
Cardiac Arrhythmias Requiring Electric Countershock during the Neonatal Period—A Systematic Review

 , ,
, ,  ,
, Highlights
- Electric countershock therapy is an effective alternative to drug therapy for neonatal arrhythmias.
- Electric countershock therapy has shown excellent outcomes, particularly in cases of atrial flutter, during the neonatal period.
- Atrial flutter is the most common arrhythmia in neonates requiring electric countershock therapy.
- Synchronized cardioversion is the main type of electric countershock therapy used in neonates.
Abstract
1. Introduction
2. Materials and Methods
2.1. Search Strategy and Inclusion Criteria
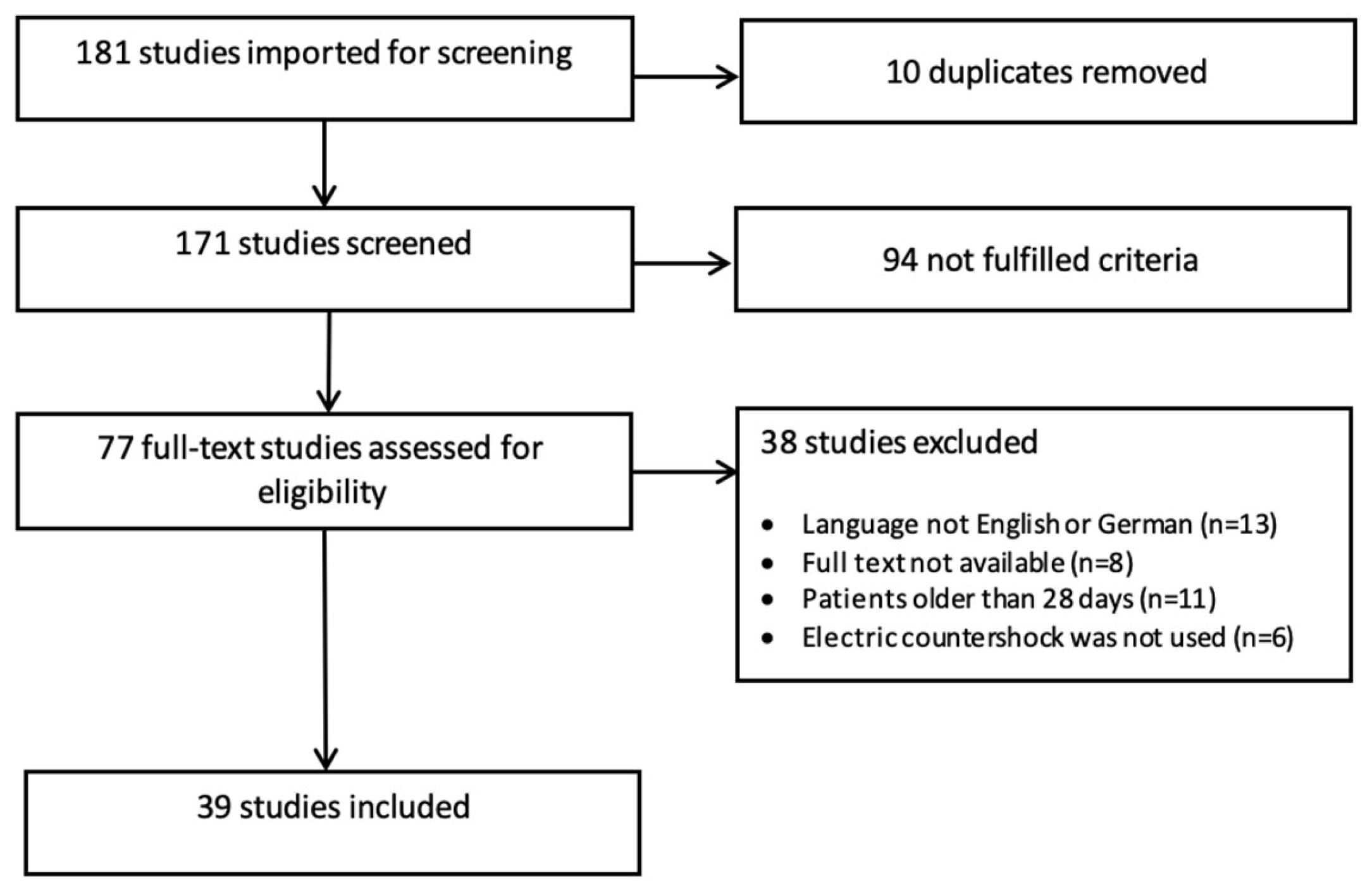
2.2. Study Selection
2.3. Data Extraction and Charting
3. Results
3.1. Gestational Age and Gender Distribution
3.2. Age at Electric Countershock
3.3. Congenital Heart Disease
3.4. Arrhythmias
3.5. Type of Electric Countershock

{kind=link}
{kind=link}
{kind=link}
| Publication | Year | Study Design | Patient(-s) (n = ) | Age at ES (Days) | Congenital Heart Defect | Gestational Age (Weeks) | ECG Diagnosis (n = ) | Arrhythmia Prenatally Detected | Medication before ES (n = ) | Success | Energy Level | Recurrence during Follow-Up (n = ) |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Barclay et al. [39] | 1972 | Case report | 1 | 10 | ASD | ≥37 | AFL | No | Digoxin | CV: yes | n/a | No |
| Heinonen et al. [18] | 1992 | Case report | 1 | 0 | No | ≥37 | VT | No | No | CV: yes | 1 J/kg | No |
| Casey et al. [34] | 1997 | Retrospective study | 18 | 0–30 | n/a | 30–38 | AFL (n = 16) SVT (n = 2) | Yes (n = 3) | Digoxin (n = 16) | CV: n = 16 TEP: n = 2 | n/a | No (n = 18) |
| Allegaert et al. [17] | 2002 | Case report | 1 | 0 | No | 38 + 0 | AFL | Yes | No | CV: yes | 1 × 1 J/kg 1 × 1.5 J/kg | No |
| Cornwell et al. [16] | 2005 | Case report | 2 | 0 | No | 34–40 | AFL (n = 2) | Yes (n = 2) | Adenosine (n = 2) | CV: yes (n = 2) | 1 J/kg 2 J/kg | No (n = 2) |
| Ceresnak et al. [35] | 2009 | Retrospective study | 6 | 0–14 | TGA (n = 1) pulmonary atresia + intact IVS (n = 1) | 34–40 | AFL (n = 6) | Yes (n = 4) | No | CV: yes | 1 J/kg | Yes n = 2 |
| Silva et al. [40] | 2010 | Case report | 1 | 14 | No | ≥37 | SVT | No | No | CV: yes | 1 J/kg | No |
| Gulletta et al. [15] | 2011 | Case report | 1 | 0 | n/a | ≥37 | AFL | Yes | Adenosine Propafenone | CV: yes | 1 J/kg | No |
| Rein et al. [24] | 1986 | Case report | 1 | 0 | No | 33 | SVT | No | Digoxin | CV: yes | 3 J/kg | Yes |
| Lisowski et al. [7] | 1999 | Retrospective study | 9 | 0 | n/a | 34–40 | AFL (n = 9) | Yes (n = 9) | Yes | CV: yes (n = 9) | n/a | n/a (n = 9) |
| Paech et al. [21] | 2001 | Case report | 1 | 0 | No | ≥37 | TdP | No | no | CV: yes | 2 J/kg | No |
| Sinha et al. [25] | 2005 | Case report | 1 | 0 | No | ≥37 | AFL | No | no | CV: yes | 2 × 0.5 J/kg 1 × 1 J/kg | No |
| Konak et al. [19] | 2013 | Case report | 1 | 0 | Pulmonary hypertension | 34 + 0 | AFL | No | Adenosine Amiodarone | CV: yes | 1.4 J/kg | Yes |
| Nijres et al. [20] | 2015 | Case report | 1 | 0 | Pulmonary hypertension | ≥37 | SVT | Yes | Adenosine | CV: yes | 2 J/kg | Yes |
| Poryo et al. [22] | 2017 | Case report | 1 | 0 | Hypertrophic cardiomyopathy | 34 + 3 | AFL | Yes | Adenosine | CV yes | 1.4 J/kg | No |
| Apostolidou et al. [23] | 2018 | Case report | 1 | 0 | No | ≥37 | AFL | Yes | Adenosine | CV: yes | 1 × 1 J/kg 2 × 1.5 J/kg | No |
| Theodorou et al. [41] | 2003 | Case report | 1 | 10 | Truncus arteriosus | ≥37 | VF | No | No | DF: no | 1 × 3 J/kg 5 × 6 J/kg | Died |
| Umeh et al. [13] | 2017 | Case report | 1 | 0 | no | 25 + 2 | AF | No | Adenosine | CV: yes | 1 J/kg | No |
| Vintzileos et al. [26] | 1986 | Case report | 1 | 0 | no | 33 | AFL | Yes | Digoxin | CV: yes | 1.7 J/kg | Died |
| Hassenrück et al. [27] | 1965 | Case report | 1 | 0 | no | 36 | AFL | No | Digoxin | CV: yes | n/a | No |
| Liberman et al. [42] | 2006 | Prospective study | 1 | 14 | no | n/a | AFL | No | n/a | CV: yes | 0.5 J/kg | No |
| Mehta et al. [36] | 1993 | Retrospective study | 3 | 0–4 | Interrupted arch + VSD (n = 1) | n/a | AFL (n = 3) | No | Digoxin (n = 3) | CV: yes (n = 3) | 0.25 J/kg | n/a (n = 3) |
| Miyake et al. [11] | 2013 | Retrospective study | 1 | 14 | no | n/a | VF | No | n/a | DF: yes | n/a | Yes |
| Peng et al. [46] | 1998 | Retrospective study | 2 | 1–3 | No | ≥37 | AFL (n = 2) | No | No | CV: yes (n = 2) | n/a | No (n = 2) |
| Roumiantsev et al. [47] | 2017 | Retrospective study | 1 | 2 | No | 36 + 3 | AFL | No | Adenosine Esmolol | CV: yes | 0.5 J/kg | No |
| Saidi et al. [43] | 1998 | Case report | 1 | 9 | No | ≥37 | VT | No | Adenosine Amiodarone Lidocaine | CV: yes | 2 × 1.5 J/kg 1 × 1.5 J/kg | Yes |
| Singh et al. [44] | 1989 | Case report | 1 | 24 | No | ≥37 | SVT | No | No | CV: yes | 20 J * | Yes |
| Sugrue et al. [45] | 1985 | Case report | 2 | 9–21 | No | ≥37 | SVT (n = 2) | No | No | CV: yes (n = 2) | 2 J/kg | Yes (n = 2) |
| Suzumura et al. [28] | 2004 | Case report | 1 | 0 | No | ≥37 | AFL | Yes | No | TEP: no CV: no | 2 J/kg | No |
| Takei et al. [29] | 2015 | Case report | 1 | 0 | No | 37 + 0 | AFL | Yes | No | CV: yes | n/a | No |
| Texter et al. [8] | 2006 | Retrospective study | 20 | 0–11 | No | ≥37 | AFL (n = 20) | Yes (n = 3) | No | CV (n = 20) TEP (n = 7) | n/a | Yes (n = 5) |
| Tunca Sahin et al. [14] | 2021 | Retrospective study | 6 | 0 | Ebstein (n = 1) | 28–41 | AFL (n = 6) | Yes (n = 6) | No | CV: yes (n = 6) | n/a | Yes (n = 4) |
| Wells et al. [30] | 1987 | Case report | 1 | 0 | No | ≥37 | SVT | No | No | CV: yes | 5 J/kg | No |
| Wójtowicz-Marzec et al. [31] | 2020 | Case report | 1 | 0 | No | 34 + 0 | AFL | No | Adenosine | CV: yes | 1 J/kg | No |
| Yilmaz-Semerci et al. [32] | 2018 | Case report | 3 | 0 | no | 34–38 | AFL (n = 2) SVT (n = 1) | Yes (n = 1) | Propanolol (n = 2) Adenosine (n = 1) | CV: yes (n = 3) | 1 J/kg | Yes (n = 3) |
| Tejman-Yarden et al. [12] | 2017 | Case report | 1 | 14 | no | ≥37 | VT | No | No | DF: yes | 60 J/kg | No |
| Tibballs et al. [37] | 2011 | Prospective observation Study | 5 | <30 | n/a | n/a | VT VF | n/a | n/a | DF: yes (n = 5) | 0.5–3 J/kg | n/a (n = 5) |
| Dick et al. [38] | 1988 | Retrospective study | 10 | <30 | TGA UVH | n/a | AFL SVT | n/a | n/a | TEP: yes (n = 10) | n/a | n/a (n = 10) |
| Mileder et al. [33] | 2021 | Case report | 1 | 0 | no | ≥37 | VT | No | Epinephrine Calcium Magnesium | DF: yes | 1.4 J/kg | No |
3.6. Energy Levels for Electric Countershock
3.7. Outcome and Recurrence
4. Discussion
5. Conclusions
6. Limitation
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Badrawi, N.; Hegazy, R.A.; Tokovic, E.; Lotfy, W.; Mahmoud, F.; Aly, H. Arrhythmia in the neonatal intensive care unit. Pediatr. Cardiol. 2009, 30, 325–330. [Google Scholar] [CrossRef]
- Dawson, J.; Kamlin, C.O.F.; Wong, C.; Pas, A.T.; Vento, M.; Cole, T.; Donath, S.; Hooper, S.B.; Davis, P.G.; Morley, C. Changes in heart rate in the first minutes after birth. Arch. Dis. Child. Fetal Neonatal Ed. 2010, 95, F177–F181. [Google Scholar] [CrossRef]
- Jaeggi, E.; Öhman, A. Fetal and Neonatal Arrhythmias. Clin. Perinatol. 2016, 43, 99–112. [Google Scholar] [CrossRef]
- Jaeggi, E.T.; Carvalho, J.S.; De Groot, E.; Api, O.; Clur, S.-A.B.; Rammeloo, L.; McCrindle, B.W.; Ryan, G.; Manlhiot, C.; Blom, N.A. Comparison of Transplacental Treatment of Fetal Supraventricular Tachyarrhythmias with Digoxin, Flecainide, and Sotalol. Circulation 2011, 124, 1747–1754. [Google Scholar] [CrossRef]
- Huang, Y.; He, Q.; Yang, L.J.; Liu, G.J.; Jones, A. Cardiopulmonary resuscitation (CPR) plus delayed defibrillation versus immediate defibrillation for out-of-hospital cardiac arrest. Cochrane Database Syst. Rev. 2014, 2014, CD009803. [Google Scholar] [CrossRef]
- Prasad, D.; Steinberg, J.; Snyder, C. Cost-effectiveness of digoxin, pacing, and direct current cardioversion for conversion of atrial flutter in neonates. Cardiol. Young 2018, 28, 725–729. [Google Scholar] [CrossRef]
- Lisowski, L.A.; Verheijen, P.M.; Benatar, A.A.; Soyeur, D.J.G.; Stoutenbeek, P.; Brenner, J.I.; Kleinman, C.S.; Meijboom, E.J. Atrial Flutter in the Perinatal Age Group: Diagnosis, Management and Outcome. J. Am. Coll. Cardiol. 2000, 35, 771–777. [Google Scholar] [CrossRef] [PubMed]
- Texter, K.M.; Kertesz, N.J.; Friedman, R.A.; Fenrich, A.L. Atrial Flutter in Infants. J. Am. Coll. Cardiol. 2006, 48, 1040–1046. [Google Scholar] [CrossRef] [PubMed]
- Dunnigan, A.; Benson, W.; Benditt, D.G. Atrial flutter in infancy: Diagnosis, clinical features, and treatment. Pediatrics 1985, 75, 725–729. [Google Scholar] [CrossRef] [PubMed]
- Saudi, A.; Sucu, M.; Davutoglu, V.; Ozer, O. Electrical cardioversion. Ann. Saudi Med. 2009, 29, 201–206. [Google Scholar]
- Miyake, C.Y.; Davis, A.M.; Motonaga, K.S.; Dubin, A.M.; Berul, C.I.; Cecchin, F. Infant ventricular fibrillation after ST-segment changes and QRS widening: A new cause of sudden infant death? Circ. Arrhythm. Electrophysiol. 2013, 6, 712–718. [Google Scholar] [CrossRef]
- Tejman-Yarden, S.; Katz, U.; Rubinstein, M.; Attias, Y.; Yahia, R.; Mishali, D.; Glikson, M. Inappropriate Shocks and Power Delivery Using Adult Automatic External Defibrillator Pads in a Pediatric Patient. Pediatr. Emerg. Care 2021, 37, e1708–e1710. [Google Scholar] [CrossRef] [PubMed]
- Umeh, M.; Klutse, T.; Richards, J.; Kulkarni, A. Electrical direct current cardioversion for the treatment of atrial flutter in extremely premature neonate. Arch. Dis. Child. Fetal Neonatal Ed. 2017, 102, F466–F467. [Google Scholar] [CrossRef] [PubMed]
- Tunca Sahin, G.; Lewis, M.; Uzun, O. Association of Fetal Atrial Flutter with Neonatal Atrioventricular Re-entry Tachycardia Involving Accessory Pathway: A Link to be Remembered. Pediatr. Cardiol. 2021, 42, 849–856. [Google Scholar] [CrossRef]
- Gulletta, S.; Rovelli, R.; Fiori, R.; Bella, P.D. Multiple external electrical cardioversions for refractory neonatal atrial flutter. Pediatr. Cardiol. 2012, 33, 354–356. [Google Scholar] [CrossRef]
- Cornwell, L.; Mukherjee, R.; Kelsall, A.W.R. Problems with the use of self-adhesive electrode pads in neonates. Resuscitation 2006, 68, 425–428. [Google Scholar] [CrossRef]
- Allegaert, M.D.K.; Naulaers, M.D.G.; Devlieger, M.D.H. The use of methohexital during neonatal cardioversion. Paediatr. Anaesth. 2002, 12, 371–373. [Google Scholar] [CrossRef]
- Heinonen, K.M. Rare procedures during delivery room resuscitation—Cardioversion of ventricular tachycardia in an asphyctic neonate. Intensive Care Med. 1992, 18, 491–492. [Google Scholar] [CrossRef] [PubMed]
- Konak, M.; Alp, H.; Tarakçı, N.; Baysal, T.; Örs, R. Successful treatment of atrial flutter with propafenone and synchronized cardioversion in a newborn. Indian J. Pediatr. 2014, 81, 413–414. [Google Scholar] [CrossRef]
- Mohammad Nijres, B.; Cummings, S.; Rodriguez, A.M.; Morales, L. Term Infant with Fetal Tachyarrhythmia, Hydrops, and Persistent Pulmonary Hypertension. Indian J. Pediatr. 2015, 82, 1069–1070. [Google Scholar] [CrossRef]
- Paech, C.; Suchowerskyj, P.; Gebauer, R.A. Successful treatment of a newborn with genetically confirmed long QT syndrome 3 and repetitive Torsades de Pointes tachycardia. Pediatr. Cardiol. 2011, 32, 1060–1061. [Google Scholar] [CrossRef] [PubMed]
- Poryo, M.; Löffler, G.; Abedini, M. Sawtooth Waves-Atrial Flutter in a Premature Infant. Dtsch. Arztebl. Int. 2017, 114, 262. [Google Scholar] [CrossRef] [PubMed]
- Apostolidou, S.; Stute, F.; Tavares-de-Sousa, M.; Hecher, K.; Arndt, F.; Rkozlik-Feldmann, R.; Singer, D. Erfolgreiche Kardioversion bei neonatalem Vorhofflattern. Z. Geburtshilfe Neonatol. 2018, 222, 169–170. [Google Scholar] [CrossRef] [PubMed]
- Rein, A.J.J.T.; Lotan, C.; Goiten, K.J.; Simcha, A. Severe hydrops fetalis due to congenital supraventricular tachycardia. Eur. J. Pediatr. 1986, 144, 511–512. [Google Scholar] [CrossRef] [PubMed]
- Sinha, A.; Fernandes, C.J.; Kim, J.J.; Fenrich, A.L.; Enciso, J. Atrial flutter following placement of an umbilical venous catheter. Am. J. Perinatol. 2005, 22, 275–277. [Google Scholar] [CrossRef] [PubMed]
- Vintzileos, A.M.; Campbell, W.A.; Sobermann, S.M.; Nochimson, D.J. Fetal atrial flutter and X-linked dominant vitamin D-resistant rickets. Obs. Gynecol. 1985, 65 (Suppl. 3), 39S–44S. [Google Scholar]
- Hassenrück, A.; Chojnacki, B.; Barker, H.J. Direct Current Cardioversion in a Case of Congential Atrial Flutter. Am. J. Cardiol. 1965, 15, 726–731. [Google Scholar] [CrossRef]
- Suzumura, H.; Nitta, A.; Ono, M.; Arisaka, O. Neonatal Intractable Atrial Flutter Successfully Treated with Intravenous Flecainide. Pediatr. Cardiol. 2004, 25, 154–156. [Google Scholar] [CrossRef]
- Takei, K.; Morikawa, M.; Cho, K.; Minakami, H. Resolution of tachyarrhythmia-related fetal hydrops after corticosteroid administration for fetal lung maturation. BMJ Case Rep. 2015, 2015, bcr2015211948. [Google Scholar] [CrossRef]
- David Wells, L.H.; Usnr, M.; Shaw, L.G.G.; McNeal, L.R.M.; Ronlov, L.C.S.; Usn, M. Neonatal paroxysmal supraventricular tachycardia. The importance of recognition by fetal ECG and of treatment with DC cardioversion. Clin. Pediatr. 1978, 17, 581–583. [Google Scholar] [CrossRef] [PubMed]
- Wójtowicz-Marzec, M.; Wysokińska, B.; Respondek-Liberska, M. Successful treatment of neonatal atrial flutter by synchronized cardioversion: Case report and literature review. BMC Pediatr. 2020, 20, 370. [Google Scholar] [CrossRef]
- Yılmaz-Semerci, S.; Bornaun, H.; Kurnaz, D.; Cebeci, B.; Babayigit, A.; Büyükkale, G.; Çetinkaya, M. Neonatal atrial flutter: Three cases and review of the literature. Turk. J. Pediatr. 2018, 60, 306–309. [Google Scholar] [CrossRef] [PubMed]
- Mileder, L.P.; Morris, N.M.; Kurath-Koller, S.; Pansy, J.; Pichler, G.; Pocivalnik, M.; Schwaberger, B.; Burmas, A.; Urlesberger, B. Successful postnatal cardiopulmonary resuscitation due to defibrillation. Children 2021, 8, 421. [Google Scholar] [CrossRef]
- Casey, F.A.; Mccrindle, B.W.; Hamilton, R.M.; Gow, R.M.; Toronto, C. Neonatal atrial flutter: Significant early morbidity and excellent long-term prognosis. Am. Heart J. 1997, 133, 302–306. [Google Scholar] [CrossRef]
- Ceresnak, S.R.; Starc, T.J.; Hordof, A.J.; Pass, R.H.; Bonney, W.J.; Liberman, L. Elevated impedance during cardioversion in neonates with atrial flutter. Pediatr. Cardiol. 2009, 30, 436–440. [Google Scholar] [CrossRef] [PubMed]
- Mehta, A.V.; Ewing, L.L. Pediatric Cardiology Atrial Tachycardia in Infants and Children: Electrocardiographic Classification and Its Significance. Pediatr. Cardiol. 1993, 14, 199–203. [Google Scholar] [CrossRef]
- Tibballs, J.; Carter, B.; Kiraly, N.J.; Ragg, P.; Clifford, M. External and internal biphasic direct current Shock dosis for pediatric ventricular fibrillation and pulseless ventricular tachycardia. Pediatr. Crit. Care Med. 2011, 12, 14–20. [Google Scholar] [CrossRef] [PubMed]
- Dick, M.I.; Scott, W.A.; Serwer, G.S.; Bromberg, B.I.; Beekman, R.H.; Rocchini, A.P.; Snider, A.R.; Crowley, D.C.; Rosenthal, A. Acute termination of supraventricular tachyarrhythmias in children by transesophageal atrial pacing. Am. J. Cardiol. 1988, 61, 925–927. [Google Scholar] [CrossRef]
- Barclay, R.P.C.; Barr, D.G.D. Direct Current Cardioversion in a Case of Congenital Atrial Flutter. Arch. Dis. Child. 1972, 47, 833–834. [Google Scholar] [CrossRef]
- Da Silva, P.S.L.; Waisberg, J. Induction of life-threatening supraventricular tachycardia during central venous catheter placement: An unusual complication. J. Pediatr. Surg. 2010, 45, E13–E16. [Google Scholar] [CrossRef]
- Theodorou, A.; Gutierrez, J.; Berg Robert, A. Fire Attributable to a Defibrillation Attempt in a Neonate. Pediatrics 2003, 112 Pt 1, 677–679. [Google Scholar] [CrossRef] [PubMed]
- Liberman, L.; Hordof, A.J.; Altmann, K.; Pass, R.H. Low Energy Biphasic Waveform Cardioversion of Atrial Arrhythmias in Pediatric Patients and Young Adults. Pacing Clin. Electrophysiol. 2006, 29, 1383–1386. [Google Scholar] [CrossRef]
- Saidi, A.S.; Friedman, B.R.A.; El Said, H.; Nuchtern, J.G.; Fenrich, A.L. Ventricular Tachycardia during Repair of Gastroschisis. Tex. Heart Inst. J. 1998, 25, 306–308. [Google Scholar]
- Singh, S.; Narang, A.; Bhakoo, O.N. DC Cardioversion of supraventricular Tachycardia in Neonate. Indian Pediatr. 1989, 26, 846–847. [Google Scholar] [PubMed]
- Sugrue, D.D.; Mclaran, C.; Hammill, S.C.; Gersh, B.J.; Mair, D.D.; Holmes, D.R. Refractory Supraventricular Tachycardia in the Neonate: Treatment with Temporary Antitachycardial Pacing. Mayo Clin. Proc. 1985, 60, 169–172. [Google Scholar] [CrossRef] [PubMed]
- Peng, C.C.; Chen, M.R.; Hou, C.J.; Hung, H.Y.; Kao, H.A.; Hsu, C.H.; Huang, F.Y. Atrial Flutter in the Neonate and Early Infancy. Jpn. Heart J. 1998, 39, 287–295. [Google Scholar] [CrossRef]
- Roumiantsev, S.; Doyle, S.M. Atrial Flutter in the Neonate: A case Study. Neonatal Netw. 2017, 36, 313–317. [Google Scholar] [CrossRef]
- Coleman, H.N.; Taylor, R.R.; Pool, P.E.; Whipple, G.H.; Covell, J.W.; Ross, J.; Braunwald, E. Congestive heart failure following chronic tachycardia. Am. Heart J. 1971, 81, 790–798. [Google Scholar] [CrossRef]
- Wacker-Gussmann, A.; Strasburger, J.F.; Cuneo, B.F.; Wakai, R.T. Diagnosis and treatment of fetal arrhythmia. Am. J. Perinatol. 2014, 31, 617–628. [Google Scholar] [CrossRef]
- Strasburger, J.F.; Eckstein, G.; Butler, M.; Noffke, P.; Wacker-Gussmann, A. Fetal Arrhythmia Diagnosis and Pharmacologic Management. J. Clin. Pharmacol. 2022, 62 (Suppl. 1), S53–S66. [Google Scholar] [CrossRef]
- Brugada, J.; Blom, N.; Sarquella-Brugada, G.; Blomstrom-Lundqvist, C.; Deanfield, J.; Janousek, J.; Abrams, D.; Bauersfeld, U.; Brugada, R.; Drago, F.; et al. Pharmacological and non-pharmacological therapy for arrhythmias in the pediatric population: EHRA and AEPC-Arrhythmia Working Group joint consensus statement. Europace 2013, 15, 1337–1382. [Google Scholar] [CrossRef]
- Schwartz, P.J.; Garson, A.; Paul, T.; Stramba-Badiale, M.; Vetter, V.L.; Villain, E.; Wren, C.; European Society of Cardiology. Guidelines for the interpretation of the neonatal electrocardiogram: A Task Force of the European Society of Cardiology. Eur. Heart J. 2002, 23, 1329–1344. [Google Scholar] [CrossRef] [PubMed]
- Moak, J.P. Supraventricular tachycardia in neonate and infand. Prog. Pediatr. Cardiol. 2000, 11, 25–38. [Google Scholar] [CrossRef] [PubMed]
- Van de Voorde, P.; Turner, N.M.; Djakow, J.; de Lucas, N.; Martinez-Mejias, A.; Biarent, D.; Bingham, R.; Brissaud, O.; Hoffman, F.; Johannesdottir, G.B.; et al. European Resuscitation Council Guidelines 2021: Paediatric Life Support. Resuscitation 2021, 161, 327–387. [Google Scholar] [CrossRef]
- Wyckoff, M.H.; Wyllie, J.; Aziz, K.; de Almeida, M.F.; Fabres, J.; Fawke, J.; Guinsburg, R.; Hosono, S.; Isayama, T.; Kapadia, V.S.; et al. Neonatal Life Support: 2020 International Consensus on Cardiopulmonary Resuscitation and Emergency Cardiovascular Care Science with Treatment Recommendations. Circulation 2020, 142, S185–S221. [Google Scholar] [CrossRef] [PubMed]
- Walker, T.C.; Renno, M.S.; Parra, D.A.; Guthrie, S.O. Neonatal ventricular fibrillation and an elusive ALCAPA: Things are not always as they seem. BMJ Case Rep. 2016, 2016, bcr2015214239. [Google Scholar] [CrossRef]
- Moore, J.A.; Stephens, S.B.; Kertesz, N.J.; Evans, D.L.; Kim, J.J.; Howard, T.S.; Pham, T.D.; Valdés, S.O.; de la Uz, C.M.; Raymond, T.T.; et al. Clinical Predictors of Recurrent Supraventricular Tachycardia in Infancy. J. Am. Coll. Cardiol. 2022, 80, 1159–1172. [Google Scholar] [CrossRef]
- Ratnasamy, C.; Rossique-Gonzalez, M.; Young, M.L. Pharmacological Therapy in Children with Atrioventricular Reentry: Which Drug? Curr. Pharm. Des. 2008, 14, 753–761. [Google Scholar] [CrossRef]
- Joye, R.; Beghetti, M.; Wacker, J.; Malaspinas, I.; Bouhabib, M.; Polito, A.; Bordessoule, A.; Shah, D. Early and Late Postoperative Tachyarrhythmias in Children and Young Adults Undergoing Congenital Heart Disease Surgery. Pediatr. Cardiol. 2023, 44, 312–324. [Google Scholar] [CrossRef] [PubMed]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Moher, D.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef]



| Patient | Publication | ECG Diagnosis | Medication before ES | ES Successful | Energy Level | Total Number of Shocks (n) | Recurrence after First Shock (Hours) | ES Repeats (n) | Energy Level | Medication after ES | Follow-Up Period |
|---|---|---|---|---|---|---|---|---|---|---|---|
| 1 | Ceresnak et al. [35] | AFL | No | CV: yes | 1.5 J/kg | n/a | n/a | n/a | n/a | Digoxin | n/a |
| 2 | Ceresnak et al. [35] | AFL | No | CV: yes | 1.5 J/kg | n/a | n/a | n/a | n/a | Digoxin | n/a |
| 3 | Konak et al. [19] | AFL | Amiodarone | CV: yes | 1.4 J/kg | n = 1 | 6–48 | n = 4 | 1.4 J/kg | Propafenone | 3 months |
| 4 | Miyake et al. [11] | VF | Amiodarone | DF: yes | n/a | n/a | 2 | n = 5 | n/a | Amiodarone Propanolol | 17 months |
| 5 | Saidi et al. [43] | VT | Adenosine Amiodarone Lidocaine | CV: yes | 1.5 J/kg | n = 2 | 24 | n = 1 | 2 J/kg | Amiodarone | n/a |
| 6 | Singh et al. [44] | SVT | No | CV: yes | n/a | n = 1 | 12 | n = 1 | n/a | Digoxin | 9 months |
| 7 | Singh et al. [44] | SVT | No | CV: yes | 20 J * | n = 1 | 12 | n = 1 | 10 J * | Digoxin | n/a |
| 8 | Sugrue et al. [45] | SVT | No | CV: yes | 2 J/kg | 1 | <12 | n = 6 | 2 J/kg | Digoxin Quinidine | 2 months |
| 9 | Sugrue et al. [45] | SVT | No | CV: yes | 2 J/kg | 1 | <72 | n = 10 | 2 J/kg | Digoxin Verapamil | 3 months |
| 10 | Texter et al. [8] | AFL | No | TEP: yes | n/a | n/a | n/a | n/a | n/a | Digoxin Propanolol | n/a |
| 11 | Texter et al. [8] | SVT | Flecainide Amiodarone | TEP: no | n/a | n/a | n/a | n/a | n/a | Digoxin Amiodarone | n/a |
| 12 | Texter et al. [8] | AFL | Amiodarone | TEP: no CV: no | n/a | n/a | n/a | n/a | n/a | Amiodarone Propanolol Digoxin | n/a |
| 13 | Texter et al. [8] | SVT | Procain-amide | TEP: no CV: yes | n/a | n/a | n/a | n/a | n/a | Flecainide | n/a |
| 14 | Texter et al. [8] | AFL | No | TEP: no | n/a | n/a | n/a | n/a | n/a | Flecainide Digoxin | n/a |
| 15 | Tunca Sahin et al. [14] | AFL | No | CV: yes | n/a | n/a | <6 | n/a | n/a | No | 13 years |
| 16 | Tunca Sahin et al. [14] | AFL | No | CV: yes | n/a | n/a | <6 | n/a | n/a | Flecainide Atenolol Digoxin | 16 years |
| 17 | Yilmaz-Semerci et al. [32] | AFL | Propanolol | CV: yes | 1 J/kg | n = 1 | 36–48 | n = 1 | 2 J/kg | Sotalol | 12 months |
| 18 | Yilmaz-Semerci et al. [32] | SVT | Adenosine | CV: yes | n/a | n = 1 | 3 | n = 2 | n/a | Propanolol | 12 months |
| 19 | Yilmaz-Semerci et al. [32] | AFL | Adenosine, propanolol | CV: yes | n/a | n = 1 | <1 | n/a | n/a | Amiodarone Propanolol | 12 months |
| 20 | Tunca Sahin et al. [14] | AFL | No | CV: yes | n/a | n/a | <6 | n/a | n/a | Flecainide Digoxin | 10 years |
| 21 | Tunca Sahin et al. [14] | AFL | No | CV: yes | n/a | n/a | <6 | n/a | n/a | Flecainide Amiodarone Digoxin | 11 years |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Oeffl, N.; Krainer, M.; Kurath-Koller, S.; Koestenberger, M.; Schwaberger, B.; Urlesberger, B.; Mileder, L.P. Cardiac Arrhythmias Requiring Electric Countershock during the Neonatal Period—A Systematic Review. Children 2023, 10, 838. https://doi.org/10.3390/children10050838
Oeffl N, Krainer M, Kurath-Koller S, Koestenberger M, Schwaberger B, Urlesberger B, Mileder LP. Cardiac Arrhythmias Requiring Electric Countershock during the Neonatal Period—A Systematic Review. Children. 2023; 10(5):838. https://doi.org/10.3390/children10050838
Chicago/Turabian StyleOeffl, Nathalie, Marlies Krainer, Stefan Kurath-Koller, Martin Koestenberger, Bernhard Schwaberger, Berndt Urlesberger, and Lukas P. Mileder. 2023. "Cardiac Arrhythmias Requiring Electric Countershock during the Neonatal Period—A Systematic Review" Children 10, no. 5: 838. https://doi.org/10.3390/children10050838
APA StyleOeffl, N., Krainer, M., Kurath-Koller, S., Koestenberger, M., Schwaberger, B., Urlesberger, B., & Mileder, L. P. (2023). Cardiac Arrhythmias Requiring Electric Countershock during the Neonatal Period—A Systematic Review. Children, 10(5), 838. https://doi.org/10.3390/children10050838