

Body Mass Trajectory Affects the Long-Term Occurrence of Metabolic Syndrome in Adult Patients with Severe Obesity

 , , , and
, , , and
Abstract
1. Introduction
2. Methods
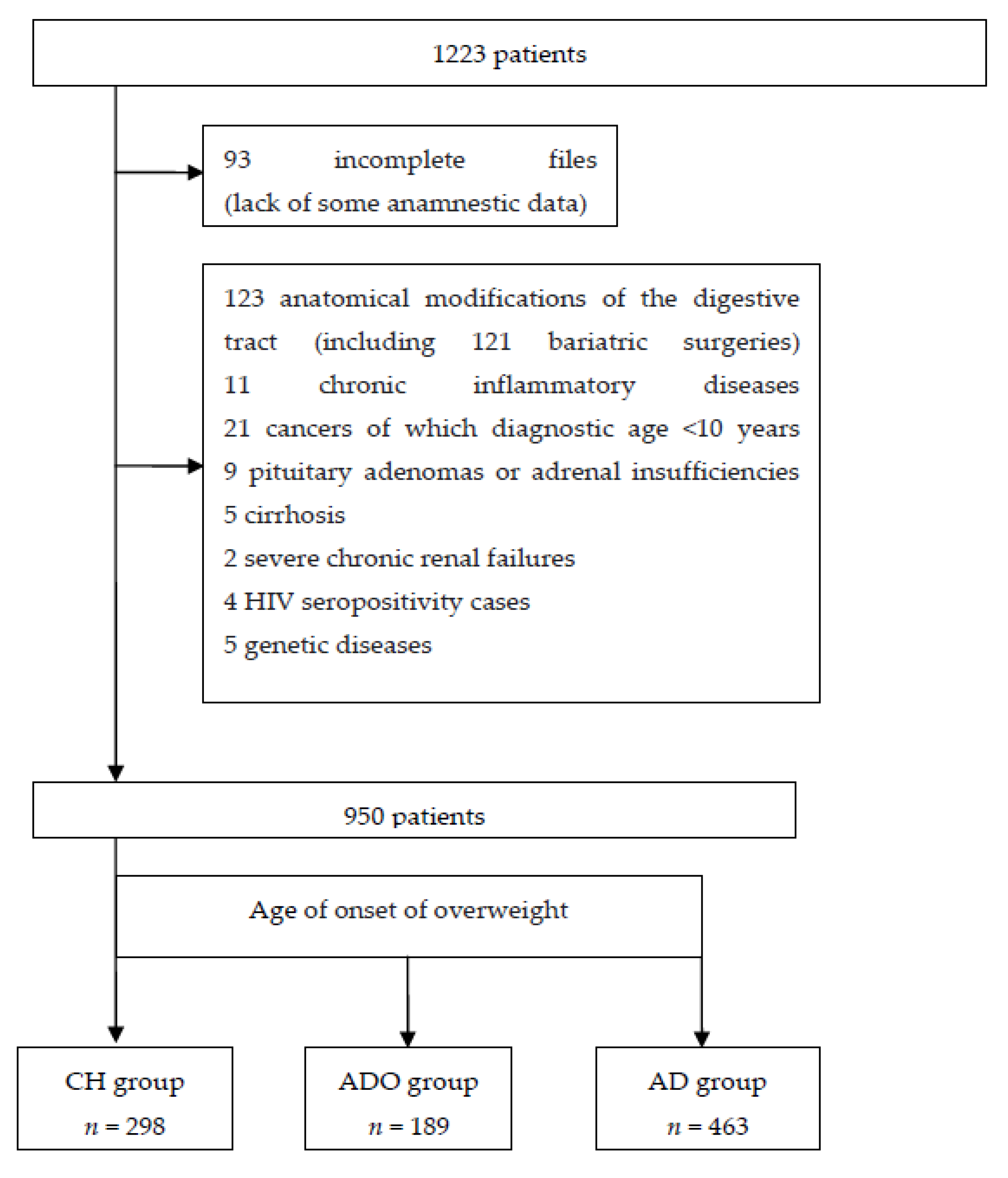
2.1. Design and Eligibility Criteria
2.2. Data Collection
2.3. Statistical Analyses
2.4. Ethical Approval
3. Results
3.1. Anthropometric, Clinical, and Medical History Characteristics
3.2. Overweight History
3.3. Body Composition
3.4. Biological Data
3.5. Metabolic Syndrome and its Criteria
Description
3.6. Univariate Analysis of Metabolic Syndrome by Age, Sex, BMI, Weight History, Body Composition, and Biological Variables
3.7. Multivariate Analysis of Metabolic Syndrome with Propensity Score Weighting
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- The GBD 2013 Obesity Collaboration; Ng, M.; Fleming, T.; Robinson, M.; Thomson, B.; Graetz, N.; Margono, C.; Mullany, E.; Biryukov, S.; Abbafati, C.; et al. Global, regional, and national prevalence of overweight and obesity in children and adults during 1980–2013: A systematic analysis for the Global Burden of Disease Study 2013. Lancet 2014, 384, 766–781. [Google Scholar] [CrossRef]
- GBD 2015 Obesity Collaborators; Afshin, A.; Forouzanfar, M.H.; Reitsma, M.B.; Sur, P.; Estep, K.; Lee, A.; Marczak, L.; Mokdad, A.H.; Moradi-Lakeh, M.; et al. Health Effects of Overweight and Obesity in 195 Countries over 25 Years. N. Engl. J. Med. 2017, 377, 13–27. [Google Scholar]
- Verdot, C.; Torres, M.; Salanave, B.; Deschamps, V. Corpulence des enfants et des adultes en France métropolitaine en 2015. Résultats de l’étude Esteban et évolution depuis 2006. Bull. Epidémiol. Hebd. 2017, 13, 234–241. [Google Scholar]
- Grundy, S.M. Obesity, Metabolic Syndrome, and Cardiovascular Disease. J. Clin. Endocrinol. Metab. 2004, 89, 2595–2600. [Google Scholar] [CrossRef]
- Global BMI Mortality Collaboration; Di Angelantonio, E.; Bhupathiraju, S.; Wormser, D.; Gao, P.; Kaptoge, S.; de Gonzalez, A.B.; Cairns, B.; Huxley, R.; Jackson, C.; et al. Body-mass index and all-cause mortality: Individual-participant-data meta-analysis of 239 prospective studies in four continents. Lancet 2016, 388, 776–786. [Google Scholar] [CrossRef]
- Phillips, C.M. Metabolically healthy obesity across the life course: Epidemiology, determinants, and implications. Ann. N. Y. Acad. Sci. 2017, 1391, 85–100. [Google Scholar] [CrossRef]
- Roberson, L.L.; Aneni, E.C.; Maziak, W.; Agatston, A.S.; Feldman, T.; Rouseff, M.; Tran, T.; Blaha, M.J.; Santos, R.D.; Sposito, A.C.; et al. Beyond BMI: The ‘Metabolically healthy obese’ phenotype & its association with clinical/subclinical cardiovascular disease and all-cause mortality—A systematic review. BMC Public Health 2014, 14, 14. [Google Scholar]
- Rey-López, J.P.; de Rezende, L.F.; Pastor-Valero, M.; Tess, B.H. The prevalence of metabolically healthy obesity: A systematic review and critical evaluation of the definitions used. Obes. Rev. 2014, 15, 781–790. [Google Scholar] [CrossRef]
- Samocha-Bonet, D.; Dixit, V.D.; Kahn, C.R.; Leibel, R.L.; Lin, X.; Nieuwdorp, M.; Pietiläinen, K.; Rabasa-Lhoret, R.; Roden, M.; Scherer, P.E.; et al. Metabolically healthy and unhealthy obese—The 2013 Stock Conference report. Obes. Rev. 2014, 15, 697–708. [Google Scholar] [CrossRef]
- Phillips, C.M.; Dillon, C.; Harrington, J.M.; McCarthy, V.J.C.; Kearney, P.M.; Fitzgerald, A.P.; Perry, I.J. Defining metabolically healthy obesity: Role of dietary and lifestyle factors. PLoS ONE 2013, 8, e76188. [Google Scholar] [CrossRef]
- Spalding, K.L.; Arner, E.; Westermark, P.O.; Bernard, S.; Buchholz, B.A.; Bergmann, O.; Blomqvist, L.; Hoffstedt, J.; Naslund, E.; Britton, T.; et al. Dynamics of fat cell turnover in humans. Nature 2008, 453, 783–787. [Google Scholar] [CrossRef] [PubMed]
- Brochu, M.; Tchernof, A.; Dionne, I.J.; Sites, C.K.; Eltabbakh, G.H.; Sims, E.A.; Poehlman, E.T. What are the physical characteristics associated with a normal metabolic profile despite a high level of obesity in postmenopausal women? J. Clin. Endocrinol. Metab. 2001, 86, 1020–1025. [Google Scholar] [PubMed]
- Lloyd, L.J.; Langley-Evans, S.C.; McMullen, S. Childhood obesity and risk of the adult metabolic syndrome: A systematic review. Int. J. Obes. 2012, 36, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Lloyd, L.J.; Langley-Evans, S.C.; McMullen, S. Childhood obesity and adult cardiovascular disease risk: A systematic review. Int. J. Obes. 2010, 34, 18–28. [Google Scholar] [CrossRef]
- Howe, L.D.; Zimmermann, E.; Weiss, R.; Sørensen, T.I.A. Do rapid BMI growth in childhood and early-onset obesity offer cardiometabolic protection to obese adults in mid-life? Analysis of a longitudinal cohort study of Danish men. BMJ Open 2014, 4, e004827. [Google Scholar] [CrossRef][Green Version]
- Krakauer, N.Y.; Krakauer, J.C. A new body shape index predicts mortality hazard independently of body mass index. PLoS ONE 2012, 7, e39504. [Google Scholar] [CrossRef]
- Jiménez, A.; Omaña, W.; Flores, L.; Coves, M.J.; Bellido, D.; Perea, V.; Vidal, J. Prediction of whole-body and segmental body composition by bioelectrical impedance in morbidly obese subjects. Obes. Surg. 2012, 22, 587–593. [Google Scholar] [CrossRef]
- Janssen, I.; Heymsfield, S.B.; Baumgartner, R.N.; Ross, R. Estimation of skeletal muscle mass by bioelectrical impedance analysis. J. Appl. Physiol. 2000, 89, 465–471. [Google Scholar] [CrossRef]
- Prado, C.; Wells, J.; Smith, S.; Stephan, B.; Siervo, M. Sarcopenic obesity: A Critical appraisal of the current evidence. Clin. Nutr. 2012, 31, 583–601. [Google Scholar] [CrossRef]
- Matthews, D.R.; Hosker, J.P.; Rudenski, A.S.; Naylor, B.A.; Treacher, D.F.; Turner, R.C. Homeostasis model assessment: Insulin resistance and beta-cell function from fasting plasma glucose and insulin concentrations in man. Diabetologia 1985, 28, 412–419. [Google Scholar] [CrossRef]
- Friedewald, W.T.; Levy, R.I.; Fredrickson, D.S. Estimation of the concentration of low-density lipoprotein cholesterol in plasma, without use of the preparative ultracentrifuge. Clin. Chem. 1972, 18, 499–502. [Google Scholar] [CrossRef] [PubMed]
- Norman, A.W.; Bouillon, R.; Whiting, S.J.; Vieth, R.; Lips, P. 13th Workshop consensus for vitamin D nutritional guidelines. J. Steroid Biochem. Mol. Biol. 2007, 103, 204–205. [Google Scholar] [CrossRef] [PubMed]
- Ford, E.S.; Giles, W.H.; Dietz, W.H. Prevalence of the metabolic syndrome among US adults: Findings from the third National Health and Nutrition Examination Survey. JAMA 2002, 287, 356–359. [Google Scholar] [CrossRef] [PubMed]
- Austin, P.C. An Introduction to Propensity Score Methods for Reducing the Effects of Confounding in Observational Studies. Multivar. Behav. Res. 2011, 46, 399–424. [Google Scholar] [CrossRef] [PubMed]
- Salonen, M.; Kajantie, E.; Osmond, C.; Forsén, T.; Ylihärsilä, H.; Paile-Hyvärinen, M.; Barker, D.; Eriksson, J. Role of childhood growth on the risk of metabolic syndrome in obese men and women. Diabetes Metab. 2009, 35, 94–100. [Google Scholar] [CrossRef] [PubMed]
- Aubertin-Leheudre, M.; Lord, C.; Goulet, D.; Khalil, A.; Dionne, I.J. Effect of sarcopenia on cardiovascular disease risk factors in obese postmenopausal women. Obesity 2006, 14, 2277–2283. [Google Scholar] [CrossRef] [PubMed]
- Thearle, M.S.; Bunt, J.C.; Knowler, W.C.; Krakoff, J. Childhood predictors of adult acute insulin response and insulin action. Diabetes Care 2009, 32, 938–943. [Google Scholar] [CrossRef]
- Arner, P.; Bernard, S.; Appelsved, L.; Fu, K.Y.; Andersson, D.P.; Salehpour, M.; Thorell, A.; Rydén, M.; Spalding, K.L. Adipose lipid turnover and long-term changes in body weight. Nat. Med. 2019, 251, 385–1389. [Google Scholar] [CrossRef]


{kind=link}
| Anthropometric, Clinical, and Anamnestic Characteristics | ||||||||
|---|---|---|---|---|---|---|---|---|
| CH a | ADO a | AD a | p | CH b | ADO b | AD b | p | |
| Female % | 75.5 | 86.2 | 73.9 | 0.002 | 78.8 | 76.8 | 76.6 | 0.85 |
| Age (years) | 36.5 (11.9) | 40.1 (12.5) | 51.1 (11.8) | <0.001 | 45.5 (14.9) | 44.1 (13.6) | 45.0 (13.0) | 0.73 |
| BMI c (kg/m2), mean (sd) | 44.4 (7.8) | 42.0 (5.7) | 41.6 (6.8) | <0.001 | 42.6 (7.44) | 42.4 (5.84) | 42.9 (7.66) | 0.76 |
| 30–35% | 7.4 | 6.3 | 13.6 | <0.001 | 15.1 | 5.4 | 10.9 | 0.13 |
| 35–40% | 23.2 | 32.8 | 33.5 | 26.1 | 31.8 | 30.2 | ||
| >40% | 69.5 | 60.8 | 52.9 | 58.8 | 62.8 | 58.9 | ||
| Waist size (cm), mean (sd) | 129 (17.3) | 124 (12.8) | 126 (15.0) | 0.001 | 126 (16.9) | 126 (13.2) | 128 (16.4) | 0.55 |
| Treated arterial hypertension (%) | 22.6 | 27.0 | 48.2 | <0.001 | 38.5 | 36.7 | 37.8 | 0.94 |
| Treated type 2 diabetes (%) | 11.9 | 15.0 | 21.0 | 0.003 | 15.2 | 21.9 | 16 | 0.23 |
| Treated dyslipidemia (%) | 10.4 | 11.3 | 25.6 | <0.001 | 21.3 | 16.7 | 19.6 | 0.66 |
| Weight history | ||||||||
| Weight at age 18, mean (kg) (sd) | 88.9 (22.5) | 77.9 (18.0) | 63.7 (13.2) | <0.001 | 80.5 (21.4) | 78.1 (18.2) | 65.7 (14.1) | <0.001 |
| BMI at age 18, mean (sd) | 32.2 (7.5) | 28.9 (5.8) | 23.6 (3.7) | <0.001 | 29.8 (6.7) | 28.6 (5.7) | 24.3 (4.1) | <0.001 |
| Weight gain since age 18(kg), average percentage (sd) | 43.3 (34.9) | 50.1 (32.9) | 79.3 (33.2) | <0.001 | 47.2 (33.5) | 52.6 (31.9) | 80.8 (34.8) | <0.001 |
| Duration of weight gain (years), mean (sd) | 27.9 (11.5) | 25.6 (12.0) | 21.4 (11.5) | <0.001 | 37.4 (16.2) | 29.2 (13) | 17.7 (10.9) | <0.001 |
| Body composition | ||||||||
| % lean mass, mean (sd) | 55.1 (6.0) | 55.5 (5.3) | 57.5 (6.6) | <0.001 | 56.6 (6.7) | 56.2 (5.7) | 56.3 (6.4) | 0.93 |
| % fat mass, mean (sd) | 44.9 (6.0) | 44.4 (5.3) | 42.5 (6.6) | <0.001 | 43.4 (6.7) | 43.8 (5.7) | 43.7 (6.4) | 0.93 |
| FFMI d (kg/m2), mean (sd) | 24.1 (3.8) | 23.0 (2.5) | 23.7 (3.7) | 0.007 | 23.8 (3.7) | 23.6 (2.8) | 23.9 (4.0) | 0.69 |
| SMI e (kg/m2), mean (sd) | 11.0 (2.1) | 10.3 (1.4) | 10.5 (2.3) | 0.002 | 10.6 (2.2) | 10.6 (1.7) | 10.7 (2.4) | 0.82 |
| FyM f ratio (%) | ||||||||
| <0.4 | 1.48 | 0 | 3.0 | 0.001 | 4.1 | 0 | 2.1 | 0.271 |
| 0.4–0.8 | 43.2 | 48.3 | 54.8 | 49.0 | 51.2 | 49.5 | ||
| >0.8 | 55.4 | 51.7 | 42.2 | 46.9 | 48.8 | 48.4 | ||
| ABSI g (m11/6/kg2/3), mean (sd) | 0.0806 (0.0061) | 0.0805 (0.0054) | 0.0824 (0.0054) | <0.001 | 0.0812 (0.0056) | 0.0812 (0.0057) | 0.0816 (0.0055) | 0.54 |
| Biological characteristics | ||||||||
| Fasting glycemia (g/L), median [IQR] | 0.94 [0.85; 1.03] | 0.96 [0.87; 1.09] | 1.00 [0.90; 1.16] | <0.001 | 0.96 [0.85; 1.04] | 0.98 [0.88; 1.15] | 0.98 [0.87; 1.12] | 0.01 |
| HDL h-cholesterol (g/L), mean (sd) | 0.45 (0.14) | 0.46 (0.12) | 0.47 (0.13) | 0.17 | 0.48 (0.14) | 0.47 (0.12) | 0.45 (0.12) | 0.19 |
| LDL i-cholesterol (g/L), mean (sd) | 1.17 (0.35) | 1.18 (0.31) | 1.20 (0.35) | 0.53 | 1.21 (0.36) | 1.17 (0.33) | 1.18 (0.34) | 0.75 |
| Triglyceridemia (g/L), median [IQR] | 1.14 [0.84; 1.64] | 1.14 [0.81; 1.66] | 1.23 [0.90; 1.67] | 0.06 | 1.13 [0.81; 1.75] | 1.14 [0.8; 1.66] | 1.23 [0.88; 1.66] | 0.66 |
| Hba1c j median [IQR] | 5.70 [5.40; 6.10] | 5.70 [5.40; 6.20] | 6.00 [5.60; 6.50] | <0.001 | 5.9 [5.5; 6.1] | 5.7 [5.4; 6.6] | 5.9 [5.6; 6.3] | 0.27 |
| Homa IR ≥ 2.5 (%) | 72.3 | 69.1 | 75.9 | 0.23 | 65.2 | 71.5 | 77.0 | 0.12 |
| CRP (mg/L), median [IQR] | 5.90 [3.10; 11.2] | 6.40 [3.6; 10.6] | 5.70 [3.00; 9.72] | 0.12 | 4.80 [2.90; 9.5] | 6.5 [3.50; 10.4] | 6.3 [3.0; 10.9] | 0.08 |
| Ferritin (µg/L), median [IQR] | 82 [42; 161] | 79 [40; 179] | 126 [59; 247] | <0.001 | 86 [55; 169] | 105 [45; 213] | 116 [56; 229] | 0.01 |
| Vitamin D (µg/L), mean (sd) | 14.1 (7.5) | 14.4 (8.0) | 13.9 (8.0) | 0.80 | 15.2 (7.81) | 14 (7.9) | 13.8 (7.76) | 0.28 |
| <10 | 4.3 | 3.3 | 4.9 | 0.59 | 5.4 | 3.5 | 4.1 | 0.48 |
| 10–30 | 60.3 | 64.1 | 56.6 | 65.2 | 61.1 | 57 | ||
| >30 | 35.5 | 32.7 | 38.5 | 29.4 | 35.5 | 38.9 | ||
| Metabolic syndrome and its criteria | ||||||||
| Measured or treated arterial hypertension k (%) | 56.0 | 50.3 | 72.1 | <0.001 | 64.2 | 59.5 | 61.2 | 0.62 |
| Measured or treated type 2 diabetes k (%) | 20.1 | 25.4 | 37.4 | <0.001 | 22.7 | 33.6 | 32.1 | 0.06 |
| Hyper HDL j (%) | 62.1 | 62.8 | 55.0 | 0.07 | 59.7 | 57.7 | 61.1 | 0.80 |
| Hypertriglyceridemia k (%) | 30.9 | 29.8 | 32.9 | 0.70 | 33.5 | 32.1 | 32.5 | 0.95 |
| Metabolic syndrome (%) | 51.7 | 52.9 | 63.7 | 0.001 | 54.4 | 57.7 | 59.8 | 0.59 |
| No MetS (n = 401) | MetS (n = 549) | p | |
|---|---|---|---|
| Anthropometric, clinical, and anamnestic characteristics | |||
| Female (%) | 83.3 | 72.1 | <0.001 |
| Age, mean (sd) | 41.28 (13.83) | 46.54 (13.28) | <0.001 |
| BMI, mean (sd) | 41.70 (6.86) | 43.16 (7.11) | 0.002 |
| 30–35 | 13.5 | 7.8 | 0.003 |
| 35–40 | 32.2 | 28.6 | |
| >40 | 54.4 | 63.6 | |
| Weight history | |||
| BMI at 18, mean (sd) | 28.41 (7.20) | 26.79 (6.43) | 0.001 |
| Weight gain since age 18 (kg), average % (sd) | 53.90 (38.65) | 67.38 (35.71) | <0.001 |
| Duration of weight gain (years), mean (sd) | 23.34 (11.33) | 24.72 (12.30) | 0.128 |
| % of lean mass, mean (sd) | 56.09 (5.81) | 56.59 (6.61) | 0.25 |
| % of fat mass, mean (sd) | 43.91 (5.81) | 43.43 (6.59) | 0.27 |
| FFMI (kg/m2), mean (sd) | 10.31 (1.88) | 10.86 (2.27) | <0.001 |
| SMI (kg/m2), mean (sd) | 0.80 (0.18) | 0.79 (0.21) | 0.42 |
| FyM, mean (sd) | 0.08 (0.01) | 0.08 (0.01) | 0.99 |
| ABSI (m11/6/kg2/3), mean (sd) | 111.25 (21.28) | 118.00 (24.64) | <0.001 |
| Biological characteristics | |||
| CRP, median [IQR] | 6 [3; 10] | 6 [3.2; 10.6] | 0.29 |
| Fasting glycemia (g/L), median [IQR] | 0.91 [0.85; 0.98] | 1.05 [0.93; 1.24] | <0.001 |
| Hba1c, median [IQR] | 5.7 [5.4,;5.9] | 6 [5.6; 6.65] | <0.001 |
| Insulinemia, median [IQR] | 14.6 [8.8; 20.8] | 19.4 [13.2; 27.7] | <0.001 |
| Homa IR, median [IQR] | 3.1 [1.8; 4.5] | 5 [3.15; 7.95] | <0.001 |
| Homa IR ≥ 2.5 | |||
| Ferritin (µg/L), median [IQR] | 75 [38; 150] | 128 [59; 236] | <0.001 |
| Vitamin D (µg/L), mean (sd) | 15.05 (8.01) | 13.34 (7.68) | 0.003 |
| <10 | 15 (4.7) | 18 (4.1) | 0.05 |
| 10–30 | 206 (64) | 243 (55.7) | |
| >30 | 101 (31.4) | 175 (40.1) | |
| Variables | ||
|---|---|---|
| OR [95% CI] | p | |
| Onset of overweight | ||
| Childhood (Ref) | ||
| Adolescence | 1.14 [0.69; 1.92] | 0.60 |
| Adulthood | 0.99 [0.62; 1.56] | 0.95 |
| Weight gain by more than 50% of weight at age 18 years (%) | 1.75 [1.07; 2.88] | 0.03 |
| Age < 35 (Ref) | ||
| 35–45 | 1.27 [0.81; 1.98] | 0.30 |
| 45–55 | 1.60 [0.97; 2.62] | 0.07 |
| >55 | 2.11 [1.04; 4.26] | 0.04 |
| ABSI 1000 (m11/6/kg2/3) | 1.07 [1.04–1.11] | <0.0001 |
| Female | 0.60 [0.37; 0.96] | 0.03 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hazart, J.; Montel, F.; Gentes, E.; Lahaye, C.; Pouget, M.; Farigon, N.; Miolanne, M.; Mulliez, A.; Boirie, Y. Body Mass Trajectory Affects the Long-Term Occurrence of Metabolic Syndrome in Adult Patients with Severe Obesity. Children 2023, 10, 27. https://doi.org/10.3390/children10010027
Hazart J, Montel F, Gentes E, Lahaye C, Pouget M, Farigon N, Miolanne M, Mulliez A, Boirie Y. Body Mass Trajectory Affects the Long-Term Occurrence of Metabolic Syndrome in Adult Patients with Severe Obesity. Children. 2023; 10(1):27. https://doi.org/10.3390/children10010027
Chicago/Turabian StyleHazart, Juliette, Florence Montel, Elodie Gentes, Clément Lahaye, Mélanie Pouget, Nicolas Farigon, Magalie Miolanne, Aurélien Mulliez, and Yves Boirie. 2023. "Body Mass Trajectory Affects the Long-Term Occurrence of Metabolic Syndrome in Adult Patients with Severe Obesity" Children 10, no. 1: 27. https://doi.org/10.3390/children10010027
APA StyleHazart, J., Montel, F., Gentes, E., Lahaye, C., Pouget, M., Farigon, N., Miolanne, M., Mulliez, A., & Boirie, Y. (2023). Body Mass Trajectory Affects the Long-Term Occurrence of Metabolic Syndrome in Adult Patients with Severe Obesity. Children, 10(1), 27. https://doi.org/10.3390/children10010027