
Kinematic Gait Impairments in Children with Clubfeet Treated by the Ponseti Method: A Systematic Review and Meta-Analysis

 , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Protocol and Registration
2.2. Eligibility Criteria
2.3. Literature Search
2.4. Study Selection Procedure
2.5. Data Extraction
2.6. Risk of Bias Assessment
2.7. Data Synthesis and Analysis
3. Results
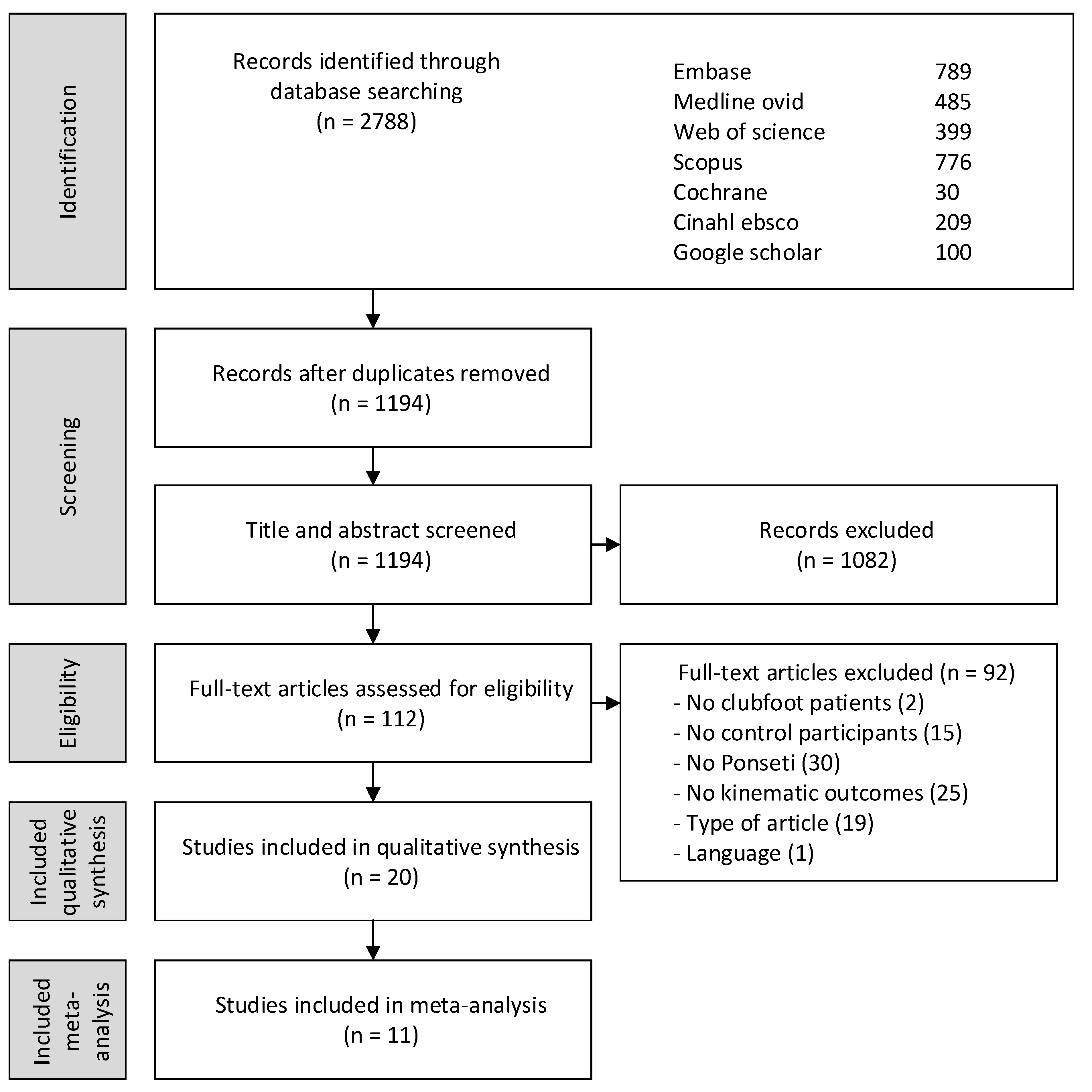
3.1. Study Selection and Characteristics
3.2. Risk of Bias Assessment
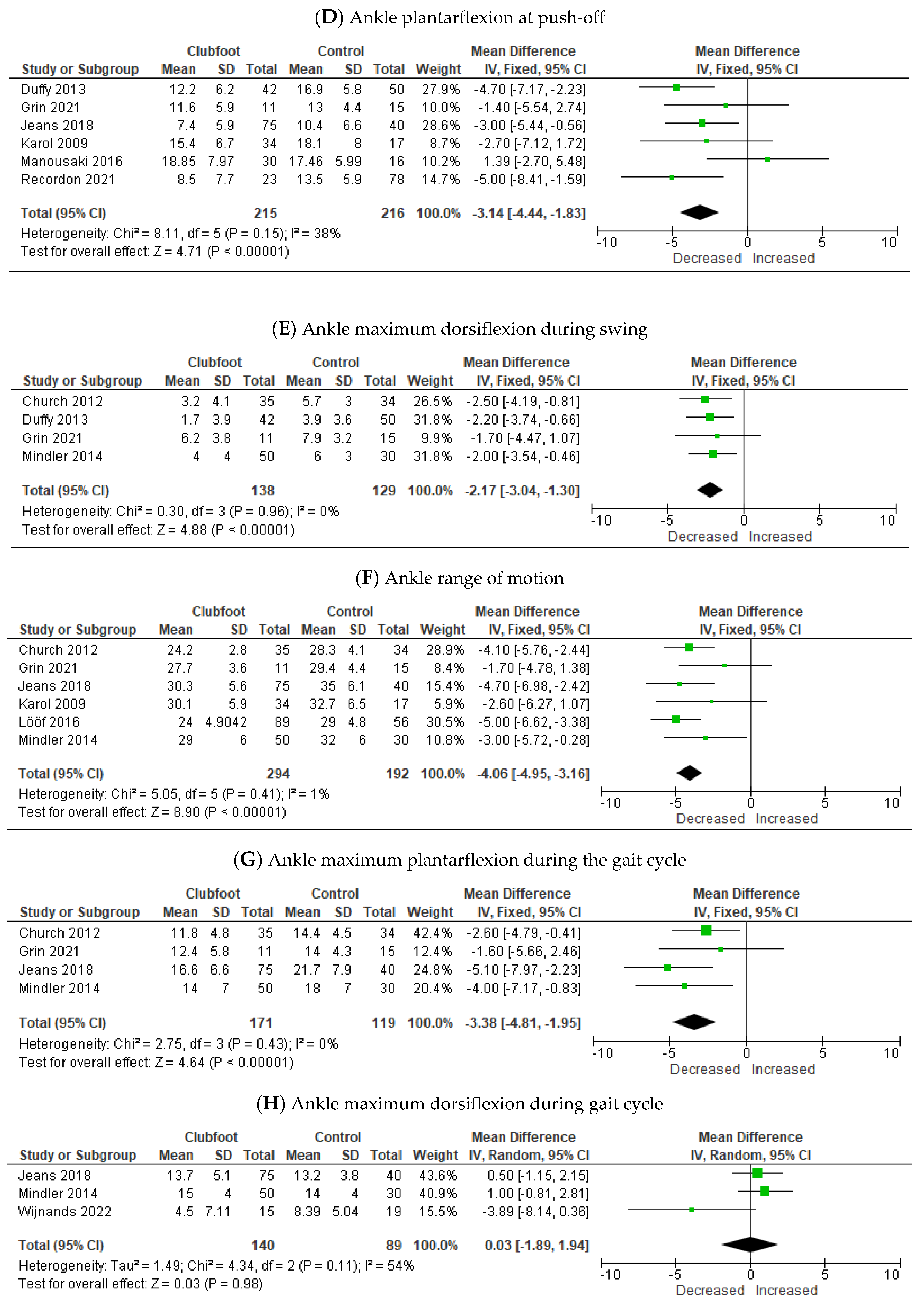
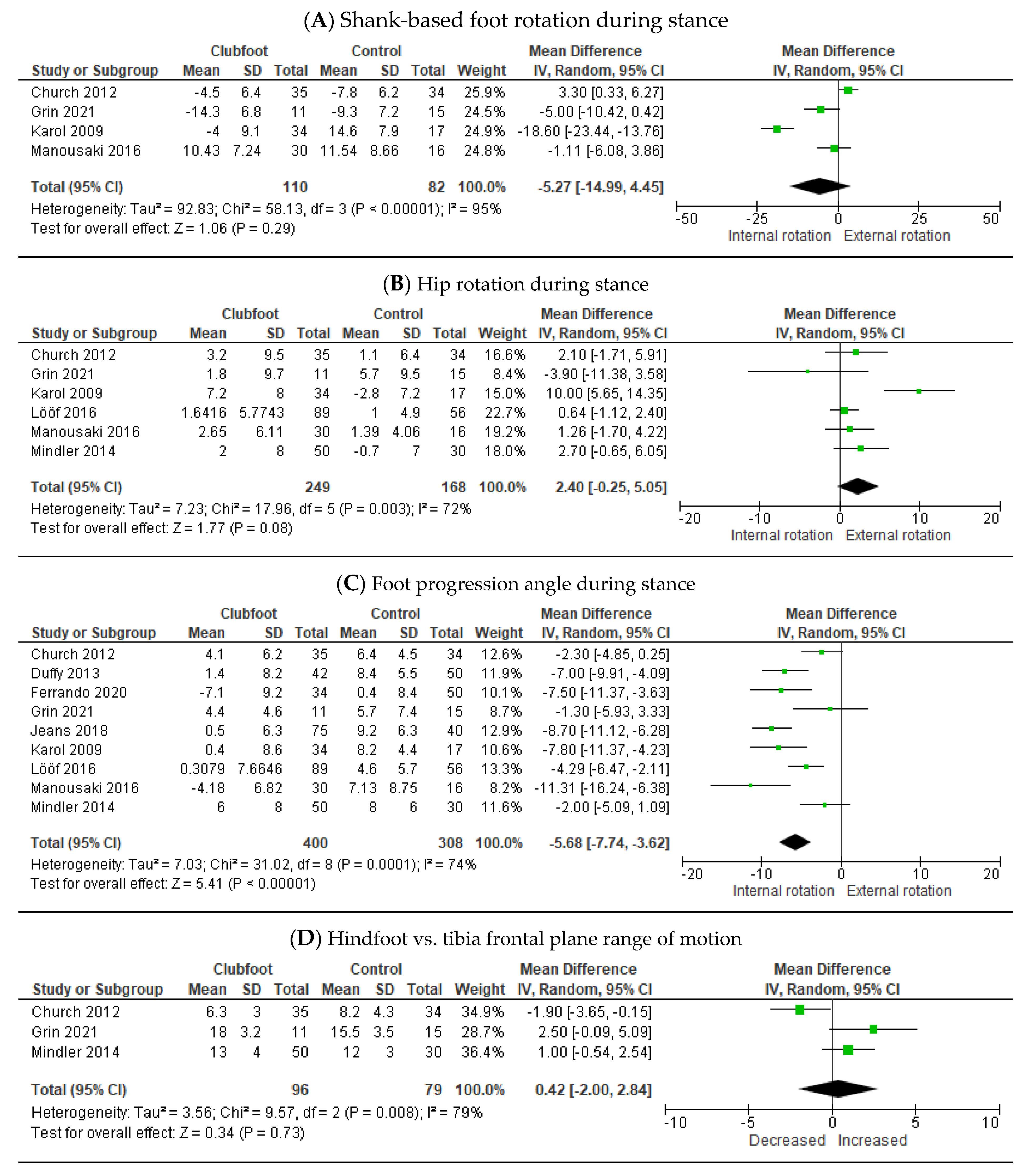
3.3. Meta-Analysis Clubfoot Treated with the Ponseti Method versus Controls
3.4. Qualitative Analysis Clubfoot Treated with the Ponseti Method versus Controls
3.4.1. Stance Phase
3.4.2. Swing phase
3.4.3. Gait Cycle
3.5. Qualitative Analysis Pre-Treatment Relapsed Clubfoot versus Controls
3.5.1. Multi-Segment Foot Model
3.5.2. Conventional Gait Model
3.5.3. Conflicting Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A. Example Literature Search Embase.com
- Embase.com
Appendix B. Risk of Bias

{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Study | Selection | Groups | Measurement | Blinded | Prognostic Factors |
|---|---|---|---|---|---|
| Karol 2009 [24] | − | + | + | ? | + |
| Church 2012 [25] | + | ? | + | ? | ? |
| Duffy 2012 [36] | ? | + | + | ? | ? |
| Smith 2014 [37] | − | − | + | − | − |
| Mindler 2014 [38] | ? | + | + | ? | ? |
| Manousaki 2016 [39] | + | ? | + | ? | ? |
| Lööf 2016 [40] | ? | + | + | ? | ? |
| Jeans 2018 [41] | − | ? | + | ? | + |
| Manousaki 2019 [42] | + | ? | + | ? | − |
| Lööf 2019 [43] | ? | + | + | ? | + |
| Dussa 2020 [26] | + | + | + | ? | ? |
| Ferrando 2020 [27] | + | + | + | ? | ? |
| McCahill 2020 [28] | ? | + | + | ? | ? |
| Mindler 2020 [29] | + | + | + | ? | ? |
| Grin 2021 [30] | − | + | + | ? | ? |
| Li 2021 [31] | + | + | + | ? | + |
| Recordon 2021 [32] | ? | ? | + | ? | + |
| Brierty 2022 [35] | ? | + | + | ? | ? |
| Grin 2022 [33] | − | + | + | ? | ? |
| Wijnands 2022 [34] | − | + | + | ? | ? |
Appendix C. Results Dussa et al. (Overcorrected Clubfoot vs. Controls)
| Outcome Measure | Moment in Gait Cycle | Significance | |
|---|---|---|---|
| Hindfoot vs. tibia |
Peak dorsiflexion Peak eversion Peak internal rotation ROM sagittal (DF/PF) ROM frontal (INV/EV) ROM transversal (INT/EXT) Plantar flexion Inversion | Stance Stance Stance Stance Stance Stance Toe-off Toe-off |
Overcorrect < controls Overcorrect > controls No significance Overcorrect < controls Overcorrect < controls Overcorrect > controls No significance Overcorrect < controls |
| Forefoot vs. hindfoot |
Mean supination Peak dorsiflexion Peak pronation Peak adduction Sagittal ROM (PF/DF) Frontal ROM (PRO/SUP) Transversal ROM (AB/AD) | Gait cycle Stance Stance Stance Stance Stance Stance |
Overcorrect > controls Overcorrect > controls Overcorrect > controls No significance No significance No significance No significance |
| Hallux vs. forefoot |
Sagittal ROM (FLEX/EXT) Flexion Mean flexion Sagittal ROM (FLEX/EXT) | Stance Toe-off Swing Swing |
No significance Overcorrect < controls Overcorrect < controls No significance |
Appendix D. Ponseti vs. Controls—Additional Outcome Measures Presented in Different Studies
| Outcome Measure | Moment in Gait Cycle | Studies | Significance | |
|---|---|---|---|---|
| Foot |
Foot progression Shank-based foot rotation (INT) |
Mid-stance Swing | [32] [30] |
No significant difference No significant difference |
| Hindfoot vs. tibia |
ROM sagittal (DF/PF) ROM transversal (INT/EXT) Max. plantar flexion Dorsiflexion Max. dorsiflexion Mean dorsiflexion Mean adduction Mean inversion/eversion Plantar flexion Adduction Mean adduction Mean plantar/dorsiflexion Max. dorsiflexion Mean inversion/eversion |
Gait cycle Gait cycle Gait cycle Initial contact Stance Stance Stance Stance Toe-off Toe-off Swing Swing Swing Swing | [30,38] [30,38] [30] [30] [30] [30] [25,30] [30] [30] [30] [30] [30] [30] [30] |
No significant difference No significant difference No significant difference No significant difference No significant difference No significant difference No significant difference No significant difference No significant difference No significant difference No significant difference No significant difference No significant difference No significant difference |
| Forefoot vs. hindfoot |
ROM frontal (PRO/SUP) ROM transversal (AB/AD) Max. plantar flexion Dorsiflexion Max. dorsiflexion Mean dorsiflexion Mean adduction Mean supination/pronation Plantar flexion Adduction Mean adduction Mean plantar/dorsiflexion Max. dorsiflexion Mean supiation/pronation |
Gait cycle Gait cycle Gait cycle Initial contact Stance Stance Stance Stance Toe-off Toe-off Swing Swing Swing Swing | [30,38] [30,38] [30] [30] [30] [30] [30] [25,30] [30] [30] [30] [30] [30] [30] |
No significant difference No significant difference No significant difference No significant difference No significant difference No significant difference No significant difference No significant difference No significant difference No significant difference No significant difference No significant difference No significant difference No significant difference |
| Forefoot vs. tibia |
Peak plantar flexion Dorsiflexion Max. dorsiflexion Mean dorsiflexion Mean adduction Mean supination/pronation Plantar flexion Adduction Mean adduction Mean plantar/dorsiflexion Max. dorsiflexion Mean supination/pronation |
Gait cycle Initial contact Stance Stance Stance Stance Toe-off Toe-off Swing Swing Swing Swing | [30] [30] [30] [30] [30] [30] [30] [30] [30] [30] [30] [30] |
No significant difference No significant difference No significant difference No significant difference No significant difference No significant difference No significant difference No significant difference No significant difference No significant difference No significant difference No significant difference |
| Ankle |
Mean dorsiflexion ROM PF/DF Dorsiflexion Mean dorsiflexion |
Stance Stance End of swing Terminal swing | [24,30] [32] [24,39] [40] |
No significant difference No significant difference No significant difference No significant difference |
| Knee |
Mean rotation ROM sagittal |
Gait cycle Gait cycle | [38] [30] |
No significant difference No significant difference |
| Hip | External rotation | Initial contact | [40] | No significant difference |
| Pelvis | Mean tilt ROM transversal Max. rotation (EXT) Max. rotation (INT) | Gait cycle Gait cycle Gait cycle Gait cycle | [30] [30] [30] [30] | No significant difference No significant difference No significant difference No significant difference |
| Total gait scores |
GPS overall GPS affected side GVS pelvis anterior/posterior GVS pelvis int/ext rotation GVS pelvis up/down GVS hip flexion/extension GVS hip adduction/abduction GVS hip int/ext rotation GVS knee flexion/extension GVS ankle dorsal/plantar flexion GVS foot int/ext rotation GDI * FDI * cFDI * |
Gait cycle Gait cycle Gait cycle Gait cycle Gait cycle Gait cycle Gait cycle Gait cycle Gait cycle Gait cycle Gait cycle Gait cycle Gait cycle Gait cycle | [42] [42] [42] [42] [42] [42] [42] [42] [42] [42] [42] [33] [33] [33] |
- - - - - - - - - - - No deviation 1 No deviation 1 No deviation 1 |
Appendix E. Relapsed Clubfoot Pre-Treatment vs. Controls—Additional Outcome Measures Presented in Different Studies
| Outcome Measure | Moment in Gait Cycle | Studies | Significance | |
|---|---|---|---|---|
| Foot | Foot progression angle | Gait cycle | [28] | Foot progression angle |
| Hindfoot vs. tibia |
ROM frontal (INV/EV) Max. plantarflexion Mean dorsiflexion Mean inversion Inversion/eversion Adduction Mean dorsiflexion Mean inversion/eversion Plantarflexion Adduction Mean adduction Mean plantar/dorsiflexion Max. dorsiflexion Mean inversion/eversion Varus |
Gait cycle Gait cycle Gait cycle Gait cycle Initial contact Initial contact Stance Stance Toe-off Toe-off Swing Swing Swing Swing 80% gait cycle | [26,27,28] [27,28] [26] [26] [27] [27] [28] [28] [28] [28] [27,28] [28] [28] [28] [27] |
No significant difference No significant difference No significant difference No significant difference No significant difference No significant difference No significant difference No significant difference No significant difference No significant difference No significant difference No significant difference No significant difference No significant difference No significant difference |
| Forefoot vs. hindfoot |
ROM transversal (AB/AD) Mean dorsiflexion Mean supination Mean adduction Supination Adduction Mean dorsiflexion Mean supination/pronation Plantarflexion Mean adduction Mean plantar/dorsiflexion Mean supination/pronation Supination |
Gait cycle Gait cycle Gait cycle Gait cycle Initial contact Initial contact Stance Stance Toe-off Swing Swing Swing 80% gait cycle | [26,27,28] [26] [26] [26] [27] [27] [28] [28] [28] [27,28] [28] [28] [27] |
No significant difference No significant difference No significant difference No significant difference No significant difference No significant difference No significant difference No significant difference No significant difference No significant difference No significant difference No significant difference No significant difference |
| Forefoot vs. tibia |
ROM frontal (PRO/SUP) Mean dorsiflexion Mean supination Dorsiflexion Max. dorsiflexion Mean dorsiflexion Mean supination/pronation Adduction Mean plantar/dorsiflexion Max. dorsiflexion |
Gait cycle Gait cycle Gait cycle Initial contact Stance Stance Stance Toe-off Swing Swing | [28] [26] [26] [27,28] [27,28] [28] [28] [28] [28] [28] |
No significant difference No significant difference No significant difference No significant difference No significant difference No significant difference No significant difference No significant difference No significant difference No significant difference |
| Ankle |
Max. plantarflexion Dorsiflexion Mean dorsiflexion Max. dorsiflexion Max. dorsiflexion Mean plantar/dorsiflexion |
Gait cycle Initial contact Stance Stance Swing Swing | [28] [28] [28] [28] [28] [28] |
No significant difference No significant difference No significant difference No significant difference No significant difference No significant difference |
| Knee |
ROM sagittal (PF/DF) Max. extension Max. flexion |
Gait cycle Stance Swing | [28] [28] [28] |
No significant difference No significant difference No significant difference |
| Hip | Max. rotation (EXT) | Gait cycle | [28] | Max. rotation (EXT) |
| Pelvis | Mean tilt ROM transversal Max. rotation (EXT) Max. rotation (INT) | Gait cycle Gait cycle Gait cycle Gait cycle | [28] [28] [28] [28] | No significant difference No significant difference No significant difference No significant difference |
| Total gait scores |
FDI * FVS forefoot frontal |
Gait cycle Gait cycle | [31] [26] |
No deviation 1 No significant difference |
References
- Mustari, M.N.; Faruk, M.; Bausat, A.; Fikry, A. Congenital Talipes Equinovarus: A Literature Review. Ann. Med. Surg. 2022, 81, 104394. [Google Scholar] [CrossRef] [PubMed]
- Dibello, D.; Torelli, L.; Di Carlo, V.; D’Adamo, A.P.; Faletra, F.; Mangogna, A.; Colin, G. Incidence of Congenital Clubfoot: Preliminary Data from Italian CeDAP Registry. Int. J. Environ. Res. Public Health 2022, 19, 5406. [Google Scholar] [CrossRef] [PubMed]
- Esbjörnsson, A.-C.; Johansson, A.; Andriesse, H.; Wallander, H. Epidemiology of Clubfoot in Sweden from 2016 to 2019: A National Register Study. PLoS ONE 2021, 16, e0260336. [Google Scholar] [CrossRef] [PubMed]
- Ponseti, I.V.; Zhivkov, M.; Davis, N.; Sinclair, M.; Dobbs, M.B.; Morcuende, J.A. Treatment of the Complex Idiopathic Clubfoot. Clin. Orthop. Relat. Res. 2006, 451, 171–176. [Google Scholar] [CrossRef]
- Gray, K.; Pacey, V.; Gibbons, P.; Little, D.; Burns, J. Interventions for Congenital Talipes Equinovarus (Clubfoot). Cochrane Database Syst. Rev. 2014, 2014, CD008602. [Google Scholar] [CrossRef] [PubMed]
- Bergerault, F.; Fournier, J.; Bonnard, C. Idiopathic Congenital Clubfoot: Initial Treatment. Orthop. Traumatol. Surg. Res. 2013, 99, S150–S159. [Google Scholar] [CrossRef] [PubMed]
- Shabtai, L.; Specht, S.C.; Herzenberg, J.E. Worldwide Spread of the Ponseti Method for Clubfoot. World J. Orthop. 2014, 5, 585–590. [Google Scholar] [CrossRef]
- Thomas, H.M.; Sangiorgio, S.N.; Ebramzadeh, E.; Zionts, L.E. Relapse Rates in Patients with Clubfoot Treated Using the Ponseti Method Increase with Time: A Systematic Review. JBJS Rev. 2019, 7, e6. [Google Scholar] [CrossRef]
- Gelfer, Y.; Wientroub, S.; Hughes, K.; Fontalis, A.; Eastwood, D.M. Congenital Talipes Equinovarus: A Systematic Review of Relapse as a Primary Outcome of the Ponseti Method. Bone Jt. J. 2019, 101-B, 639–645. [Google Scholar] [CrossRef]
- Hu, W.; Ke, B.; Niansu, X.; Li, S.; Li, C.; Lai, X.; Huang, X. Factors Associated with the Relapse in Ponseti Treated Congenital Clubfoot. BMC Musculoskelet. Disord. 2022, 23, 88. [Google Scholar] [CrossRef]
- Radler, C. The Treatment of Recurrent Congenital Clubfoot. Foot Ankle Clin. 2021, 26, 619–637. [Google Scholar] [CrossRef] [PubMed]
- Gaber, K.; Mir, B.; Shehab, M.; Kishta, W. Updates in the Surgical Management of Recurrent Clubfoot Deformity: A Scoping Review. Curr. Rev. Musculoskelet. Med. 2022, 15, 75–81. [Google Scholar] [CrossRef] [PubMed]
- WHO-FIC CC. International Classification of Functioning, Disability and Health, Children & Youth Version; Bohn Stafleu van Loghum: Houten, The Netherlands, 2018. [Google Scholar]
- Gelfer, Y.; Leo, D.G.; Russell, A.; Bridgens, A.; Perry, D.C.; Eastwood, D.M. The Outcomes of Idiopathic Congenital Talipes Equinovarus: A Core Outcome Set for Research and Treatment. Bone Jt. Open 2022, 3, 98–106. [Google Scholar] [CrossRef] [PubMed]
- Cimolin, V.; Galli, M. Summary Measures for Clinical Gait Analysis: A Literature Review. Gait Posture 2014, 39, 1005–1010. [Google Scholar] [CrossRef] [PubMed]
- Graf, A.; Wu, K.W.; Smith, P.A.; Kuo, K.N.; Krzak, J.; Harris, G. Comprehensive Review of the Functional Outcome Evaluation of Clubfoot Treatment: A Preferred Methodology. J. Pediatr. Orthop. B 2012, 21, 20–27. [Google Scholar] [CrossRef] [PubMed]
- Karol, L.A.; Jeans, K.A. Assessment of Clubfoot Treatment Using Movement Analysis. J. Exp. Clin. Med. 2011, 3, 228–232. [Google Scholar] [CrossRef]
- Bent, M.; Hauschild, M.; Rethlefsen, S.A.; Wren, T.A.L.; Liang, A.; Goldstein, R.Y.; Kay, R.M. Gait Analysis Characteristics in Relapsed Clubfoot. J. Pediatr. Orthop. 2023, 43, 65–69. [Google Scholar] [CrossRef]
- Tuinsma, A.B.M.; Vanwanseele, B.; van Oorschot, L.; Kars, H.J.J.; Grin, L.; Reijman, M.; Besselaar, A.T.; van der Steen, M.C. Gait Kinetics in Children with Clubfeet Treated Surgically or with the Ponseti Method: A Meta-Analysis. Gait Posture 2018, 66, 94–100. [Google Scholar] [CrossRef]
- Pierz, K.A.; Lloyd, J.R.; Solomito, M.J.; Mack, P.; Õunpuu, S. Lower Extremity Characteristics in Recurrent Clubfoot: Clinical and Gait Analysis Findings That May Influence Decisions for Additional Surgery. Gait Posture 2020, 75, 85–92. [Google Scholar] [CrossRef]
- Liberati, A.; Altman, D.G.; Tetzlaff, J.; Mulrow, C.; Gotzsche, P.C.; Ioannidis, J.P.; Clarke, M.; Devereaux, P.J.; Kleijnen, J.; Moher, D. The PRISMA Statement for Reporting Systematic Reviews and Meta-Analyses of Studies That Evaluate Health Care Interventions: Explanation and Elaboration. PLoS Med. 2009, 6, e1000100. [Google Scholar] [CrossRef]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; Group, P. Preferred Reporting Items for Systematic Reviews and Meta-Analyses: The PRISMA Statement. BMJ 2009, 339, b2535. [Google Scholar] [CrossRef] [PubMed]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 Statement: An Updated Guideline for Reporting Systematic Reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef] [PubMed]
- Karol, L.A.; Jeans, K.; Elhawary, R. Gait Analysis after Initial Nonoperative Treatment for Clubfeet: Intermediate Term Followup at Age 5. Clin. Orthop. Relat. Res. 2009, 467, 1206–1213. [Google Scholar] [CrossRef] [PubMed]
- Church, C.; Coplan, J.A.; Poljak, D.; Thabet, A.M.; Kowtharapu, D.; Lennon, N.; Marchesi, S.; Henley, J.; Starr, R.; Mason, D.; et al. A Comprehensive Outcome Comparison of Surgical and Ponseti Clubfoot Treatments with Reference to Pediatric Norms. J. Child. Orthop. 2012, 6, 51–59. [Google Scholar] [CrossRef]
- Dussa, C.U.; Böhm, H.; Döderlein, L.; Forst, R.; Fujak, A. Does an Overcorrected Clubfoot Caused by Surgery or by the Ponseti Method Behave Differently? Gait Posture 2020, 77, 308–314. [Google Scholar] [CrossRef]
- Ferrando, A.; Salom, M.; Page, A.; Perez-Girbes, A.; Atienza, C.; Minguez, M.F.; Prat, J. Talipes Equinovarus Treatment in Infants Treated by the Ponseti Method Compared with Posterior-Only Release: A Mid-Childhood Comparison of Results. J. Foot Ankle Surg. 2020, 59, 919–926. [Google Scholar] [CrossRef]
- McCahill, J.L.; Stebbins, J.; Harlaar, J.; Prescott, R.; Theologis, T.; Lavy, C. Foot Function during Gait and Parental Perceived Outcome in Older Children with Symptomatic Club Foot Deformity. Bone Jt. Open 2020, 1, 384–391. [Google Scholar] [CrossRef]
- Mindler, G.T.; Kranzl, A.; Radler, C. Normalization of Forefoot Supination after Tibialis Anterior Tendon Transfer for Dynamic Clubfoot Recurrence. J. Pediatr. Orthop. 2020, 40, 418–424. [Google Scholar] [CrossRef]
- Grin, L.; van der Steen, M.C.; Wijnands, S.D.N.; van Oorschot, L.; Besselaar, A.T.; Vanwanseele, B. Forefoot Adduction and Forefoot Supination as Kinematic Indicators of Relapse Clubfoot. Gait Posture 2021, 90, 415–421. [Google Scholar] [CrossRef]
- Li, J.; Xun, F.; Li, Y.; Liu, Y.; Xu, H.; Canavese, F. Three-Dimensional Gait Analysis in Children with Recurrent Idiopathic Clubfoot Undergoing Complete Tibialis Anterior Tendon Transfer. J. Pediatr. Orthop. B 2022, 31, 397–406. [Google Scholar] [CrossRef]
- Recordon, J.A.F.; Halanski, M.A.; Boocock, M.G.; McNair, P.J.; Stott, N.S.; Crawford, H.A. A Prospective, Median 15-Year Comparison of Ponseti Casting and Surgical Treatment of Clubfoot. J. Bone Jt. Surg. Am. 2021, 103, 1986–1995. [Google Scholar] [CrossRef] [PubMed]
- Grin, L.; Wijnands, S.; Besselaar, A.; van Oorschot, L.; Vanwanseele, B.; van der Steen, M. The Relation between Clinical and Objective Gait Scores in Clubfoot Patients with and without a Relapse. Gait Posture 2022, 97, 210–215. [Google Scholar] [CrossRef] [PubMed]
- Wijnands, S.D.N.; van der Steen, M.C.; Grin, L.; van Oorschot, L.; Besselaar, A.T.; Vanwanseele, B. Muscle-Tendon Properties and Functional Gait Outcomes in Clubfoot Patients with and without a Relapse Compared to Typically Developing Children. Gait Posture 2022, 93, 47–53. [Google Scholar] [CrossRef] [PubMed]
- Brierty, A.; Horan, S.; Giacomozzi, C.; Johnson, L.; Bade, D.; Carty, C.P. Kinematic Differences in the Presentation of Recurrent Congenital Talipes Equinovarus (Clubfoot). Gait Posture 2022, 96, 195–202. [Google Scholar] [CrossRef] [PubMed]
- Duffy, C.M.; Salazar, J.J.; Humphreys, L.; McDowell, B.C. Surgical versus Ponseti Approach for the Management of CTEV: A Comparative Study. J. Pediatr. Orthop. 2013, 33, 326–332. [Google Scholar] [CrossRef]
- Smith, P.A.; Kuo, K.N.; Graf, A.N.; Krzak, J.; Flanagan, A.; Hassani, S.; Caudill, A.K.; Dietz, F.R.; Morcuende, J.; Harris, G.F. Long-Term Results of Comprehensive Clubfoot Release versus the Ponseti Method: Which Is Better? Clin. Orthop. Relat. Res. 2014, 472, 1281–1290. [Google Scholar] [CrossRef]
- Mindler, G.T.; Kranzl, A.; Lipkowski, C.A.M.; Ganger, R.; Radler, C. Results of Gait Analysis Including the Oxford Foot Model in Children with Clubfoot Treated with the Ponseti Method. J. Bone Jt. Surg. 2014, 96, 1593–1599. [Google Scholar] [CrossRef]
- Manousaki, E.; Czuba, T.; Hägglund, G.; Mattsson, L.; Andriesse, H. Evaluation of Gait, Relapse and Compliance in Clubfoot Treatment with Custom-Made Orthoses. Gait Posture 2016, 50, 8–13. [Google Scholar] [CrossRef]
- Lööf, E.; Andriesse, H.; André, M.; Böhm, S.; Broström, E.W. Gait in 5-Year-Old Children with Idiopathic Clubfoot: A Cohort Study of 59 Children, Focusing on Foot Involvement and the Contralateral Foot. Acta Orthop. 2016, 87, 522–528. [Google Scholar] [CrossRef]
- Jeans, K.A.; Karol, L.A.; Erdman, A.L.; Stevens, W.R. Functional Outcomes Following Treatment for Clubfoot Ten-Year Follow-Up. J. Bone Jt. Surg. 2018, 100, 2015–2023. [Google Scholar] [CrossRef]
- Manousaki, E.; Esbjörnsson, A.C.; Mattsson, L.; Andriesse, H. Correlations between the Gait Profile Score and Standard Clinical Outcome Measures in Children with Idiopathic Clubfoot. Gait Posture 2019, 71, 50–55. [Google Scholar] [CrossRef] [PubMed]
- Lööf, E.; Andriesse, H.; André, M.; Böhm, S.; Iversen, M.D.; Broström, E.W. Gross Motor Skills in Children with Idiopathic Clubfoot and the Association between Gross Motor Skills, Foot Involvement, Gait, and Foot Motion. J. Pediatr. Orthop. 2019, 39, 359–365. [Google Scholar] [CrossRef] [PubMed]
- Dimeglio, A.; Bensahel, H.; Souchet, P.; Mazeau, P.; Bonnet, F. Classification of Clubfoot. J. Pediatr. Orthop. B 1995, 4, 129–136. [Google Scholar] [CrossRef]
- Karol, L.A.; Jeans, K.A. This Is a Narrative Review of the Functional Evaluation of Clubfoot Treatment with Gait Analysis. Ann. Transl. Med. 2021, 9, 1105. [Google Scholar] [CrossRef] [PubMed]
- Perry, J.; Burnfield, J.M. Gait Analysis, Normal and Pathological Function; SLACK Incorporated, Ed.; National Library of Medicine: Bethesda, MD, USA, 2010. [Google Scholar]
- Gintautienė, J.; Čekanauskas, E.; Barauskas, V.; Žalinkevičius, R. Comparison of the Ponseti Method versus Early Tibialis Anterior Tendon Transfer for Idiopathic Clubfoot: A Prospective Randomized Study. Medicina 2016, 52, 163–170. [Google Scholar] [CrossRef]
- Theologis, T.N.; Harrington, M.E.; Thompson, N.; Benson, M.K.D. Dynamic Foot Movement in Children Treated for Congenital Talipes Equinovarus. J. Bone Jt. Surg. 2003, 85, 572–577. [Google Scholar] [CrossRef] [PubMed]
- Sankar, W.N.; Rethlefsen, S.A.; Weiss, J.; Kay, R.M. The Recurrent Clubfoot: Can Gait Analysis Help Us Make Better Preoperative Decisions? Clin. Orthop. Relat. Res. 2009, 467, 1214–1222. [Google Scholar] [CrossRef]
- McCahill, J.; Stebbins, J.; Koning, B.; Harlaar, J.; Theologis, T. Repeatability of the Oxford Foot Model in Children with Foot Deformity. Gait Posture 2018, 61, 86–89. [Google Scholar] [CrossRef]
- Baker, R.; McGinley, J.L.; Schwartz, M.H.; Beynon, S.; Rozumalski, A.; Graham, H.K.; Tirosh, O. The Gait Profile Score and Movement Analysis Profile. Gait Posture 2009, 30, 265–269. [Google Scholar] [CrossRef]
- Schwartz, M.H.; Rozumalski, A. The Gait Deviation Index: A New Comprehensive Index of Gait Pathology. Gait Posture 2008, 28, 351–357. [Google Scholar] [CrossRef]
- McCahill, J.; Stebbins, J.; Lewis, A.; Prescott, R.; Harlaar, J.; Theologis, T. Validation of the Foot Profile Score. Gait Posture 2019, 71, 120–125. [Google Scholar] [CrossRef] [PubMed]
- Dobbs, M.B.; Nunley, R.; Schoenecker, P.L. Long-Term Follow-up of Patients with Clubfeet Treated with Extensive Soft-Tissue Release. J. Bone Jt. Surg. 2006, 88, 986–996. [Google Scholar] [CrossRef]
- Stouten, J.H.; Besselaar, A.T.; Van Der Steen, M.C. Identification and Treatment of Residual and Relapsed Idiopathic Clubfoot in 88 Children. Acta Orthop. 2018, 89, 448–453. [Google Scholar] [CrossRef] [PubMed]
- Ponseti, I.V. Relapsing Clubfoot: Causes, Prevention, and Treatment. Iowa Orthop. J. 2002, 22, 55–56. [Google Scholar]
- Dietz, F.R. Treatment of a Recurrent Clubfoot Deformity after Initial Correction with the Ponseti Technique. Instr. Course Lect. 2006, 55, 625–629. [Google Scholar]
- Jeans, K.A.; Erdman, A.L.; Jo, C.-H.H.; Karol, L.A. A Longitudinal Review of Gait Following Treatment for Idiopathic Clubfoot: Gait Analysis at 2 and 5 Years of Age. J. Pediatr. Orthop. 2016, 36, 565–571. [Google Scholar] [CrossRef]
- Liu, Y.-B.; Jiang, S.-Y.; Zhao, L.; Yu, Y.; Zhao, D.-H. Can Repeated Ponseti Management for Relapsed Clubfeet Produce the Outcome Comparable with the Case Without Relapse? A Clinical Study in Term of Gait Analysis. J. Pediatr. Orthop. 2020, 40, 29–35. [Google Scholar] [CrossRef]
- Gray, K.; Gibbons, P.; Little, D.; Burns, J. Bilateral Clubfeet Are Highly Correlated: A Cautionary Tale for Researchers. Clin. Orthop. Relat. Res. 2014, 472, 3517–3522. [Google Scholar] [CrossRef]




| Study | Treatment | N (feet) | Gender | Mean Age in Years (Range) or ± SD | N TATT | N Additional Treatment | Marker Position | Dimeglio Scale 1 |
|---|---|---|---|---|---|---|---|---|
| Karol 2009 [24] | Ponseti | - (34 feet) | - | 5 | 2 | - | 12.8 (10–15) a | |
| Control | - (17) | - | 5 | |||||
| Church 2012 [25] | Ponseti | 22 (35 feet) 3 | 9M | 6.3 ± 1.4 (5.0–10.0) | 1 subject | Multi-segment foot model and single-segment marker set | 4.0 (3.0) b | |
| Control | 34 | - | - (4.0–17.0) | |||||
| Duffy 2012 [36] | Ponseti | 29 (42 feet) | 20M | 6.5 (5.0–8.0) | 14 feet | 4 subjects | - | - |
| Control | 26 (50 feet) | 17M | 7.9 (5.2–10.8) | |||||
| Smith 2014 [37] | Ponseti | 18 (29 feet) | 9M | 29.2 ± 5.6 | 10 feet | 6 feet | Milwaukee foot model | - |
| Control | 48 | 29M | 23.2 ± 2.4 | |||||
| Mindler 2014 [38] | Ponseti | 32 (50 feet) | 22M | 6.0 (3.0–8.0) | 5 feet | Cleveland model and Oxford foot model | - | |
| Control | 15 (30 feet) | 9M | 6.0 (3.0–9.0) | |||||
| Manousaki 2016 [39] | Ponseti | 20 (30 feet) | 17M | 7 ± 3.4 months | 3 feet | 3 feet | Plug in gait model including seven markers on the torso | 11 (9–13) c |
| Control | 16 | 8.5 (6.1–12) 4 | ||||||
| Lööf 2016 [40] | Ponseti | 59 (89 feet) | 41M | 5.4 ± 0.5 | 3 feet | Plug in gait model | 16 moderated, 48 severed, 24 very severed d | |
| Control | 28 (56 feet) | 18M | 5.5 ± 0.6 | |||||
| Jeans 2018 [41] | Ponseti | 50 (75 feet) | - | 10 | Plug in gait model | 13.4 ± 1.9 | ||
| Control | 20 (40 feet) | - | 10 | |||||
| Manousaki 2019 [42] | Ponseti | 20 (20 feet) | 17M | 7 ± 3.4 months | 3 feet | Plug in gait model | - | |
| Control | 16 (32 feet) | 8.5 (6.1–12.0) 4 | ||||||
| Loof 2019 [43] | Ponseti | 47 (69 feet) | 35M | 5.4 (0.5) | 3 feet | Plug in gait model | 15 moderated, 36 severed 17 very severed d | |
| Control | 28 (56 feet) | 18M | 5.5 (0.6) | |||||
| Dussa 2020 [26] | Ponseti overcorrected | 14 | - | 9.9 (1.5) | Plug in gait model and Oxford foot model | - | ||
| Control | 25 | - | 9.9 (2.7) | |||||
| Ferrando 2020 [27] | Ponseti Control | 22 (34 feet) 25 (50 feet) | 14M 18M | 8 ± 1 9 ± 2 | 11 feet | 5 feet | - | - |
| McCahill 2020 [28] | Ponseti relapse | 31 | 24M | 8.3 (5–16) | 10 subjects | Oxford foot model | - | |
| Control | 30 | 21M | 10.7 (5–16) | |||||
| Mindler 2020 [29] | Ponseti relapse | 17 (25 feet) | 11M | 6.8 (5.1–9.1) | Cleveland model and Oxford foot model | - | ||
| Control | 18 (36 feet) | 6M | 6 (4–9) | |||||
| Grin 2021 [30] | Ponseti | 11 | 9M | 5.6 ± 1.6 | Extended Helen Hayes and Oxford foot model | - | ||
| Ponseti relapse | 11 | 8M | 5.7 ± 1.5 | |||||
| Control | 15 | 8M | 5.7 ± 1.4 | |||||
| Li 2021 [31] | Ponseti relapse | 17 (24 feet) | 12M | 6.34 ± 1.65 (4.47–10.2) | Helen Hayes model | - | ||
| Control | 16 | M:F = 1.14:1 | 7.12 ± 2.23 | |||||
| Recordon 2021 [32] | Ponseti | 16 (23 feet) | - | 15 (13–17) | 5 | 5 | - | 5.8 ± 1.7 |
| Control | 39 (78 feet) | - | Age-matched | |||||
| Brierty 2022 [35] | Ponseti relapse | 16 (23 feet) | 13M | 5.58 (3.27–8.57) | Plug in gait model and Oxford foot model | - | ||
| Control | 9 | - | 6.31 (4.47–7.96) | |||||
| Grin 2022 [33] | Ponseti | 18 | 18M | 5.39 ± 1.46 | Extended Helen Hayes and Oxford foot model | - | ||
| Ponseti relapse | 13 | 8M | 5.46 ± 1.51 | |||||
| Control | 21 | 12M | 6 ± 1.57 | |||||
| Wijnands 2022 [34] | Ponseti | 15 | 12M | 5.13 ± 1.25 | Extended Helen Hayes and Oxford foot model | - | ||
| Ponseti relapse | 10 | 6M | 5.70 ± 1.57 | |||||
| Control | 19 | 11M | 5.79 ± 1.40 |
| Outcome Measure | Moment in Gait Cycle | Studies | Significance | |
|---|---|---|---|---|
| Foot | Mean tibial torsion (EXT) Foot progression (EXT) | Stance Preswing | [25] [37] | Clubfoot < controls Clubfoot > controls |
| Forefoot vs. hindfoot | ROM sagittal (DF/PF) Plantarflexion | Gait cycle 20% gait cycle 1 | [30,38] [37] | Conflicting outcome 2 Clubfoot < controls |
| Forefoot vs. tibia | ROM sagittal (DF/PF) ROM frontal (PRO/SUP) ROM transversal (AB/AD) | Gait cycle Gait cycle Gait cycle | [30,38] [30,38] [30,38] | Conflicting outcome 2 Conflicting outcome 2 Conflicting outcome 2 |
| Ankle | Dorsiflexion Max. plantarflexion Dorsiflexion | Mid-stance Terminal stance Swing 1 | [24,39] [40] [30,37] | Conflicting outcome 2 Clubfoot < controls Conflicting outcome 2 |
| Knee | Max. extension Max. extension Max. flexion | Mid-stance 2nd half of stance Swing | [36] [38] [30,38] | Clubfoot < controls Clubfoot < controls Conflicting outcome 2 |
| Hip | Mean abduction Max. rotation (EXT) Mean rotation (EXT) | Gait cycle Gait cycle Mid-stance | [38] [30,38] [36] | Clubfoot > controls Conflicting outcome 2 Clubfoot > controls |
| Total gait scores | GDI | Gait cycle | [36,39,43] | Clubfoot < controls |
| Outcome Measure | Moment in Gait Cycle | Studies | Significance | |
|---|---|---|---|---|
| Foot | Shank-based foot rotation (INT) Foot progression angle (EXT) Foot progression angle (EXT) Shank-based foot rotation (INT) | Stance Stance 70% gait cycle 1 Swing | [30] [29] [35] [30] | Relapse > controls Relapse < controls Relapse < controls Relapse > controls |
| Hindfoot vs. tibia | Mean adduction ROM sagittal (DF/PF) ROM transversal (INT/EXT) Inversion Adduction Dorsiflexion Max. dorsiflexion Mean adduction | Gait cycle Gait cycle Gait cycle Gait cycle 1 Gait cycle 1 Initial contact Stance Stance | [28] [28,29,30] [28,29,30] [35] [35] [29,30] [29,30] [29,30] | Relapse > controls Conflicting outcome 2 Conflicting outcome 2 Relapse > controls Relapse > controls Conflicting outcome 2 Conflicting outcome 2 Conflicting outcome 2 |
| Forefoot vs. hindfoot | ROM sagittal (DF/PF) ROM frontal (PRO/SUP) Max. plantarflexion Adduction Dorsiflexion Max. dorsiflexion Mean adduction Adduction Max. dorsiflexion Supination | Gait cycle Gait cycle Gait cycle Gait cycle1 Initial contact Stance Stance Toe-off Swing 80% gait cycle | [28,29,30] [28,29,30] [29,30] [35] [29,30] [29,30] [29,30] [30] [29,30] [29] | Conflicting outcome 2 Conflicting outcome 2 Conflicting outcome 2 Relapse > controls Conflicting outcome 2 Conflicting outcome 2 Conflicting outcome 2 Relapse > controls Conflicting outcome 2 Relapse > controls |
| Forefoot vs. tibia | ROM sagittal (DF/PF) ROM transversal (AB/AD) Max. plantarflexion Mean adduction Adduction Supination Mean adduction Plantarflexion Mean adduction Mean supination/pronation Dorsiflexion Adduction | Gait cycle Gait cycle Gait cycle Gait cycle Initial contact Initial contact Stance Toe-off Swing Swing 80% gait cycle 80% gait cycle | [29,30] [29,30] [29,30] [28] [29] [29] [29,30] [30] [29,30] [29,30] [29] [29] | Conflicting outcome 2 Conflicting outcome 2 Conflicting outcome 2 Relapse > controls Relapse > controls Relapse > controls Relapse > controls Relapse < controls Conflicting outcome 2 Conflicting outcome 2 Relapse > controls Relapse > controls |
| Ankle | ROM sagittal (PF/DF) Max. dorsiflexion Plantarflexion | Gait cycle Gait cycle Toe-off | [29,30] [29,34] [30] | Relapse < controls Conflicting outcome 2 Relapse < controls |
| Knee | Mean rotation (EXT) Flexion | Stance End of swing 1 | [29] [35] | Relapse < controls Relapse > control |
| Hip | Mean rotation (INT) External rotation Abduction | Stance 30–60% gait cycle 1 50–90% gait cycle 1 | [29,30] [35] [35] | Conflicting outcome 2 Relapse > controls Relapse > controls |
| Total gait scores | GDI GDI* cFDI* Foot profile score FVS hindfoot sagittal FVS hindfoot frontal FVS hindfoot transversal FVS forefoot sagittal FVS forefoot transversal | Gait cycle Gait cycle Gait cycle Gait cycle Gait cycle Gait cycle Gait cycle Gait cycle Gait cycle | [31] [33] [33] [28] [28] [28] [28] [28] [28] | Deviated from normal 3 Deviated from normal 3 Deviated from normal 3 Relapse > controls Relapse > controls Relapse > controls Relapse > controls Relapse > controls Relapse > controls |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Grin, L.; van Oorschot, L.; Vanwanseele, B.; Wijnands, S.D.N.; Kars, H.J.J.; Besselaar, A.T.; van der Steen, M.C. Kinematic Gait Impairments in Children with Clubfeet Treated by the Ponseti Method: A Systematic Review and Meta-Analysis. Children 2023, 10, 785. https://doi.org/10.3390/children10050785
Grin L, van Oorschot L, Vanwanseele B, Wijnands SDN, Kars HJJ, Besselaar AT, van der Steen MC. Kinematic Gait Impairments in Children with Clubfeet Treated by the Ponseti Method: A Systematic Review and Meta-Analysis. Children. 2023; 10(5):785. https://doi.org/10.3390/children10050785
Chicago/Turabian StyleGrin, Lianne, Lisa van Oorschot, Benedicte Vanwanseele, Saskia D. N. Wijnands, H. J. J. (Cojanne) Kars, Arnold T. Besselaar, and M. C. (Marieke) van der Steen. 2023. "Kinematic Gait Impairments in Children with Clubfeet Treated by the Ponseti Method: A Systematic Review and Meta-Analysis" Children 10, no. 5: 785. https://doi.org/10.3390/children10050785
APA StyleGrin, L., van Oorschot, L., Vanwanseele, B., Wijnands, S. D. N., Kars, H. J. J., Besselaar, A. T., & van der Steen, M. C. (2023). Kinematic Gait Impairments in Children with Clubfeet Treated by the Ponseti Method: A Systematic Review and Meta-Analysis. Children, 10(5), 785. https://doi.org/10.3390/children10050785