



Enhanced Cognition and Modulation of Brain Connectivity in Mild Neurocognitive Disorder: The Promise of Transcranial Pulse Stimulation
 , , , , ,
, , , , ,
Abstract

1. Introduction
2. Materials and Methods
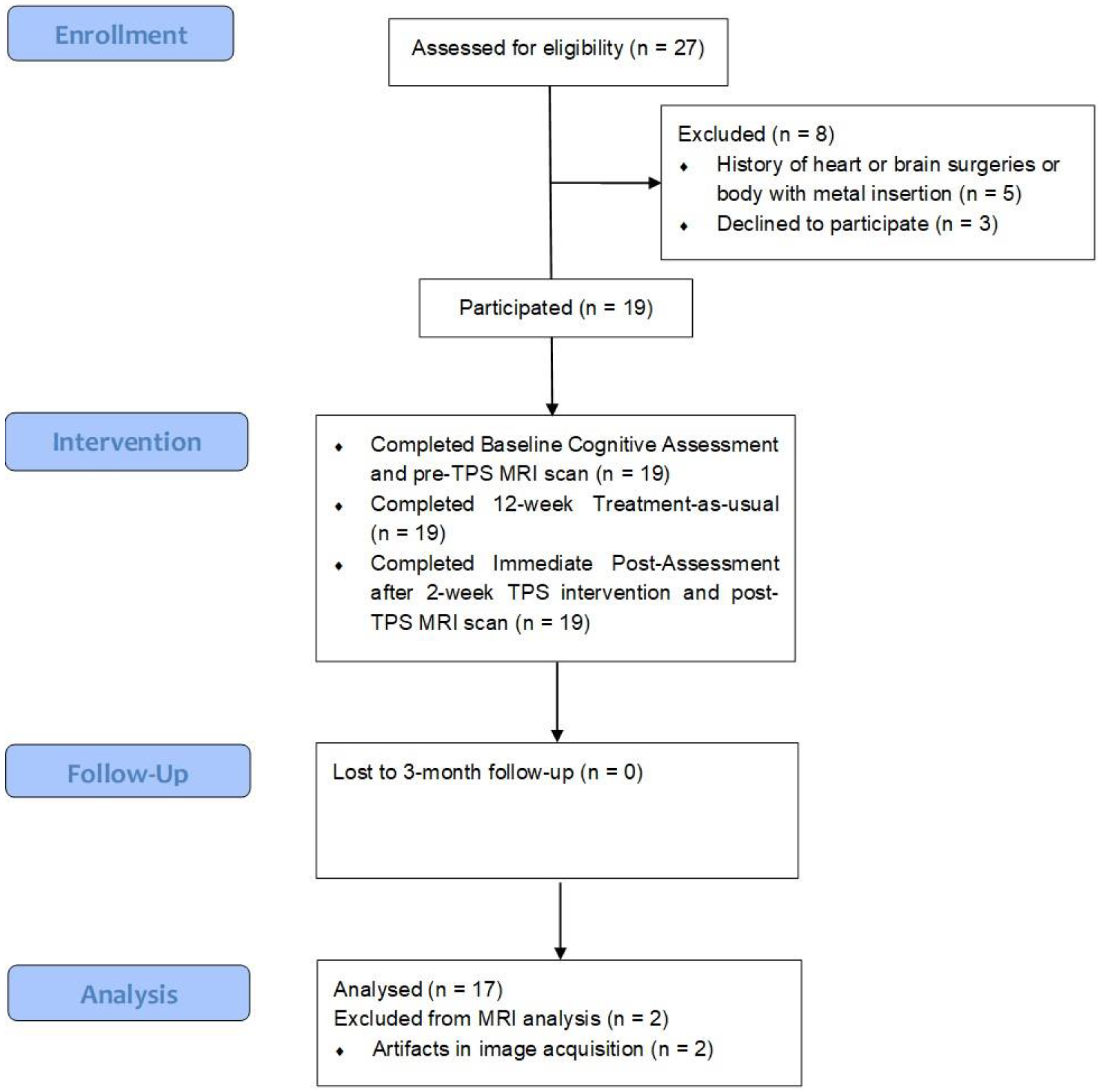
2.1. Participants
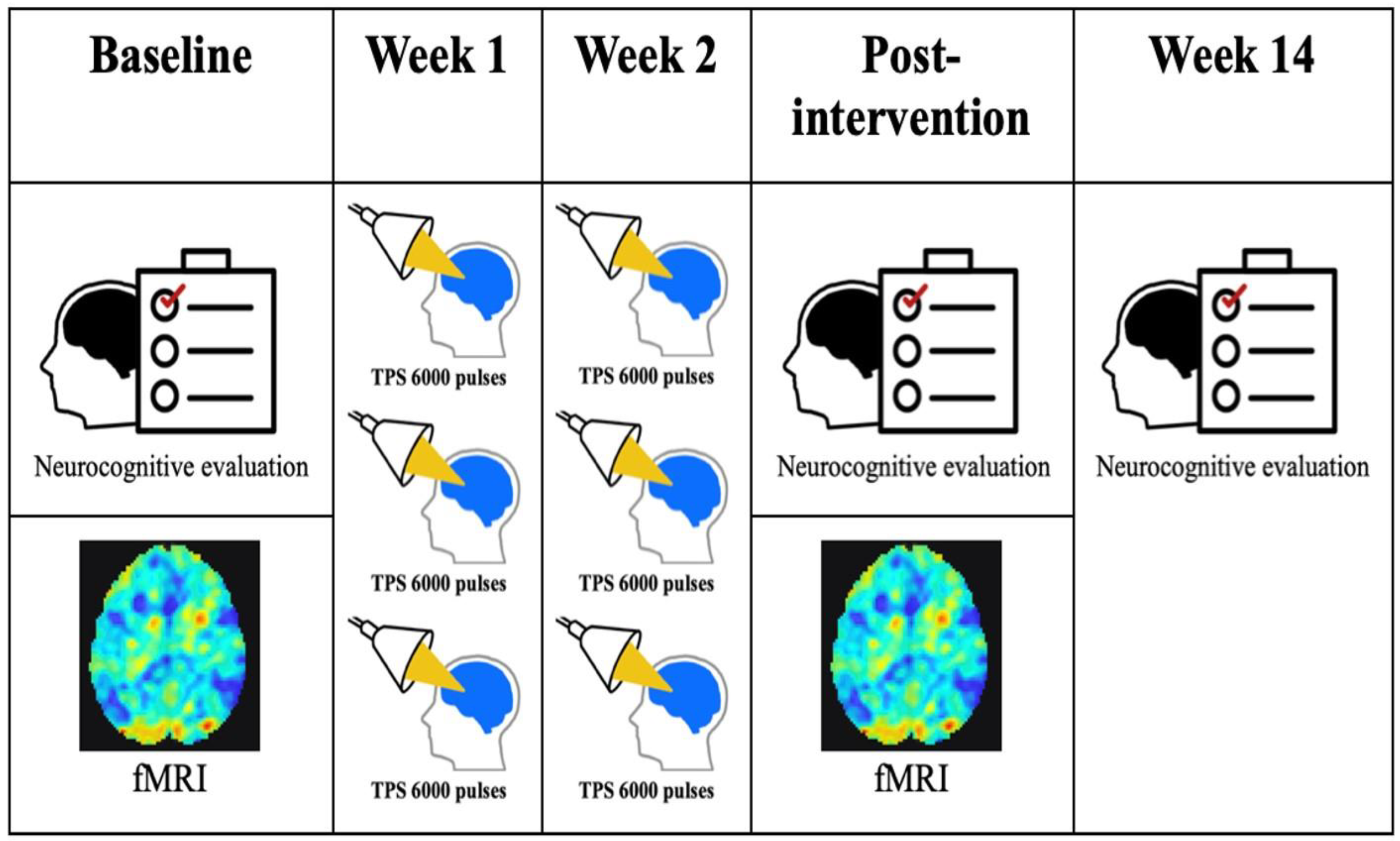
2.2. Study Design
2.3. TPS
2.4. Measures
2.5. Imaging Data Acquisition and Preprocessing
2.6. Functional Connectivity Analysis
2.7. Cortical Thickness Analysis
3. Results
3.1. Functional MRI Results
3.2. Cortical Thickness Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Nichols, E.; Steinmetz, J.D.; Vollset, S.E.; Abd-Allah, F.; Abdoli, A.; Abu-Gharbieh, E.; Alipour, V.; Almustanyir, S.; Amu, H.; Arabloo, J.; et al. Estimation of the global prevalence of dementia in 2019 and forecasted prevalence in 2050: An analysis for the Global Burden of Disease Study 2019. Lancet Public Health 2022, 7, e105–e125. [Google Scholar] [CrossRef] [PubMed]
- Sachs-Ericsson, N.; Blazer, D. The new DSM-5 diagnosis of mild neurocognitive disorder and its relation to research in mild cognitive impairment. Aging Ment. Health 2015, 19, 2–12. [Google Scholar] [CrossRef] [PubMed]
- Stokin, G.; Krell-Roesch, J.; Petersen, R.; Geda, Y. Mild Neurocognitive Disorder: An Old Wine in a New Bottle. Harv. Rev. Psychiatry 2015, 23, 368–376. [Google Scholar] [CrossRef] [PubMed]
- Sherman, S.; Schnyer, D. Major and Mild Neurocognitive Disorders. In Encyclopedia of Mental Health, 2nd ed.; Howard, S., Ed.; Academic Press: Cambridge, MA, USA, 2016; pp. 33–38. ISBN 9780123977533. [Google Scholar] [CrossRef]
- Luck, T.; Then, F.; Schroeter, M.; Witte, V.; Engel, C.; Loeffler, M.; Thiery, J.; Villringer, A.; Riedel-Heller, S. Prevalence of DSM-5 Mild Neurocognitive Disorder in Dementia-Free Older Adults: Results of the Population-Based LIFE-Adult-Study. Am. J. Geriatr. Psychiatry 2017, 25, 328–339. [Google Scholar] [CrossRef]
- Hategan, A.; Xiong, G. Major or Mild Neurocognitive Disorder Due to Alzheimer Disease. In Geriatric Psychiatry; Hategan, A., Bourgeois, J., Hirsch, C., Giroux, C., Eds.; Springer: New York, NY, USA, 2018; pp. 369–401. ISBN 978-3-319-67554-1. [Google Scholar] [CrossRef]
- Raschetti, R.; Albanese, E.; Vanacore, N.; Maggini, M. Cholinesterase inhibitors in mild cognitive impairment: A systematic review of randomised trials. PLoS Med. 2007, 4, e338. [Google Scholar] [CrossRef]
- Bernardo-Filho, M.; de Sá-Caputo, D.C. Editorial: Highlights in psychology of aging: Non-pharmacological interventions for people at risk of or living with dementia. Front. Psychol. 2024, 15, 1359171. [Google Scholar] [CrossRef]
- Beisteiner, R.; Matt, E.; Fan, C.; Baldysiak, H.; Schönfeld, M.; Philippi Novak, T.; Amini, A.; Aslan, T.; Reinecke, R.; Lehrner, J.; et al. Transcranial Pulse Stimulation with Ultrasound in Alzheimer’s Disease—A New Navigated Focal Brain Therapy. Adv. Sci. 2020, 7, 1902583. [Google Scholar] [CrossRef]
- Beisteiner, R.; Lozano, A. Treating the brain at the speed of sound. Brain Stimulat. 2020, 13, 1087–1088. [Google Scholar] [CrossRef]
- Minjoli, S.; Saturnino, G.B.; Blicher, J.U.; Stagg, C.J.; Siebner, H.R.; Antunes, A.; Thielscher, A. The impact of large structural brain changes in chronic stroke patients on the electric field caused by transcranial brain stimulation. NeuroImage Clin. 2017, 15, 106–117. [Google Scholar] [CrossRef]
- Spagnolo, P.A.; Wang, H.; Srivanitchapoom, P.; Schwandt, M.; Heilig, M.; Hallett, M. Lack of Target Engagement Following Low-Frequency Deep Transcranial Magnetic Stimulation of the Anterior Insula. Neuromodulation 2019, 22, 877–883. [Google Scholar] [CrossRef]
- Collins, M.N.; Legon, W.; Mesce, K.A. The Inhibitory Thermal Effects of Focused Ultrasound on an Identified, Single Motoneuron. eNeuro 2021, 8, ENEURO.0514-20.2021. [Google Scholar] [CrossRef] [PubMed]
- Darrow, D.P.; O’Brien, P.; Richner, T.J.; Netoff, T.I.; Ebbini, E.S. Reversible neuroinhibition by focused ultrasound is mediated by a thermal mechanism. Brain Stimulat. 2019, 12, 1439–1447. [Google Scholar] [CrossRef]
- Mueller, J.K.; Ai, L.; Bansal, P.; Legon, W. Numerical evaluation of the skull for human neuromodulation with transcranial focused ultrasound. J. Neural Eng. 2017, 14, 066012. [Google Scholar] [CrossRef] [PubMed]
- Matt, E.; Kaindl, L.; Tenk, S.; Egger, A.; Kolarova, T.; Karahasanović, N.; Amini, A.; Arslan, A.; Sariçiçek, K.; Weber, A.; et al. First evidence of long-term effects of transcranial pulse stimulation (TPS) on the human brain. J. Transl. Med. 2022, 20, 26. [Google Scholar] [CrossRef] [PubMed]
- Zhang, J.; Kang, N.; Yu, X.; Ma, Y.; Pang, X. Radial Extracorporeal Shock Wave Therapy Enhances the Proliferation and Differentiation of Neural Stem Cells by Notch, PI3K/AKT, and Wnt/β-catenin Signaling. Sci. Rep. 2017, 7, 15321. [Google Scholar] [CrossRef] [PubMed]
- d’Agostino, M.C.; Craig, K.; Tibalt, E.; Respizzi, S. Shock wave as biological therapeutic tool: From mechanical stimulation to recovery and healing, through mechanotransduction. Int. J. Surg. 2015, 24, 147–153. [Google Scholar] [CrossRef] [PubMed]
- Mariotto, S.; Cavalieri, E.; Amelio, E.; Ciampa, A.R.; de Prati, A.C.; Marlinghaus, E.; Russo, S.; Suzuki, H. Extracorporeal shock waves: From lithotripsy to anti-inflammatory action by NO production. Nitric Oxide 2005, 12, 89–96. [Google Scholar] [CrossRef] [PubMed]
- Lohse-Busch, H.; Reime, U.; Falland, R. Symptomatic treatment of unresponsive wakefulness syndrome with transcranially focused extracorporeal shock waves. Neurorehabilitation 2014, 35, 235–244. [Google Scholar] [CrossRef]
- Dörl, G.; Matt, E.; Beisteiner, R. Functional Specificity of TPS Brain Stimulation Effects in Patients with Alzheimer’s Disease: A Follow-up fMRI Analysis. Neurol. Ther. 2022, 11, 1391–1398. [Google Scholar] [CrossRef]
- Matt, E.; Dörl, G.; Beisteiner, R. Transcranial pulse stimulation (TPS) improves depression in AD patients on state-of-the-art treatment. Alzheimer’s Dement. Transl. Res. Clin. Interv. 2022, 8, e12245. [Google Scholar] [CrossRef]
- Satorres, E.; Torrella, J.; Real, E.; Pitarque, A.; Delhom, I.; Mélendez, J. Home-based transcranial direct current stimulation in mild neurocognitive disorder due to possible Alzheimer’s disease. A randomised, single-blind, controlled-placebo study. Front. Psychol. 2023, 13, 1071737. [Google Scholar] [CrossRef] [PubMed]
- Marra, H.; Myczkowski, M.; Memória, C.; Arnaut, D.; Ribeiro, P.; Mansur, C.; Alberto, R.; Bellini, B.; Silva, A.; Tortella, G.; et al. Transcranial Magnetic Stimulation to Address Mild Cognitive Impairment in the Elderly: A Randomized Controlled Study. Behav. Neurol. 2015, 2015, 287843. [Google Scholar] [CrossRef]
- Somaa, F.; Graaf, T.; Sack, A. Transcranial Magnetic Stimulation in the Treatment of Neurological Diseases. Front. Neurol. 2022, 13, 793253. [Google Scholar] [CrossRef]
- Cont, C.; Stute, N.; Galli, A.; Schulte, C.; Logmin, K.; Trenado, C.; Wojtecki, L. Retrospective real-world pilot data on transcranial pulse stimulation in mild to severe Alzheimer’s patients. Front. Neurol. 2022, 13, 948204. [Google Scholar] [CrossRef] [PubMed]
- Chen, X.; You, J.; Ma, H.; Zhou, M.; Huang, C. Transcranial pulse stimulation in Alzheimer’s disease. CNS Neurosci. Ther. 2023, 30, e14372. [Google Scholar] [CrossRef]
- Baggio, H.; Segura, B.; Sala-Llonch, R.; Marti, M.; Valldeoriola, F.; Compta, Y.; Tolosa, E.; Junqué, C. Cognitive impairment and resting-state network connectivity in Parkinson’s disease. Hum. Brain Mapp. 2015, 36, 199–212. [Google Scholar] [CrossRef]
- Ibrahim, B.; Suppiah, S.; Ibrahim, N.; Mohamad, M.; Hassan, H.; Nasser, N.; Saripan, M. Diagnostic power of resting-state fMRI for detection of network connectivity in Alzheimer’s disease and mild cognitive impairment: A systematic review. Hum. Brain Mapp. 2020, 42, 2941–2968. [Google Scholar] [CrossRef]
- Park, J.; Park, B.; Kim, S.; Kim, H.; Choi, C.; Jung, S.; Oh, J.; Lee, J.; Roh, J.; Shim, W. Improved Diagnostic Accuracy of Alzheimer’s Disease by Combining Regional Cortical Thickness and Default Mode Network Functional Connectivity: Validated in the Alzheimer’s Disease Neuroimaging Initiative Set. Korean J. Radiol. 2017, 18, 983–991. [Google Scholar] [CrossRef]
- Peterson, C.; Osborne, N.; Stingo, F.; Bourgeat, P.; Doecke, J.; Vannucci, M. Bayesian modeling of multiple structural connectivity networks during the progression of Alzheimer’s disease. Biometrics 2020, 76, 1120–1132. [Google Scholar] [CrossRef]
- So, K.I.; Leung, C.M.; Chung, D.; Liu, Z.; Fong, S. The Chinese bilingual SCID-I/P Project: Stage 1—Reliability for Mood Disorders and Schizophrenia. Hong Kong J. Psychiatry 2003, 13, 7–18. [Google Scholar]
- Linn, B.S.; Linn, M.W.; Gurel, L.E.E. Cumulative illness rating scale. J. Am. Geriatr. Soc. 1968, 16, 622–626. [Google Scholar] [CrossRef] [PubMed]
- Veale, J.F. Edinburgh handedness inventory–short form: A revised version based on confirmatory factor analysis. Laterality Asymmetries Body Brain Cogn. 2014, 19, 164–177. [Google Scholar] [CrossRef] [PubMed]
- Wong, A.; Xiong, Y.Y.; Kwan, P.W.L.; Chan, A.Y.Y.; Lam, W.W.M.; Wang, K.; Chu, W.C.W.; Nyenhuis, D.L.; Nasreddine, Z.; Wong, L.K.S.; et al. The validity, reliability and clinical utility of the Hong Kong Montreal Cognitive Assessment (HK-MoCA) in patients with cerebral small vessel disease. Dement. Geriatr. Cogn. Disord. 2009, 28, 81–87. [Google Scholar] [CrossRef] [PubMed]
- Yeung, P.Y.; Wong, L.L.; Chan, C.C.; Leung, J.L.; Yung, C.Y. A validation study of the Hong Kong version of Montreal Cognitive Assessment (HK-MoCA) in Chinese older adults in Hong Kong. Hong Kong Med. J. 2014, 20, 504–510. [Google Scholar] [CrossRef]
- Grégoire, J.; Van der Linden, M. Effect of age on forward and backward digit spans. Aging Neuropsychol. Cogn. 1997, 4, 140–149. [Google Scholar] [CrossRef]
- Bench, C.; Frith, C.D.; Grasby, P.M.; Friston, K.J.; Paulesu, E.; Frackowiak, R.S.J.; Dolan, R.J. Investigations of the functional anatomy of attention using the Stroop test. Neuropsychologia 1993, 31, 907–922. [Google Scholar] [CrossRef]
- Bowie, C.R.; Harvey, P.D. Administration and interpretation of the Trail Making Test. Nat. Protoc. 2006, 1, 2277–2281. [Google Scholar] [CrossRef]
- Graf, C. The Lawton instrumental activities of daily living scale. AJN Am. J. Nurs. 2008, 108, 52–62. [Google Scholar] [CrossRef]
- Williams, J.B. A structured interview guide for the Hamilton Depression Rating Scale. Arch. Gen. Psychiatry 1988, 45, 742–747. [Google Scholar] [CrossRef]
- Whitfield-Gabrieli, S.; Nieto-Castanon, A. Conn: A functional connectivity toolbox for correlated and anticorrelated brain networks. Brain Connect. 2012, 2, 125–141. [Google Scholar] [CrossRef]
- Mikl, M.; Mareček, R.; Hluštík, P.; Pavlicová, M.; Drastich, A.; Chlebus, P.; Brázdil, M.; Krupa, P. Effects of spatial smoothing on fMRI group inferences. Magn. Reson. Imaging 2008, 26, 490–503. [Google Scholar] [CrossRef] [PubMed]
- Behzadi, Y.; Restom, K.; Liau, J.; Liu, T.T. A component based noise correction method (CompCor) for BOLD and perfusion based fMRI. Neuroimage 2007, 37, 90–101. [Google Scholar] [CrossRef] [PubMed]
- Fair, D.A.; Cohen, A.L.; Power, J.D.; Dosenbach, N.U.F.; Church, J.A.; Miezin, F.M.; Schlaggar, B.L.; Petersen, S.E. Functional brain networks develop from a “local to distributed” organization. PLoS Comput. Biol. 2009, 5, e1000381. [Google Scholar] [CrossRef] [PubMed]
- Liston, C.; Chen, A.C.; Zebley, B.D.; Drysdale, A.T.; Gordon, R.; Leuchter, B.; Voss, H.U.; Casey, B.J.; Etkin, A.; Dubin, M.J. Default Mode Network Mechanisms of Transcranial Magnetic Stimulation in Depression. Biol. Psychiatry 2014, 76, 517–526. [Google Scholar] [CrossRef]
- Fischl, B.; Sereno, M.I.; Tootell, R.B.; Dale, A.M. High-resolution intersubject averaging and a coordinate system for the cortical surface. Hum. Brain Mapp. 1999, 8, 272–284. [Google Scholar] [CrossRef]
- Reuter, M.; Schmansky, N.J.; Rosas, H.D.; Fischl, B. Within-subject template estimation for unbiased longitudinal image analysis. Neuroimage 2012, 61, 1402–1418. [Google Scholar] [CrossRef]
- Reuter, M.; Fischl, B. Avoiding asymmetry-induced bias in longitudinal image processing. Neuroimage 2011, 57, 19–21. [Google Scholar] [CrossRef]
- Dale, A.M.; Fischl, B.; Sereno, M.I. Cortical Surface-Based Analysis: I. Segmentation and Surface Reconstruction. NeuroImage 1999, 9, 179–194. [Google Scholar] [CrossRef]
- Dale, A.M.; Sereno, M.I. Improved Localizadon of Cortical Activity by Combining EEG and MEG with MRI Cortical Surface Reconstruction: A Linear Approach. J. Cogn. Neurosci. 1993, 5, 162–176. [Google Scholar] [CrossRef]
- Desikan, R.S.; Ségonne, F.; Fischl, B.; Quinn, B.T.; Dickerson, B.C.; Blacker, D.; Buckner, R.L.; Dale, A.M.; Maguire, R.P.; Hyman, B.T.; et al. An automated labeling system for subdividing the human cerebral cortex on MRI scans into gyral based regions of interest. Neuroimage 2006, 31, 968–980. [Google Scholar] [CrossRef]
- Cheng, C.P.W.; Fong, T.K.H. TU-144. Efficacy and safety of transcranial pulse stimulation (TPS) in mild neurocognitive disorder—An open-label trial. Clin. Neurophysiol. 2022, 141, S18–S19. [Google Scholar] [CrossRef]
- Li, Y.; Luo, H.; Yu, Q.; Yin, L.; Li, K.; Li, Y.; Fu, J. Cerebral Functional Manipulation of Repetitive Transcranial Magnetic Stimulation in Cognitive Impairment Patients After Stroke: An fMRI Study. Front. Neurol. 2020, 11, 977. [Google Scholar] [CrossRef] [PubMed]
- Zhang, S.; Liu, L.; Zhang, L.; Ma, L.; Wu, H.; He, X.; Cao, M.; Li, R. Evaluating the treatment outcomes of repetitive transcranial magnetic stimulation in patients with moderate-to-severe Alzheimer’s disease. Front. Aging Neurosci. 2023, 14, 1070535. [Google Scholar] [CrossRef] [PubMed]
- Burgess, N.; Maguire, E.A.; O’Keefe, J. The Human Hippocampus and Spatial and Episodic Memory. Neuron 2002, 35, 625–641. [Google Scholar] [CrossRef]
- Grady, C.L.; McIntosh, A.R.; Craik, F.I.M. Age-related differences in the functional connectivity of the hippocampus during memory encoding. Hippocampus 2003, 13, 572–586. [Google Scholar] [CrossRef]
- Polanía, R.; Nitsche, M.A.; Ruff, C.C. Studying and modifying brain function with non-invasive brain stimulation. Nat. Neurosci. 2018, 21, 174–187. [Google Scholar] [CrossRef]
- Buckner, R.L.; Andrews-Hanna, J.R.; Schacter, D.L. The Brain’s Default Network: Anatomy, Function, and Relevance to Disease. Ann. N. Y. Acad. Sci. 2008, 1124, 1–38. [Google Scholar] [CrossRef]
- Boes, A.D.; Uitermarkt, B.D.; Albazron, F.M.; Lan, M.J.; Liston, C.; Pascual-Leone, A.; Dubin, M.J.; Fox, M.D. Rostral anterior cingulate cortex is a structural correlate of repetitive TMS treatment response in depression. Brain Stimulat. 2018, 11, 575–581. [Google Scholar] [CrossRef]
- Popescu, T.; Pernet, C.; Beisteiner, R. Transcranial ultrasound pulse stimulation reduces cortical atrophy in Alzheimer’s patients: A follow-up study. Alzheimer’s Dement. Transl. Res. Clin. Interv. 2021, 7, e12121. [Google Scholar] [CrossRef]
- Fox, M.D.; Buckner, R.L.; White, M.P.; Greicius, M.D.; Pascual-Leone, A. Efficacy of Transcranial Magnetic Stimulation Targets for Depression Is Related to Intrinsic Functional Connectivity with the Subgenual Cingulate. Biol. Psychiatry 2012, 72, 595–603. [Google Scholar] [CrossRef]
- Reinhart, R.; Nguyen, J. Working memory revived in older adults by synchronizing rhythmic brain circuits. Nat. Neurosci. 2019, 22, 820–827. [Google Scholar] [CrossRef] [PubMed]
- Summers, J.; Kang, N.; Cauraugh, J. Does transcranial direct current stimulation enhance cognitive and motor functions in the ageing brain? A systematic review and meta- analysis. Ageing Res. Rev. 2016, 25, 42–54. [Google Scholar] [CrossRef] [PubMed]
- Indahlastari, A.; Hardcastle, C.; Albizu, A.; Alvarez-Alvarado, S.; Boutzoukas, E.; Evangelista, N.; Hausman, H.; Kraft, J.; Langer, K.; Woods, A. A Systematic Review and Meta-Analysis of Transcranial Direct Current Stimulation to Remediate Age-Related Cognitive Decline in Healthy Older Adults. Neuropsychiatr. Dis. Treat. 2021, 17, 971–990. [Google Scholar] [CrossRef] [PubMed]
- Siegert, A.; Diedrich, L.; Antal, A. New Methods, Old Brains—A Systematic Review on the Effects of tDCS on the Cognition of Elderly People. Front. Hum. Neurosci. 2021, 15, 730134. [Google Scholar] [CrossRef]
- Hassanzahraee, M.; Zoghi, M.; Jaberzadeh, S. How different priming stimulations affect the corticospinal excitability induced by noninvasive brain stimulation techniques: A systematic review and meta-analysis. Rev. Neurosci. 2018, 29, 883–899. [Google Scholar] [CrossRef]
- Iyer, P.; Madhavan, S. Non-invasive brain stimulation in the modulation of cerebral blood flow after stroke: A systematic review of Transcranial Doppler studies. Clin. Neurophysiol. 2018, 129, 2544–2551. [Google Scholar] [CrossRef]
- Terranova, C.; Rizzo, V.; Cacciola, A.; Chillemi, G.; Calamuneri, A.; Milardi, D.; Quartarone, A. Is There a Future for Non-invasive Brain Stimulation as a Therapeutic Tool? Front. Neurol. 2019, 9, 1146. [Google Scholar] [CrossRef]
- Bergmann, T. Brain State-Dependent Brain Stimulation. Front. Psychol. 2018, 9, 2108. [Google Scholar] [CrossRef]
- Assenza, G.; Capone, F.; Biase, L.; Ferreri, F.; Florio, L.; Guerra, A.; Marano, M.; Paolucci, M.; Ranieri, F.; Salomone, G.; et al. Oscillatory Activities in Neurological Disorders of Elderly: Biomarkers to Target for Neuromodulation. Front. Aging Neurosci. 2017, 9, 189. [Google Scholar] [CrossRef]
- Sasaki, R.; Kojima, S.; Onishi, H. Do Brain-Derived Neurotrophic Factor Genetic Polymorphisms Modulate the Efficacy of Motor Cortex Plasticity Induced by Non-invasive Brain Stimulation? A Systematic Review. Front. Hum. Neurosci. 2021, 15, 742373. [Google Scholar] [CrossRef]
- Xia, M.; Wang, J.; He, Y. BrainNet Viewer: A network visualization tool for human brain connectomics. PLoS ONE 2013, 8, e68910. [Google Scholar] [CrossRef] [PubMed]
- Kühn, S.; Gallinat, J. Segregating cognitive functions within hippocampal formation: A quantitative meta-analysis on spatial navigation and episodic memory. Hum. Brain Mapp. 2014, 35, 1129–1142. [Google Scholar] [CrossRef] [PubMed]
- Murty, V.P.; Ritchey, M.; Adcock, R.A.; LaBar, K.S. fMRI studies of successful emotional memory encoding: A quantitative meta-analysis. Neuropsychologia 2010, 48, 3459–3469. [Google Scholar] [CrossRef] [PubMed]
- Mah, L.; Lanctôt, K.; Kumar, S.; Fischer, C. Novel neurostimulation approaches: Focus on neuropsychiatric symptoms. Am. J. Geriatr. Psychiatry 2021, 29, S10–S11. [Google Scholar] [CrossRef]
- Meng, Y.; Pople, C.B.; Lea-Banks, H.; Abrahao, A.; Davidson, B.; Suppiah, S.; Vecchio, L.M.; Samuel, N.; Mahmud, F.; Hynynen, K.; et al. Safety and efficacy of focused ultrasound induced blood-brain barrier opening, an integrative review of animal and human studies. J. Control Release 2019, 309, 25–36. [Google Scholar] [CrossRef]
- di Biase, L.; Falato, E.; Di Lazzaro, V. Transcranial Focused Ultrasound (tFUS) and Transcranial Unfocused Ultrasound (tUS) Neuromodulation: From Theoretical Principles to Stimulation Practices. Front. Neurol. 2019, 10, 549. [Google Scholar] [CrossRef]
- Wang, N.; Tytell, J.D.; Ingber, D.E. Mechanotransduction at a distance: Mechanically coupling the extracellular matrix with the nucleus. Nat. Rev. Mol. Cell Biol. 2009, 10, 75–82. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Overall (n = 17) | # χ2 | ||
|---|---|---|---|
| n | % | ||
| Gender | 0.49 | ||
| Male | 7 | 41.2 | |
| Female | 10 | 58.8 | |
| Age | 0.17 | ||
| 60–69 | 4 | 23.5 | |
| 70–79 | 9 | 53.0 | |
| 80 or above | 4 | 23.5 | |
| Marital status | 0.67 | ||
| Married | 9 | 52.9 | |
| Single/Separated/Widowed | 8 | 47.1 | |
| Education level | 0.56 | ||
| Elementary or below | 8 | 47.1 | |
| High School/College | 7 | 41.2 | |
| University or higher | 2 | 11.7 | |
| Family history of mental disorders | 0.16 | ||
| Yes | 4 | 23.5 | |
| No | 13 | 76.5 | |
| Brain Region | MNI Coordinates | Cluster Size | t-Value | ||
|---|---|---|---|---|---|
| x | y | z | |||
| Supramarginal gyrus (posterior right) | 58 | −50 | 50 | 85 | −5.58 |
| Supramarginal gyrus (posterior left) | −50 | −46 | 16 | 86 | −7.97 |
| Variable | B | 95% CI for B | p-Value |
|---|---|---|---|
| (constant) | −3.664 | ||
| HK-MoCA Total | 0.087 | 0.007, 0.167 | 0.038 * |
| VFT—60 s | 0.033 | −0.016, 0.083 | 0.146 |
| Stroop Interference | −0.001 | −0.016, 0.014 | 0.857 |
| Forward DS Span Length | 0.593 | −0.077, 1.263 | 0.072 |
| Forward DS Total | −0.253 | −0.564, 0.058 | 0.090 |
| Backward DS Span Length | 0.207 | −0.746, 1.159 | 0.601 |
| Backward DS Total | −0.129 | −0.653, 0.396 | 0.556 |
| HAM-D Total | 0.053 | −0.017, 0.123 | 0.110 |
| AES-C Total | 0.005 | −0.019, 0.029 | 0.592 |
| Chinese IADL Total | −0.009 | −0.072, 0.053 | 0.722 |
| Pre-Intervention | Post-Intervention | r | p-Value | |
|---|---|---|---|---|
| Mean (S.D.) | Mean (S.D.) | (FDR Adjusted) | ||
| HK-MoCA | 19.41 (4.784) | 20.76 (4.280) | −0.764 | 0.019 * |
| Right Precuneus | 2.080 (0.179) | 2.040 (0.176) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lo, H.K.-Y.; Fong, T.K.-H.; Cheung, T.; Ngan, S.-T.J.; Lui, W.-Y.V.; Chan, W.-C.; Wong, C.S.-M.; Wong, T.K.-T.; Cheng, C.P.-W. Enhanced Cognition and Modulation of Brain Connectivity in Mild Neurocognitive Disorder: The Promise of Transcranial Pulse Stimulation. Biomedicines 2024, 12, 2081. https://doi.org/10.3390/biomedicines12092081
Lo HK-Y, Fong TK-H, Cheung T, Ngan S-TJ, Lui W-YV, Chan W-C, Wong CS-M, Wong TK-T, Cheng CP-W. Enhanced Cognition and Modulation of Brain Connectivity in Mild Neurocognitive Disorder: The Promise of Transcranial Pulse Stimulation. Biomedicines. 2024; 12(9):2081. https://doi.org/10.3390/biomedicines12092081
Chicago/Turabian StyleLo, Heidi Ka-Ying, Tommy Kwan-Hin Fong, Teris Cheung, Sze-Ting Joanna Ngan, Wai-Yan Vivian Lui, Wai-Chi Chan, Corine Sau-Man Wong, Teenie Kwan-Tung Wong, and Calvin Pak-Wing Cheng. 2024. "Enhanced Cognition and Modulation of Brain Connectivity in Mild Neurocognitive Disorder: The Promise of Transcranial Pulse Stimulation" Biomedicines 12, no. 9: 2081. https://doi.org/10.3390/biomedicines12092081
APA StyleLo, H. K.-Y., Fong, T. K.-H., Cheung, T., Ngan, S.-T. J., Lui, W.-Y. V., Chan, W.-C., Wong, C. S.-M., Wong, T. K.-T., & Cheng, C. P.-W. (2024). Enhanced Cognition and Modulation of Brain Connectivity in Mild Neurocognitive Disorder: The Promise of Transcranial Pulse Stimulation. Biomedicines, 12(9), 2081. https://doi.org/10.3390/biomedicines12092081