
Treating Parental Burnout: Impact and Particularities of a Mindfulness- and Compassion-Based Approach

 , and
, and
Abstract
1. Introduction
2. Materials and Methods
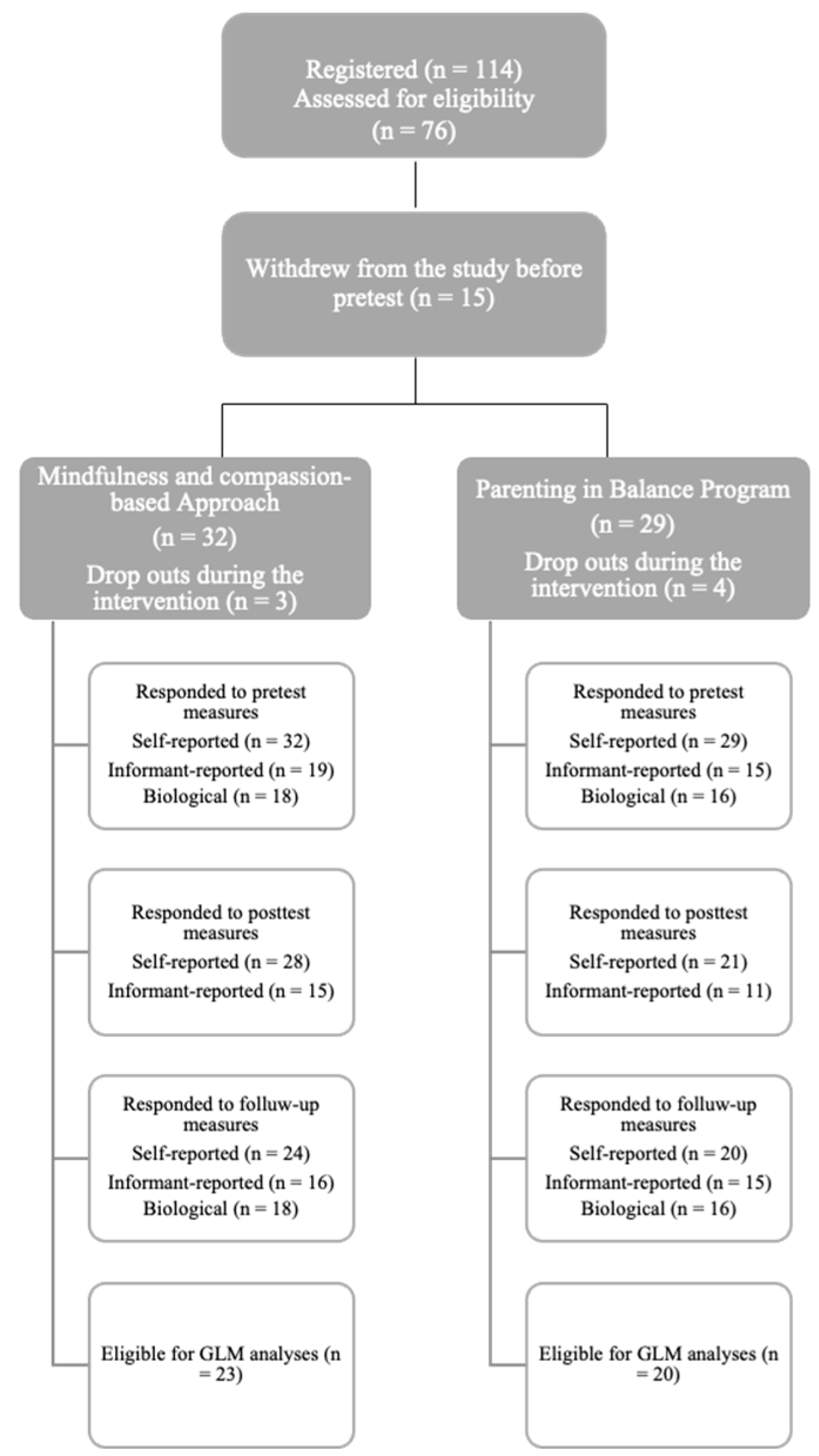
2.1. Participants
2.2. Measures
2.2.1. Self-Reported Outcomes
2.2.2. Informant-Reported Outcomes
2.2.3. Biological Outcome
2.3. Data Analysis
3. Results
3.1. Variance Analyses
3.2. Correlation Analyses
3.3. Complementary Analyses
4. Discussion
Limitations and Future Research
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Roskam, I.; Aguiar, J.; Akgun, E.; Arikan, G.; Artavia, M.; Avalosse, H.; Aunola, K.; Bader, M.; Bahati, C.; Barham, E.J.; et al. Parental Burnout Around the Globe: A 42-Country Study. Affect. Sci. 2021, 2, 58–79. [Google Scholar] [CrossRef]
- Roskam, I.; Brianda, M.-E.; Mikolajczak, M. A Step Forward in the Conceptualization and Measurement of Parental Burnout: The Parental Burnout Assessment (PBA). Front. Psychol. 2018, 9, 758. [Google Scholar] [CrossRef]
- Mikolajczak, M.; Roskam, I. A Theoretical and Clinical Framework for Parental Burnout: The Balance Between Risks and Resources (BR2). Front. Psychol. 2018, 9, 886. [Google Scholar] [CrossRef] [PubMed]
- Lin, G.-X.; Szczygieł, D.; Piotrowski, K. Child-Oriented Perfectionism and Parental Burnout: The Moderating Role of Parents’ Emotional Intelligence. Personal. Individ. Differ. 2022, 198, 111805. [Google Scholar] [CrossRef]
- Lebert-Charron, A.; Wendland, J.; Vivier-Prioul, S.; Boujut, E.; Dorard, G. Does Perceived Partner Support Have an Impact on Mothers’ Mental Health and Parental Burnout? Marriage Fam. Rev. 2022, 58, 362–382. [Google Scholar] [CrossRef]
- Le Vigouroux, S.; Bernat, K.; Charbonnier, E. Risk Factors and Consequences of Parental Burnout: Role of Early Maladaptive Schemas and Emotion-Focused Coping. Trends Psychol. 2023. [Google Scholar] [CrossRef]
- Liu, Y.; Chee, J.H.; Wang, Y. Parental Burnout and Resilience Intervention among Chinese Parents during the COVID-19 Pandemic. Front. Psychol. 2022, 13, 1034520. [Google Scholar] [CrossRef]
- Griffith, A.K.; Bedard, K.E.; Eaton, A.; Ackerlund Brandt, J.A.; Jha, P. Effects of the COVID-19 Pandemic on Parental Burnout and Parenting Practices: Analyses Using a Retrospective Pretest. Chronic Stress 2022, 6, 24705470221114059. [Google Scholar] [CrossRef]
- Kanter, J.B.; Proulx, C.M. The Longitudinal Association between Maternal Parenting Stress and Spousal Supportiveness. J. Fam. Psychol. 2019, 33, 121–131. [Google Scholar] [CrossRef]
- Paucsik, M.; Urbanowicz, A.; Leys, C.; Kotsou, I.; Baeyens, C.; Shankland, R. Self-Compassion and Rumination Type Mediate the Relation between Mindfulness and Parental Burnout. Int. J. Environ. Res. Public Health 2021, 18, 8811. [Google Scholar] [CrossRef]
- van Bakel, H.; Bastiaansen, C.; Hall, R.; Schwabe, I.; Verspeek, E.; Gross, J.J.; Brandt, J.A.; Aguiar, J.; Akgun, E.; Arikan, G.; et al. Parental Burnout across the Globe during the COVID-19 Pandemic. Int. Perspect. Psychol. Res. Pract. Consult. 2022, 11, 141–152. [Google Scholar] [CrossRef]
- Aguiar, J.; Matias, M.; Braz, A.C.; César, F.; Coimbra, S.; Gaspar, M.F.; Fontaine, A.M. Parental Burnout and the COVID-19 Pandemic: How Portuguese Parents Experienced Lockdown Measures. Fam. Relat. 2021, 70, 927–938. [Google Scholar] [CrossRef] [PubMed]
- Cluver, L.; Lachman, J.M.; Sherr, L.; Wessels, I.; Krug, E.; Rakotomalala, S.; Blight, S.; Hillis, S.; Bachman, G.; Green, O.; et al. Parenting in a Time of COVID-19. Lancet 2020, 395, e64. [Google Scholar] [CrossRef] [PubMed]
- Kerr, M.L.; Fanning, K.A.; Huynh, T.; Botto, I.; Kim, C.N. Parents’ Self-Reported Psychological Impacts of COVID-19: Associations With Parental Burnout, Child Behavior, and Income. J. Pediatr. Psychol. 2021, 46, 1162–1171. [Google Scholar] [CrossRef] [PubMed]
- Skjerdingstad, N.; Johnson, M.S.; Johnson, S.U.; Hoffart, A.; Ebrahimi, O.V. Parental Burnout during the COVID-19 Pandemic. Fam. Process 2022, 61, 1715–1729. [Google Scholar] [CrossRef]
- Stevenson, M.C.; Schaefer, C.T.; Ravipati, V.M. COVID-19 Patient Care Predicts Nurses’ Parental Burnout and Child Abuse: Mediating Effects of Compassion Fatigue. Child Abus. Negl. 2022, 130, 105458. [Google Scholar] [CrossRef]
- Mikolajczak, M.; Brianda, M.E.; Avalosse, H.; Roskam, I. Consequences of Parental Burnout: Its Specific Effect on Child Neglect and Violence. Child Abus. Negl. 2018, 80, 134–145. [Google Scholar] [CrossRef]
- Mikolajczak, M.; Gross, J.J.; Stinglhamber, F.; Norberg, A.L.; Roskam, I. Is Parental Burnout Distinct from Job Burnout and Depressive Symptomatology? Clin. Psychol. Sci. 2020, 8, 673–689. [Google Scholar] [CrossRef]
- Lindahl Norberg, A. Burnout in Mothers and Fathers of Children Surviving Brain Tumour. J. Clin. Psychol. Med. Settings 2007, 14, 130–137. [Google Scholar] [CrossRef]
- Urbanowicz, A.M.; Shankland, R.; Rance, J.; Bennett, P.; Leys, C.; Gauchet, A. Cognitive Behavioral Stress Management for Parents: Prevention and Reduction of Parental Burnout. Int. J. Clin. Health Psychol. 2023, 23, 100365. [Google Scholar] [CrossRef]
- Lindström, C.; Åman, J.; Anderzén-Carlsson, A.; Lindahl Norberg, A. Group Intervention for Burnout in Parents of Chronically Ill Children—A Small-Scale Study. Scand. J. Caring Sci. 2016, 30, 678–686. [Google Scholar] [CrossRef] [PubMed]
- Brianda, M.E.; Roskam, I.; Gross, J.J.; Franssen, A.; Kappala, F.; Gérard, F.; Mikolajczak, M. A Randomized Controlled Trial of Two Group Interventions for “Burned out” Parents: Effects on Psychological and Biological Outcomes. Psychother. Psychosom. 2020, 89, 330–332. [Google Scholar] [CrossRef] [PubMed]
- Lin, G.-X.; Szczygieł, D.; Hansotte, L.; Roskam, I.; Mikolajczak, M. Aiming to Be Perfect Parents Increases the Risk of Parental Burnout, but Emotional Competence Mitigates It. Curr. Psychol. 2021, 42, 1362–1370. [Google Scholar] [CrossRef]
- Stalder, T.; Steudte-Schmiedgen, S.; Alexander, N.; Klucken, T.; Vater, A.; Wichmann, S.; Kirschbaum, C.; Miller, R. Stress-Related and Basic Determinants of Hair Cortisol in Humans: A Meta-Analysis. Psychoneuroendocrinology 2017, 77, 261–274. [Google Scholar] [CrossRef] [PubMed]
- Brianda, M.E.; Roskam, I.; Mikolajczak, M. Comment Traiter Le Burn out Parental? Manuel D’intervention Clinique; De Boeck Supérieur: Louvain-la-Neuve, Belgium, 2019. [Google Scholar]
- Kil, H.; Grusec, J.E. Links among Mothers’ Dispositional Mindfulness, Stress, Perspective-Taking, and Mother-Child Interactions. Mindfulness 2020, 11, 1710–1722. [Google Scholar] [CrossRef]
- Lippold, M.A.; Jensen, T.M.; Duncan, L.G.; Nix, R.L.; Coatsworth, J.D.; Greenberg, M.T. Mindful Parenting, Parenting Cognitions, and Parent-Youth Communication: Bidirectional Linkages and Mediational Processes. Mindfulness 2021, 12, 381–391. [Google Scholar] [CrossRef]
- Zhang, W.; Liu, T.; Zhang, S.; Li, X. The Mutual Role of Mindful Parenting on Parents’ Subjective Well-Being and Young Children’s Emotional Regulation Through Reducing Perceived Parenting Daily Hassles. Mindfulness 2022, 13, 2777–2787. [Google Scholar] [CrossRef]
- Duncan, L.G.; Coatsworth, J.D.; Greenberg, M.T. A Model of Mindful Parenting: Implications for Parent–Child Relationships and Prevention Research. Clin. Child Fam. Psychol. Rev. 2009, 12, 255–270. [Google Scholar] [CrossRef]
- Dumas, J.E. Mindfulness-Based Parent Training: Strategies to Lessen the Grip of Automaticity in Families With Disruptive Children. J. Clin. Child Adolesc. Psychol. 2005, 34, 779–791. [Google Scholar] [CrossRef]
- Lindström, C.; Åman, J.; Norberg, A.L. Parental Burnout in Relation to Sociodemographic, Psychosocial and Personality Factors as Well as Disease Duration and Glycaemic Control in Children with Type 1 Diabetes Mellitus. Acta Paediatr. 2011, 100, 1011–1017. [Google Scholar] [CrossRef]
- Hölzel, B.K.; Lazar, S.W.; Gard, T.; Schuman-Olivier, Z.; Vago, D.R.; Ott, U. How Does Mindfulness Meditation Work? Proposing Mechanisms of Action From a Conceptual and Neural Perspective. Perspect. Psychol. Sci. 2011, 6, 537–559. [Google Scholar] [CrossRef]
- Gilbert, P.; Procter, S. Compassionate Mind Training for People with High Shame and Self-Criticism: Overview and Pilot Study of a Group Therapy Approach. Clin. Psychol. Psychother. 2006, 13, 353–379. [Google Scholar] [CrossRef]
- Sorkkila, M.; Aunola, K. Risk Factors for Parental Burnout among Finnish Parents: The Role of Socially Prescribed Perfectionism. J. Child Fam. Stud. 2020, 29, 648–659. [Google Scholar] [CrossRef]
- Meunier, J.-C.; Roskam, I. Self-Efficacy Beliefs amongst Parents of Young Children: Validation of a Self-Report Measure. J. Child Fam. Stud. 2009, 18, 495–511. [Google Scholar] [CrossRef]
- Breines, J.G.; Chen, S. Self-Compassion Increases Self-Improvement Motivation. Pers. Soc. Psychol. Bull. 2012, 38, 1133–1143. [Google Scholar] [CrossRef]
- Mancini, V.O.; De Palma, M.; Barker, J.L.; Kharrazi, S.; Izett, E.; Rooney, R.; Finlay-Jones, A.L. Paternal Attachment in the First Five Years: The Role of Self-Compassion, Negative Emotional Symptoms, Parenting Stress, and Parent Self-Efficacy. Mindfulness 2023, 14, 335–347. [Google Scholar] [CrossRef]
- Kirby, J.N. The Role of Mindfulness and Compassion in Enhancing Nurturing Family Environments. Clin. Psychol. Sci. Pract. 2016, 23, 142–157. [Google Scholar] [CrossRef]
- Zheng, Y.; Gu, X.; Jiang, M.; Zeng, X. How Might Mindfulness-Based Interventions Reduce Job Burnout? Testing a Potential Self-Regulation Model with a Randomized Controlled Trial. Mindfulness 2022, 13, 1907–1922. [Google Scholar] [CrossRef]
- Kinnunen, S.M.; Puolakanaho, A.; Tolvanen, A.; Mäkikangas, A.; Lappalainen, R. Improvements in Mindfulness Facets Mediate the Alleviation of Burnout Dimensions. Mindfulness 2020, 11, 2779–2792. [Google Scholar] [CrossRef]
- Potharst, E.S.; Baartmans, J.M.D.; Bögels, S.M. Mindful Parenting Training in a Clinical Versus Non-Clinical Setting: An Explorative Study. Mindfulness 2018, 12, 504–518. [Google Scholar] [CrossRef]
- Anclair, M.; Lappalainen, R.; Muotka, J.; Hiltunen, A.J. Cognitive Behavioural Therapy and Mindfulness for Stress and Burnout: A Waiting List Controlled Pilot Study Comparing Treatments for Parents of Children with Chronic Conditions. Scand. J. Caring Sci. 2018, 32, 389–396. [Google Scholar] [CrossRef]
- Brianda, M.E.; Roskam, I.; Mikolajczak, M. Hair Cortisol Concentration as a Biomarker of Parental Burnout. Psychoneuroendocrinology 2020, 117, 104681. [Google Scholar] [CrossRef]
- Brianda, M.E.; Mikolajczak, M.; Bader, M.; Bon, S.; Déprez, A.; Favez, N.; Holstein, L.; Le Vigouroux, S.; Lebert-Charron, A.; Sánchez-Rodríguez, R.; et al. Optimizing the Assessment of Parental Burnout: A Multi-Informant and Multimethod Approach to Determine Cutoffs for the Parental Burnout Inventory and the Parental Burnout Assessment. Assessment 2023, 30, 2234–2246. [Google Scholar] [CrossRef]
- Duncan, L.G. Assessment of Mindful Parenting among Parents of Early Adolescents: Development and Validation of the Interpersonal Mindfulness in Parenting Scale. Unpublished Dissertation, Doctoral Thesis, The Pennsylvania State University, Old Main, University Park, Pennsylvania, USA, 2007. [Google Scholar]
- Smith, B.W.; Guzman, A.; Erickson, K. The Unconditional Self-Kindness Scale: Assessing the Ability to Respond with Kindness to Threats to the Self. Mindfulness 2018, 9, 1713–1722. [Google Scholar] [CrossRef]
- Craig, K.J.; Hietanen, H.; Markova, I.S.; Berrios, G.E. The Irritability Questionnaire: A New Scale for the Measurement of Irritability. Psychiatry Res. 2008, 159, 367–375. [Google Scholar] [CrossRef]
- Sauvé, B.; Koren, G.; Walsh, G.; Tokmakejian, S.; Uum, S.H.V. Measurement of Cortisol in Human Hair as a Biomarker of Systemic Exposure. Clin. Investig. Med. 2007, 30, E183–E191. [Google Scholar] [CrossRef]
- Chen, Z.; Zhang, Q.; Chen, S.; Wang, W.; Liu, G.; Deng, H. Determination, Intercorrelation and Intraindividual Stability of Five Steroids in Hair, Saliva and Urine among Chinese College Students. Steroids 2019, 149, 108418. [Google Scholar] [CrossRef]
- Staufenbiel, S.M.; Penninx, B.W.J.H.; de Rijke, Y.B.; van den Akker, E.L.T.; van Rossum, E.F.C. Determinants of Hair Cortisol and Hair Cortisone Concentrations in Adults. Psychoneuroendocrinology 2015, 60, 182–194. [Google Scholar] [CrossRef] [PubMed]
- Parsons, C.E.; Crane, C.; Parsons, L.J.; Fjorback, L.O.; Kuyken, W. Home Practice in Mindfulness-Based Cognitive Therapy and Mindfulness-Based Stress Reduction: A Systematic Review and Meta-Analysis of Participants’ Mindfulness Practice and Its Association with Outcomes. Behav. Res. Ther. 2017, 95, 29–41. [Google Scholar] [CrossRef] [PubMed]
- Bayot, M.; Brianda, M.E.; van der Straten, N.; Mikolajczak, M.; Shankland, R.; Roskam, I. Mindfulness and Compassion-Based Approach to Parental Burnout. 2023. [Google Scholar] [CrossRef]
- Segal, Z.V.; Williams, J.M.G.; Teasdale, J.D. Mindfulness-Based Cognitive Therapy for Depression: A New Approach to Preventing Relapse, 1st ed.; The Guilford Press: New York, NY, USA, 2001; ISBN 978-1-57230-706-3. [Google Scholar]
- Bögels, S.; Restifo, K. Mindful Parenting: A Guide for Mental Health Practitioners; Mindfulness in Behavioral Health; Singh, N.N., Ed.; Springer: New York, NY, USA, 2014. [Google Scholar]
- Cohen, J. Statistical Power Analysis for the Behavioral Sciences, 2nd ed.; Routledge: New York, NY, USA, 1988; ISBN 978-0-203-77158-7. [Google Scholar]
- Manigault, A.W.; Slutsky, J.; Raye, J.; Creswell, J.D. Examining Practice Effects in a Randomized Controlled Trial: Daily Life Mindfulness Practice Predicts Stress Buffering Effects of Mindfulness Meditation Training. Mindfulness 2021, 12, 2487–2497. [Google Scholar] [CrossRef]
- van den Hurk, P.A.M.; Wingens, T.; Giommi, F.; Barendregt, H.P.; Speckens, A.E.M.; van Schie, H.T. On the Relationship Between the Practice of Mindfulness Meditation and Personality—An Exploratory Analysis of the Mediating Role of Mindfulness Skills. Mindfulness 2011, 2, 194–200. [Google Scholar] [CrossRef] [PubMed]
- Barkan, T.; Hoerger, M.; Gallegos, A.M.; Turiano, N.A.; Duberstein, P.R.; Moynihan, J.A. Personality Predicts Utilization of Mindfulness-Based Stress Reduction During and Post-Intervention in a Community Sample of Older Adults. J. Altern. Complement. Med. 2016, 22, 390–395. [Google Scholar] [CrossRef]
- Kinnunen, S.M.; Puolakanaho, A.; Tolvanen, A.; Mäkikangas, A.; Lappalainen, R. Does Mindfulness-, Acceptance-, and Value-Based Intervention Alleviate Burnout?—A Person-Centered Approach. Int. J. Stress Manag. 2018, 26, 89–101. [Google Scholar] [CrossRef]
- Lyubomirsky, S.; Layous, K. How Do Simple Positive Activities Increase Well-Being? Curr. Dir. Psychol. Sci. 2013, 22, 57–62. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
| Characteristic | N (%) 1 | |||
|---|---|---|---|---|
| MCA | PBP | Total | ||
| Sex | Men | 3 (10.7) | 3 (15) | 6 (12.5) |
| Women | 25 (89.3) | 17 (85) | 42 (87.5) | |
| Age category | 30–34 years | 5 (17.9) | 2 (10) | 7 (14.6) |
| 35–39 years | 12 (42.9) | 10 (50) | 22 (45.8) | |
| 40–44 years | 6 (21.4) | 6 (30) | 12 (25) | |
| 45–49 years | 3 (10.7) | 1 (5) | 4 (8.3) | |
| 50–54 years | 1 (3.6) | 1 (5) | 2 (4.2) | |
| 55–59 years | 1 (3.6) | 0 | 1 (2.1) | |
| Number of children | 1 | 2 (7.1) | 1 (4.8) | 3 (6.1) |
| 2 | 16 (57.1) | 10 (47.6) | 26 (53.1) | |
| 3 | 6 (21.4) | 10 (47.6) | 16 (32.7) | |
| 4 | 3 (10.7) | 0 | 3 (6.1) | |
| 5 | 1 (3.6) | 0 | 1 (2) | |
| Marital status | Living with a partner | 20 (71.4) | 15 (75) | 35 (72.9) |
| Solo parent | 8 (28.6) | 5 (25) | 13 (27.1) | |
| Level of education | Secondary | 2 (7.1) | 2 (10) | 4 (8.3) |
| Bachelor’s or master’s | 23 (82.1) | 14 (70) | 37 (77.1) | |
| Doctoral or equivalent | 3 (10.7) | 4 (20) | 7 (14.6) | |
| Work regime | Full-time | 14 (50) | 7 (35) | 21 (43.8) |
| Half-time | 1 (3.6) | 4 (20) | 5 (10.4) | |
| Part-time | 6 (21.4) | 5 (25) | 11 (22.9) | |
| Unemployed | 3 (10.7) | 3 (15) | 6 (12.5) | |
| Inability to work | 3 (10.7) | 1 (5) | 4 (8.3) | |
| Stay-at-home parent | 1 (3.6) | 0 | 1 (2.1) | |
| Session | Exercises |
|---|---|
| 1. Being a parent in the 21st century | Presentations; raisin exercise; detecting idealization Child as a raisin 1; detecting pressure for perfect parenting; mindful breathing |
| 2. Each burnout has its own story | Body scan; morning stress exercise 1; list of depleting/resourcing activities Body scan; calendar of positive experiences |
| 3. About parental perfectionism | Yoga/stretching; mental imagery on overinvestment; bringing kindness to yourself 1 Yoga/stretching; breathing space; calendar of negative experiences |
| 4. Developing emotional competencies | Mental imagery on guilt; meditation on the breath and body Meditation on the breath and body; breathing space in difficult times; calendar of reactions/responses |
| 5. Revaluing the relationship with children | Mindful walking; meditation on sounds and thoughts; imagination exercise: Limits 1 Meditation on sounds and thoughts or yoga; calendar of child’s positive emotions; mindful quality time with child |
| 6. The parental team | Imagination exercise: sharing parenthood; perspective taking in conflict situations; active listening Sitting meditation or yoga; calendar of coparental interactions |
| 7. Asking for help | Mental imagery on help seeking; chocolate exercise (awareness of interdependency); non-violent communication Chosen meditation; calendar of help requests; encouraging children’s autonomy |
| 8. Preventing relapse | 3-walk exercise; balance exercise; discussion on follow-up |
| Pretest | Post-Test | Follow-Up | % of Change | F(df) * | η2p | ||
|---|---|---|---|---|---|---|---|
| PBA | MCA | 90.83 (30.32) | 70.12 (30.09) | 65.46 (35) | −28% | 34.74 (1.76, 73.78) | 0.45 |
| PBP | 87.2 (31.66) | 60.85 (28.24) | 57.35 (32.85) | −30% | |||
| Neglect | MCA | 20.79 (11.89) | 17.13 (11.2) | 14.21 (8.92) | −32% | 11.99 (2, 84) | 0.22 |
| PBP | 19.65 (12.33) | 14.9 (6.75) | 14.5 (9.55) | −26% | |||
| Violence | MCA | 16.09 (8.32) | 12.13 (7.66) | 11.52 (7.42) | −28% | 14.88 (1.59, 63.54) | 0.27 |
| PBP | 17.95 (11.95) | 11.37 (6.98) | 11.84 (7.12) | −34% | |||
| PBA-i | MCA | 79 (39.23) | 61.25 (29.89) | 66 (37.7) | −16% | 9.87 (2, 36) | 0.35 |
| PBP | 94.38 (31.26) | 77.63 (42.48) | 62.38 (38.26) | −34% | |||
| IRR-i | MCA | 2.52 (1.35) | 2.23 (1.53) | 2.43 (1.48) | −4% | 2.73 (2, 36) | 0.13 |
| PBP | 3.23 (1.07) | 2.72 (1.26) | 2.32 (1.35) | −28% | |||
| BR2 | MCA | −19.71 (48.2) | 0.79 (48.72) | −6.08 (55.13) | +13.63 b | 4.98 (1.67, 68.6) | 0.11 |
| PBP | −0.95 (23.89) | 15.84 (31.24) | 30.32 (31.01) | +31.27 b | |||
| IM-P | MCA | 3.13 (0.47) | 3.42 (0.39) | 3.31 (0.4) | +6% | 12.98 (1.73, 72.67) | 0.24 |
| PBP | 3.11 (0.33) | 3.34 (0.25) | 3.37 (0.23) | +8% | |||
| USK | MCA | 2.95 (0.98) | 3.66 (1.2) | 3.55 (1.4) | +20% | 16.22 (2, 84) | 0.28 |
| PBP | 2.68 (1.09) | 3.47 (1.12) | 3.84 (0.73) | +43% |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bayot, M.; Brianda, M.E.; van der Straten, N.; Mikolajczak, M.; Shankland, R.; Roskam, I. Treating Parental Burnout: Impact and Particularities of a Mindfulness- and Compassion-Based Approach. Children 2024, 11, 168. https://doi.org/10.3390/children11020168
Bayot M, Brianda ME, van der Straten N, Mikolajczak M, Shankland R, Roskam I. Treating Parental Burnout: Impact and Particularities of a Mindfulness- and Compassion-Based Approach. Children. 2024; 11(2):168. https://doi.org/10.3390/children11020168
Chicago/Turabian StyleBayot, Marie, Maria Elena Brianda, Nastasya van der Straten, Moïra Mikolajczak, Rebecca Shankland, and Isabelle Roskam. 2024. "Treating Parental Burnout: Impact and Particularities of a Mindfulness- and Compassion-Based Approach" Children 11, no. 2: 168. https://doi.org/10.3390/children11020168
APA StyleBayot, M., Brianda, M. E., van der Straten, N., Mikolajczak, M., Shankland, R., & Roskam, I. (2024). Treating Parental Burnout: Impact and Particularities of a Mindfulness- and Compassion-Based Approach. Children, 11(2), 168. https://doi.org/10.3390/children11020168