1. Introduction
Pregnancy and the first few months following childbirth represent a period of mental-health vulnerability for women, as symptoms of depression, anxiety and stress are prevalent [
1,
2,
3]. The COVID-19 pandemic has added further stressors, making everyone, but particularly women in the perinatal period, particularly vulnerable in terms of their well-being and mental health. During the pandemic, perinatal care was modified to comply with sanitary measures, social support was diminished due to social distancing measures and women could have additional worries about their health and the health of their child [
4].
Child development is likely to be influenced by exposure to maternal prepartum and postpartum mental health. Exposure to prepartum and postpartum maternal stress has been associated with lower cognitive development [
5,
6], as well as to the development of a difficult temperament and the child’s social–emotional development [
7,
8]. Exposure to increased prepartum and postpartum maternal anxiety is associated with a risk of unfavourable development in the child’s social-emotional behaviour [
9]. Exposure to maternal postpartum depression has been linked to the child’s cognitive [
10] and behavioural [
11,
12] development.
Several aspects of the mother–child interaction may have consequences on child development [
10,
11,
12]. Indeed, mothers experiencing depressive and anxiety-related symptoms may be less sensitive and attentive to their child’s needs, which can in turn prevent the child from developing a secure attachment, and lead to associated difficulties in social functioning and emotional regulation [
11]. The lack of maternal sensitivity and attention may also affect the child’s temperament, influencing their behavioural development [
12]. Moreover, depressed mothers may be less disposed to offer a sufficient stimulation [
10]. Lack of stimulation may affect the quantity and quality of verbal interactions, affecting children’s cognitive development [
10].
While most studies have focused on diminished environmental opportunities for children raised by mothers with distress symptoms, few have investigated the impact of maternal prepartum and postpartum mental health on the child’s ability to process sensory stimuli [
13,
14,
15,
16]. While sensory sensitivity varies from person to person, the way one perceives and responds to a stimulus can vary greatly [
17]. Some people with sensory hypersensitivity will exhibit over-reactivity to sensory stimuli, which can lead to intense and aversive reactions [
17]. On a developmental level, poor sensory processing skills in children are likely to have a negative impact on their social, cognitive and sensorimotor development [
18]. According to the conceptual model presented by Dunn (1997), sensory avoidance corresponds to a sensory processing profile for which the neurological threshold for perception is low, i.e., there is sensory hypersensitivity, for which active self-regulatory strategies are employed to avoid excessive sensory stimulation [
18]. Thus, children with sensory-avoidance behaviours may be reticent or withdraw from certain activities and adopt routines or rituals so that sensory input and neural activity become predictable and familiar patterns [
18]. From a clinical perspective, these children may not be able to tolerate physical touch or commonly encountered sounds, have a restricted diet and withdraw from activities normally perceived as pleasurable, thus becoming overwhelmed by sensory stimulation, resulting in strong emotional reactions or disruptive behaviour [
19].
Very few studies have investigated the links between exposure to symptoms of prepartum maternal distress and childhood sensory development [
13,
14,
15,
16], and even fewer on the biological mechanisms underlying these associations [
14,
15,
16,
20]. However, several studies have delved into the neurobiological and endocrine mechanisms that underly the association between prenatal maternal stress and foetal brain development. According to the foetal programming hypothesis, during critical periods of prepartum development, organ structure and function can be permanently altered as a function of the intrauterine environment and the time of exposure [
21,
22,
23]. Prepartum stress is likely to reduce the activity of the 11β-hydroxysteroid dehydrogenase type 2 (11β-HSD2) enzyme, which regulates foetal exposure to cortisol by converting it into its inactive form, cortisone [
21,
24,
25,
26,
27]. This could lead to increased foetal exposure to maternal cortisol, which may affect the neuroendocrine, structural and behavioural phenotype of the offspring [
21,
26,
27]. More specifically, glucocorticoids have important effects on brain development, for instance by modulating synaptic development, as well as cell proliferation and differentiation in various brain regions [
23,
24,
25]. Under high-stress conditions, long-term effects on foetal brain development could result from exposure to higher levels of maternal cortisol [
27]. Downregulation of the placental 11β-HSD2 gene has also been associated with prepartum maternal anxiety and, to a lesser extent, prepartum maternal depression [
28]. High levels of maternal stress could also lead to increased levels of corticotropin-releasing hormone (CRH) in the placenta, which, by activating CRH receptors, could influence the development of certain foetal brain areas rich in CRH receptors, like the amygdala, the hippocampus and limbic cortical areas [
21,
29]. For example, prepartum exposure to glucocorticoids leads to higher levels of CRH in the amygdala, which is associated with the altered functioning of this brain structure involved in the expression of anxiety and fear [
25]. Prepartum maternal stress has also been associated with sleep disorders during pregnancy and a less healthy diet, which can lead to immune and inflammatory responses, as well as to nutrient deficiencies that can impair foetal brain development [
22,
24]. One theory to explain greater sensory sensitivity, and even sensory hypersensitivity, puts forward an imbalance between neuronal excitation and inhibition through differences in levels of the excitatory neurotransmitter glutamate or inhibitory neurotransmitter GABA (gamma-aminobutyric acid) in neural circuits of the neocortex involved in sensory perception [
17,
20]. Exposure to prepartum maternal stress is likely to disrupt the development of GABAergic and glutamatergic pathways in offspring, as it has been associated with the altered expression of certain receptor subunits and markers of synthesis and the transport of the GABAergic and glutamatergic pathways in the offspring [
30,
31].
Current evidence and recent studies highlight the impact of distress-provoking factors in women during the prepartum and postpartum period in association with the child’s neurological, cognitive and behavioural development [
5,
6,
7,
8,
9,
10,
17,
21,
26,
30,
31,
32,
33]. However, few studies have focused on the potential effects of prepartum and postpartum maternal depression, anxiety and stress on children’s sensory development and behavioural responses during sensory stimulation [
13,
14,
15,
16,
20]. There are still several factors and mechanisms related to childhood sensory avoidance that are not fully understood. Therefore, the aim of the present study is to assess the associations between prepartum and postpartum maternal symptoms of depression, anxiety and stress related to the COVID-19 pandemic and childhood sensory avoidance.
4. Discussion
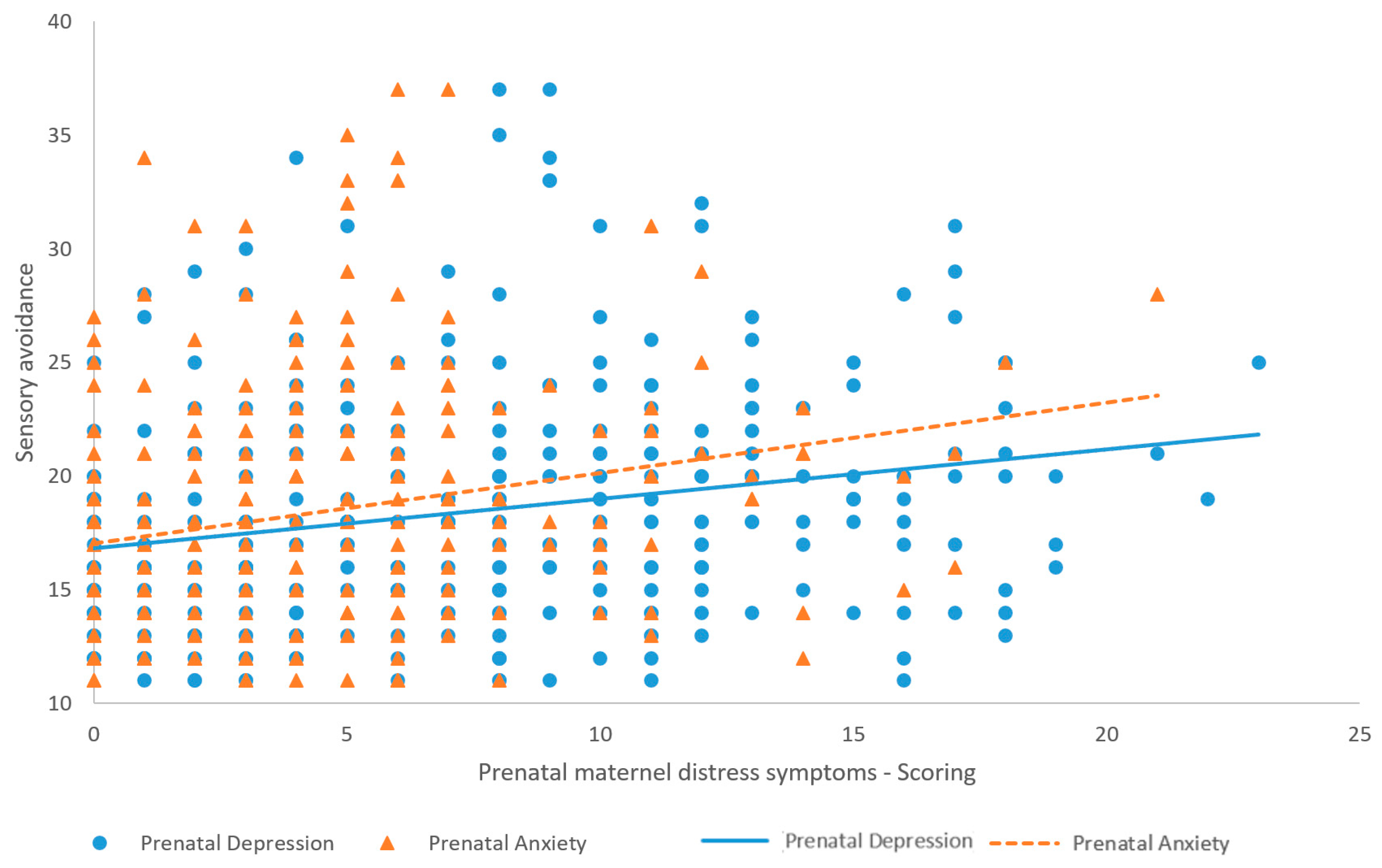
This study demonstrates that higher levels of maternal prepartum and 18-month postpartum symptoms of depression and anxiety are associated with higher levels of childhood sensory avoidance at 18 months. The results support that together, prepartum and 18-month postpartum depression and anxiety predict the variance of childhood sensory avoidance at 18 months. However, none of these maternal distress symptoms stand out as a better predictor of childhood sensory avoidance at 18 months. These results concur with those of Gee et al. (2021) [
13], who found that higher levels of maternal prepartum anxiety and depression, as well as higher levels of maternal anxiety and depression at 6 months postpartum, were associated with more “outside of the majority” scores on the sensory sensitivity scale in 14-month-old infants. Whereas sensory avoidance involves active self-regulatory strategies to sensory overstimulation, sensory sensitivity is characterized by passive responses to sensory overstimulation [
18]. Our results, together with those obtained by Gee et al. (2021) [
13], suggest an association between prepartum and postpartum maternal distress and sensory processing profiles characterized by sensory hypersensitivity. Hence, our study complements the latter, indicating that the association is maintained in time, and suggesting the association between maternal prepartum and postpartum distress symptoms and infants’ sensory sensitivity symptoms can also involve avoidance behaviours.
Associations found between maternal postpartum depression and anxiety and childhood sensory avoidance suggest that maternal postpartum distress might influence children’s behavioural responses to sensory overstimulation. Indeed, postpartum maternal distress is susceptible to influencing childhood behavioural development through a reduced number of positive mother–infant interactions [
12]. In particular, maternal postpartum distress has been associated with a child’s difficult temperament [
8], which is reflected in withdrawal responses to new sensorial stimulation and intense emotional responses [
51]. These responses associated with having a difficult temperament are in line with active withdrawal and avoidance behaviours observed in children who are prone to sensory avoidance [
18].
Since maternal prepartum depression and anxiety symptoms were also associated with child sensory avoidance at 18 months, the involvement of biological mechanisms in these associations are likely. It was suggested that prepartum maternal stress could increase foetal exposure to maternal cortisol and increased levels of corticotropin-releasing hormone (CRH) in the placenta [
21,
28]. This could affect the neuroendocrine, structural and behavioural phenotype of the offspring, as well as the development of certain foetal-brain areas rich in CRH receptors [
21,
26]. Maternal prepartum stress has also been linked to the alteration of the expression of certain components of the GABAergic and glutamatergic pathways [
30,
31]. An imbalance in the levels of the excitatory neurotransmitter glutamate or the inhibitory neurotransmitter GABA is likely to lead to hyperexcitability in the neocortex neural circuits involved in sensory perception [
17,
20,
52]. Prepartum maternal stress has also been associated with alterations in the serotonergic and norepinephrine systems, with neurotransmitters playing a crucial role in brain development [
53,
54,
55,
56,
57]. Several brain-development processes (cell migration, neuronal division and synaptogenesis) are influenced by serotonin, which acts as a trophic factor [
58]. The development of noradrenergic neurons is regulated by norepinephrine, which contributes to the shaping of the nervous system [
56]. The disruption of these processes by excessive or insufficient levels of these neurotransmitters is likely to alter the developmental trajectory of the brain, leading to lasting changes in brain function [
54,
56,
58]. In fact, prepartum exposure to selective serotonin reuptake inhibitors (SSRIs) has been associated with anatomical and functional changes in somatosensory cortical neurons [
55]. For instance, SSRI use during pregnancy was associated with improved infant performance on a language discrimination task, suggesting accelerated perceptual development in the auditory cortex [
15]. Consequently, exposure to maternal prepartum stress could affect the development of certain brain areas involved in cerebral excitability and sensory processing, lowering the neurological threshold [
17,
20,
21,
26,
52,
53,
54,
55,
56,
57,
58,
59,
60].
Genetic factors could also partly explain the results obtained in our study. Sensory-processing abnormalities are particularly common in children and adults with neurodevelopmental disorders caused by genetically guided mechanisms, such as autism spectrum disorders (ASDs) [
61]. Studies have shown a greater prevalence of sensory abnormalities among parents of children with ASDs than among parents of typically developing children [
61,
62], and among parents of multiplex ASD families than among parents of simplex ASD families [
61]. The concordance rate of defensive behaviours to tactile and auditory stimuli was also higher in monozygotic than in dizygotic twins [
63]. Some polymorphisms in the CNTNAP2 (contactin-associated protein-like 2) and Gabrb3 genes, which are known genetic risk factors for ASD, were associated with hypersensitivity to heat and tactile stimuli [
64,
65,
66]. These findings support the idea that genetic predispositions could also lead to sensory-processing abnormalities and could partly explain the results obtained in our study.
Our results could also be explained by epigenetic modifications induced by prepartum and postpartum exposure to maternal stress. Indeed, according to the Dual-Activation Hypothesis, exposure to prepartum maternal stress during critical periods of neural development may lead, via hormonal and synaptic alterations, to epigenetic modifications in stress-related and other connected neural networks, including sensory and emotional networks [
14]. Genes coding for the glucocorticoid receptor (Gr) [
14,
67,
68,
69,
70] and the FK506-binding protein 5 (Fkbp5) [
14,
67] in the hippocampus, along with the neuropeptide arginine vasopressin (Avp) [
14,
67,
68,
71] and the corticotropin-releasing factor (Crf) [
14,
67] in the hypothalamus, may be implicated in the epigenetic programming of the stress response [
14]. These epigenetic modifications, while facilitating specific adaptations to stressors, may also lead to functional maladaptation depending on the timing and the intensity of the stimulation [
14,
72,
73]. For example, prior research has shown alterations in brain structures, such as increased grey matter density in the left superior temporal gyrus of the primary auditory cortex in children exposed to verbal abuse [
14,
72], and reduced grey matter volume in the visual cortex in those witnessing domestic violence [
14,
73]. Thus, the associations we observed between prepartum and postpartum maternal depression and anxiety could also result from epigenetic changes due to early exposure to maternal distress. To acquire a thorough understanding of the transgenerational transmission of sensory sensitivity, it is essential to gather genetic, epigenetic and symptom evaluations from both infants and parents.
Moreover, our study stands out for having examined prepartum and postpartum maternal stress related to the COVID-19 pandemic and its possible association with sensory avoidance. However, prepartum and 18-month postpartum stress related to the COVID-19 pandemic were not associated with or predictive of infant sensory sensitivity. This was not expected, considering the literature supporting a link between prepartum and postpartum maternal stress and child development [
6,
8,
21,
26]. Indeed, it is possible that stress specifically linked to the COVID-19 pandemic has not had a detectable effect on child development, but overall maternal stress does. In fact, our results suggest that regardless of the reason or source of the distress experienced by the mother, it can influence the child’s sensory development. On the other hand, our sample was made up of participants who were predominantly employed, with high incomes and living with a partner. Therefore, our participants may had protective factors that prevented them from being impacted by the additional stress factors arising from the pandemic (e.g., social isolation, job loss and lockdown) [
4,
74]. Also, the level of distress associated with the COVID-19 pandemic could have fluctuated considerably depending on the level of contagion and public health policies in place, which were modified considerably throughout the pandemic. The level of distress could also have stabilized or decreased over time as the COVID-19 pandemic unfolded over a long period of time. Our scale, which assessed the overall stress levels experienced in relation to the COVID-19 pandemic, may thus have lacked sensitivity. Future studies could evaluate the effects of prepartum and postpartum maternal distress experienced during the COVID-19 pandemic while considering the different waves of the pandemic, as well as the impacts of certain additional stressors resulting from the pandemic (e.g., job loss and social isolation).
Most participants were in their second trimester of pregnancy when they completed their prepartum questionnaires, which is a particularly vulnerable window for foetal neurodevelopment, as neurogenesis and neuronal migration processes are particularly active [
75,
76]. Thus, exposure to prepartum maternal stress during the second trimester of pregnancy may particularly influence foetal brain development [
75,
76,
77], affecting subsequent childhood cognitive development [
78]. As we found a higher effect of anxiety during the prepartum period, and considering that most of our participants were in their second trimester when they completed their prepartum questionnaires, our results corroborate studies regarding the timing of exposure to prepartum maternal distress on child development [
75,
76,
77,
78]. On the other hand, foetal brain development begins as early as the first trimester of pregnancy. As early as the fifth week of pregnancy, all major subdivisions of the brain (i.e., myelencephalon, metencephalon, mesencephalon, diencephalon and telencephalon), as well as the interhemispheric fissure, are identifiable [
79]. The thickening of the hippocampus begins at 5 weeks postmenstrual age (PMA) [
79]. Moreover, maternal distress experienced during the first trimester of pregnancy has been associated with the child’s cognitive development [
78] and having difficult temperament [
80,
81]. While a proportion of our participants were in their first trimester of pregnancy at the time of completing their prepartum questionnaires, distress experienced during this trimester of pregnancy may also have influenced the results obtained in this study.
Associations were found between some maternal diagnoses (i.e., asthma, high blood pressure, migraines, anaemia or blood disease, diabetes, ulcer or stomach disease) and treatments (i.e., asthma, anaemia or blood disease), and maternal prepartum and postpartum depression, anxiety and stress related to COVID-19. These findings are consistent with studies investigating the distress experienced by pregnant women with chronic illnesses [
82,
83,
84]. Some chronic illnesses (e.g., diabetes, thyroid and kidney disease) can lead to adverse outcomes for pregnant women (e.g., pre-eclampsia and gestational hypertension) [
83,
85,
86,
87] and their infants [
83,
88,
89]. Pregnant women with chronic illnesses may therefore experience distress resulting from managing the risk of these chronic diseases on their health and that of their infant [
83], or from perceptions of a lack of control and low self-efficacy [
82]. Interestingly, even after controlling for the potential impacts of chronic diseases during pregnancy on foetal development and maternal stress [
82,
83,
84,
85,
86,
87,
88,
89], associations were still observed between prepartum and 18-month postpartum maternal depression and anxiety and childhood sensory avoidance.
The respective associations between prepartum and 18-month postpartum symptoms of maternal distress and child sensory avoidance at 18 months were observed among children with typical development. In this sample of the CONCEPTION study, the developmental spheres assessed using the ASQ-3 (i.e., communication, gross motor, fine motor, problem solving and personal–social) were not significantly associated with prepartum and 18-month postpartum symptoms of depression, anxiety and stress related to the COVID-19 pandemic, nor with sensory avoidance at 18 months. However, numerous studies support an association between exposure to prepartum and postpartum symptoms of maternal distress and childhood cognitive, motor, behavioural and socio-emotional development [
6,
8,
9,
10,
11,
12]. Given that a large proportion of the children in the sample showed normal development across the different developmental spheres assessed (i.e., between 60.8% and 72.6%), it is possible that prepartum and 18-month postpartum maternal distress did not impact the developmental spheres as assessed through the ASQ-3 for the majority of children. Thus, the associations observed between prepartum and 18-month postpartum symptoms of maternal distress and childhood sensory avoidance at 18 months were unlikely to be influenced by atypical child development.
The limitations of this study must be considered. For example, some of the measurement scales used are very circumscribed in time, since the depression- and anxiety-screening scales assess symptoms experienced in the seven to fourteen days preceding the completion of the questionnaire. Thus, it is not possible to know whether these symptoms persisted over time, and what effect the persistence of symptoms would have had on the study results. However, we have used validated tools to measure maternal mental health, which yields results indicative of symptoms of depression and anxiety. Also, this study cannot reveal the relation between sensory avoidance and temperament peculiarities, which have been observed as influencing child behavioural development [
90]. This limits the interpretation of the observed associations between maternal distress symptoms and sensory avoidance, which could be due either to neurological reasons, such as a particular sensory-processing profile such as sensory hypersensitivity, or to behavioural tendencies, arising, for example, from a difficult temperament. In addition, since our sample consisted mainly of white Canadians with a high socioeconomic status, the generalizability of our results to diverse populations is limited. To ensure better generalizability, future studies investigating the associations between maternal mental health and childhood sensory development should include participants from more diverse cultural communities and socioeconomic statuses. Lastly, all variables were measured from questionnaires completed by the mothers, including variables relating to their child. The condition of the mother could have led to a bias in the evaluation of variables related to the child’s health and development. The size of the observed associations could have been artificially inflated. Despite these limitations, this study revealed for the first time associations between prepartum maternal emotional symptoms and sensory avoidance, which can subsequently affect infants’ and children’s behaviours. As a result, the findings reveal new mechanistic avenues to explain the associations between prepartum maternal emotional symptoms and postpartum childhood neurodevelopment.





{kind=link}
{kind=link}