
Investigation of Lung Cancer Cell Response to Cryoablation and Adjunctive Gemcitabine-Based Cryo-Chemotherapy Using the A549 Cell Line

 ,
,
Abstract
1. Introduction
2. Materials and Methods
2.1. Cell Culture
2.2. Gemcitibine Exposure
2.3. Freeze Procedure
2.4. Cell Viability Assessment
2.5. Flow Cytometry Assessment of the Modes of Cell Death
2.6. Protien Immunoblot Analysis
2.7. Data Analysis
3. Results
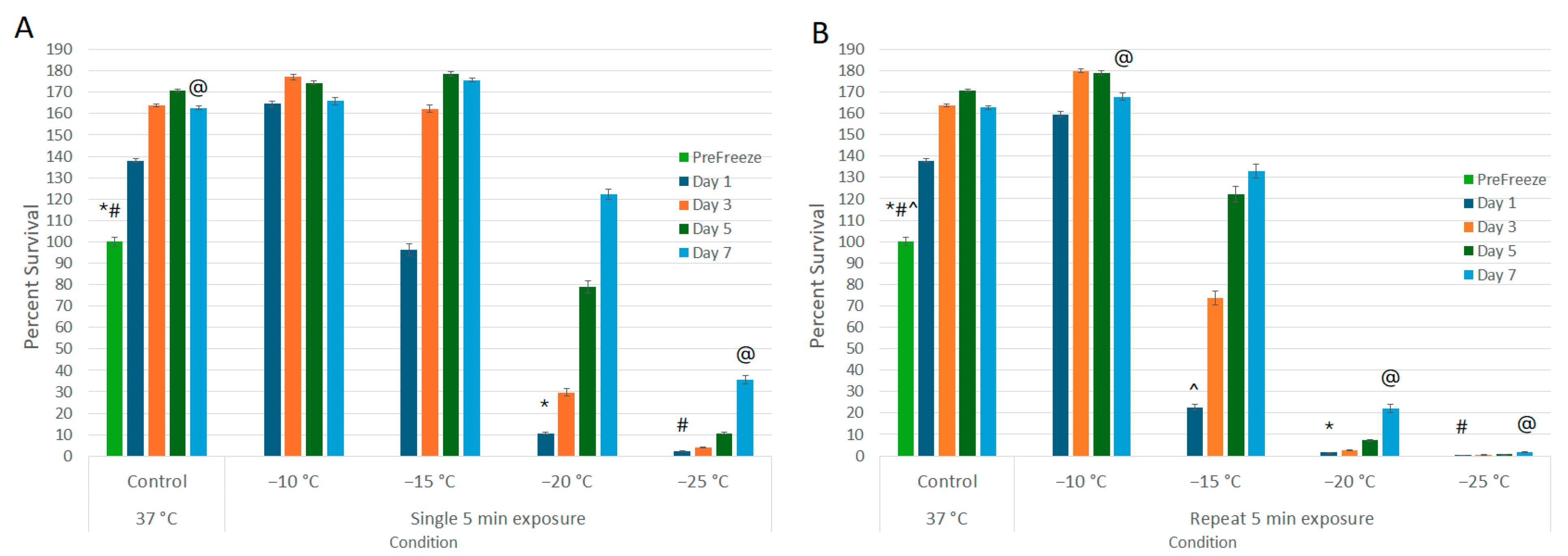
3.1. Establishment of the Minimal Lethal Temperature for A549 Cells
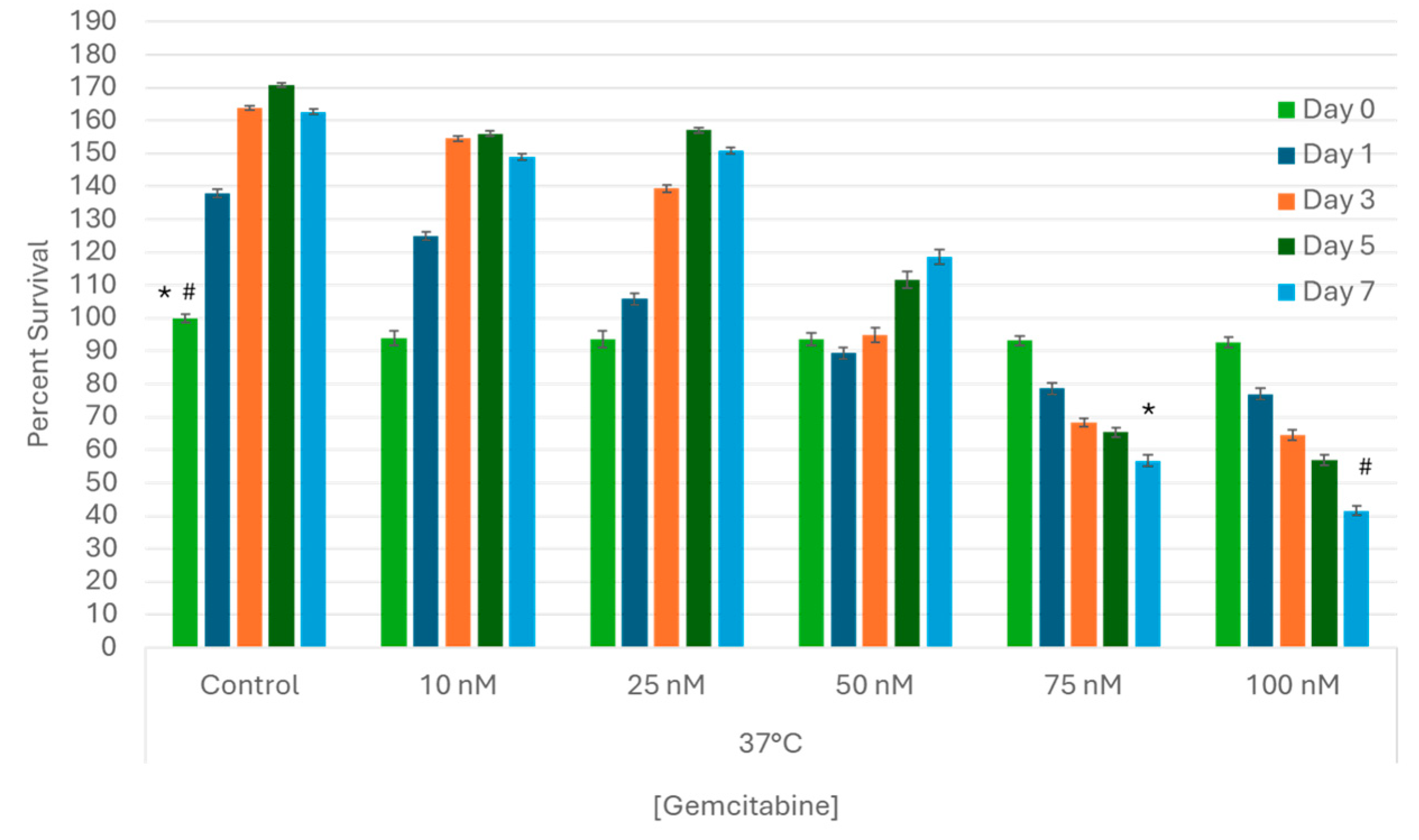
3.2. Establishment of the Gemcitabine LC50 for A549 Cells In Vitro
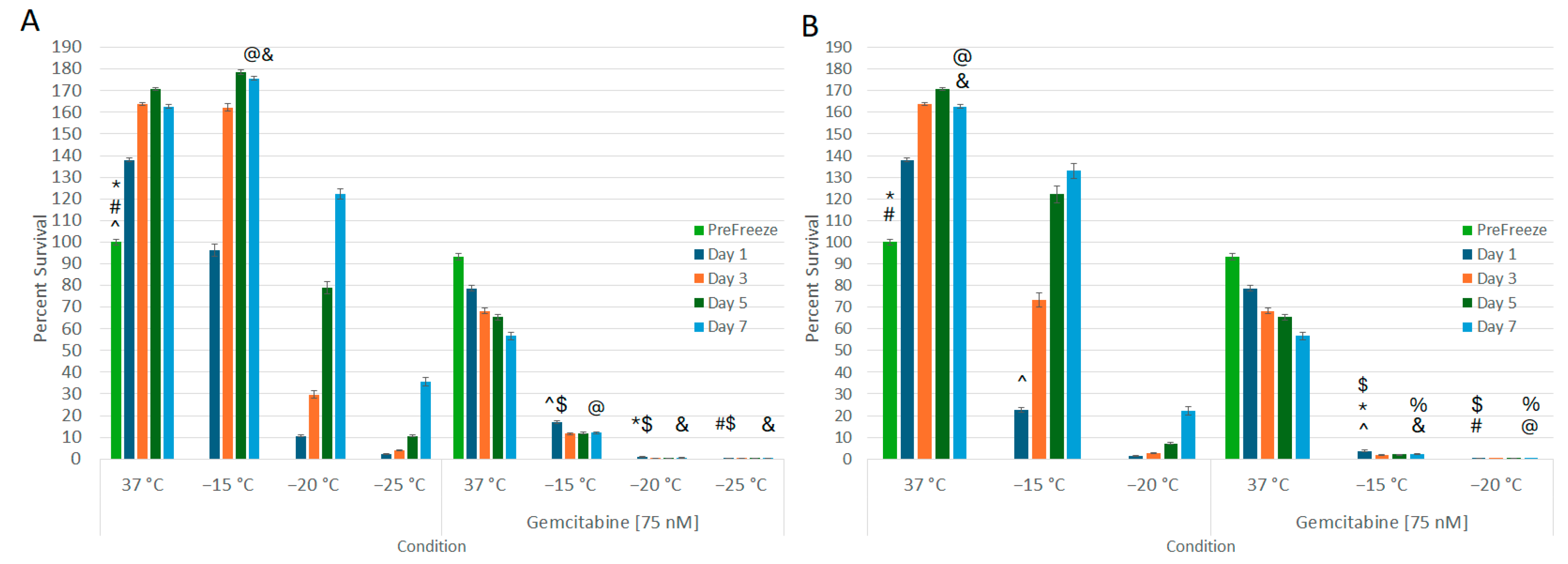
3.3. Impact of Combination Gemcitabine Pretreatment and Freezing
3.4. Assessment of the Mode of Cell Death Activated following Treatment
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- American Cancer Society. Facts & Figures 2023; American Cancer Society: Atlanta, GA, USA, 2024. [Google Scholar]
- Kratzer, T.B.; Bandi, P.; Freedman, N.D.; Smith, R.A.; Travis, W.D.; Jemal, A.; Siegel, R.L. Lung cancer statistics, 2023. Cancer 2024, 130, 1330–1348. [Google Scholar] [CrossRef]
- Molina, J.R.; Yang, P.; Cassivi, S.D.; Schild, S.E.; Adjei, A.A. Non-small cell lung cancer: Epidemiology, risk factors, treatment, and survivorship. Mayo Clin. Proc. 2008, 83, 584–594. [Google Scholar] [CrossRef]
- Remon, J.; Soria, J.C.; Peters, S. Early and locally advanced non-small-cell lung cancer: An update of the ESMO Clinical Practice Guidelines focusing on diagnosis, staging, systemic and local therapy. Ann. Oncol. 2021, 32, 1637–1642. [Google Scholar] [CrossRef]
- Ettinger, D.S.; Wood, D.E.; Aisner, D.L.; Akerley, W.; Bauman, J.R.; Bharat, A.; Bruno, D.S.; Chang, J.Y.; Chirieac, L.R.; D’Amico, T.A.; et al. Non-Small Cell Lung Cancer, Version 3.2022, NCCN Clinical Practice Guidelines in Oncology. J. Natl. Compr. Canc Netw. 2022, 20, 497–530. [Google Scholar] [CrossRef]
- Xu, Z.; Wang, X.; Ke, H.; Lyu, G. Cryoablation is superior to radiofrequency ablation for the treatment of non-small cell lung cancer: A meta-analysis. Cryobiology 2023, 112, 104560. [Google Scholar] [CrossRef]
- Zhang, X.; Tian, J.; Zhao, L.; Wu, B.; Kacher, D.S.; Ma, X.; Liu, S.; Ren, C.; Xiao, Y.Y. CT-guided conformal cryoablation for peripheral NSCLC: Initial experience. Eur. J. Radiol. 2012, 81, 3354–3362. [Google Scholar] [CrossRef]
- Yamauchi, Y.; Izumi, Y.; Hashimoto, K.; Yashiro, H.; Inoue, M.; Nakatsuka, S.; Goto, T.; Anraku, M.; Ohtsuka, T.; Kohno, M.; et al. Percutaneous cryoablation for the treatment of medically inoperable stage I non-small cell lung cancer. PLoS ONE 2012, 7, e33223. [Google Scholar] [CrossRef]
- Yamauchi, Y.; Izumi, Y.; Kawamura, M.; Nakatsuka, S.; Yashiro, H.; Tsukada, N.; Inoue, M.; Asakura, K.; Nomori, H. Percutaneous cryoablation of pulmonary metastases from colorectal cancer. PLoS ONE 2011, 6, e27086. [Google Scholar] [CrossRef]
- Eiken, P.W.; Welch, B.T. Cryoablation of Lung Metastases: Review of Recent Literature and Ablation Technique. Semin. Intervent Radiol. 2019, 36, 319–325. [Google Scholar] [CrossRef]
- Callstrom, M.R.; Woodrum, D.A.; Nichols, F.C.; Palussiere, J.; Buy, X.; Suh, R.D.; Abtin, F.G.; Pua, B.B.; Madoff, D.C.; Bagla, S.L.; et al. Multicenter Study of Metastatic Lung Tumors Targeted by Interventional Cryoablation Evaluation (SOLSTICE). J. Thorac. Oncol. 2020, 15, 1200–1209. [Google Scholar] [CrossRef]
- Kawamura, M.; Izumi, Y.; Tsukada, N.; Asakura, K.; Sugiura, H.; Yashiro, H.; Nakano, K.; Nakatsuka, S.; Kuribayashi, S.; Kobayashi, K. Percutaneous cryoablation of small pulmonary malignant tumors under computed tomographic guidance with local anesthesia for nonsurgical candidates. J. Thorac. Cardiovasc. Surg. 2006, 131, 1007–1013. [Google Scholar] [CrossRef]
- Bourgouin, P.P.; Wrobel, M.M.; Mercaldo, N.D.; Murphy, M.C.; Leppelmann, K.S.; Levesque, V.M.; Muniappan, A.; Silverman, S.G.; Shepard, J.O.; Shyn, P.B.; et al. Comparison of Percutaneous Image-Guided Microwave Ablation and Cryoablation for Sarcoma Lung Metastases: A 10-Year Experience. AJR Am. J. Roentgenol. 2022, 218, 494–504. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Y.S.; Niu, L.Z.; Zhan, K.; Li, Z.H.; Huang, Y.G.; Yang, Y.; Chen, J.B.; Xu, K.C. Percutaneous imaging-guided cryoablation for lung cancer. J. Thorac. Dis. 2016, 8, S705–S709. [Google Scholar] [CrossRef] [PubMed]
- Vyas, V.; Paul, M. Catastrophic complications following cryoablation of lung cancer. Proceedings (Bayl. Univ. Med. Cent) 2020, 34, 131–132. [Google Scholar] [CrossRef]
- Baust, J.G.; Gage, A.A.; Bjerklund Johansen, T.E.; Baust, J.M. Mechanisms of cryoablation: Clinical consequences on malignant tumors. Cryobiology 2014, 68, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Baust, J.M.; Rabin, Y.; Polascik, T.J.; Santucci, K.L.; Snyder, K.K.; Buskirk, R.G.V.; Baust, J.G. Defeating Cancers’ Adaptive Defensive Strategies Using Thermal Therapies: Examining Cancer’s Therapeutic Resistance, Ablative, and Computational Modeling Strategies as a means for Improving Therapeutic Outcome. Technol. Cancer Res. Treat. 2018, 17, 1–16. [Google Scholar] [CrossRef] [PubMed]
- Gage, A.A.; Baust, J.M.; Baust, J.G. Experimental cryosurgery investigations in vivo. Cryobiology 2009, 59, 229–243. [Google Scholar] [CrossRef] [PubMed]
- Baust, J.M.; Santucci, K.L.; Van Buskirk, R.G.; Raijman, I.; Fisher, W.E.; Baust, J.G.; Snyder, K.K. An In Vitro Investigation into Cryoablation and Adjunctive Cryoablation/Chemotherapy Combination Therapy for the Treatment of Pancreatic Cancer Using the PANC-1 Cell Line. Biomedicines 2022, 10, 450. [Google Scholar] [CrossRef] [PubMed]
- Santucci, K.L.; Snyder, K.K.; Baust, J.G.; Van Buskirk, R.G.; Baust, J.M. Investigation of Liver Cancer Cell Response to Cryoablation and Adjunctive Based Cryo/Chemotherapy. Br. J. Cancer Res. 2020, 3, 407–414. [Google Scholar] [CrossRef]
- Snyder, K.K.; Van Buskirk, R.G.; Baust, J.G.; Baust, J.M. Breast Cancer Cryoablation: Assessment of the Impact of Fundamental Procedural Variables in an In Vitro Human Breast Cancer Model. Breast Cancer Basic. Clin. Res. 2020, 14, 1–9. [Google Scholar] [CrossRef]
- Robilotto, A.T.; Santucci, K.L.; Snyder, K.K.; Van Buskirk, R.G.; Baust, J.G.; Baust, J.M. Assessment of a novel supercritical nitrogen cryosurgical device using prostate and renal cancer tissue engineered models. Med. Devices Diagn. Eng. 2020, 5, 1–8. [Google Scholar] [CrossRef]
- Baust, J.M.; Robilotto, A.; Snyder, K.K.; Santucci, K.; Stewart, J.; Van Buskirk, R.; Baust, J.G. Assessment of Cryosurgical Device Performance Using a 3D Tissue-Engineered Cancer Model. Technol. Cancer Res. Treat. 2017, 16, 900–909. [Google Scholar] [CrossRef] [PubMed]
- Hinshaw, J.L.; Lee, F.T., Jr.; Laeseke, P.F.; Sampson, L.A.; Brace, C. Temperature isotherms during pulmonary cryoablation and their correlation with the zone of ablation. J. Vasc. Interv. Radiol. 2010, 21, 1424–1428. [Google Scholar] [CrossRef] [PubMed]
- McDevitt, J.L.; Mouli, S.K.; Nemcek, A.A.; Lewandowski, R.J.; Salem, R.; Sato, K.T. Percutaneous Cryoablation for the Treatment of Primary and Metastatic Lung Tumors: Identification of Risk Factors for Recurrence and Major Complications. J. Vasc. Interv. Radiol. 2016, 27, 1371–1379. [Google Scholar] [CrossRef] [PubMed]
- Permpongkosol, S.; Nicol, T.L.; Link, R.E.; Varkarakis, I.; Khurana, H.; Zhai, Q.J.; Kavoussi, L.R.; Solomon, S.B. Differences in ablation size in porcine kidney, liver, and lung after cryoablation using the same ablation protocol. AJR Am. J. Roentgenol. 2007, 188, 1028–1032. [Google Scholar] [CrossRef] [PubMed]
- Robilotto, A.T.; Baust, J.M.; Van Buskirk, R.G.; Gage, A.A.; Baust, J.G. Temperature-dependent activation of differential apoptotic pathways during cryoablation in a human prostate cancer model. Prostate Cancer Prostatic Dis. 2013, 16, 41–49. [Google Scholar] [CrossRef] [PubMed]
- Clarke, D.M.; Baust, J.M.; Van Buskirk, R.G.; Baust, J.G. Chemo-cryo combination therapy: An adjunctive model for the treatment of prostate cancer. Cryobiology 2001, 42, 274–285. [Google Scholar] [CrossRef] [PubMed]
- Clarke, D.M.; Baust, J.M.; Van Buskirk, R.G.; Baust, J.G. Addition of anticancer agents enhances freezing-induced prostate cancer cell death: Implications of mitochondrial involvement. Cryobiology 2004, 49, 45–61. [Google Scholar] [CrossRef] [PubMed]
- Clarke, D.M.; Robilotto, A.T.; Van Buskirk, R.G.; Baust, J.G.; Gage, A.A.; Baust, J.M. Targeted induction of apoptosis via TRAIL and cryoablation: A novel strategy for the treatment of prostate cancer. Prostate Cancer Prostatic Dis. 2007, 10, 175–184. [Google Scholar] [CrossRef]
- Goel, R.; Swanlund, D.; Coad, J.; Paciotti, G.F.; Bischof, J.C. TNF-alpha-based accentuation in cryoinjury--dose, delivery, and response. Mol. Cancer Ther. 2007, 6, 2039–2047. [Google Scholar] [CrossRef]
- Liu, C.; Cao, F.; Xing, W.; Si, T.; Yu, H.; Yang, X.; Guo, Z. Efficacy of cryoablation combined with sorafenib for the treatment of advanced renal cell carcinoma. Int. J. Hyperthermia 2019, 36, 220–228. [Google Scholar] [CrossRef] [PubMed]
- Clarke, D.M.; Robilotto, A.T.; Rhee, E.; VanBuskirk, R.G.; Baust, J.G.; Gage, A.A.; Baust, J.M. Cryoablation of renal cancer: Variables involved in freezing-induced cell death. Technol. Cancer Res. Treat. 2007, 6, 69–79. [Google Scholar] [CrossRef] [PubMed]
- Medlej, Z.A.A.; Medlej, W.; Slaba, S.; Torrecillas, P.; Cueto, A.; Urbaneja, A.; Garrido, A.J.; Lugnani, F. Cryoablation and Immunotherapy: An Enthralling Synergy for Cancer Treatment. Curr. Oncol. 2023, 30, 4844–4860. [Google Scholar] [CrossRef]
- Han, B.; Swanlund, D.J.; Bischof, J.C. Cryoinjury of MCF-7 human breast cancer cells and inhibition of post-thaw recovery using TNF-alpha. Technol. Cancer Res. Treat. 2007, 6, 625–634. [Google Scholar] [CrossRef] [PubMed]
- Wang, C.L.; Teo, K.Y.; Han, B. An amino acidic adjuvant to augment cryoinjury of MCF-7 breast cancer cells. Cryobiology 2008, 57, 52–59. [Google Scholar] [CrossRef] [PubMed]
- Hou, Y.; Sun, X.; Yao, S.; Rao, W.; He, X. Cryoablation-activated enhanced nanodoxorubicin release for the therapy of chemoresistant mammary cancer stem-like cells. J. Mater. Chem. B 2020, 8, 908–918. [Google Scholar] [CrossRef] [PubMed]
- Gu, X.Y.; Jiang, Z.; Fang, W. Cryoablation combined with molecular target therapy improves the curative effect in patients with advanced non-small cell lung cancer. J. Int. Med. Res. 2011, 39, 1736–1743. [Google Scholar] [CrossRef] [PubMed]
- Forest, V.; Peoc’h, M.; Campos, L.; Guyotat, D.; Vergnon, J.M. Benefit of a combined treatment of cryotherapy and chemotherapy on tumour growth and late cryo-induced angiogenesis in a non-small-cell lung cancer model. Lung Cancer 2006, 54, 79–86. [Google Scholar] [CrossRef]
- Yuanying, Y.; Lizhi, N.; Feng, M.; Xiaohua, W.; Jianying, Z.; Fei, Y.; Feng, J.; Lihua, H.; Jibing, C.; Jialiang, L.; et al. Therapeutic outcomes of combining cryotherapy, chemotherapy and DC-CIK immunotherapy in the treatment of metastatic non-small cell lung cancer. Cryobiology 2013, 67, 235–240. [Google Scholar] [CrossRef]
- Feng, J.; Guiyu, D.; Xiongwen, W. The clinical efficacy of argon-helium knife cryoablation combined with nivolumab in the treatment of advanced non-small cell lung cancer. Cryobiology 2021, 102, 92–96. [Google Scholar] [CrossRef]
- Goel, R.; Anderson, K.; Slaton, J.; Schmidlin, F.; Vercellotti, G.; Belcher, J.; Bischof, J.C. Adjuvant approaches to enhance cryosurgery. J. Biomech. Eng. 2009, 131, 074003. [Google Scholar] [CrossRef]
- Han, B.; Iftekhar, A.; Bischof, J.C. Improved cryosurgery by use of thermophysical and inflammatory adjuvants. Technol. Cancer Res. Treat. 2004, 3, 103–111. [Google Scholar] [CrossRef]
- Jiang, X.; Ji, Z.; Lei, X.; He, Y.; Yuan, F. Cryotherapy for low rectal and anal cancer: Recommendation and indications. Front. Oncol. 2023, 13, 984145. [Google Scholar] [CrossRef]
- Reck, M.; Rabe, K.F. Precision Diagnosis and Treatment for Advanced Non-Small-Cell Lung Cancer. N. Engl. J. Med. 2017, 377, 849–861. [Google Scholar] [CrossRef]
- Baust, J.G.; Bischof, J.C.; Jiang-Hughes, S.; Polascik, T.J.; Rukstalis, D.B.; Gage, A.A.; Baust, J.M. Re-purposing cryoablation: A combinatorial ‘therapy’ for the destruction of tissue. Prostate Cancer Prostatic Dis. 2015, 18, 87–95. [Google Scholar] [CrossRef] [PubMed]
- Jiang, J.; Goel, R.; Iftekhar, M.A.; Visaria, R.; Belcher, J.D.; Vercellotti, G.M.; Bischof, J.C. Tumor necrosis factor-alpha-induced accentuation in cryoinjury: Mechanisms in vitro and in vivo. Mol. Cancer Ther. 2008, 7, 2547–2555. [Google Scholar] [CrossRef] [PubMed]
- Pereira, M.; Vale, N. Two Possible Strategies for Drug Modification of Gemcitabine and Future Contributions to Personalized Medicine. Molecules 2022, 27, 291. [Google Scholar] [CrossRef] [PubMed]
- Santos, E.S.; Rodriguez, E. Treatment Considerations for Patients With Advanced Squamous Cell Carcinoma of the Lung. Clin. Lung Cancer 2022, 23, 457–466. [Google Scholar] [CrossRef]
- Miller, M.; Hanna, N. Advances in systemic therapy for non-small cell lung cancer. BMJ 2021, 375, n2363. [Google Scholar] [CrossRef]
- Shu, Y.; Weng, S.; Zheng, S. Metronomic chemotherapy in non-small cell lung cancer. Oncol. Lett. 2020, 20, 307. [Google Scholar] [CrossRef]
- American Cancer Society. Chemotherapy for Non-Small Cell Lung Cancer. Available online: https://www.cancer.org/cancer/types/lung-cancer/treating-non-small-cell/chemotherapy.html (accessed on 9 May 2024).
- American Cancer Society. Treatment Choices for Non-Small Cell Lung Cancer, by Stage. Available online: https://www.cancer.org/cancer/types/lung-cancer/treating-non-small-cell/by-stage.html (accessed on 22 November 2023).
- Mornex, F.; Girard, N. Gemcitabine and radiation therapy in non-small cell lung cancer: State of the art. Ann. Oncol. 2006, 17, 1743–1747. [Google Scholar] [CrossRef]
- Zhang, X.; Wang, D.; Li, Z.; Jiao, D.; Jin, L.; Cong, J.; Zheng, X.; Xu, L. Low-Dose Gemcitabine Treatment Enhances Immunogenicity and Natural Killer Cell-Driven Tumor Immunity in Lung Cancer. Front. Immunol. 2020, 11, 331. [Google Scholar] [CrossRef] [PubMed]
- Hayashi, H.; Kurata, T.; Nakagawa, K. Gemcitabine: Efficacy in the treatment of advanced stage nonsquamous non-small cell lung cancer. Clin. Med. Insights Oncol. 2011, 5, 177–184. [Google Scholar] [CrossRef]
- Burkes, R.L.; Shepherd, F.A. Gemcitabine in the treatment of non-small-cell lung cancer. Ann. Oncol. 1995, 6 (Suppl. S3), S57–S60. [Google Scholar] [CrossRef]
- Klossner, D.P.; Robilotto, A.T.; Clarke, D.M.; Van Buskirk, R.G.; Baust, J.M.; Gage, A.A.; Baust, J.G. Cryosurgical technique: Assessment of the fundamental variables using human prostate cancer model systems. Cryobiology 2007, 55, 189–199. [Google Scholar] [CrossRef]
- Snyder, K.K.; Baust, J.M.; Van Buskirk, R.G.; Baust, J.G. Cardiomyocyte Responses to Thermal Excursions: Implications for Electrophysiological Cardiac Mapping. Cell Preserv. Technol. 2007, 5, 116–128. [Google Scholar] [CrossRef]
- Goff, R.P.; Quallich, S.G.; Buechler, R.A.; Bischof, J.C.; Iaizzo, P.A. Determination of cryothermal injury thresholds in tissues impacted by cardiac cryoablation. Cryobiology 2017, 75, 125–133. [Google Scholar] [CrossRef] [PubMed]
- Cox, J.L.; Malaisrie, S.C.; Churyla, A.; Mehta, C.; Kruse, J.; Kislitsina, O.N.; McCarthy, P.M. Cryosurgery for Atrial Fibrillation: Physiologic Basis for Creating Optimal Cryolesions. Ann. Thorac. Surg. 2021, 112, 354–362. [Google Scholar] [CrossRef] [PubMed]
- Larson, T.R.; Rrobertson, D.W.; Corica, A.; Bostwick, D.G. In vivo interstitial temperature mapping of the human prostate during cryosurgery with correlation to histopathologic outcomes. Urology 2000, 55, 547–552. [Google Scholar] [CrossRef]
- Santucci, K.L.; Baust, J.M.; Snyder, K.K.; Van Buskirk, R.G.; Katz, A.; Corcoran, A.; Baust, J.G. Investigation of Bladder Cancer Cell Response to Cryoablation and Adjunctive Cisplatin Based Cryo/Chemotherapy. Clin. Res. Open Access 2020, 6, 1–10. [Google Scholar] [CrossRef]
- Baust, J.M.; Corcoran, A.; Robilotto, A.T.; Katz, A.E.; Santucci, K.L.; Van Buskirk, R.G.; Baust, J.G.; Snyder, K.K. Evaluation of a New Cystoscopic Cryocatheter and Method for the In Situ Destruction of Bladder Cancer: Preliminary In Vivo Study. J. Endourol. 2024, 38, 513–520. [Google Scholar] [CrossRef] [PubMed]
- Littrup, P.J.; Jallad, B.; Vorugu, V.; Littrup, G.; Currier, B.; George, M.; Herring, D. Lethal isotherms of cryoablation in a phantom study: Effects of heat load, probe size, and number. J. Vasc. Interv. Radiol. 2009, 20, 1343–1351. [Google Scholar] [CrossRef] [PubMed]
- Shah, T.T.; Arbel, U.; Foss, S.; Zachman, A.; Rodney, S.; Ahmed, H.U.; Arya, M. Modeling Cryotherapy Ice Ball Dimensions and Isotherms in a Novel Gel-based Model to Determine Optimal Cryo-needle Configurations and Settings for Potential Use in Clinical Practice. Urology 2016, 91, 234–240. [Google Scholar] [CrossRef] [PubMed]
- Kaseda, K.; Asakura, K.; Nishida, R.; Okubo, Y.; Masai, K.; Hishida, T.; Inoue, M.; Yashiro, H.; Nakatsuka, S.; Jinzaki, M.; et al. Feasibility and safety of percutaneous cryoablation under local anesthesia for the treatment of malignant lung tumors: A retrospective cohort study. J. Thorac. Dis. 2022, 14, 4297–4308. [Google Scholar] [CrossRef] [PubMed]
- Pusceddu, C.; Sotgia, B.; Fele, R.M.; Melis, L. CT-guided thin needles percutaneous cryoablation (PCA) in patients with primary and secondary lung tumors: A preliminary experience. Eur. J. Radiol. 2013, 82, e246–e253. [Google Scholar] [CrossRef] [PubMed]
- Shepherd, R.W.; Radchenko, C. Bronchoscopic ablation techniques in the management of lung cancer. Ann. Transl. Med. 2019, 7, 362. [Google Scholar] [CrossRef] [PubMed]
- Gu, C.; Yuan, H.; Yang, C.; Xie, F.; Chen, J.; Zhu, L.; Jiang, Y.; Sun, J. Transbronchial cryoablation in peripheral lung parenchyma with a novel thin cryoprobe and initial clinical testing. Thorax 2024. [Google Scholar] [CrossRef] [PubMed]
- Ebrahim, A.S. bronchoscopic cryo-ablation of endobronchial lung cancer: Predictors of recanalization. Eur. Respir. J. 2018, 52, PA4168. [Google Scholar] [CrossRef]
- Zheng, X.; Yuan, H.; Gu, C.; Yang, C.; Xie, F.; Zhang, X.; Xu, B.; Sun, J. Transbronchial lung parenchyma cryoablation with a novel flexible cryoprobe in an in vivo porcine model. Diagn. Interv. Imaging 2022, 103, 49–57. [Google Scholar] [CrossRef]
- Ye, K.; Chen, Z.; Xu, Y. The double-edged functions of necroptosis. Cell Death Dis. 2023, 14, 163. [Google Scholar] [CrossRef]
- Bertheloot, D.; Latz, E.; Franklin, B.S. Necroptosis, pyroptosis and apoptosis: An intricate game of cell death. Cell Mol. Immunol. 2021, 18, 1106–1121. [Google Scholar] [CrossRef] [PubMed]
- Chen, J.; Kos, R.; Garssen, J.; Redegeld, F. Molecular Insights into the Mechanism of Necroptosis: The Necrosome As a Potential Therapeutic Target. Cells 2019, 8, 1486. [Google Scholar] [CrossRef] [PubMed]
- Li, L.; Tong, A.; Zhang, Q.; Wei, Y.; Wei, X. The molecular mechanisms of MLKL-dependent and MLKL-independent necrosis. J. Mol. Cell Biol. 2021, 13, 3–14. [Google Scholar] [CrossRef] [PubMed]
- Newton, K.; Strasser, A.; Kayagaki, N.; Dixit, V.M. Cell death. Cell 2024, 187, 235–256. [Google Scholar] [CrossRef] [PubMed]
- Jing, L.; Song, F.; Liu, Z.; Li, J.; Wu, B.; Fu, Z.; Jiang, J.; Chen, Z. MLKL-PITPalpha signaling-mediated necroptosis contributes to cisplatin-triggered cell death in lung cancer A549 cells. Cancer Lett. 2018, 414, 136–146. [Google Scholar] [CrossRef] [PubMed]
- Wei, X.; Xie, F.; Zhou, X.; Wu, Y.; Yan, H.; Liu, T.; Huang, J.; Wang, F.; Zhou, F.; Zhang, L. Role of pyroptosis in inflammation and cancer. Cell Mol. Immunol. 2022, 19, 971–992. [Google Scholar] [CrossRef] [PubMed]
- Korpan, N.N.; Goltsev, A.N.; Dronov, O.I.; Bondarovych, M.O. Cryoimmunology: Opportunities and challenges in biomedical science and practice. Cryobiology 2021, 100, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Cerqueira, M.A.; Ferrari, K.L.; de Mattos, A.C.; Monti, C.R.; Reis, L.O. T cells CD4+/CD8+ local immune modulation by prostate cancer hemi-cryoablation. World J. Urol. 2020, 38, 673–680. [Google Scholar] [CrossRef] [PubMed]
- Aarts, B.M.; Klompenhouwer, E.G.; Rice, S.L.; Imani, F.; Baetens, T.; Bex, A.; Horenblas, S.; Kok, M.; Haanen, J.; Beets-Tan, R.G.H.; et al. Cryoablation and immunotherapy: An overview of evidence on its synergy. Insights Imaging 2019, 10, 53. [Google Scholar] [CrossRef]
- Tian, Y.; Qi, X.; Jiang, X.; Shang, L.; Xu, K.; Shao, H. Cryoablation and immune synergistic effect for lung cancer: A review. Front. Immunol. 2022, 13, 950921. [Google Scholar] [CrossRef]
- Katzman, D.; Wu, S.; Sterman, D.H. Immunological Aspects of Cryoablation of Non-Small Cell Lung Cancer: A Comprehensive Review. J. Thorac. Oncol. 2018, 13, 624–635. [Google Scholar] [CrossRef] [PubMed]
- Velez, A.; DeMaio, A.; Sterman, D. Cryoablation and immunity in non-small cell lung cancer: A new era of cryo-immunotherapy. Front. Immunol. 2023, 14, 1203539. [Google Scholar] [CrossRef] [PubMed]
- Gravett, A.M.; Dalgleish, A.G.; Copier, J. In vitro culture with gemcitabine augments death receptor and NKG2D ligand expression on tumour cells. Sci. Rep. 2019, 9, 1544. [Google Scholar] [CrossRef] [PubMed]
- Chern, Y.J.; Tai, I.T. Adaptive response of resistant cancer cells to chemotherapy. Cancer Biol. Med. 2020, 17, 842–863. [Google Scholar] [CrossRef] [PubMed]
- Morales-Valencia, J.; David, G. The origins of cancer cell dormancy. Curr. Opin. Genet. Dev. 2022, 74, 101914. [Google Scholar] [CrossRef] [PubMed]
- Hohenforst-Schmidt, W.; Zarogoulidis, P.; Darwiche, K.; Vogl, T.; Goldberg, E.P.; Huang, H.; Simoff, M.; Li, Q.; Browning, R.; Turner, F.J.; et al. Intratumoral chemotherapy for lung cancer: Re-challenge current targeted therapies. Drug Des. Devel Ther. 2013, 7, 571–583. [Google Scholar] [CrossRef] [PubMed]
- Meng, L.; Wei, Y.; Xiao, Y. Chemo-immunoablation of solid tumors: A new concept in tumor ablation. Front. Immunol. 2022, 13, 1057535. [Google Scholar] [CrossRef] [PubMed]
- Celikoglu, F.; Celikoglu, S.I.; Goldberg, E.P. Intratumoural chemotherapy of lung cancer for diagnosis and treatment of draining lymph node metastasis. J. Pharm. Pharmacol. 2010, 62, 287–295. [Google Scholar] [CrossRef] [PubMed]
- Plummer, R.; Dean, E.; Arkenau, H.T.; Redfern, C.; Spira, A.I.; Melear, J.M.; Chung, K.Y.; Ferrer-Playan, J.; Goddemeier, T.; Locatelli, G.; et al. A phase 1b study evaluating the safety and preliminary efficacy of berzosertib in combination with gemcitabine in patients with advanced non-small cell lung cancer. Lung Cancer 2022, 163, 19–26. [Google Scholar] [CrossRef]
- Hatami, E.; Nagesh, P.K.B.; Jaggi, M.; Chauhan, S.C.; Yallapu, M.M. Gambogic acid potentiates gemcitabine induced anticancer activity in non-small cell lung cancer. Eur. J. Pharmacol. 2020, 888, 173486. [Google Scholar] [CrossRef]
- Ye, W.; Huang, Q.; Tang, T.; Qin, G. Synergistic effects of piperlongumine and gemcitabine against KRAS mutant lung cancer. Tumori 2021, 107, 119–124. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Condition | % Live | % Apoptotic | % Necrotic |
|---|---|---|---|
| 37 °C Control | 89.7 (4.9) | 2.1 (1.6) | 7.9 (5.2) |
| 37 °C GEM 75nM | 71.8 (6.1) | 6.9 (5.4) | 19.9 (7.3) |
| Freeze (−15 °C) | 64.1 (6.6) | 4.0 (2.9) | 30.6 (8.4) |
| GEM Freeze | 27.7 (2.5) | 2.9 (1.0) | 67.7 (3.8) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Santucci, K.L.; Snyder, K.K.; Van Buskirk, R.G.; Baust, J.G.; Baust, J.M. Investigation of Lung Cancer Cell Response to Cryoablation and Adjunctive Gemcitabine-Based Cryo-Chemotherapy Using the A549 Cell Line. Biomedicines 2024, 12, 1239. https://doi.org/10.3390/biomedicines12061239
Santucci KL, Snyder KK, Van Buskirk RG, Baust JG, Baust JM. Investigation of Lung Cancer Cell Response to Cryoablation and Adjunctive Gemcitabine-Based Cryo-Chemotherapy Using the A549 Cell Line. Biomedicines. 2024; 12(6):1239. https://doi.org/10.3390/biomedicines12061239
Chicago/Turabian StyleSantucci, Kimberly L., Kristi K. Snyder, Robert G. Van Buskirk, John G. Baust, and John M. Baust. 2024. "Investigation of Lung Cancer Cell Response to Cryoablation and Adjunctive Gemcitabine-Based Cryo-Chemotherapy Using the A549 Cell Line" Biomedicines 12, no. 6: 1239. https://doi.org/10.3390/biomedicines12061239
APA StyleSantucci, K. L., Snyder, K. K., Van Buskirk, R. G., Baust, J. G., & Baust, J. M. (2024). Investigation of Lung Cancer Cell Response to Cryoablation and Adjunctive Gemcitabine-Based Cryo-Chemotherapy Using the A549 Cell Line. Biomedicines, 12(6), 1239. https://doi.org/10.3390/biomedicines12061239