków, Polska, 2017; Volume 1, pp. 460–467. [Google Scholar]
- Gross Motor Function Classification System. Available online: https://cerebralpalsy.org.au/cerebral-palsy/gross-motor-function-classification-system/ (accessed on 29 December 2023).
- Gonçalves, P.; Araújo, J.R.; Di Santo, J.P. A Cross-Talk Between Microbiota-Derived Short-Chain Fatty Acids and the Host Mucosal Immune System Regulates Intestinal Homeostasis and Inflammatory Bowel Disease. Inflamm. Bowel Dis. 2018, 15, 558–572. [Google Scholar] [CrossRef]
- Treem, W.R.; Ahsan, N.; Shoup, M.; Hyams, J.S. Fecal short-chain fatty acids in children with inflammatory bowel disease. J. Pediatr. Gastroenterol. Nutr. 1994, 18, 159–164. [Google Scholar] [CrossRef] [PubMed]
- Kaczmarczyk, O.; Dąbek-Drobny, A.; Woźniakiewicz, M.; Paśko, P.; Piątek-Guziewicz, A.; Zwolińska-Wcisło, M. Altered fecal short-chain fatty acid profile as a potential marker of disease activity in patients with ulcerative colitis and Crohn’s disease: A pilot study. Pol. Arch. Intern. Med. 2022, 29, 16254. [Google Scholar] [CrossRef] [PubMed]
- Ashton, J.J.; Colquhoun, C.M.; Cleary, D.W.; Coelho, T.; Haggarty, R.; Mulder, I.; Batra, A.; Afzal, N.A.; Beattie, R.M.; Scott, K.P.; et al. 16S sequencing and functional analysis of the fecal microbiome during treatment of newly diagnosed pediatric inflammatory bowel disease. Medicine 2017, 96, e7347. [Google Scholar] [CrossRef] [PubMed]
- Zhuang, X.; Li, T.; Li, M.; Huang, S.; Qiu, Y.; Feng, R.; Zhang, S.; Chen, M.; Xiong, L.; Zeng, Z. Systematic Review and Meta-analysis: Short-Chain Fatty Acid Characterization in Patients with Inflammatory Bowel Disease. Inflamm. Bowel Dis. 2019, 18, 1751–1763. [Google Scholar] [CrossRef] [PubMed]
- Gerasimidis, K.; Bertz, M.; Hanske, L.; Junick, J.; Biskou, O.; Aguilera, M.; Garrick, V.; Russell, R.K.; Blaut, M.; McGrogan, P.; et al. Decline in presumptively protective gut bacterial species and metabolites are paradoxically associated with disease improvement in pediatric Crohn’s disease during enteral nutrition. Inflamm. Bowel Dis. 2014, 20, 861–871. [Google Scholar] [CrossRef]
- Tjellström, B.; Högberg, L.; Stenhammar, L.; Magnusson, K.-E.; Midtvedt, T.; Norin, E.; Sundqvist, T. Effect of exclusive enteral nutrition on gut microflora function in children with Crohn’s disease. Scand. J. Gastroenterol. 2012, 47, 1454–1459. [Google Scholar] [CrossRef]
- Luo, M.; Zhuang, X.; Tian, Z.; Xiong, L. Alterations in short-chain fatty acids and serotonin in irritable bowel syndrome: A systematic review and meta-analysis. BMC Gastroenterol. 2021, 6, 14. [Google Scholar] [CrossRef]
- Kamil, R.Z.; Murdiati, A.; Juffrie, M.; Rahayu, E.S. Gut Microbiota Modulation of Moderate Undernutrition in Infants through Gummy Lactobacillus plantarum Dad-13 Consumption: A Randomized Double-Blind Controlled Trial. Nutrients 2022, 14, 1049. [Google Scholar] [CrossRef]
- Gordon, J.I.; Dewey, K.G.; Mills, D.A.; Medzhitov, R.M. The human gut microbiota and undernutrition. Sci. Transl. Med. 2012, 6, 137ps12. [Google Scholar] [CrossRef]
- Monira, S.; Nakamura, S.; Gotoh, K.; Izutsu, K.; Watanabe, H.; Alam, N.H.; Endtz, H.P.; Cravioto, A.; Ali, S.I.; Nakaya, T.; et al. Gut microbiota of healthy and malnourished children in Bangladesh. Front. Micribiol. 2011, 2, 228. [Google Scholar] [CrossRef]
- Kaźmierczak-Siedlecka, K.; Skonieczna-Żydecka, K.; Palma, J.; Sobocki, B.K.; Świerblewski, M.; Siedlecka-Kroplewska, K.; Kalinowski, L.; Połom, K. Microbiota-derived metabolites in colorectal cancer patients in preoperative period. Eur. Rev. Med. Pharm. Sci. 2023, 227, 1443–1449. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| SCFA | Producers |
|---|---|
| Acetate (C2) | Butyrate and propionic acid conversion with the participation of Acetobacterium, Acetogenium, Eubacterium, Clostridium spp. [9] Akkermansia muciniphila, Bacteroides spp., Bifidobacterium spp., Provotella spp., Ruminococcus spp., Blautia hydrogenotrophica, Streptococcus spp. [6] |
| Propionate (C3) | Bacteroidetes, Propionobacterium Acetate conversion with the participation of Firmicutes [9] Bacteroides spp., Dialister spp., Veilonella spp., Salmonella spp. [6] Coprococcus comes, Coprococcus eutactus, Anaerostipes spp., Coprococcus catus, Eubacterium rectale, Eubacterium hallii, Fecalibacterium prausnitzi, Roseburia spp. |
| Butyrate (C4) | Clostridium leptum. Roseburia spp., Fecalibacterium prausnitzi, Coproccus spp., Fusobacterium, Eubacterium Acetate conversion with the participation of Firmicutes [9] Coprococcus comes, Coprococcus eutactus, Anaerostipes spp., Coprococcus catus, Eubacterium rectale, Eubacterium hallii, Fecalibacterium prausnitzi, Roseburia spp. [6] |
| Valerate (C5) | Megasphaera elsdenii [7] |
| Group | Presence of Cerebral Palsy | Enteral Feeding |
|---|---|---|
| CPEN | + | + |
| CPC | + | − |
| HC | − | − |
| Characteristics | CPEN | CPC | HC |
|---|---|---|---|
| Age | 10.80 (±3.96) | 8.96 (±4.38) | 8.08 (±4.34) |
| Length/Height (cm) | 131.18 (±16.65) | 122.96 (±25.30) | 127.56 (±29.31) |
| Body mass (kg) | 22.92 (±5.95) | 22.69 (±13.66) | 32.30 (±21.90) |
| BMI | 13.30 (±2.28) | 13.93 (±3.30) | 17.50 (±3.90) |
| GMFCS | 4.767 (±0.50) | 4.21 (±0.88) | No data |
| Level | Description |
|---|---|
| Level I | Walks without limitations |
| Level II | Walks with limitations |
| Level III | Walks with a hand-held mobility device |
| Level IV | Requires physical assistance or uses powered mobility |
| Level V | Transported in a manual wheelchair in all settings |
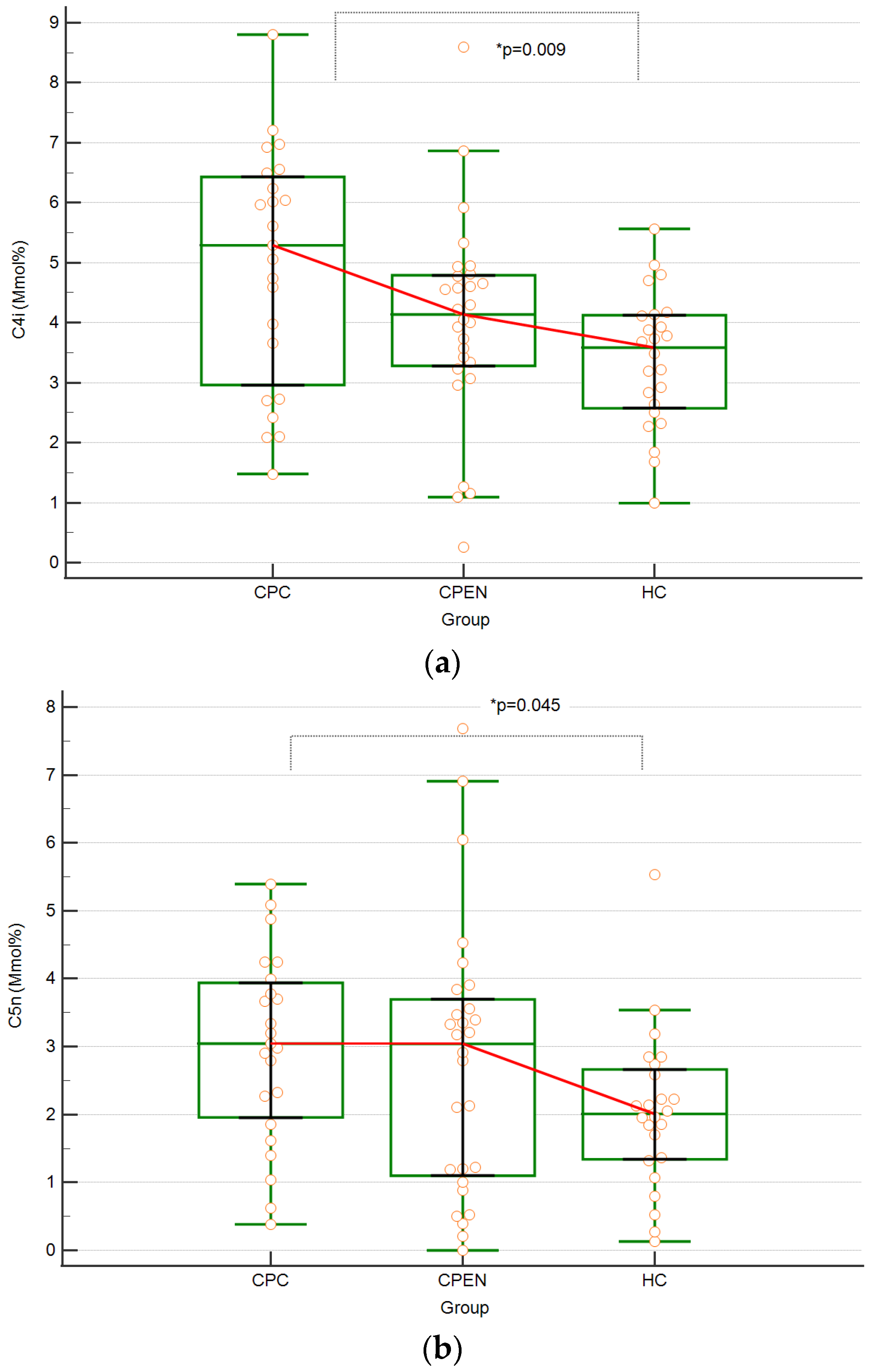
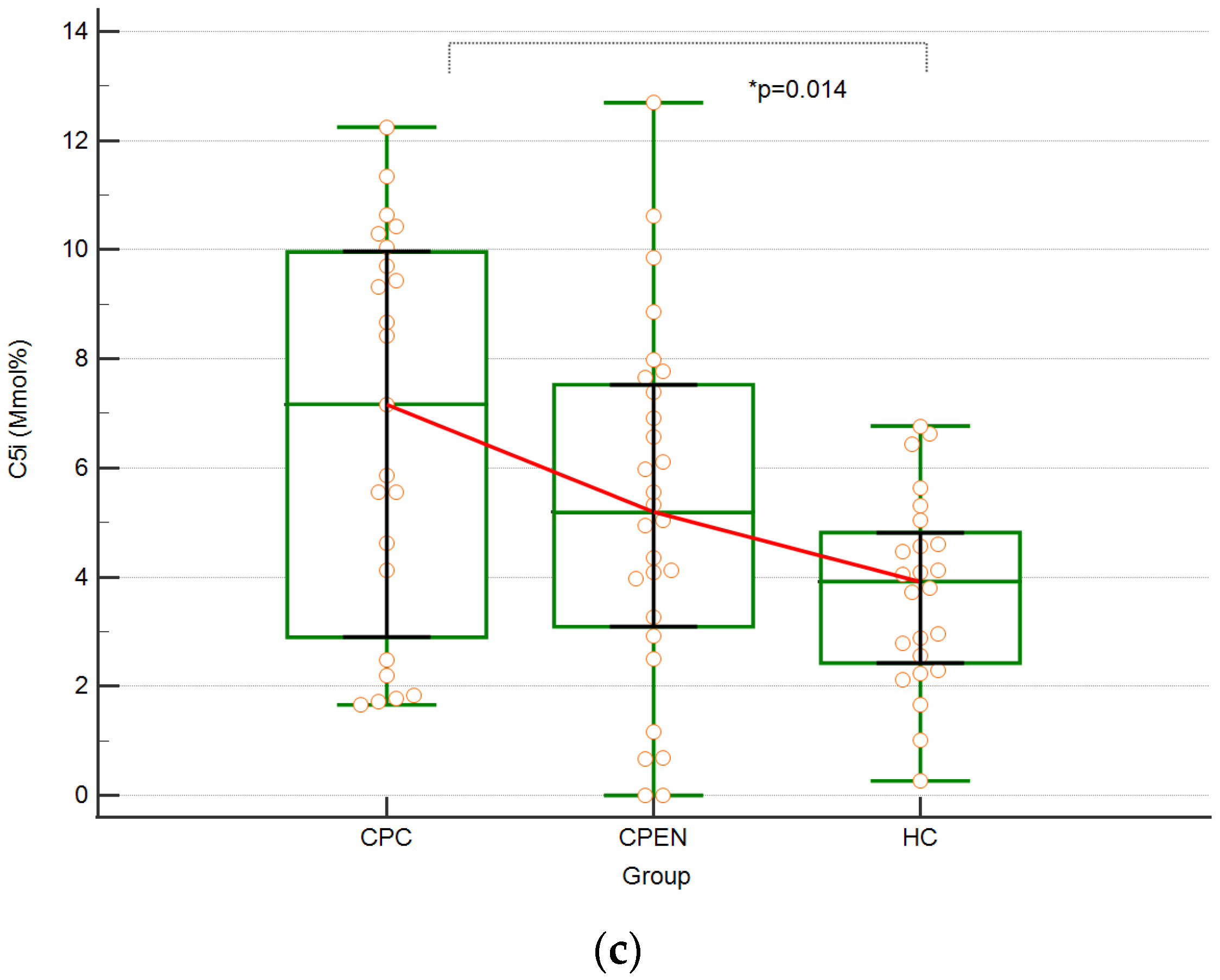
| Group | Acetic Acid (C2) [mmol%] | Propionic Acid (C3) [mmol%] | Isobutyric Acid (C4i) [mmol%] | Butyric Acid (C4n) [mmol%] | Isovaleric Acid (C5i) [mmol%] | Valeric Acid (C5n) [mmol%] | |
|---|---|---|---|---|---|---|---|
| CPEN | Median | 57.132 | 16.989 | 4.137 | 13.209 | 5.186 | 3.04 |
| Range | 41.15–85.593 | 1.156–26.126 | 0.259–8.589 | 1.737–24.353 | 0–12.696 | 0–7.686 | |
| Mean ± SD | 58.194 ± 9.775 | 15.969 ± 5.249 | 4.006 ± 1.731 | 13.805 ± 5.225 | 5.251 ± 3.246 | 2.775 ± 1.992 | |
| CPC | Median | 53.617 | 14.993 | 5.29 | 15.346 | 7.169 | 3.045 |
| Range | 43.973–64.512 | 9.951–20.097 | 1.479–8.804 | 9.122–31.099 | 1.758–12.247 | 0.384–5.395 | |
| Mean ± SD | 53.739 ± 6.032 | 15.008 ± 2.713 | 4.942 ± 1.977 | 16.577 ± 4.646 | 6.745 ± 3.618 | 2.99 ± 1.392 | |
| HC | Median | 58.902 | 16.012 | 3.585 | 15.398 | 3.921 | 2.01 |
| Range | 44.128–71.315 | 0.55–24.31 | 0.992–5.565 | 6.705–27.192 | 0.263–6.77 | 0.131–5.538 | |
| Mean ± SD | 57.979 ± 5.781 | 16.995 ± 3.608 | 3.39 ± 1.1202 | 15.852 ± 4.228 | 3.749 ± 1.735 | 2.036 ± 1.155 | |
| p-value | p = 0.09 | p = 0.15 | p = 0.009 | p = 0.11 | p = 0.014 | p = 0.045 |
| Group | (C2 + C3 + C4) Median Range Mean ± SD | C2 Median Range Mean ± SD | C3 Median Range Mean ± SD | C4 Median Range Mean ± SD |
|---|---|---|---|---|
| Recommendation | 95 (%) | 3 | 1 | 1 |
| CPEN | 92.09 (%) | 3.15 | 0.91 | 0.97 |
| 82.47–100 | 2.25–4.27 | 0.06–1.39 | 0.37–1.70 | |
| 91.97 ± 4.80 | 3.15 ± 0.42 | 0.87 ± 0.28 | 0.98 ± 0.31 | |
| Lower than recommended | 64.29% (n = 18) | 42.86% (n = 12) | 60.71% (n = 17) | 53.57% (n = 15) |
| CPC | 88.46 | 2.95 | 0.85 | 1.24 |
| 82.87–97.18 | 2.55–3.35 | 0.52–1.03 | 0.79–1.68 | |
| 89.93 ± 4.58 | 2.96 ± 0.21 | 0.82 ± 0.14 | 1.22 ± 0.25 | |
| Lower than recommended | 69.57% (n = 16) | 56.52% (n = 13) | 82.61% (n = 19) | 26.09% (n = 6) |
| HC | 94.44 | 3.13 | 0.86 | 1.02 |
| 89.16–99.21 | 2.47–0.55 | 0.55–1.28 | 0.52–1.42 | |
| 94.22 ± 2.47 | 3.07 ± 0.27 | 0.90 ± 0.19 | 1.02 ± 0.24 | |
| Lower than recommended | 66.67% (n = 16) | 37.5% (n = 9) | 70.83% (n = 17) | 33.33% (n = 8) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mickiewicz-Góra, D.; Sznurkowska, K.; Drozd, A.; Borkowska, A.; Zagierski, M.; Troch, J.; Skonieczna-Żydecka, K.; Szlagatys-Sidorkiewicz, A. No Impact of Enteral Nutrition on Fecal Short-Chain Fatty Acids in Children with Cerebral Palsy. Biomedicines 2024, 12, 897. https://doi.org/10.3390/biomedicines12040897
Mickiewicz-Góra D, Sznurkowska K, Drozd A, Borkowska A, Zagierski M, Troch J, Skonieczna-Żydecka K, Szlagatys-Sidorkiewicz A. No Impact of Enteral Nutrition on Fecal Short-Chain Fatty Acids in Children with Cerebral Palsy. Biomedicines. 2024; 12(4):897. https://doi.org/10.3390/biomedicines12040897
Chicago/Turabian StyleMickiewicz-Góra, Dorota, Katarzyna Sznurkowska, Arleta Drozd, Anna Borkowska, Maciej Zagierski, Joanna Troch, Karolina Skonieczna-Żydecka, and Agnieszka Szlagatys-Sidorkiewicz. 2024. "No Impact of Enteral Nutrition on Fecal Short-Chain Fatty Acids in Children with Cerebral Palsy" Biomedicines 12, no. 4: 897. https://doi.org/10.3390/biomedicines12040897
APA StyleMickiewicz-Góra, D., Sznurkowska, K., Drozd, A., Borkowska, A., Zagierski, M., Troch, J., Skonieczna-Żydecka, K., & Szlagatys-Sidorkiewicz, A. (2024). No Impact of Enteral Nutrition on Fecal Short-Chain Fatty Acids in Children with Cerebral Palsy. Biomedicines, 12(4), 897. https://doi.org/10.3390/biomedicines12040897