
Biomarkers for Gastric Cancer Screening and Early Diagnosis

 , , and
, , and
Abstract
1. Introduction
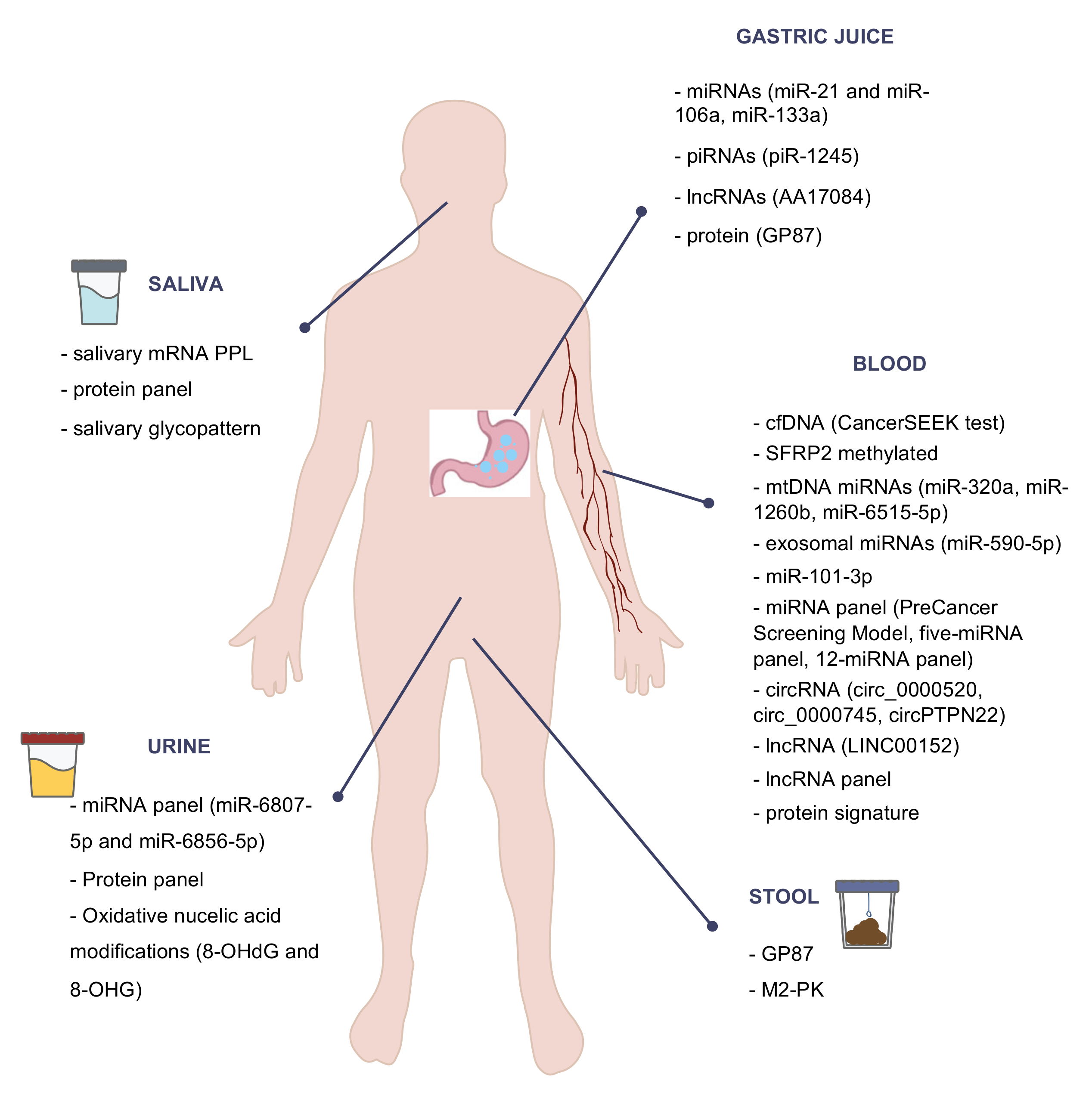
2. Blood Biomarkers
2.1. Circulating Free DNA
2.2. Noncoding RNA
2.2.1. miRNA
2.2.2. circRNA
2.2.3. lncRNA
2.3. Proteins
3. Saliva Biomarkers
4. Urine Biomarkers
5. Stool Biomarkers
6. Gastric Juice
6.1. DNA
6.2. Noncoding RNA
6.2.1. miRNA
6.2.2. Other Noncoding RNAs
6.3. Proteins
7. Conclusions
Author Contributions
Funding
Data Availability Statement
Conflicts of Interest
References
- Bray, F.; Ferlay, J.; Soerjomataram, I.; Siegel, R.L.; Torre, L.A.; Jemal, A. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J. Clin. 2018, 68, 394–424. [Google Scholar] [CrossRef]
- Vogelaar, I.; Van Der Post, R.S.; van Krieken, J.; Spruijt, L.; Van Zelst-Stams, W.A.; Kets, C.M.; Lubinski, J.; Jakubowska, A.; Teodorczyk, U.; Aalfs, C.M.; et al. Unraveling genetic predisposition to familial or early onset gastric cancer using germline whole-exome sequencing. Eur. J. Hum. Genet. 2017, 25, 1246–1252. [Google Scholar] [CrossRef]
- Isaeva, G.; Isaeva, R. Molecular methods for the detection of Helicobacter pylori. Minerva Biotecnol. 2021, 32, 182–187. [Google Scholar] [CrossRef]
- Van Cutsem, E.; Sagaert, X.; Topal, B.; Haustermans, K.; Prenen, H. Gastric cancer. Lancet 2016, 388, 2654–2664. [Google Scholar] [CrossRef]
- Asplund, J.; Kauppila, J.H.; Mattsson, F.; Lagergren, J. Survival Trends in Gastric Adenocarcinoma: A Population-Based Study in Sweden. Ann. Surg. Oncol. 2018, 25, 2693–2702. [Google Scholar] [CrossRef] [PubMed]
- Choi, K.S.; Jun, J.K.; Park, E.-C.; Park, S.; Jung, K.W.; Han, M.A.; Choi, I.J.; Lee, H.-Y. Performance of Different Gastric Cancer Screening Methods in Korea: A Population-Based Study. PLoS ONE 2012, 7, e50041. [Google Scholar] [CrossRef] [PubMed]
- Jun, J.K.; Choi, K.S.; Lee, H.-Y.; Suh, M.; Park, B.; Song, S.H.; Jung, K.W.; Lee, C.W.; Choi, I.J.; Park, E.-C.; et al. Effectiveness of the Korean National Cancer Screening Program in Reducing Gastric Cancer Mortality. Gastroenterology 2017, 152, 1319–1328.e7. [Google Scholar] [CrossRef] [PubMed]
- Khanderia, E.; Markar, S.R.; Acharya, A.; Kim, Y.; Kim, Y.-W.; Hanna, G.B. The Influence of Gastric Cancer Screening on the Stage at Diagnosis and Survival. J. Clin. Gastroenterol. 2016, 50, 190–197. [Google Scholar] [CrossRef] [PubMed]
- Cubiella, J.; Aisa, Á.P.; Cuatrecasas, M.; Redondo, P.D.; Esparrach, G.F.; Marín-Gabriel, J.C.; Moreira, L.; Núñez, H.; López, M.L.P.; de Santiago, E.R.; et al. Documento de posicionamiento de la AEG, la SEED y la SEAP sobre cribado de cáncer gástrico en poblaciones con baja incidencia. Gastroenterol. Hepatol. 2021, 44, 67–86. [Google Scholar] [CrossRef]
- Fernández-Esparrach, G.; Marín-Gabriel, J.C.; Redondo, P.D.; Núñez, H.; de Santiago, E.R.; Rosón, P.; Calvet, X.; Cuatrecasas, M.; Cubiella, J.; Moreira, L.; et al. Documento de posicionamiento de la AEG, la SEED y la SEAP sobre calidad de la endoscopia digestiva alta para la detección y vigilancia de las lesiones precursoras de cáncer gástrico. Gastroenterol. Hepatol. 2021, 44, 448–464. [Google Scholar] [CrossRef]
- Matsuoka, T.; Yashiro, M. Biomarkers of gastric cancer: Current topics and future perspective. World J. Gastroenterol. 2018, 24, 2818–2832. [Google Scholar] [CrossRef]
- Feng, F.; Tian, Y.; Xu, G.; Liu, Z.; Liu, S.; Zheng, G.; Guo, M.; Lian, X.; Fan, D.; Zhang, H. Diagnostic and prognostic value of CEA, CA19–9, AFP and CA125 for early gastric cancer. BMC Cancer 2017, 17, 1–6. [Google Scholar] [CrossRef]
- Biomarkers Definitions Working Group. Biomarkers and surrogate endpoints: Preferred definitions and conceptual framework. Clin. Pharmacol. Ther. 2001, 69, 89–95. [Google Scholar] [CrossRef]
- De Mattos-Arruda, L.; Olmos, D.; Tabernero, J. Prognostic and predictive roles for circulating biomarkers in gastrointestinal cancer. Futur. Oncol. 2011, 7, 1385–1397. [Google Scholar] [CrossRef]
- Qian, C.; Ju, S.; Qi, J.; Zhao, J.; Shen, X.; Jing, R.; Yu, J.; Li, L.; Shi, Y.; Zhang, L.; et al. Alu-based cell-free DNA: A novel biomarker for screening of gastric cancer. Oncotarget 2017, 8, 54037–54045. [Google Scholar] [CrossRef]
- Kim, K.; Shin, D.G.; Park, M.K.; Baik, S.H.; Kim, T.H.; Kim, S.; Lee, S. Circulating cell-free DNA as a promising biomarker in patients with gastric cancer: Diagnostic validity and significant reduction of cfDNA after surgical resection. Ann. Surg. Treat. Res. 2014, 86, 136–142. [Google Scholar] [CrossRef]
- Huang, Z.-B.; Zhang, H.-T.; Yu, B.; Yu, D.-H. Cell-free DNA as a liquid biopsy for early detection of gastric cancer (Review). Oncol. Lett. 2020, 21, 1. [Google Scholar] [CrossRef] [PubMed]
- Cohen, J.D.; Li, L.; Wang, Y.; Thoburn, C.; Afsari, B.; Danilova, L.; Douville, C.; Javed, A.A.; Wong, F.; Mattox, A.; et al. Detection and localization of surgically resectable cancers with a multi-analyte blood test. Science 2018, 359, 926–930. [Google Scholar] [CrossRef] [PubMed]
- Padmanabhan, N.; Ushijima, T.; Tan, N.P.P. How to stomach an epigenetic insult: The gastric cancer epigenome. Nat. Rev. Gastroenterol. Hepatol. 2017, 14, 467–478. [Google Scholar] [CrossRef] [PubMed]
- Hideura, E.; Suehiro, Y.; Nishikawa, J.; Shuto, T.; Fujimura, H.; Ito, S.; Goto, A.; Hamabe, K.; Saeki, I.; Okamoto, T.; et al. Blood Free-Circulating DNA Testing of Methylated RUNX3 Is Useful for Diagnosing Early Gastric Cancer. Cancers 2020, 12, 789. [Google Scholar] [CrossRef]
- Miao, J.; Liu, Y.; Zhao, G.; Liu, X.; Ma, Y.; Li, H.; Li, S.; Zhu, Y.; Xiong, S.; Zheng, M.; et al. Feasibility of Plasma-Methylated SFRP2 for Early Detection of Gastric Cancer. Cancer Control 2020, 27, 27. [Google Scholar] [CrossRef]
- Alarcón, M.A.; Olivares, W.; Córdova-Delgado, M.; Muñoz-Medel, M.; De Mayo, T.; Carrasco-Aviño, G.; Wichmann, I.; Landeros, N.; Amigo, J.; Norero, E.; et al. The Reprimo-Like Gene Is an Epigenetic-Mediated Tumor Suppressor and a Candidate Biomarker for the Non-Invasive Detection of Gastric Cancer. Int. J. Mol. Sci. 2020, 21, 9472. [Google Scholar] [CrossRef]
- Liu, L.; Yang, X. Implication of Reprimo and hMLH1 gene methylation in early diagnosis of gastric carcinoma. Int. J. Clin. Exp. Pathol. 2015, 8, 14977–14982. [Google Scholar]
- Fernandes, J.; Michel, V.; Camorlinga-Ponce, M.; Gomez, A.; Maldonado, C.; DE Reuse, H.; Torres, J.; Touati, E. Circulating Mitochondrial DNA Level, a Noninvasive Biomarker for the Early Detection of Gastric Cancer. Cancer Epidemiol. Biomark. Prev. 2014, 23, 2430–2438. [Google Scholar] [CrossRef]
- Ueda, T.; Volinia, S.; Okumura, H.; Shimizu, M.; Taccioli, C.; Rossi, S.; Alder, H.; Liu, C.-G.; Oue, N.; Yasui, W.; et al. Relation between microRNA expression and progression and prognosis of gastric cancer: A microRNA expression analysis. Lancet Oncol. 2010, 11, 136–146. [Google Scholar] [CrossRef]
- Yao, Y.; Ding, Y.; Bai, Y.; Zhou, Q.; Lee, H.; Li, X.; Teng, L. Identification of Serum Circulating MicroRNAs as Novel Diagnostic Biomarkers of Gastric Cancer. Front. Genet. 2021, 11, 591515. [Google Scholar] [CrossRef] [PubMed]
- Huang, T.; Song, C.; Zheng, L.; Xia, L.; Li, Y.; Zhou, Y. The roles of extracellular vesicles in gastric cancer development, microenvironment, anti-cancer drug resistance, and therapy. Mol. Cancer 2019, 18, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Koga, Y.; Yasunaga, M.; Moriya, Y.; Akasu, T.; Fujita, S.; Yamamoto, S.; Matsumura, Y. Exosome Can Prevent RNase from Degrading MicroRNA in Feces. J. Gastrointest. Oncol. 2011, 2, 215–222. [Google Scholar] [PubMed]
- Zheng, G.-D.; Xu, Z.-Y.; Hu, C.; Lv, H.; Xie, H.-X.; Huang, T.; Zhang, Y.-Q.; Chen, G.-P.; Fu, Y.-F.; Cheng, X.-D. Exosomal miR-590-5p in Serum as a Biomarker for the Diagnosis and Prognosis of Gastric Cancer. Front. Mol. Biosci. 2021, 8, 1–10. [Google Scholar] [CrossRef]
- Shi, Y.; Wang, Z.; Zhu, X.; Chen, L.; Ma, Y.; Wang, J.; Yang, X.; Liu, Z. Exosomal miR-1246 in serum as a potential biomarker for early diagnosis of gastric cancer. Int. J. Clin. Oncol. 2019, 25, 89–99. [Google Scholar] [CrossRef] [PubMed]
- Hung, P.-S.; Chen, C.-Y.; Chen, W.-T.; Kuo, C.-Y.; Fang, W.-L.; Huang, K.-H.; Chiu, P.-C.; Lo, S.-S. miR-376c promotes carcinogenesis and serves as a plasma marker for gastric carcinoma. PLoS ONE 2017, 12, e0177346. [Google Scholar] [CrossRef]
- Wu, J.; Li, G.; Wang, Z.; Yao, Y.; Chen, R.; Pu, X.; Wang, J. Circulating MicroRNA-21 Is a Potential Diagnostic Biomarker in Gastric Cancer. Dis. Mark. 2015, 2015, 1–8. [Google Scholar] [CrossRef]
- Zeng, W.; Zhang, S.; Yang, L.; Wei, W.; Gao, J.; Guo, N.; Wu, F. Serum miR-101-3p combined with pepsinogen contributes to the early diagnosis of gastric cancer. BMC Med. Genet. 2020, 21, 1–7. [Google Scholar] [CrossRef]
- Cheng, J.; Yang, A.; Cheng, S.; Feng, L.; Wu, X.; Lu, X.; Zu, M.; Cui, J.; Yu, H.; Zou, L. Circulating miR-19a-3p and miR-483-5p as Novel Diagnostic Biomarkers for the Early Diagnosis of Gastric Cancer. Med. Sci. Monit. 2020, 26, e923444. [Google Scholar] [CrossRef]
- Zhu, C.; Ren, C.; Han, J.; Ding, Y.; Du, J.; Dai, N.; Dai, J.; Ma, H.; Hu, Z.; Shen, H.; et al. A five-microRNA panel in plasma was identified as potential biomarker for early detection of gastric cancer. Br. J. Cancer 2014, 110, 2291–2299. [Google Scholar] [CrossRef]
- So, J.B.Y.; Kapoor, R.; Zhu, F.; Koh, C.; Zhou, L.; Zou, R.; Tang, Y.C.; Goo, P.C.K.; Rha, S.Y.; Chung, H.C.; et al. Development and validation of a serum microRNA biomarker panel for detecting gastric cancer in a high-risk population. Gut 2021, 70, 829–837. [Google Scholar] [CrossRef]
- Sun, H.; Tang, W.; Rong, D.; Jin, H.; Fu, K.; Zhang, W.; Liu, Z.; Cao, H.; Cao, X. Hsa_circ_0000520, a potential new circular RNA biomarker, is involved in gastric carcinoma. Cancer Biomark. 2018, 21, 299–306. [Google Scholar] [CrossRef]
- Shao, Y.; Tao, X.; Lu, R.; Zhang, H.; Ge, J.; Xiao, B.; Ye, G.; Guo, J. Hsa_circ_0065149 is an Indicator for Early Gastric Cancer Screening and Prognosis Prediction. Pathol. Oncol. Res. 2020, 26, 1475–1482. [Google Scholar] [CrossRef]
- Huang, M.; He, Y.-R.; Liang, L.-C.; Huang, Q.; Zhu, Z.-Q. Circular RNA hsa_circ_0000745 may serve as a diagnostic marker for gastric cancer. World J. Gastroenterol. 2017, 23, 6330–6338. [Google Scholar] [CrossRef]
- Ma, S.; Kong, S.; Gu, X.; Xu, Y.; Tao, M.; Shen, L.; Shen, X.; Ju, S. As a biomarker for gastric cancer, circPTPN22 regulates the progression of gastric cancer through the EMT pathway. Cancer Cell Int. 2021, 21, 1–14. [Google Scholar] [CrossRef]
- Dong, L.; Qi, P.; Xu, M.-D.; Ni, S.-J.; Huang, D.; Xu, Q.-H.; Weng, W.-W.; Tan, C.; Sheng, W.-Q.; Zhou, X.-Y.; et al. Circulating CUDR, LSINCT-5 and PTENP1 long noncoding RNAs in sera distinguish patients with gastric cancer from healthy controls. Int. J. Cancer 2015, 137, 1128–1135. [Google Scholar] [CrossRef]
- Zhang, K.; Shi, H.; Xi, H.; Wu, X.; Cui, J.; Gao, Y.; Liang, W.; Hu, C.; Liu, Y.; Li, J.; et al. Genome-Wide lncRNA Microarray Profiling Identifies Novel Circulating lncRNAs for Detection of Gastric Cancer. Theranostics 2017, 7, 213–227. [Google Scholar] [CrossRef]
- Lijun, Q.; Shao, Y.; Zhang, X.; Zheng, T.; Miao, M.; Qin, L.; Wang, B.; Ye, G.; Xiao, B.; Guo, J. Plasma long noncoding RNA protected by exosomes as a potential stable biomarker for gastric cancer. Tumor Biol. 2015, 36, 2007–2012. [Google Scholar] [CrossRef]
- Lin, L.-Y.; Yang, L.; Zeng, Q.; Wang, L.; Chen, M.-L.; Zhao, Z.-H.; Ye, G.-D.; Luo, Q.-C.; Lv, P.-Y.; Guo, Q.-W.; et al. Tumor-originated exosomal lncUEGC1 as a circulating biomarker for early-stage gastric cancer. Mol. Cancer 2018, 17, 84. [Google Scholar] [CrossRef]
- Zhao, R.; Zhang, Y.; Zhang, X.; Yang, Y.; Zheng, X.; Li, X.; Liu, Y.; Zhang, Y. Exosomal long noncoding RNA HOTTIP as potential novel diagnostic and prognostic biomarker test for gastric cancer. Mol. Cancer 2018, 17, 68. [Google Scholar] [CrossRef]
- Qin, J.; Yang, Q.; Ye, H.; Wang, K.; Zhang, M.; Zhu, J.; Wang, X.; Dai, L.; Wang, P.; Zhang, J. Using Serological Proteome Analysis to Identify and Evaluate Anti-GRP78 Autoantibody as Biomarker in the Detection of Gastric Cancer. J. Oncol. 2020, 2020, 1–10. [Google Scholar] [CrossRef]
- Song, Y.; Wang, J.; Sun, J.; Chen, X.; Shi, J.; Wu, Z.; Yu, D.; Zhang, F.; Wang, Z. Screening of Potential Biomarkers for Gastric Cancer with Diagnostic Value Using Label-free Global Proteome Analysis. Genom. Proteom. Bioinform. 2020, 18, 679–695. [Google Scholar] [CrossRef]
- Suo, J.; Zhang, D.Y.; Tong, W.; Ye, F.; He, L.; Cui, L.; Cui, M.; Hu, Y.; Li, W.; Jiang, J. Serum biomarker panels for diagnosis of gastric cancer. OncoTargets Ther. 2016, 9, 2455–2463. [Google Scholar] [CrossRef]
- Liu, S.; Cui, M.; Zang, J.; Wang, J.; Shi, X.; Qian, F.; Xu, S.; Jing, R. SLC6A3 as a potential circulating biomarker for gastric cancer detection and progression monitoring. Pathol. Res. Pract. 2021, 221, 153446. [Google Scholar] [CrossRef]
- Zhou, B.; Zhou, Z.; Chen, Y.; Deng, H.; Cai, Y.; Rao, X.; Yin, Y.; Rong, L. Plasma proteomics-based identification of novel biomarkers in early gastric cancer. Clin. Biochem. 2020, 76, 5–10. [Google Scholar] [CrossRef]
- Loong, T.H.; Soon, N.C.; Mahmud, N.R.K.N.; Naidu, J.; Rani, R.A.; Hamid, N.A.; Elias, M.H.; Rose, I.M.; Tamil, A.M.; Mokhtar, N.M.; et al. Serum pepsinogen and gastrin-17 as potential biomarkers for pre-malignant lesions in the gastric corpus. Biomed. Rep. 2017, 7, 460–468. [Google Scholar] [CrossRef]
- McNicholl, A.G.; Forné, M.; Barrio, J.; De la Coba, C.; González, B.; Rivera, R.; Esteve, M.; Fernández-Bañares, F.; Madrigal, B.; Gras-Miralles, B.; et al. Accuracy of GastroPanel for the diagnosis of atrophic gastritis. Eur. J. Gastroenterol. Hepatol. 2014, 26, 941–948. [Google Scholar] [CrossRef]
- Aikou, S.; Ohmoto, Y.; Gunji, T.; Matsuhashi, N.; Ohtsu, H.; Miura, H.; Kubota, K.; Yamagata, Y.; Seto, Y.; Nakajima, A.; et al. Tests for Serum Levels of Trefoil Factor Family Proteins Can Improve Gastric Cancer Screening. Gastroenterology 2011, 141, 837–845.e7. [Google Scholar] [CrossRef]
- Choi, B.; Lee, H.-J.; Min, J.; Choe, H.-N.; Choi, Y.-S.; Son, Y.-G.; Ahn, H.-S.; Suh, Y.-S.; Goldenring, J.R.; Yang, H.-K. Plasma expression of the intestinal metaplasia markers CDH17 and TFF3 in patients with gastric cancer. Cancer Biomark. 2017, 19, 231–239. [Google Scholar] [CrossRef]
- Huang, Z.; Zhang, X.; Lu, H.; Wu, L.; Wang, D.; Zhang, Q.; Ding, H. Serum trefoil factor 3 is a promising non-invasive biomarker for gastric cancer screening: A monocentric cohort study in China. BMC Gastroenterol. 2014, 14, 74. [Google Scholar] [CrossRef]
- Altun, E.; Yildiz, A.; Cevik, C.; Turan, G. The role of high sensitive C-reactive protein and histopathological evaluation in chronic gastritis patients with or without Helicobacter pylori infection. Acta Cir. Bras. 2019, 34, e201900310. [Google Scholar] [CrossRef]
- Chung, H.W.; Kim, J.W.; Lee, J.-H.; Song, S.Y.; Chung, J.B.; Kwon, O.H.; Lim, J.-B. Comparison of the Validity of Three Biomarkers for Gastric Cancer Screening. J. Clin. Gastroenterol. 2009, 43, 19–26. [Google Scholar] [CrossRef]
- He, X.-X.; Yang, J.; Ding, Y.-W.; Liu, W.; Shen, Q.-Y.; Xia, H.H.-X. Increased epithelial and serum expression of macrophage migration inhibitory factor (MIF) in gastric cancer: Potential role of MIF in gastric carcinogenesis. Gut 2006, 55, 797–802. [Google Scholar] [CrossRef]
- Pan, K.-F.; Formichella, L.; Zhang, L.; Zhang, Y.; Ma, J.-L.; Li, Z.-X.; Liu, C.; Wang, Y.-M.; Goettner, G.; Ulm, K.; et al. Helicobacter pyloriantibody responses and evolution of precancerous gastric lesions in a Chinese population. Int. J. Cancer 2014, 134, 2118–2125. [Google Scholar] [CrossRef]
- Yamamoto, H.; Watanabe, Y.; Sato, Y.; Maehata, T.; Itoh, F. Non-Invasive Early Molecular Detection of Gastric Cancers. Cancers 2020, 12, 2880. [Google Scholar] [CrossRef]
- Kahroba, H.; Hejazi, M.S.; Samadi, N. Exosomes: From carcinogenesis and metastasis to diagnosis and treatment of gastric cancer. Cell. Mol. Life Sci. 2019, 76, 1747–1758. [Google Scholar] [CrossRef]
- Valadi, H.; Ekström, K.; Bossios, A.; Sjöstrand, M.; Lee, J.J.; Lötvall, J.O. Exosome-mediated transfer of mRNAs and microRNAs is a novel mechanism of genetic exchange between cells. Nat. Cell Biol. 2007, 9, 654–659. [Google Scholar] [CrossRef]
- Skog, J.; Würdinger, T.; Van Rijn, S.; Meijer, D.H.; Gainche, L.; Curry, W.T., Jr.; Carter, B.S.; Krichevsky, A.M.; Breakefield, X.O. Glioblastoma microvesicles transport RNA and proteins that promote tumour growth and provide diagnostic biomarkers. Nature 2008, 10, 1470–1476. [Google Scholar] [CrossRef]
- Pegtel, D.M.; Cosmopoulos, K.; Thorley-Lawson, D.A.; van Eijndhoven, M.A.J.; Hopmans, E.S.; Lindenberg, J.L.; de Gruijl, T.D.; Würdinger, T.; Middeldorp, J.M. Functional delivery of viral miRNAs via exosomes. Proc. Natl. Acad. Sci. USA 2010, 107, 6328–6333. [Google Scholar] [CrossRef]
- Cheng, L.; Sharples, R.A.; Scicluna, B.J.; Hill, A.F. Exosomes provide a protective and enriched source of miRNA for biomarker profiling compared to intracellular and cell-free blood. J. Extracell. Vesicles 2014, 3, 23743. [Google Scholar] [CrossRef]
- Zhang, Y.; Bi, J.; Huang, J.; Tang, Y.; Du, S.; Li, P. Exosome: A Review of Its Classification, Isolation Techniques, Storage, Diagnostic and Targeted Therapy Applications. Int. J. Nanomed. 2020, 15, 6917–6934. [Google Scholar] [CrossRef]
- Xiao, Y.; Zhong, J.; Zhong, B.; Huang, J.; Jiang, L.; Jiang, Y.; Yuan, J.; Sun, J.; Dai, L.; Yang, C.; et al. Exosomes as potential sources of biomarkers in colorectal cancer. Cancer Lett. 2020, 476, 13–22. [Google Scholar] [CrossRef]
- Zhou, B.; Xu, K.; Zheng, X.; Chen, T.; Wang, J.; Song, Y.; Shao, Y.; Zheng, S. Application of exosomes as liquid biopsy in clinical diagnosis. Signal. Transduct. Target. Ther. 2020, 5, 1–14. [Google Scholar] [CrossRef]
- Li, F.; Yoshizawa, J.M.; Kim, K.-M.; Kanjanapangka, J.; Grogan, T.R.; Wang, X.; Elashoff, D.E.; Ishikawa, S.; Chia, D.; Liao, W.; et al. Discovery and Validation of Salivary Extracellular RNA Biomarkers for Noninvasive Detection of Gastric Cancer. Clin. Chem. 2018, 64, 1513–1521. [Google Scholar] [CrossRef]
- Xu, F.; Jiang, M. Evaluation of predictive role of carcinoembryonic antigen and salivary mRNA biomarkers in gastric cancer detection. Medicine 2020, 99, e20419. [Google Scholar] [CrossRef]
- Xiao, H.; Zhang, Y.; Kim, Y.; Kim, S.; Kim, J.J.; Kim, K.M.; Yoshizawa, J.; Fan, L.-Y.; Cao, C.; Wong, D.T.W. Differential Proteomic Analysis of Human Saliva using Tandem Mass Tags Quantification for Gastric Cancer Detection. Sci. Rep. 2016, 6, 22165. [Google Scholar] [CrossRef] [PubMed]
- Shu, J.; Yu, H.; Li, X.; Zhang, D.; Liu, X.; Du, H.; Zhang, J.; Yang, Z.; Xie, H.; Li, Z. Salivary glycopatterns as potential biomarkers for diagnosis of gastric cancer. Oncotarget 2017, 8, 35718–35727. [Google Scholar] [CrossRef]
- Yoshizawa, J.M.; Schafer, C.A.; Schafer, J.J.; Farrell, J.J.; Paster, B.J.; Wong, D.T.W. Salivary Biomarkers: Toward Future Clinical and Diagnostic Utilities. Clin. Microbiol. Rev. 2013, 26, 781–791. [Google Scholar] [CrossRef] [PubMed]
- Spielmann, N.; Wong, D.T. Saliva: Diagnostics and therapeutic perspectives. Oral Dis. 2010, 17, 345–354. [Google Scholar] [CrossRef] [PubMed]
- Ai, J.; Smith, B.; Wong, D.T. Saliva Ontology: An ontology-based framework for a Salivaomics Knowledge Base. BMC Bioinform. 2010, 11, 302. [Google Scholar] [CrossRef] [PubMed]
- Bonne, N.J.; Wong, D.T. Salivary biomarker development using genomic, proteomic and metabolomic approaches. Genome Med. 2012, 4, 82. [Google Scholar] [CrossRef]
- Rapado-González, Ó.; Martínez-Reglero, C.; Salgado-Barreira, A.; Takkouche, B.; López-López, R.; Suárez-Cunqueiro, M.M.; Muinelo-Romay, L. Salivary biomarkers for cancer diagnosis: A meta-analysis. Ann. Med. 2020, 52, 131–144. [Google Scholar] [CrossRef]
- Iwasaki, H.; Shimura, T.; Yamada, T.; Okuda, Y.; Natsume, M.; Kitagawa, M.; Horike, S.-I.; Kataoka, H. A novel urinary microRNA biomarker panel for detecting gastric cancer. J. Gastroenterol. 2019, 54, 1061–1069. [Google Scholar] [CrossRef]
- Shimura, T.; Dagher, A.; Sachdev, M.; Ebi, M.; Yamada, T.; Yamada, T.; Joh, T.; Moses, M.A. Urinary ADAM12 and MMP-9/NGAL Complex Detect the Presence of Gastric Cancer. Cancer Prev. Res. 2015, 8, 240–248. [Google Scholar] [CrossRef]
- Shimura, T.; Dayde, D.; Wang, H.; Okuda, Y.; Iwasaki, H.; Ebi, M.; Kitagawa, M.; Yamada, T.; Yamada, T.; Hanash, S.M.; et al. Novel urinary protein biomarker panel for early diagnosis of gastric cancer. Br. J. Cancer 2020, 123, 1656–1664. [Google Scholar] [CrossRef]
- Chen, Q.; Hu, Y.; Fang, Z.; Ye, M.; Li, J.; Zhang, S.; Yuan, Y.; Guo, C. Elevated Levels of Oxidative Nucleic Acid Modification Markers in Urine from Gastric Cancer Patients: Quantitative Analysis by Ultra Performance Liquid Chromatography-Tandem Mass Spectrometry. Front. Chem. 2020, 8, 606495. [Google Scholar] [CrossRef]
- Shirasu, M.; Touhara, K. The scent of disease: Volatile organic compounds of the human body related to disease and disorder. J. Biochem. 2011, 150, 257–266. [Google Scholar] [CrossRef]
- Marimuthu, A.; O’Meally, R.N.; Chaerkady, R.; Subbannayya, Y.; Nanjappa, V.; Kumar, P.; Kelkar, D.S.; Pinto, S.M.; Sharma, R.; Renuse, S.; et al. A Comprehensive Map of the Human Urinary Proteome. J. Proteome Res. 2011, 10, 2734–2743. [Google Scholar] [CrossRef]
- Bax, C.; Taverna, G.; Eusebio, L.; Sironi, S.; Grizzi, F.; Guazzoni, G.; Capelli, L. Innovative Diagnostic Methods for Early Prostate Cancer Detection through Urine Analysis: A Review. Cancers 2018, 10, 123. [Google Scholar] [CrossRef] [PubMed]
- Bax, C.; Lotesoriere, B.J.; Sironi, S.; Capelli, L. Bax Review and Comparison of Cancer Biomarker Trends in Urine as a Basis for New Diagnostic Pathways. Cancers 2019, 11, 1244. [Google Scholar] [CrossRef] [PubMed]
- Oshi, M.; Murthy, V.; Takahashi, H.; Huyser, M.; Okano, M.; Tokumaru, Y.; Rashid, O.; Matsuyama, R.; Endo, I.; Takabe, K. Urine as a Source of Liquid Biopsy for Cancer. Cancers 2021, 13, 2652. [Google Scholar] [CrossRef] [PubMed]
- Qiao, S.-X.; Yuan, M.; Liu, Y.-L.; Lin, X.-S.; Zhang, X.-P.; Tobi, M. Detection of gastric cancer and premalignant lesions by novel marker glycoprotein 87 using monoclonal antibody Adnab-9. Cancer Epidemiol. Biomark. Prev. 2003, 12, 1095–1099. [Google Scholar]
- Zhang, B.; Chen, J.-Y.; Chen, D.-D.; Wang, G.-B.; Shen, P. Tumor type M2pyruvate kinase expression in gastric cancer, colorectal cancer and controls. World J. Gastroenterol. 2004, 10, 1643–1646. [Google Scholar] [CrossRef]
- Shimura, T. Novel Biomarkers of Gastrointestinal Cancer. Cancers 2021, 13, 1501. [Google Scholar] [CrossRef]
- Liu, S.; Dai, J.; Lan, X.; Fan, B.; Dong, T.; Zhang, Y.; Han, M. Intestinal bacteria are potential biomarkers and therapeutic targets for gastric cancer. Microb. Pathog. 2021, 151, 104747. [Google Scholar] [CrossRef]
- Wu, J.; Zhang, C.; Xu, S.; Xiang, C.; Wang, R.; Yang, D.; Lu, B.; Shi, L.; Tong, R.; Teng, Y.; et al. Fecal Microbiome Alteration May Be a Potential Marker for Gastric Cancer. Dis. Mark. 2020, 2020, 1–17. [Google Scholar] [CrossRef]
- Kon, O.L.; Yip, T.-T.; Ho, M.F.; Chan, W.H.; Wong, W.K.; Tan, S.Y.; Ng, W.H.; Kam, S.Y.; Eng, A.K.; Ho, P.; et al. The distinctive gastric fluid proteome in gastric cancer reveals a multi-biomarker diagnostic profile. BMC Med. Genom. 2008, 1, 54. [Google Scholar] [CrossRef]
- Virgilio, E.; Giarnieri, E.; Giovagnoli, M.R.; Montagnini, M.; Proietti, A.; D’Urso, R.; Mercantini, P.; Balducci, G.; Cavallini, M. Gastric Juice MicroRNAs as Potential Biomarkers for Screening Gastric Cancer: A Systematic Review. Anticancer. Res. 2018, 38, 613–616. [Google Scholar] [CrossRef]
- Huang, L.; Xu, A. Detection of digestive malignancies and post-gastrectomy complications via gastrointestinal fluid examination. Front. Med. 2017, 11, 20–31. [Google Scholar] [CrossRef] [PubMed]
- Yim, S.; Gultepe, E.; Gracias, D.H.; Sitti, M. Biopsy using a Magnetic Capsule Endoscope Carrying, Releasing, and Retrieving Untethered Microgrippers. IEEE Trans. Biomed. Eng. 2014, 61, 513–521. [Google Scholar] [CrossRef]
- Zhao, A.-J.; Qian, Y.-Y.; Sun, H.; Hou, X.; Pan, J.; Liu, X.; Zhou, W.; Chen, Y.-Z.; Jiang, X.; Li, Z.-S.; et al. Screening for gastric cancer with magnetically controlled capsule gastroscopy in asymptomatic individuals. Gastrointest. Endosc. 2018, 88, 466–474.e1. [Google Scholar] [CrossRef] [PubMed]
- Muretto, P.; Graziano, F.; Staccioli, M.P.; Barbanti, I.; Bartolucci, A.; Paolini, G.; Giordano, D.; Testa, E.; De Gaetano, A. An endogastric capsule for measuring tumor markers ingastric juice: An evaluation of the safety and efficacy of a new diagnostic tool. Ann. Oncol. 2003, 14, 105–109. [Google Scholar] [CrossRef] [PubMed]
- Muretto, P.; Ruzzo, A.; Pizzagalli, F.; Graziano, F.; Maltese, P.E.; Zingaretti, C.; Berselli, E.; Donnarumma, N.; Magnani, M. Endogastric capsule for E-cadherin gene (CDH1) promoter hypermethylation assessment in DNA from gastric juice of diffuse gastric cancer patients. Ann. Oncol. 2008, 19, 516–519. [Google Scholar] [CrossRef]
- Yamamoto, H.; Watanabe, Y.; Oikawa, R.; Morita, R.; Yoshida, Y.; Maehata, T.; Yasuda, H.; Itoh, F. BARHL2 Methylation Using Gastric Wash DNA or Gastric Juice Exosomal DNA is a Useful Marker for Early Detection of Gastric Cancer in an H. pylori-Independent Manner. Clin. Transl. Gastroenterol. 2016, 7, e184. [Google Scholar] [CrossRef]
- Yu, X.; Luo, L.; Wu, Y.; Yu, X.; Liu, Y.; Yu, X.; Zhao, X.; Zhang, X.; Cui, L.; Ye, G.; et al. Gastric juice miR-129 as a potential biomarker for screening gastric cancer. Med. Oncol. 2013, 30, 365. [Google Scholar] [CrossRef]
- Zhang, X.; Cui, L.; Ye, G.; Zheng, T.; Song, H.; Xia, T.; Yu, X.; Xiao, B.; Le, Y.; Guo, J. Gastric juice microRNA-421 is a new biomarker for screening gastric cancer. Tumor Biol. 2012, 33, 2349–2355. [Google Scholar] [CrossRef] [PubMed]
- Cui, L.; Zhang, X.; Ye, G.; Zheng, T.; Song, H.; Deng, H.; Xiao, B.; Xia, T.; Yu, X.; Le, Y.; et al. Gastric juice MicroRNAs as potential biomarkers for the screening of gastric cancer. Cancer 2013, 119, 1618–1626. [Google Scholar] [CrossRef] [PubMed]
- Shao, J.; Fang, P.-H.; He, B.; Guo, L.-L.; Shi, M.-Y.; Zhu, Y.; Bo, P.; Zhen-Wen, Z.-W. Downregulated MicroRNA-133a in Gastric Juice as a Clinicopathological Biomarker for Gastric Cancer Screening. Asian Pac. J. Cancer Prev. 2016, 17, 2719–2722. [Google Scholar]
- Shao, Y.; Li, J.; Lu, R.; Li, T.; Yang, Y.; Xiao, B.; Guo, J. Global circular RNA expression profile of human gastric cancer and its clinical significance. Cancer Med. 2017, 6, 1173–1180. [Google Scholar] [CrossRef]
- Zhou, X.; Liu, J.; Meng, A.; Zhang, L.; Wang, M.; Fan, H.; Peng, W.; Lu, J. Gastric juice piR-1245: A promising prognostic biomarker for gastric cancer. J. Clin. Lab. Anal. 2020, 34, e23131. [Google Scholar] [CrossRef]
- Shao, Y.; Ye, M.; Bs, X.J.; Sun, W.; Ding, X.; Liu, Z.; Ye, G.; Zhang, X.; Xiao, B.; Guo, J. Gastric juice long noncoding RNA used as a tumor marker for screening gastric cancer. Cancer 2014, 120, 3320–3328. [Google Scholar] [CrossRef]
- Shao, Y.; Ye, M.; Li, Q.; Sun, W.; Ye, G.; Zhang, X.; Yang, Y.; Xiao, B.; Guo, J. LncRNA-RMRP promotes carcinogenesis by acting as a miR-206 sponge and is used as a novel biomarker for gastric cancer. Oncotarget 2016, 7, 37812–37824. [Google Scholar] [CrossRef]
- Yang, Y.; Shao, Y.; Zhu, M.; Li, Q.; Yang, F.; Lu, X.; Xu, C.; Xiao, B.; Sun, Y.; Guo, J. Using gastric juice lncRNA-ABHD11-AS1 as a novel type of biomarker in the screening of gastric cancer. Tumor Biol. 2015, 37, 1183–1188. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Sample | Type | Biomarker | Patients | AUC (95% CI) | Sensitivity (%) | Specificity (%) | Ref. |
|---|---|---|---|---|---|---|---|
| Blood Biomarkers | |||||||
| Blood (serum) | DNA | Circulating free DNA | 216 patients (92 healthy patients and 124 primary gastric cancer patients) | 0.94 (0.91–0.97) | 78.96 | 91.81 | [15] |
| Blood (plasma) | DNA | Circulating free DNA | 132 patients (34 healthy patients, 34 GC patients, and 64 benign gastric patients) | 0.99 | 96.67 | 94.11 | [16] |
| Blood (plasma) | DNA + protein | Mutations in circulating free DNA (16 genes + 8 proteins) | 1817 patients (812 healthy patients, 68 GC patients, 209 breast cancer patients, 388 colorectal cancer patients, 45 esophagus cancer patients, 44 liver cancer patients, 104 lung cancer patients, 54 ovary cancer patients, and 93 pancreatic cancer) | 0.91 (0.90–0.92) | 70.00 for GC | 99.00 | [18] |
| Blood (plasma) | DNA | Methylated RUNX3 | 111 patients (61 healthy patients and 50 GC patients) | 0.69 | 50.00 | 80.30 | [20] |
| Blood (plasma) | DNA | Methylated SFRP2 | 236 patients (50 healthy patients, 92 GC patients, 16 intestinal metaplasia patients, 26 gastric fundic gland polyp patients, 13 small adenoma patients, and 39 hyperplastic polyp patients) | 0.78 (0.71–0.86) | 60.90 | 86.0 | [21] |
| Blood (plasma) | DNA | Methylated RPRML | 50 patients (25 healthy patients and 25 GC patients) | 0.73 (0.58–0.87) | 56.00 | 88.00 | [22] |
| Blood | DNA | mtDNA | 276 patients (48 healthy patients, 74 patients with non-atrophic gastritis, 31 patients with intestinal metaplasia, and 123 GC patients) | - | 47.00 | 80.00 | [24] |
| Blood (plasma) | miRNA | hsa-miR-320a | 3408 patients (3174 healthy patients and 234 GC patients) | 0.96–1.00 | 99.10–100.00 | 88.8–100.00 | [26] |
| Blood (plasma) | miRNA | hsa-miR-1260b | 3408 patients (3174 healthy patients and 234 GC patients) | 0.97–1.00 | 97.40–98.00 | 89.60–100.00 | [26] |
| Blood (plasma) | miRNA | hsa-miR-6515-5p | 3408 patients (3174 healthy patients and 234 GC patients) | 0.95–0.99 | 92.20–98.00 | 88.70–92.70 | [26] |
| Blood (serum) | miRNA | Exosomal miR-590-5p | 218 patients (50 healthy patients and 168 GC patients) | 0.81 | 63.70 | 86.00 | [29] |
| Blood (plasma) | miRNA | Exosomal miR-1246 | 165 patients (50 healthy patients, 30 patients with benign gastric disease, and 85 GC patients) | 0.91 (0.86–0.96) | 82.30 | 86.00 | [30] |
| Blood (serum) | miRNA | miR-101-3p | 197 patients (50 healthy patients, 86 GC patients and 61 atrophic gastritis patients) | 0.88 | 72.09 | 86.49 | [33] |
| Blood (plasma) | miRNA | miR-376c | 173 patients (108 healthy patients and 65 GC patients) | 0.77 | 71.00 | 78.00 | [31] |
| Blood (plasma) | miRNA | miR-21 | 100 patients (50 healthy patients and 50 GC patients) | 0.91 (0.87–0.97) | 88.40 | 79.60 | [32] |
| Blood (plasma) | miRNA panel | Pre-Cancer Screening Model (age, miR-19a-3p and miR-483-5p) | 180 patients (70 gastritis subjects, 20 low-grade intraepithelial neoplasia, 34 high-grade intraepithelial neoplasia, and 56 early GC) | Early GC and prec. lesions: 0.84 (0.77–0.90) | Early GC and prec. lesions: 87.70 | Early GC and prec. lesions: 62.80 | [34] |
| Blood (plasma) | miRNA panel | miR-16, miR-25, miR-92a, miR-451 and miR-486-5p | 320 patients (160 healthy patients, 124 non cardia GC patients, and 36 cardia GC patients) | Non-cardia GC: 0.81 | Non-cardia GC: 72.90 | Non-cardia GC: 89.20 | [35] |
| Blood (serum) | miRNA panel | 12 miRNA panel | 5248 patients (4803 healthy patients and 445 GC) | 0.85 (0.81–0.88) | 87.00 | 68.40 | [36] |
| Blood (serum) | miRNA panel + other factors | miRNA panel + age + H. pylori serology + pepsinogen I/II ratio | 5248 patients (4803 healthy patients and 445 GC) | 0.88 | 87.00 | 69.40 | [36] |
| Blood (plasma) | circRNA | hsa_circ_0000520 | 62 patients (17 healthy patients and 45 GC) | 0.90 | 82.35 | 84.44 | [37] |
| Blood (plasma) | circRNA | Exosomal circ_0065149 | 80 patients (41 healthy patients and 39 early GC) | 0.64 | 48.70 | 90.20 | [38] |
| Blood (plasma) | circRNA | circ_0000745 | 120 patients (60 healthy patients and 60 GC patients) | 0.68 | 85.50 | 45.00 | [39] |
| Blood (plasma) | circRNA | circ_0000745 + CEA | 120 patients (60 healthy patients and 60 GC patients) | 0.78 | 80.00 | 63.30 | [39] |
| Blood (plasma) | circRNA | circPTPN22 | 294 patients (104 healthy patients, 120 plasma of GC patients, and 70 gastritis patients) | 0.857 (0.808–0.907) | 78.00 | 84.00 | [40] |
| Blood (plasma) | circRNA + antigens | circPTPN22 + CEA + CA199 | 294 patients (104 healthy patients, 120 plasma of GC patients, and 70 gastritis patients) | 0.89 | 83.00 | 87.00 | [40] |
| Blood (serum) | lncRNA | multi-lncRNA diagnostic panel (CUDR, LSINCT-5 and PTENP1) | 231 patients (124 healthy patients, 110 GC patients, 9 early-stage GC, 21 later-stage GC, and 15 gastric peptic ulcer patients without GC) | GC:0.83 Early-GC: 0.83 Later-GC: 0.83 | GC: 81.80 Early-GC: 77.80 Later-GC: 85.70 | GC: 85.20 Early-stage: 97.00 Later-stage: 84.80 | [41] |
| Blood (plasma) | lncRNA | TINCR, CCAT2, AOC4P, BANCR and LINC00857 | 321 patients (110 healthy patients, 162 GC patients, 28 prec. Patients, and 21 GIST) | GC: 0.90 (0.86–0.95) Prec: 0.82 (0.71–0.92) GIST: 0.80 (0.68–0.91 | GC: 0.81 (0.71–0.89) Prec: 0.68 (0.50–0.82) GIST: 0.68 (0.50–0.82) | GC: 0.86 (0.77–0.93) Prec: 0.89 (0.72–0.98) GIST: 0.86 (0.64–0.97) | [42] |
| Blood (plasma) | lncRNA | Exosomal LINC00152 | 191 patients (81 healthy patients, 79 GC patients, and 31 gastric epithelial dysplasia patients) | 0.66 (0.57–0.74) | 48.10 | 85.20 | [43] |
| Blood (plasma) | lncRNA | Exosomal lncUEGC1 | 144 patients (65 healthy patients, 18 CAG, and 61 stage I/II GC patients) | 0.88 | - | - | [44] |
| Blood (serum) | lncRNA | Exosomal lncRNA HOTTIP | 246 patients (120 healthy patients and 126 GC patients) | 0.83 | 69.80 | 85.00 | [45] |
| Blood (serum) | lncRNA | Exosomal lncRNA HOTTIP + CEA + CA19-19 + CA72-4 | 246 patients (120 healthy patients and 126 GC patients) | 0.87 | - | - | [45] |
| Blood (plasma) | Protein | Protein signature (ATP5B-ATP5O-NDUFB4-NDUFB8) | 71 patients (34 healthy patients and 37 GC patients) | 0.79 | - | - | [47] |
| Blood (serum) | Protein panel | Protein signature (VEGF, ADAM8, IgG to H. pylori status, serum pepsinogen I, and pepsinogen II) | 523 patients (238 healthy patients and 285 GC patients) | 0.85 (0.77–0.93) | 88.60 | 83.20 | [48] |
| Blood (serum) | Protein | SLC6A3 | 220 patients (56 healthy patients, 113 GC patients, and 51 patients with polyps) | 0.72 (0.64–0.80) | 55.75 | 78.57 | [49] |
| Blood (serum) | Protein panel | SLC6A3, CEA and CA19-9 | 220 patients (56 healthy patients, 113 GC patients, and 51 patients with polyps) | 0.82 (0.75–0.88) | 84.07 | 58.93 | [49] |
| Blood (serum) | Protein | anti-GRP78 autoantibody | 866 patients (433 healthy patients and 433 GC patients) | 0.67 | 35.30 | - | [46] |
| Blood (plasma) | Protein | Q8NBP7 | 30 patients (15 healthy controls and 15 early GC) | 0.702 | 60.0 | 80.0 | [50] |
| Blood (plasma) | Protein | P00441 | 30 patients (15 healthy controls and 15 early GC) | 0.707 | 93.3 | 46.7 | [50] |
| Blood (plasma) | Protein | Q86UD1 | 30 patients (15 healthy controls and 15 early GC) | 0.711 | 46.7 | 100 | [50] |
| Blood (plasma) | Protein | A0A2R8Y7X9 | 30 patients (15 healthy controls and 15 early GC) | 0.796 | 80.0 | 86.7 | [50] |
| Blood (plasma) | Protein | P62979 | 30 patients (15 healthy controls and 15 early GC) | 0.724 | 86.7 | 66.7 | [50] |
| Blood (plasma) | Protein | A0A0G2JMC9 | 30 patients (15 healthy controls and 15 early GC) | 0.747 | 60.0 | 93.3 | [50] |
| Blood (plasma) | Protein | P08493 | 30 patients (15 healthy controls and 15 early GC) | 0.813 | 73.3 | 80.0 | [50] |
| Blood (plasma) | Protein | P16157 | 30 patients (15 healthy controls and 15 early GC) | 0.653 | 46.7 | 86.7 | [50] |
| Blood (plasma) | Protein | A0A087WTY6 | 30 patients (15 healthy controls and 15 early GC) | 0.64 | 80.0 | 53.3 | [50] |
| Blood (plasma) | Protein | P14207 | 30 patients (15 healthy controls and 15 early GC) | 0.689 | 60.0 | 80.0 | [50] |
| Blood (plasma) | Protein | Q9H939 | 30 patients (15 healthy controls and 15 early GC) | 0.573 | 73.3 | 53.3 | [50] |
| Blood (plasma) | Protein panel | 11 protein panel | 30 patients (15 healthy controls and 15 early GC) | 0.711 | 66.7 | 86.7 | [50] |
| Blood (serum) | Protein | PGI | 72 patients (35 healthy controls, 34 CAG and 3 GC) | 0.659 | 66.7 | 85.3 | [51] |
| Blood (serum) | Protein | PGI:II ratio | 72 patients (35 healthy controls, 34 CAG and 3 GC) | 0.902 | 83.3 | 77.9 | [51] |
| Blood (serum) | Protein | TFF3 | 567 patients (325 healthy controls and 242 GC patients) | 0.890 | 80.9 | 81.0 | [53] |
| Blood (plasma) | Protein | TFF3 | 86 patients (44 healthy controls and 42 stage I GC patients) | 0.703 | 83.3 | 54.5 | [54] |
| Blood (serum) | Protein | Hs-CRP + PGI:II ratio | 378 patients (69 healthy controls, 47 CAG, 75 IM, 41 early GC, 43, AGC, and 87 metastasis GC) | - | AGC: 67.0 IM: 67.0 | AGC: 85.0 IM: 72.0 | [57] |
| Blood (serum) | Protein | Hs-CRP | 378 patients (69 healthy controls, 47 CAG, 75 IM, 41 early GC, 43, AGC, and 87 metastasis GC) | - | AGC: 67.0 | AGC: 85.0 | [57] |
| Sample | Type | Biomarker | Patients | AUC (95% CI) | Sensitivity (%) | Specificity (%) | Ref. |
|---|---|---|---|---|---|---|---|
| Saliva Biomarkers | |||||||
| Saliva | miRNA + mRNA | 3 mRNAs (SPINK7, PPL, and SEMA4B) and 2 miRNAs (MIR140-5p and MIR301a) + demographic | 294 patients (131 healthy patients and 163 GC patients) | 0.87 (0.80–0.93) | 82.00 | 77.00 | [69] |
| Saliva + blood | Protein + mRNA | CEA + mRNA PPL | 400 patients (200 healthy patients and 200 GC patients) | - | 92.00 | 87.00 | [70] |
| Saliva | Protein | CSTB + TPI1 + DMBT1 | 80 patients (40 healthy patients and 40 GC patients) | 0.93 | 85.00 | 80.00 | [71] |
| Saliva | Protein glycosylation | Salivary glycopattern (for GC VVA and SBA) (for atrophic gastritis DSA and LEL) | 201 patients (60 healthy patients, 87 GC patients, and 54 atrophic gastritis patients) | GC: 0.89 Atrophic gastritis: 0.83 | GC: 0.96 Atrophic gastritis: 0.92 | GC:0.80 Atrophic gastritis: 0.72 | [72] |
| Sample | Type | Biomarker | Patients | AUC (95% CI) | Sensitivity (%) | Specificity (%) | Ref. |
|---|---|---|---|---|---|---|---|
| Urine Biomarkers | |||||||
| Urine | miRNA | miR-376c | 173 patients (108 healthy patients and 65 GC patients) | 0.70 | 60.00 | 64.00 | [31] |
| Urine | miRNA panel | miR-6807-5p/miR-6856-5p/H. pylori status | 550 patients (302 healthy patients and 248 GC patients) | GC: 0.89 (0.82–0.95) Stage I GC: 0.75 (0.68–0.81) | GC: 76.90 Stage I GC: - | GC: 88.90 Stage I GC: - | [78] |
| Urine | Protein | MMP-9/NGAL complex and ADAM12 | 70 patients (35 healthy patients and GC patients) | 0.83 (0.72–0.93) | - | - | [79] |
| Urine | Protein panel | uTFF1/uADAM12/H. pylori status for males; uTFF1/uBARD1/H. pylori status for females | 282 patients (138 healthy patients 144 GC patients) | Male: 0.86 (0.81–0.91) Female: 0.89 (0.80–0.99) | - | - | [80] |
| Urine | DNA | 8-OHdG | 130 patients (70 healthy patients and 60 GC patients) | 0.78 (0.70–0.86) | - | - | [81] |
| Urine | DNA | 8-OHG | 130 patients (70 healthy patients and 60 GC patients) | 0.84 (0.77–0.91) | - | - | [81] |
| Sample | Type | Biomarker | Patients | AUC (95% CI) | Sensitivity (%) | Specificity (%) | Ref. |
|---|---|---|---|---|---|---|---|
| Stool Biomarkers | |||||||
| Stool | Protein | GP87 | 231 patients (80 healthy patients, 82 GC patients, 20 chronic superficial gastritis patients, 14 patients with ulcer, 32 CAG patients, and 3 patients with polyps) | - | GC: 79.30 CAG: 84.40 | - | [87] |
| Stool | Protein | M2-PK | 74 patients (20 healthy patients and 54 GC patients) | 50.47 | - | [88] | |
| Sample | Type | Biomarker | Patients | AUC (95% CI) | Sensitivity (%) | Specificity (%) | Ref. |
|---|---|---|---|---|---|---|---|
| Gastric Juice Biomarkers | |||||||
| Gastric juice | DNA | BARHL2 | 30 patients (10 healthy patients, 10 early GC, and 10 advanced GC) | 0.92 | 90.0 | 100.0 | [99] |
| Gastric juice | miRNA | miR-129-1-3p and miR-129-2-3p | 141 patients (47 healthy patients, 42 GC patients, 34 gastric ulcer patients, and 18 atrophic gastritis patients) | 0.66 | 68.70 | 71.90 | [100] |
| Gastric juice | miRNA | miR-421 | 141 patients (47 healthy patients, 42 GC patients, 34 gastric ulcer patients, and 18 atrophic gastritis patients) | 0.77 (0.68–0.85) | 71.40 | 71.70 | [101] |
| Gastric juice | miRNA | miR-21 | 141 patients (47 healthy patients, 42 GC patients, 34 gastric ulcer patients, and 18 atrophic gastritis patients) | 0.97 | 85.70 | 97.80 | [102] |
| Gastric juice | miRNA | miR-106a | 141 patients (47 healthy patients, 42 GC patients, 34 gastric ulcer patients, and 18 atrophic gastritis patients) | 0.87 | 73.80 | 89.30 | [102] |
| Gastric juice | miRNA | miR-133a | 204 patients (34 healthy patients, 62 GC patients, 32 atrophic gastritis, 36 gastric ulcer, and 40 superficial gastritis patients) | 0.91 (0.86–0.96) | 85.90 | 84.80 | [103] |
| Gastric juice | circRNA | circ_0014717 | 122 patients (38 healthy patients, 30 gastric ulcer patients, 15 CAG, and 39 GC patients) | - | - | - | [104] |
| Gastric juice | piRNA | piR-1245 | 132 patients (66 healthy patients and 66 GC patients) | 0.89 | 90.90 | 74.20 | [105] |
| Gastric juice | lncRNA | RMRP | 130 patients (45 healthy patients, 39 GC patients, 30 gastric ulcer patients, and 16 CAG patients) | 0.70 | 56.40 | 75.40 | [107] |
| Gastric juice | lncRNA | AA174084 | 130 patients (45 healthy patients, 39 GC patients, 30 gastric ulcer patients, and 16 CAG patients) | 0.85 (0.78–0.92) | 46.00 | 93.00 | [106] |
| Gastric juice | lncRNA | lncRNA-ABHD11-AS1 | 39 GC patients, 30 patients with gastric ulcers, 16 patients with atrophic gastritis, and 45 patients with normal mucosa/minimal gastritis | 0.65 (0.54–0.77) | 41.00 | 93.40 | [108] |
| Gastric juice | Protein | GP87 | 231 patients (80 healthy patients, 82 GC patients, 20 chronic superficial gastritis patients, 14 patients with ulcer, 32 CAG patients, and 3 patients with polyps) | - | GC: 86.30 CAG: 60.00 | - | [87] |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Herrera-Pariente, C.; Montori, S.; Llach, J.; Bofill, A.; Albeniz, E.; Moreira, L. Biomarkers for Gastric Cancer Screening and Early Diagnosis. Biomedicines 2021, 9, 1448. https://doi.org/10.3390/biomedicines9101448
Herrera-Pariente C, Montori S, Llach J, Bofill A, Albeniz E, Moreira L. Biomarkers for Gastric Cancer Screening and Early Diagnosis. Biomedicines. 2021; 9(10):1448. https://doi.org/10.3390/biomedicines9101448
Chicago/Turabian StyleHerrera-Pariente, Cristina, Sheyla Montori, Joan Llach, Alex Bofill, Eduardo Albeniz, and Leticia Moreira. 2021. "Biomarkers for Gastric Cancer Screening and Early Diagnosis" Biomedicines 9, no. 10: 1448. https://doi.org/10.3390/biomedicines9101448
APA StyleHerrera-Pariente, C., Montori, S., Llach, J., Bofill, A., Albeniz, E., & Moreira, L. (2021). Biomarkers for Gastric Cancer Screening and Early Diagnosis. Biomedicines, 9(10), 1448. https://doi.org/10.3390/biomedicines9101448