

Examining Language, Speech and Behaviour Characteristics: A Cross-Sectional Study in Saudi Arabia Using the Arabic Version of Gilliam Autism Rating Scale-Third Edition



Abstract
:1. Introduction
1.1. An Overview of Autism Spectrum Disorder
1.2. Impact on Families and Heterogeneity of ASD
1.3. Factors Influencing the Presentation and Management of ASD
1.4. Purpose of the Present Study
2. Method
2.1. Sample
2.2. Instrument: The Translation Process
2.3. Design
2.4. Procedures
3. Results
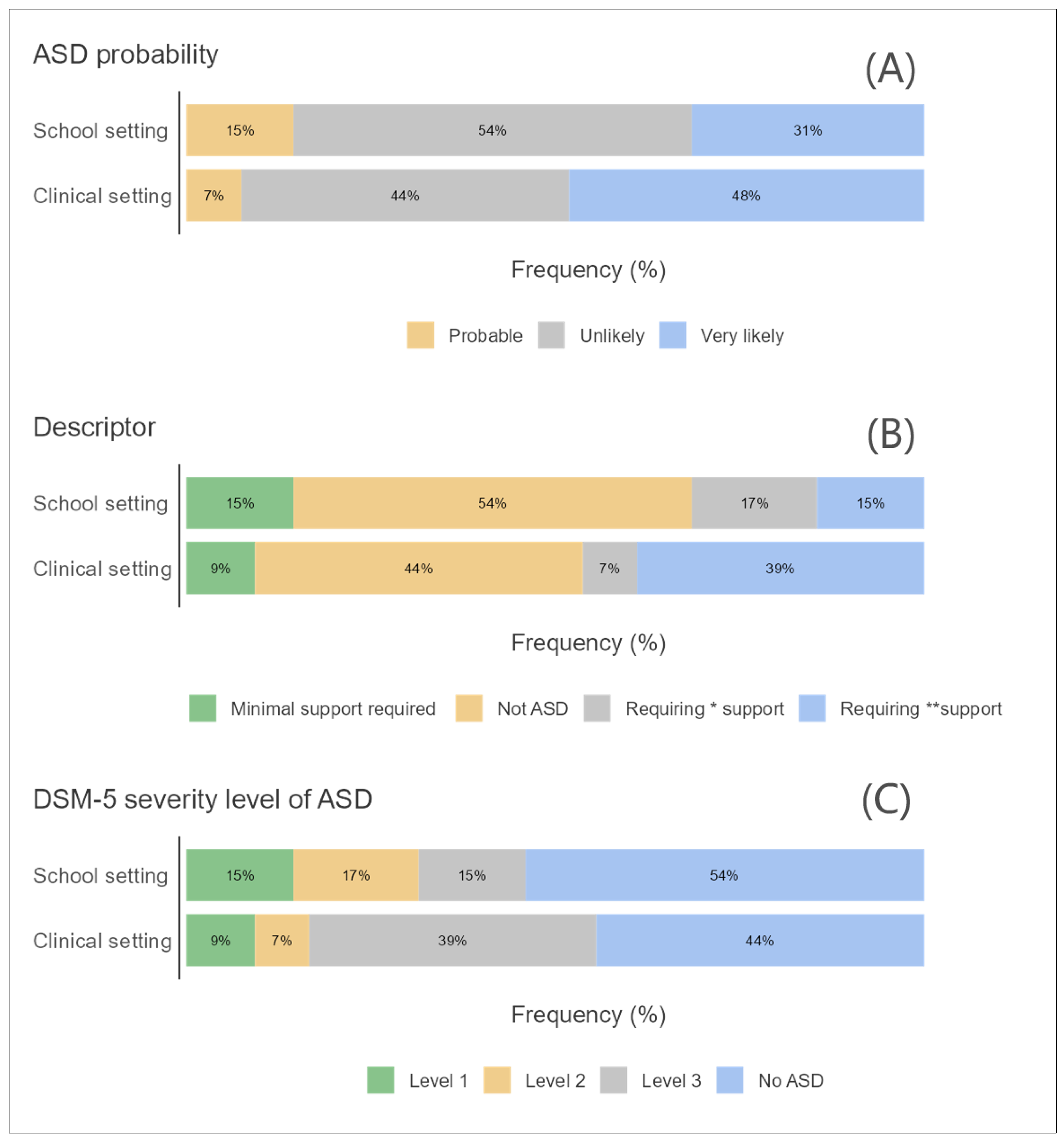
3.1. ASD and Developmental Status
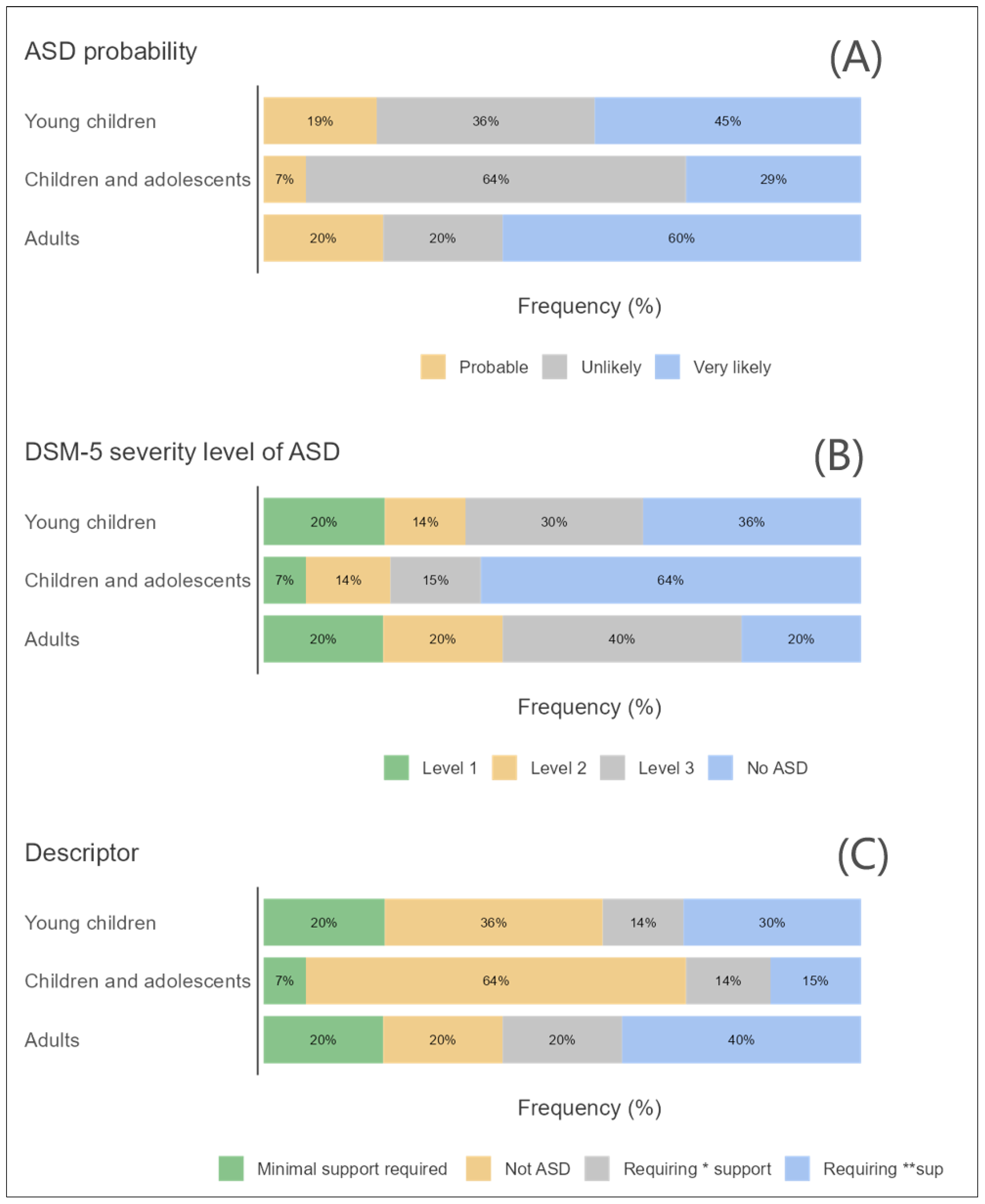
3.2. ASD and Age Groups
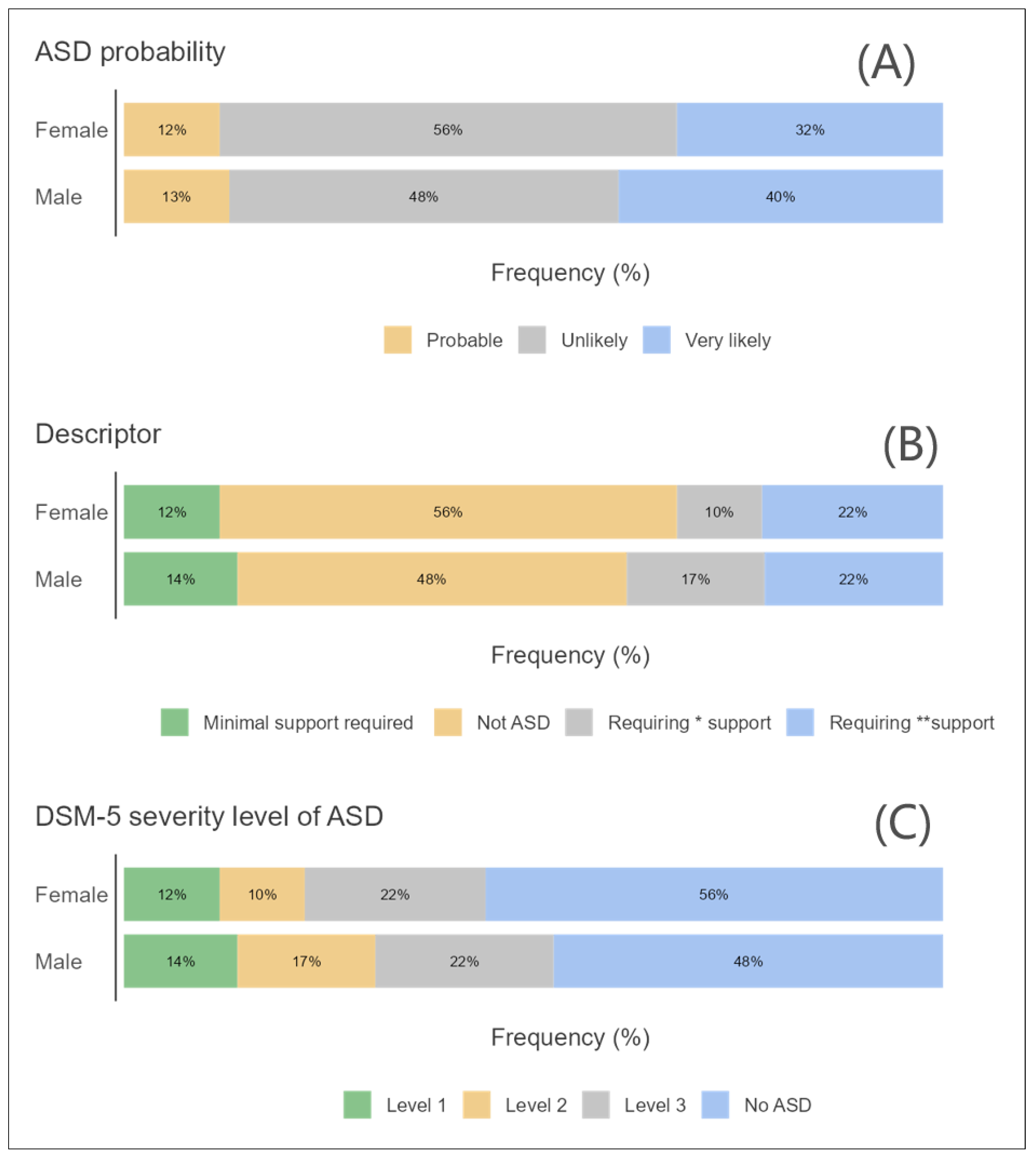
3.3. ASD and Sex
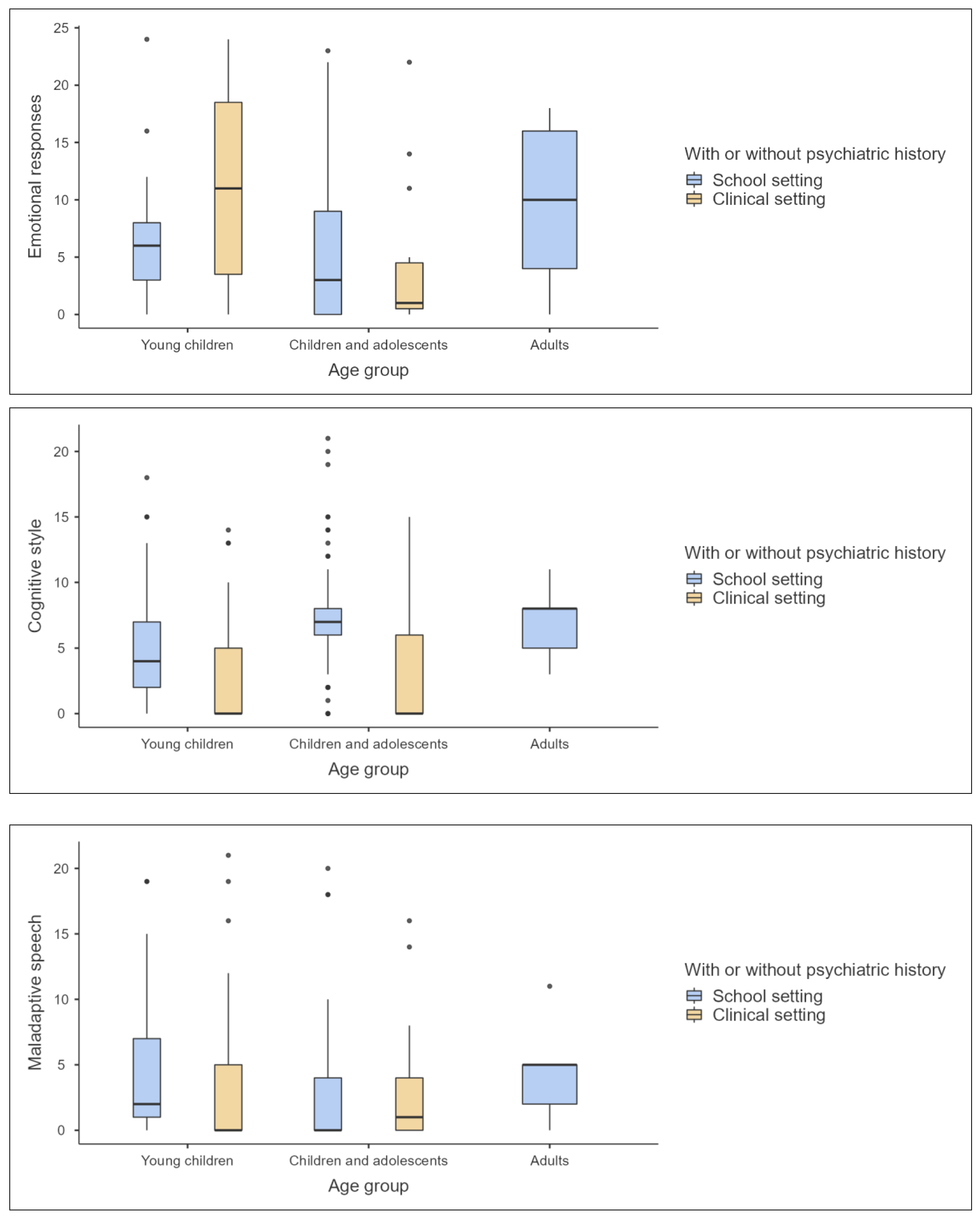
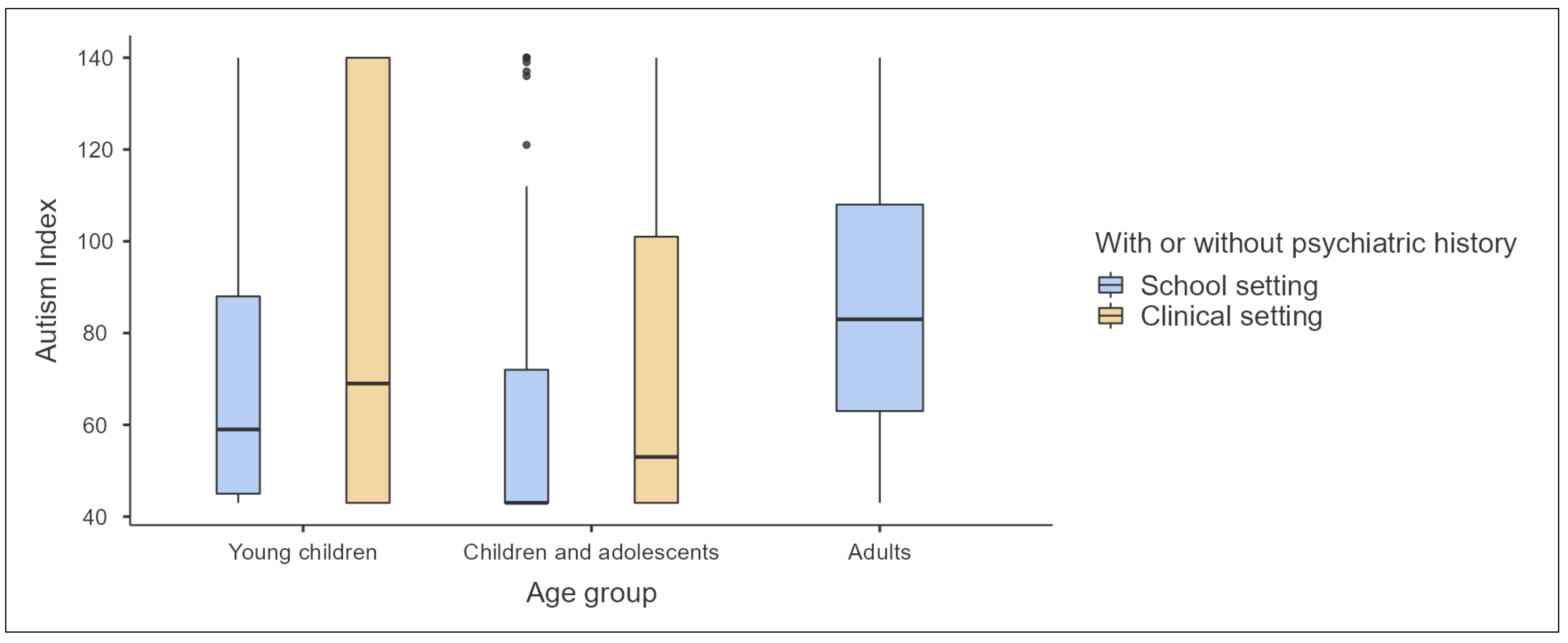
3.4. Descriptive Statistical Analysis of Age Groups and Settings
3.5. Inferential Statistical Analysis of Developmental Status, Geographical Location, Sex, Age, and Different Levels of ASD
4. Discussion
5. Limitations
6. Implications for Practice
7. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- World Health Organization. 6A02: Autism Spectrum Disorder. In International Classification of Diseases; World Health Organization: Geneva, Switzerland, 2023; 11th Revision. [Google Scholar]
- American Psychiatric Association. F84.0: Autism Spectrum Disorder. In Diagnostic and Statistical Manual of Mental Disorders: DSM-5-TR; American Psychiatric Association: Arlington, VA, USA, 2022; pp. 56–68. [Google Scholar]
- Papadopoulos, A.; Siafaka, V.; Tsapara, A.; Tafiadis, D.; Kotsis, K.; Skapinakis, P.; Tzoufi, M. Measuring Parental Stress, Illness Perceptions, Coping and Quality of Life in Families of Children Newly Diagnosed with Autism Spectrum Disorder. BJPsych Open 2023, 9, e84. [Google Scholar] [CrossRef]
- Boucher, J. Autism Spectrum Disorders Characteristics, Causes and Practical Issues, 3rd ed.; SAGE Publications Ltd.: New York, NY, USA, 2022. [Google Scholar]
- Jacobs, D.; Steyaert, J.; Dierickx, K.; Hens, K. Parents’ Multi-Layered Expectations When Requesting an Autism Spectrum Disorder Assessment of Their Young Child: An in-Depth Interview Study. BMC Psychiatry 2020, 20, 440. [Google Scholar] [CrossRef] [PubMed]
- Volkmar, F.; Siegel, M.; Woodbury-Smith, M.; King, B.; McCracken, J.; State, M. Practice Parameter for the Assessment and Treatment of Children and Adolescents with Autism Spectrum Disorder. J. Am. Acad. Child. Adolesc. Psychiatry 2014, 53, 237–257. [Google Scholar] [CrossRef]
- Ashwood, K.L.; Buitelaar, J.; Murphy, D.; Spooren, W.; Charman, T. European Clinical Network: Autism Spectrum Disorder Assessments and Patient Characterisation. Eur. Child. Adolesc. Psychiatry 2015, 24, 985–995. [Google Scholar] [CrossRef]
- Dahiya, A.V.; DeLucia, E.; McDonnell, C.G.; Scarpa, A. A Systematic Review of Technological Approaches for Autism Spectrum Disorder Assessment in Children: Implications for the COVID-19 Pandemic. Res. Dev. Disabil. 2021, 109, 103852. [Google Scholar] [CrossRef]
- Rojahn, J.; Matson, J.L. Assessment and Diagnosis of Autism and Spectrum Disorders in Children. J. Dev. Phys. Disabil. 2010, 22, 313–315. [Google Scholar] [CrossRef]
- Kantzer, A.-K.; Fernell, E.; Gillberg, C.; Miniscalco, C. Autism in Community Pre-Schoolers: Developmental Profiles. Res. Dev. Disabil. 2013, 34, 2900–2908. [Google Scholar] [CrossRef]
- Centers for Disease Control and Prevention. Data & Statistics on Autism Spectrum Disorder. Available online: https://www.cdc.gov/ncbddd/autism/data.html (accessed on 4 March 2024).
- Waligórska, A.; Kucharczyk, S.; Waligórski, M.; Kuncewicz-Sosnowska, K.; Kalisz, K.; Odom, S. National Professional Development Center on Autism Spectrum Disorders (NPDC) Model—An Integrated Model of Evidence-Based Practices for Autism Spectrum Disorder. Psychiatr. Pol. 2019, 53, 753–770. [Google Scholar] [CrossRef] [PubMed]
- Schall, C.M.; McDonough, J.T. Autism Spectrum Disorders in Adolescence and Early Adulthood: Characteristics and Issues. J. Vocat. Rehabil. 2010, 32, 81–88. [Google Scholar] [CrossRef]
- Kreiser, N.L.; White, S.W. ASD in Females: Are We Overstating the Gender Difference in Diagnosis? Clin. Child. Fam. Psychol. Rev. 2014, 17, 67–84. [Google Scholar] [CrossRef]
- Simonoff, E.; Pickles, A.; Charman, T.; Chandler, S.; Loucas, T.; Baird, G. Psychiatric Disorders in Children with Autism Spectrum Disorders: Prevalence, Comorbidity, and Associated Factors in a Population-Derived Sample. J. Am. Acad. Child. Adolesc. Psychiatry 2008, 47, 921–929. [Google Scholar] [CrossRef] [PubMed]
- Durkin, M.S.; Maenner, M.J.; Meaney, F.J.; Levy, S.E.; DiGuiseppi, C.; Nicholas, J.S.; Kirby, R.S.; Pinto-Martin, J.A.; Schieve, L.A. Socioeconomic Inequality in the Prevalence of Autism Spectrum Disorder: Evidence from a U.S. Cross-Sectional Study. PLoS ONE 2010, 5, e11551. [Google Scholar] [CrossRef] [PubMed]
- Gilliam, J.E. GARS-3: Gilliam Autism Rating Scale, 3rd ed.; Pro-Ed: Austin, TX, USA, 2014. [Google Scholar]
- Alasmari, M.; Alduais, A.; Qasem, F.; Almaghlough, S.; AlAmri, L. Arabic Validation of Gilliam Autism Rating Scale-Third Edition to Identify Individuals with and without Autism Spectrum Disorder. Psychol. Sch. 2024; under review. [Google Scholar]
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders: DSM-5, 5th ed.; American Psychiatric Association: Washington, DC, USA, 2013. [Google Scholar]
- Tudor, M.E.; Hoffman, C.D.; Sweeney, D.P. Children with Autism: Sleep Problems and Symptom Severity. Focus Autism Other Dev. Disabil. 2012, 27, 254–262. [Google Scholar] [CrossRef]
- Samadi, S.A.; McConkey, R. The Utility of the Gilliam Autism Rating Scale for Identifying Iranian Children with Autism. Disabil. Rehabil. 2014, 36, 452–456. [Google Scholar] [CrossRef] [PubMed]
- Veatch, O.J.; Sutcliffe, J.S.; Warren, Z.E.; Keenan, B.T.; Potter, M.H.; Malow, B.A. Shorter Sleep Duration Is Associated with Social Impairment and Comorbidities in ASD. Autism Res. 2017, 10, 1221–1238. [Google Scholar] [CrossRef] [PubMed]
- Driscoll, K.; Schonberg, M.; Stark, M.F.; Carter, A.S.; Hirshfeld-Becker, D. Family-Centered Cognitive Behavioral Therapy for Anxiety in Very Young Children with Autism Spectrum Disorder. J. Autism Dev. Disord. 2020, 50, 3905–3920. [Google Scholar] [CrossRef]
- Vasa, R.A.; Kalb, L.; Mazurek, M.; Kanne, S.; Freedman, B.; Keefer, A.; Clemons, T.; Murray, D. Age-Related Differences in the Prevalence and Correlates of Anxiety in Youth with Autism Spectrum Disorders. Res. Autism Spectr. Disord. 2013, 7, 1358–1369. [Google Scholar] [CrossRef]
- Anderson, L.C.; Bolling, D.Z.; Schelinski, S.; Coffman, M.C.; Pelphrey, K.A.; Kaiser, M.D. Sex Differences in the Development of Brain Mechanisms for Processing Biological Motion. NeuroImage 2013, 83, 751–760. [Google Scholar] [CrossRef]
- Baron-Cohen, S.; Richler, J.; Bisarya, D.; Gurunathan, N.; Wheelwright, S. The Systemizing Quotient: An Investigation of Adults with Asperger Syndrome or High-Functioning Autism, and Normal Sex Differences. Philos. Trans. R. Soc. B Biol. Sci. 2003, 358, 361–374. [Google Scholar] [CrossRef]
- Lai, M.-C.; Baron-Cohen, S.; Buxbaum, J.D. Understanding Autism in the Light of Sex/Gender. Mol. Autism 2015, 6, 24. [Google Scholar] [CrossRef]
- Lai, M.C.; Lombardo, M.V.; Ruigrok, A.N.V.; Chakrabarti, B.; Auyeung, B.; Szatmari, P.; Happé, F.; Baron-Cohen, S. Quantifying and Exploring Camouflaging in Men and Women with Autism. Autism 2016, 21, 690–702. [Google Scholar] [CrossRef]
- Posserud, M.; Skretting Solberg, B.; Engeland, A.; Haavik, J.; Klungsøyr, K. Male to Female Ratios in Autism Spectrum Disorders by Age, Intellectual Disability and Attention-deficit/Hyperactivity Disorder. Acta Psychiatr. Scand. 2021, 144, 635–646. [Google Scholar] [CrossRef]
- Livingston, L.A.; Shah, P.; Happe, F. Autism Spectrum Disorder. Encycl. Ment. Health 2019, 1, 124–130. [Google Scholar]
- Livingston, L.A.; Shah, P.; Happé, F. Compensatory Strategies below the Behavioural Surface in Autism: A Qualitative Study. Lancet Psychiatry 2019, 6, 766–777. [Google Scholar] [CrossRef] [PubMed]
- McPartland, J.C.; Reichow, B.; Volkmar, F.R. Sensitivity and Specificity of Proposed DSM-5 Diagnostic Criteria for Autism Spectrum Disorder. J. Am. Acad. Child. Adolesc. Psychiatry 2012, 51, 368–383. [Google Scholar] [CrossRef]
- Russell, G.; Steer, C.; Golding, J. Social and Demographic Factors That Influence the Diagnosis of Autistic Spectrum Disorders. Soc. Psychiatry Psychiatr. Epidemiol. 2011, 46, 1283–1293. [Google Scholar] [CrossRef] [PubMed]
- Pozo, P.; Sarriá, E.; Brioso, A. Family Quality of Life and Psychological Well-Being in Parents of Children with Autism Spectrum Disorders: A Double ABCX Model. J. Intellect. Disabil. Res. 2014, 58, 442–458. [Google Scholar] [CrossRef]
- Jackson, L.S.; Little, S.G.; Akin-Little, A. The Spanish Adaptation of the Gilliam Autism Rating Scale-2: Translation and Psychometric Analysis. Res. Autism Spectr. Disord. 2013, 7, 1160–1167. [Google Scholar] [CrossRef]
- Diken, İ.H.; Avşar, A.; Diken, Ö.; Gilliam, J.E. Exploring the Validity and Reliability of Turkish Version of Gilliam Autism Rating Scale-2: Turkish Standardization Study* Gilliam Otistik Bozukluk Derecelendirme Ölçeği-2 Türkçe Versiyonu’nun (GOBDÖ-2-TV) Geçerlik ve Güvenirliğinin Araştırılması: Türkiye Standardizasyon Çalışması; Turkish Education Association: Ankara, Turkey, 2012; Volume 37. [Google Scholar]
- Choi, H.; Kim, U. The Reliability and Validity of the Gilliam Autism Rating Scale with Children and Youth in the Republic of Korea: A Preliminary Study. Korean J. Spec. Eduation 2005, 40, 301–311. [Google Scholar]
- Jhin, H.-K.; Yoon, H.-J.; Park, J.-P. 한국판-Gilliam 자폐증 평정척도-2(K-GARS-2) 표준화 연구 (Korean-Gilliam Autism Rating Scale-2(K-GARS-2) Standardization). Biol. Ther. Psychiatry 2011, 17, 189. [Google Scholar]
- Samadi, S.A.; Noori, H.; Abdullah, A.; Ahmed, L.; Abdalla, B.; Biçak, C.A.; McConkey, R. The Psychometric Properties of the Gilliam Autism Rating Scale (GARS-3) with Kurdish Samples of Children with Developmental Disabilities. Children 2022, 9, 434. [Google Scholar] [CrossRef] [PubMed]
- Samadi, S.A.; McConkey, R.; Nuri, H.; Abdullah, A.; Ahmad, L.; Abdalla, B.; Biçak, C.A. Screening Children for Autism Spectrum Disorders in Low-and Middle-Income Countries: Experiences from the Kurdistan Region of Iraq. Int. J. Environ. Res. Public Health 2022, 19, 4581. [Google Scholar] [CrossRef] [PubMed]
- AlJabery, A.M. The Examination of Validity and Reliability Indicators of the Jordanian Translated Arabic Version of the Gilliam Autism Rating Scale (GARS-2). Ph.D. Thesis, Wayne State University, Detroit, MI, USA, 2008. [Google Scholar]
- Li, N. Preliminary Validation of the Childhood Autism Rating Scale-Second Edition Questionnaire for Parents or Caregivers (Cars2-Qpc) and the Gilliam Autism Rating Scale (Gars-2) with a Chinese-Speaking Population. Master’s Thesis, University of Eastern Kentucky, Richmond, KY, USA, 2005. [Google Scholar]
- Samadi, S.A.; Biçak, C.A.; Noori, H.; Abdalla, B.; Abdullah, A.; Ahmed, L. Autism Spectrum Disorder Diagnostic Criteria Changes and Impacts on the Diagnostic Scales-Utility of the 2nd and 3rd Versions of the Gilliam Autism Rating Scale (GARS). Brain Sci. 2022, 12, 537, Erratum in Brain Sci. 2023, 13, 1081. [Google Scholar] [CrossRef]
- Alasmari, M.; Alduais, A.; Qasem, F. A Thematic Review of Autism Spectrum Disorder Research in Saudi Arabia: Insights into Diagnosis, Assessment, and Language Considerations. Appl. Neuropsychol. Child. 2023, 1–15. [Google Scholar] [CrossRef]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| School Setting (n) | Clinical Setting (n) | % | ||
|---|---|---|---|---|
| Age Group | 124 | 54 | 69.66 | 30.34 |
| 3–5 | 28 | 28 | 22.58 | 51.85 |
| 6–10 | 59 | 21 | 47.58 | 38.89 |
| 11–15 | 28 | 5 | 22.58 | 9.26 |
| 16–20 | 6 | 0 | 4.84 | 0 |
| 21–22 | 3 | 0 | 2.42 | 0 |
| Gender Group | ||||
| Female | 60 | 17 | 48.39 | 31.48 |
| Male | 64 | 37 | 51.61 | 68.52 |
| City Group | ||||
| Asir province | 90 | 3 | 72.58 | 5.56 |
| Riyadh Province | 4 | 0 | 3.23 | 0 |
| Eastern Province | 10 | 0 | 8.06 | 0 |
| Medina Province | 1 | 0 | 0.81 | 0 |
| Tabuk Province | 0 | 1 | 0 | 1.85 |
| Mecca Province | 19 | 50 | 15.32 | 92.59 |
| Exceptionality Status | ||||
| No exceptionality | 124 | NA | 100 | NA |
| Attention deficit hyperactivity disorder | NA | 3 | NA | 5.56 |
| Autism spectrum disorder | NA | 16 | NA | 29.63 |
| Apraxia of speech | NA | 1 | NA | 1.85 |
| Hearing impairment | NA | 6 | NA | 11.11 |
| Dysarthria | NA | 1 | NA | 1.85 |
| Speech and language delay | NA | 27 | NA | 50.00 |
| Ethnicity | ||||
| Arabs | 124 | 54 | 69.66 | 30.34 |
| Language (mother tongue) | ||||
| Arabic (Saudi dialect) | 124 | 54 | 69.66 | 30.34 |
| Subscale | Elaboration on Relation to ASD Based on GARS-3 |
|---|---|
| Restricted/Repetitive Behaviours | This subscale measures the presence and severity of behaviours characterized by rigidity, restricted interests, and repetitive actions, which are core features of ASD. |
| Social Interaction | Assesses the individual’s ability to engage in and maintain social reciprocity, recognize social cues, and form social connections, which are often impaired in ASD. |
| Social Communication | Evaluates the capacity for verbal and non-verbal communication, including the use of language for social engagement, often disrupted in individuals with ASD. |
| Emotional Responses | Probes the range, intensity, and appropriateness of emotional reactions, which can be markedly atypical or muted in persons with ASD. |
| Cognitive Style | Examines the individual’s thinking patterns, problem-solving approach, and preference for detail, which may be rigid or idiosyncratic in ASD. |
| Maladaptive Speech | Measures aspects of speech and language such as echolalia, pronoun reversal, or atypical language processing, commonly observed in ASD. |
| 95% Confidence Interval | |||||||||
|---|---|---|---|---|---|---|---|---|---|
| ASD Covariates | Age Group | Setting | n | Mean | Lower | Upper | SD | Minimum | Maximum |
| Restricted/repetitive behaviours | Young children | School | 35 | 8.3143 | 5.910032 | 10.7185 | 6.9990 | 0 | 22 |
| Clinical | 39 | 9.8974 | 6.373936 | 13.4209 | 10.8695 | 0 | 35 | ||
| Children and adolescents | School | 84 | 4.4048 | 2.875758 | 5.9338 | 7.0457 | 0 | 28 | |
| Clinical | 15 | 4.2667 | −0.335610 | 8.8689 | 8.3106 | 0 | 24 | ||
| Adults | School | 5 | 15.2000 | 2.254499 | 28.1455 | 10.4259 | 0 | 26 | |
| Clinical | 0 | NaN | NaN | NaN | NaN | NaN | NaN | ||
| Social interaction | Young children | School | 35 | 9.3429 | 6.871448 | 11.8143 | 7.1945 | 0 | 33 |
| Clinical | 39 | 13.7436 | 9.718284 | 17.7689 | 12.4176 | 0 | 40 | ||
| Children and adolescents | School | 84 | 6.2262 | 4.443530 | 8.0089 | 8.2145 | 0 | 35 | |
| Clinical | 15 | 12.7333 | 7.362318 | 18.1043 | 9.6988 | 0 | 29 | ||
| Adults | School | 5 | 9.8000 | −1.215176 | 20.8152 | 8.8713 | 0 | 24 | |
| Clinical | 0 | NaN | NaN | NaN | NaN | NaN | NaN | ||
| Social communication | Young children | School | 35 | 5.3143 | 3.057461 | 7.5711 | 6.5699 | 0 | 27 |
| Clinical | 39 | 13.7949 | 10.342419 | 17.2473 | 10.6504 | 0 | 27 | ||
| Children and adolescents | School | 84 | 3.5000 | 2.362845 | 4.6372 | 5.2400 | 0 | 19 | |
| Clinical | 15 | 11.3333 | 7.941051 | 14.7256 | 6.1257 | 1 | 24 | ||
| Adults | School | 5 | 5.2000 | −2.218877 | 12.6189 | 5.9749 | 0 | 15 | |
| Clinical | 0 | NaN | NaN | NaN | NaN | NaN | NaN | ||
| Emotional responses | Young children | School | 35 | 6.2000 | 4.464749 | 7.9353 | 5.0515 | 0 | 24 |
| Clinical | 39 | 10.6667 | 8.046492 | 13.2868 | 8.0829 | 0 | 24 | ||
| Children and adolescents | School | 84 | 4.8333 | 3.580180 | 6.0865 | 5.7745 | 0 | 23 | |
| Clinical | 15 | 4.2667 | 0.699383 | 7.8340 | 6.4417 | 0 | 22 | ||
| Adults | School | 5 | 9.6000 | 0.078777 | 19.1212 | 7.6681 | 0 | 18 | |
| Clinical | 0 | NaN | NaN | NaN | NaN | NaN | NaN | ||
| Cognitive style | Young children | School | 35 | 5.2286 | 3.572561 | 6.8846 | 4.8208 | 0 | 18 |
| Clinical | 39 | 2.8974 | 1.518527 | 4.2763 | 4.2538 | 0 | 14 | ||
| Children and adolescents | School | 84 | 7.2857 | 6.404317 | 8.1671 | 4.0615 | 0 | 21 | |
| Clinical | 15 | 3.2667 | 0.848558 | 5.6848 | 4.3665 | 0 | 15 | ||
| Adults | School | 5 | 7.0000 | 3.172935 | 10.8271 | 3.0822 | 3 | 11 | |
| Clinical | 0 | NaN | NaN | NaN | NaN | NaN | NaN | ||
| Maladaptive speech | Young children | School | 35 | 4.6857 | 2.891520 | 6.4799 | 5.2231 | 0 | 19 |
| Clinical | 39 | 3.4872 | 1.682516 | 5.2918 | 5.5672 | 0 | 21 | ||
| Children and adolescents | School | 84 | 2.4286 | 1.478571 | 3.3786 | 4.3776 | 0 | 20 | |
| Clinical | 15 | 3.4000 | 0.493683 | 6.3063 | 5.2481 | 0 | 16 | ||
| Adults | School | 5 | 4.6000 | −0.564486 | 9.7645 | 4.1593 | 0 | 11 | |
| Clinical | 0 | NaN | NaN | NaN | NaN | NaN | NaN | ||
| Autism Index | Young children | School | 35 | 71.6000 | 61.495909 | 81.7041 | 29.4141 | 43 | 140 |
| Clinical | 39 | 89.9487 | 75.363880 | 104.5336 | 44.9924 | 43 | 140 | ||
| Children and adolescents | School | 84 | 61.2738 | 54.628896 | 67.9187 | 30.6198 | 43 | 140 | |
| Clinical | 15 | 75.0000 | 55.051782 | 94.9482 | 36.0218 | 43 | 140 | ||
| Adults | School | 5 | 87.4000 | 40.211867 | 134.5881 | 38.0039 | 43 | 140 | |
| Clinical | 0 | NaN | NaN | NaN | NaN | NaN | NaN | ||
| Predictor | Estimate | SE | t | p | Stand. Estimate |
|---|---|---|---|---|---|
| Intercept a | 36.25922 | 3.87145 | 9.365798 | <0.001 | |
| Age group: | |||||
| Children and adolescents − Young children | 0.25656 | 2.18107 | 0.117629 | 0.907 | 0.0070924 |
| Adults − Young children | 3.51402 | 7.16343 | 0.490550 | 0.624 | 0.0971435 |
| With or without psychiatric history: | |||||
| Clinical setting − School setting | 3.70333 | 5.87191 | 0.630686 | 0.529 | 0.1023769 |
| Sex: | |||||
| Male − Female | −0.59044 | 2.00372 | −0.294673 | 0.769 | −0.0163225 |
| City: | |||||
| Alahsa − Abha | 2.89860 | 7.34399 | 0.394690 | 0.694 | 0.0801304 |
| Aldammam − Abha | −9.78531 | 6.45331 | −1.516324 | 0.132 | −0.2705103 |
| Alnamas − Abha | −0.26859 | 3.36240 | −0.079880 | 0.936 | −0.0074250 |
| Bisha − Abha | −5.59268 | 3.80554 | −1.469615 | 0.144 | −0.1546071 |
| Damam − Abha | 9.73980 | 8.80952 | 1.105600 | 0.271 | 0.2692524 |
| Jedah − Abha | 7.73624 | 8.46106 | 0.914335 | 0.362 | 0.2138648 |
| Jeddah − Abha | −5.14428 | 6.79038 | −0.757583 | 0.450 | −0.1422112 |
| Madina − Abha | −0.22739 | 11.68801 | −0.019455 | 0.985 | −0.0062860 |
| Meca − Abha | 10.56277 | 6.67077 | 1.583440 | 0.115 | 0.2920029 |
| Mecca − Abha | 0.15357 | 8.23633 | 0.018646 | 0.985 | 0.0042454 |
| Riyadh − Abha | 1.77468 | 11.70869 | 0.151570 | 0.880 | 0.0490602 |
| Riyadh − Abha | 3.74127 | 8.78265 | 0.425985 | 0.671 | 0.1034258 |
| Riyadh − Abha | 11.06206 | 11.92286 | 0.927802 | 0.355 | 0.3058056 |
| Tabuk − Abha | 14.58953 | 12.84005 | 1.136252 | 0.258 | 0.4033210 |
| Taif − Abha | 28.07248 | 12.31899 | 2.278797 | 0.024 | 0.7760508 |
| Jeddah − Abha | −4.96632 | 7.07335 | −0.702116 | 0.484 | −0.1372915 |
| Restricted/repetitive behaviours | 1.23866 | 0.18274 | 6.778242 | <0.001 | 0.2941276 |
| Social interaction | 0.57525 | 0.18132 | 3.172541 | 0.002 | 0.1539529 |
| Social communication | 1.53008 | 0.20861 | 7.334672 | <0.001 | 0.3474993 |
| Emotional responses | 0.72660 | 0.21869 | 3.322467 | 0.001 | 0.1347893 |
| Cognitive style | 0.54846 | 0.26989 | 2.032135 | 0.044 | 0.0699885 |
| Maladaptive speech | 1.29200 | 0.24114 | 5.357834 | <0.001 | 0.1758611 |
| Predictor | Estimate | SE | Z | p |
|---|---|---|---|---|
| Intercept | 1.791759 | 0.40825 | 4.388896 | <0.001 |
| Age group: | ||||
| Children and adolescents − Young children | −1.098612 | 0.81650 | −1.345520 | 0.178 |
| Adults − Young children | −27.094345 | 189,338.66108 | −1.4310 × 10−4 | 1.000 |
| With or without psychiatric history: | ||||
| Clinical setting − School setting | −1.791759 | 1.08012 | −1.658847 | 0.097 |
| DSM-5 severity level of ASD: | ||||
| Level 2 − Level 1 | −0.405465 | 0.64550 | −0.628144 | 0.530 |
| Level 3 − Level 1 | −0.693147 | 0.70711 | −0.980258 | 0.327 |
| No ASD − Level 1 | −0.182322 | 0.60553 | −0.301094 | 0.763 |
| Sex: | ||||
| Male − Female | −0.405465 | 0.64550 | −0.628144 | 0.530 |
| Age group * With or without psychiatric history: | ||||
| (Children and adolescents − Young children) * (Clinical setting − School setting) | −24.203973 | 189,338.66083 | −1.2783 × 10−4 | 1.000 |
| (Adults − Young children) * (Clinical setting − School setting) | 1.791759 | 267,765.30214 | 6.6915 × 10−6 | 1.000 |
| Age group * DSM-5 severity level of ASD: | ||||
| (Children and adolescents − Young children) * (Level 2 − Level 1) | 0.405465 | 1.19024 | 0.340659 | 0.733 |
| (Adults − Young children) * (Level 2 − Level 1) | 0.405465 | 267,765.30227 | 1.5143 × 10−6 | 1.000 |
| (Children and adolescents − Young children) * (Level 3 − Level 1) | 2.197225 | 1.05409 | 2.084470 | 0.037 |
| (Adults − Young children) * (Level 3 − Level 1) | 0.693147 | 267,765.30213 | 2.5886 × 10−6 | 1.000 |
| (Children and adolescents − Young children) * (No ASD − Level 1) | 2.821379 | 0.94994 | 2.970068 | 0.003 |
| (Adults − Young children) * (No ASD − Level 1) | 25.484907 | 189,338.66108 | 1.3460 × 10−4 | 1.000 |
| With or without psychiatric history * DSM-5 severity level of ASD: | ||||
| (Clinical setting − School setting) * (Level 2 − Level 1) | −24.897120 | 189,338.66068 | −1.3150 × 10−4 | 1.000 |
| (Clinical setting − School setting) * (Level 3 − Level 1) | 2.079442 | 1.32288 | 1.571910 | 0.116 |
| (Clinical setting − School setting) * (No ASD − Level 1) | 1.974081 | 1.23828 | 1.594214 | 0.111 |
| Age group * Sex: | ||||
| (Children and adolescents − Young children) * (Male − Female) | 1.321756 | 1.05672 | 1.250805 | 0.211 |
| (Adults − Young children) * (Male − Female) | 25.708050 | 189,338.66108 | 1.3578 × 10−4 | 1.000 |
| With or without psychiatric history * Sex: | ||||
| (Clinical setting − School setting) * (Male − Female) | 1.791759 | 1.29099 | 1.387891 | 0.165 |
| DSM-5 severity level of ASD * Sex: | ||||
| (Level 2 − Level 1) * (Male − Female) | 0.628609 | 0.93095 | 0.675234 | 0.500 |
| (Level 3 − Level 1) * (Male − Female) | −4.4186 × 10−15 | 1.11803 | −3.9521 × 10−15 | 1.000 |
| (No ASD − Level 1) * (Male − Female) | 0.587787 | 0.88506 | 0.664120 | 0.507 |
| Age group * With or without psychiatric history * DSM-5 severity level of ASD: | ||||
| (Children and adolescents − Young children) * (Clinical setting − School setting) * (Level 2 − Level 1) | 50.892852 | 267,765.30190 | 1.9007 × 10−4 | 1.000 |
| (Adults − Young children) * (Clinical setting − School setting) * (Level 2 − Level 1) | 24.897120 | 423,374.11640 | 5.8806 × 10−5 | 1.000 |
| (Children and adolescents − Young children) * (Clinical setting − School setting) * (Level 3 − Level 1) | 21.719066 | 189,338.66083 | 1.1471 × 10−4 | 1.000 |
| (Adults − Young children) * (Clinical setting − School setting) * (Level 3 − Level 1) | −2.079442 | 378,677.32166 | −5.4913 × 10−6 | 1.000 |
| (Children and adolescents − Young children) * (Clinical setting − School setting) * (No ASD − Level 1) | 21.788059 | 189,338.66083 | 1.1507 × 10−4 | 1.000 |
| (Adults − Young children) * (Clinical setting − School setting) * (No ASD − Level 1) | −27.276666 | 327,944.18045 | −8.3175 × 10−5 | 1.000 |
| Age group * With or without psychiatric history * Sex: | ||||
| (Children and adolescents − Young children) * (Clinical setting − School setting) * (Male − Female) | −2.708050 | 267,765.30179 | −1.0114 × 10−5 | 1.000 |
| (Adults − Young children) * (Clinical setting − School setting) * (Male − Female) | −27.094345 | 327,944.18044 | −8.2619 × 10−5 | 1.000 |
| Age group * DSM-5 severity level of ASD * Sex: | ||||
| (Children and adolescents − Young children) ✻ (Level 2 − Level 1) * (Male − Female) | −0.040822 | 1.47573 | −0.027662 | 0.978 |
| (Adults − Young children) * (Level 2 − Level 1) * (Male − Female) | −0.628609 | 267,765.30227 | −2.3476 × 10−6 | 1.000 |
| (Children and adolescents − Young children) * (Level 3 − Level 1) * (Male − Female) | −2.420368 | 1.60035 | −1.512402 | 0.130 |
| (Adults − Young children) * (Level 3 − Level 1) * (Male − Female) | 0.693147 | 267,765.30214 | 2.5886 × 10−6 | 1.000 |
| (Children and adolescents − Young children) * (No ASD − Level 1) * (Male − Female) | −1.540445 | 1.24743 | −1.234894 | 0.217 |
| (Adults − Young children) * (No ASD − Level 1) * (Male − Female) | −51.192957 | 267,765.30216 | −1.9119 × 10−4 | 1.000 |
| With or without psychiatric history * DSM-5 severity level of ASD * Sex: | ||||
| (Clinical setting − School setting) * (Level 2 − Level 1) * (Male − Female) | 23.287682 | 189,338.66069 | 1.2299 × 10−4 | 1.000 |
| (Clinical setting − School setting) * (Level 3 − Level 1) * (Male − Female) | −0.207639 | 1.68135 | −0.123496 | 0.902 |
| (Clinical setting − School setting) * (No ASD − Level 1) * (Male − Female) | −1.463255 | 1.51658 | −0.964842 | 0.335 |
| Age group * With or without psychiatric history * DSM-5 severity level of ASD * Sex: | ||||
| (Children and adolescents − Young children) * (Clinical setting − School setting) * (Level 2 − Level 1) * (Male − Female) | −24.568616 | 327,944.18010 | −7.4917 × 10−5 | 1.000 |
| (Adults − Young children) * (Clinical setting − School setting) * (Level 2 − Level 1) * (Male − Female) | −23.287682 | 500,943.01009 | −4.6488 × 10−5 | 1.000 |
| (Children and adolescents − Young children) * (Clinical setting − School setting) * (Level 3 − Level 1) * (Male − Female) | 3.726620 | 267,765.30179 | 1.3917 × 10−5 | 1.000 |
| (Adults − Young children) * (Clinical setting − School setting) * (Level 3 − Level 1) * (Male − Female) | −0.485508 | 463,783.10756 | −1.0468 × 10−6 | 1.000 |
| (Children and adolescents − Young children) * (Clinical setting − School setting) * (No ASD − Level 1) * (Male − Female) | 2.926739 | 267,765.30179 | 1.0930 × 10−5 | 1.000 |
| (Adults − Young children) * (Clinical setting − School setting) * (No ASD − Level 1) * (Male − Female) | 52.068426 | 463,783.10754 | 1.1227 × 10−4 | 1.000 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Alasmari, M.; Alduais, A.; Qasem, F.; Almaghlouth, S.; AlAmri, L. Examining Language, Speech and Behaviour Characteristics: A Cross-Sectional Study in Saudi Arabia Using the Arabic Version of Gilliam Autism Rating Scale-Third Edition. Children 2024, 11, 472. https://doi.org/10.3390/children11040472
Alasmari M, Alduais A, Qasem F, Almaghlouth S, AlAmri L. Examining Language, Speech and Behaviour Characteristics: A Cross-Sectional Study in Saudi Arabia Using the Arabic Version of Gilliam Autism Rating Scale-Third Edition. Children. 2024; 11(4):472. https://doi.org/10.3390/children11040472
Chicago/Turabian StyleAlasmari, Muhammad, Ahmed Alduais, Fawaz Qasem, Shrouq Almaghlouth, and Lujain AlAmri. 2024. "Examining Language, Speech and Behaviour Characteristics: A Cross-Sectional Study in Saudi Arabia Using the Arabic Version of Gilliam Autism Rating Scale-Third Edition" Children 11, no. 4: 472. https://doi.org/10.3390/children11040472