
Effects of Structured Physical Activity on Motor Fitness in Preschool Children

 , and
, and 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Experimental Design
2.2. Subjects
2.2.1. Anthropometric Assessment
2.2.2. Assessment of Motor Fitness
2.2.3. Experimental Intervention
2.3. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Biddle, S.J.; Asare, M. Physical activity and mental health in children and adolescents: A review of reviews. Br. J. Sports Med. 2011, 45, 886–895. [Google Scholar] [CrossRef] [PubMed]
- Janssen, I.; LeBlanc, A.G. Systematic review of the health benefits of physical activity and fitness in school-aged children and youth. Int. J. Behav. Nutr. Phys. Act. 2010, 7, 40. [Google Scholar] [CrossRef] [PubMed]
- Fjørtoft, I. Motor fitness in pre-primary school children: The EUROFIT motor fitness test explored on 5–7-year-old children. Pediatr. Exerc. Sci. 2000, 12, 424–436. [Google Scholar] [CrossRef]
- Malambo, C.; Nová, A.; Clark, C.; Musálek, M. Associations between fundamental movement skills, physical fitness, motor competency, physical activity, and executive functions in pre-school age children: A systematic review. Children 2022, 9, 1059. [Google Scholar] [CrossRef] [PubMed]
- Bull, F.C.; Al-Ansari, S.S.; Biddle, S.; Borodulin, K.; Buman, M.P.; Cardon, G.; Carty, C.; Chaput, J.-P.; Chastin, S.; Chou, R. World Health Organization 2020 guidelines on physical activity and sedentary behaviour. Br. J. Sports Med. 2020, 54, 1451–1462. [Google Scholar] [CrossRef] [PubMed]
- Farooq, A.; Martin, A.; Janssen, X.; Wilson, M.G.; Gibson, A.M.; Hughes, A.; Reilly, J.J. Longitudinal changes in moderate-to-vigorous-intensity physical activity in children and adolescents: A systematic review and meta-analysis. Obes. Rev. 2020, 21, e12953. [Google Scholar] [CrossRef] [PubMed]
- Timmons, B.W.; Naylor, P.-J.; Pfeiffer, K.A. Physical activity for preschool children—How much and how? Appl. Physiol. Nutr. Metab. 2007, 32, S122–S134. [Google Scholar] [CrossRef] [PubMed]
- García-Hermoso, A.; Alonso-Martinez, A.M.; Ramírez-Vélez, R.; Izquierdo, M. Effects of exercise intervention on health-related physical fitness and blood pressure in preschool children: A systematic review and meta-analysis of randomized controlled trials. Sports Med. 2020, 50, 187–203. [Google Scholar] [CrossRef] [PubMed]
- Barreiro, J.A.; Howard, R. Incorporating unstructured free play into organized sports. Strength Cond. J. 2017, 39, 11–19. [Google Scholar] [CrossRef]
- Abusleme-Allimant, R.; Hurtado-Almonacid, J.; Reyes-Amigo, T.; Yáñez-Sepúlveda, R.; Cortés-Roco, G.; Arroyo-Jofré, P.; Páez-Herrera, J. Effects of Structured and Unstructured Physical Activity on Gross Motor Skills in Preschool Students to Promote Sustainability in the Physical Education Classroom. Sustainability 2023, 15, 10167. [Google Scholar] [CrossRef]
- Tan, J.S.; Nonis, K.; Chan, L.Y. The Effect of Traditional Games and Free play on Motor Skills of Preschool Children. Int. J. Child. Couns. Spec. Educ. 2020, 1, 204–223. [Google Scholar] [CrossRef]
- Palmer, K.K.; Matsuyama, A.L.; Robinson, L.E. Impact of structured movement time on preschoolers’ physical activity engagement. Early Child. Educ. J. 2017, 45, 201–206. [Google Scholar] [CrossRef]
- Frank, M.L.; Flynn, A.; Farnell, G.S.; Barkley, J.E. The differences in physical activity levels in preschool children during free play recess and structured play recess. J. Exerc. Sci. Fit. 2018, 16, 37–42. [Google Scholar] [CrossRef]
- Moghaddaszadeh, A.; Belcastro, A.N. Guided active play promotes physical activity and improves fundamental motor skills for school-aged children. J. Sports Sci. Med. 2021, 20, 86. [Google Scholar] [PubMed]
- Popović, B.; Cvetković, M.; Mačak, D.; Šćepanović, T.; Čokorilo, N.; Belić, A.; Trajković, N.; Andrašić, S.; Bogataj, Š. Nine months of a structured multisport program improve physical fitness in preschool children: A quasi-experimental study. Int. J. Environ. Res. Public Health 2020, 17, 4935. [Google Scholar] [CrossRef]
- Martínez-Vizcaíno, V.; Pozuelo-Carrascosa, D.P.; García-Prieto, J.C.; Cavero-Redondo, I.; Solera-Martínez, M.; Garrido-Miguel, M.; Díez-Fernández, A.; Ruiz-Hermosa, A.; Sánchez-López, M. Effectiveness of a school-based physical activity intervention on adiposity, fitness and blood pressure: MOVI-KIDS study. Br. J. Sports Med. 2020, 54, 279–285. [Google Scholar] [CrossRef] [PubMed]
- Roach, L.; Keats, M. Skill-based and planned active play versus free-play effects on fundamental movement skills in preschoolers. Percept. Mot. Ski. 2018, 125, 651–668. [Google Scholar] [CrossRef]
- Stupar, D.M.; Fratrić, F.F.; Nešić, M.; Rubin, P.; Međedovic, B. The effects of an experimental program of speed development on preschool children. Facta Univ. Ser. Phys. Educ. Sport 2015, 13, 139–148. [Google Scholar]
- Foulkes, J.; Knowles, Z.; Fairclough, S.; Stratton, G.; O’dwyer, M.; Ridgers, N.; Foweather, L. Effect of a 6-week active play intervention on fundamental movement skill competence of preschool children: A cluster randomized controlled trial. Percept. Mot. Ski. 2017, 124, 393–412. [Google Scholar] [CrossRef]
- Tortella, P.; Haga, M.; Lorås, H.; Fumagalli, G.F.; Sigmundsson, H. Effects of Free Play and Partly Structured Playground Activity on Motor Competence in Preschool Children: A Pragmatic Comparison Trial. Int. J. Environ. Res. Public Health 2022, 19, 7652. [Google Scholar] [CrossRef]
- Mačak, D.; Popović, B.; Babić, N.; Cadenas-Sanchez, C.; Madić, D.M.; Trajković, N. The effects of daily physical activity intervention on physical fitness in preschool children. J. Sports Sci. 2022, 40, 146–155. [Google Scholar] [CrossRef] [PubMed]
- Temmerman, N. An investigation of the music activity preferences of pre-school children. Br. J. Music Educ. 2000, 17, 51–60. [Google Scholar] [CrossRef]
- Marković, Ž.; Džinović-Kojić, D.; Ignjatović, A.; Šekeljić, G.; Stanković, S. The influence of different content on the motor engagement of preschoolers. Facta Univ. Ser. Phys. Educ. Sport 2017, 14, 371–380. [Google Scholar]
- van Hyfte, E.; Vercruysse, S.; Warlop, G.; Lenoir, M. A Physical Education Program Based Upon an Obstacle Course Positively Affects Motor Competence in 6-to 7-Year-Old Children: A Pilot Study. J. Teach. Phys. Educ. 2021, 41, 610–621. [Google Scholar] [CrossRef]
- Granacher, U.; Muehlbauer, T.; Maestrini, L.; Zahner, L.; Gollhofer, A. Can balance training promote balance and strength in prepubertal children? J. Strength Cond. Res. 2011, 25, 1759–1766. [Google Scholar] [CrossRef] [PubMed]
- Bala, G.; Popovic, B. Motor skills of preschool children. In Anthropological Characteristics and Abilities of Preschool Children; University of Novi Sad, Faculty of Physical Education: Novi Sad, Serbia, 2007; pp. 101–151. [Google Scholar]
- Džinović-Kojić, D. Fizičko Vaspitanje Predškolskog Deteta: (Metodički Priručnik za Studente i Vaspitače); Drakslar Partner: Beograd, 2002. [Google Scholar]
- Weir, J.P.; Vincent, W.J. Statistics in Kinesiology; Human Kinetics Publishers: Hanover, PA, USA, 2020. [Google Scholar]
- Field, A. Discovering Statistics Using IBM SPSS Statistics; Sage: Newcastle upon Tyne, UK, 2013. [Google Scholar]
- Cohen, J. Statistical Power Analysis for the Behavioral Sciences; Academic Press: Cambridge, MA, USA, 2013. [Google Scholar]
- Sawilowsky, S.S. New effect size rules of thumb. J. Mod. Appl. Stat. Methods 2009, 8, 26. [Google Scholar] [CrossRef]
- Hair, J.F.; Anderson, R.; Tatham, R. WC Black Multivariate Data Analysis; Prentice Hall: Upper Saddle River, NJ, USA, 1998. [Google Scholar]
- Revie, G.; Larkin, D. Task-specific intervention with children reduces movement problems. Adapt. Phys. Act. Q. 1993, 10, 29–41. [Google Scholar] [CrossRef]
- Nimphius, S.; Callaghan, S.J.; Bezodis, N.E.; Lockie, R.G. Change of direction and agility tests: Challenging our current measures of performance. Strength Cond. J. 2018, 40, 26–38. [Google Scholar] [CrossRef]
- Waters, E.; Silva-Sanigorski, A.d.; Burford, B.J.; Brown, T.; Campbell, K.J.; Gao, Y.; Armstrong, R.; Prosser, L.; Summerbell, C.D. Interventions for preventing obesity in children. Sao Paulo Med. J. 2014, 132, 128–129. [Google Scholar] [CrossRef]
- Bläsing, B.; Schack, T. Mental representation of spatial movement parameters in dance. Spat. Cogn. Comput. 2012, 12, 111–132. [Google Scholar] [CrossRef]
- Gilbert, A.G. Brain-Compatible Dance Education, 2nd ed.; Human Kinetics: Hanover, PA, USA, 2018. [Google Scholar]


{kind=link}
{kind=link}
{kind=link}
| Monday | Wednesday | Friday |
|---|---|---|
| Tag game (5 min) Warm-up exercises (5 min) | Various movements with changeable speed (5 min) Warm-up exercises (5 min) | Musical game (5 min) |
| Relay race (20 min) | Obstacle course (20 min) | Dance choreography (25 min) |
| Cool-down (5 min) | Cool-down (5 min) | Cool-down (5 min) |
| SMA | FRP | p (ANCOVA) | F (ANCOVA) | |||
|---|---|---|---|---|---|---|
| Pre | Post | Pre | Post | |||
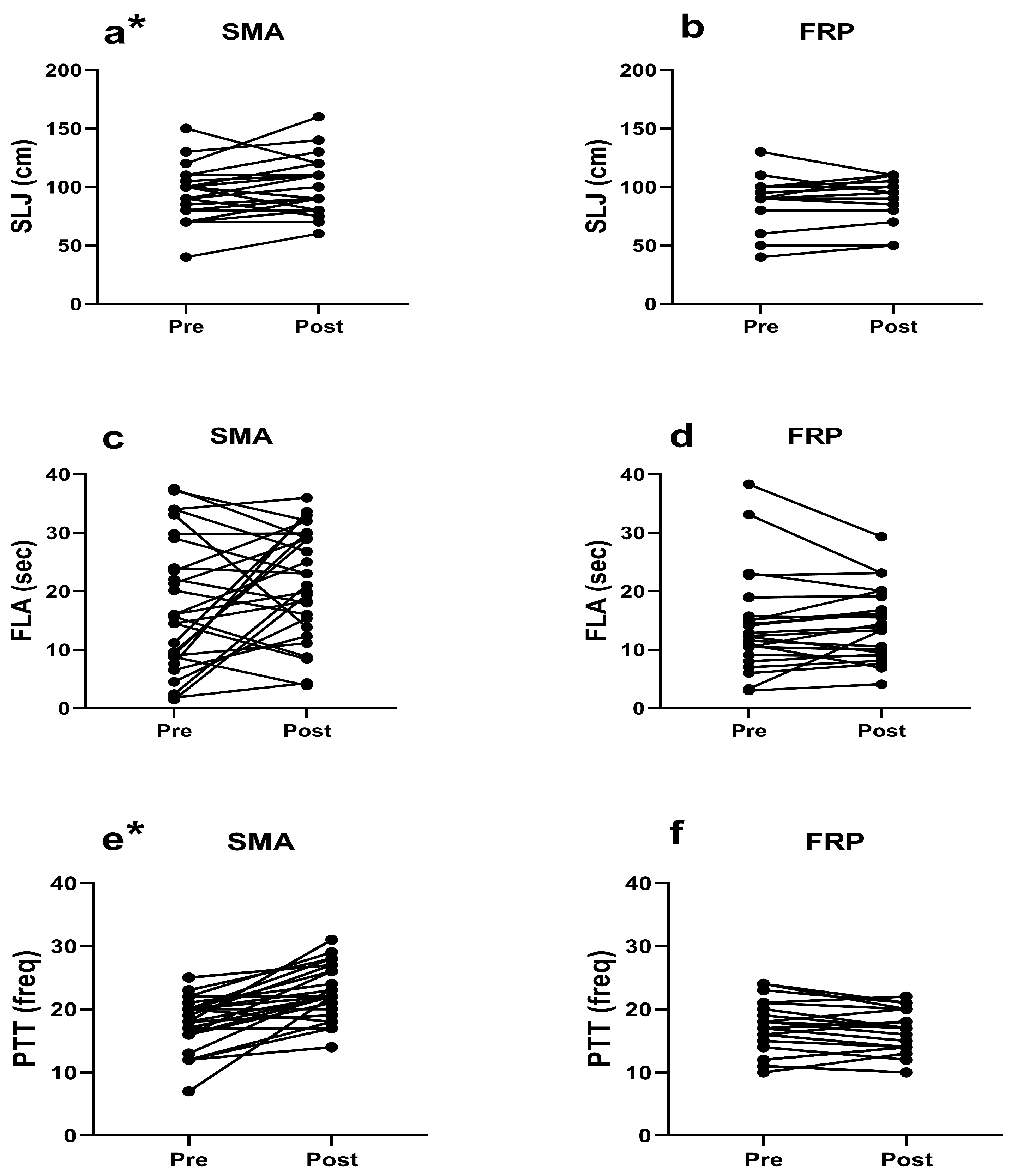
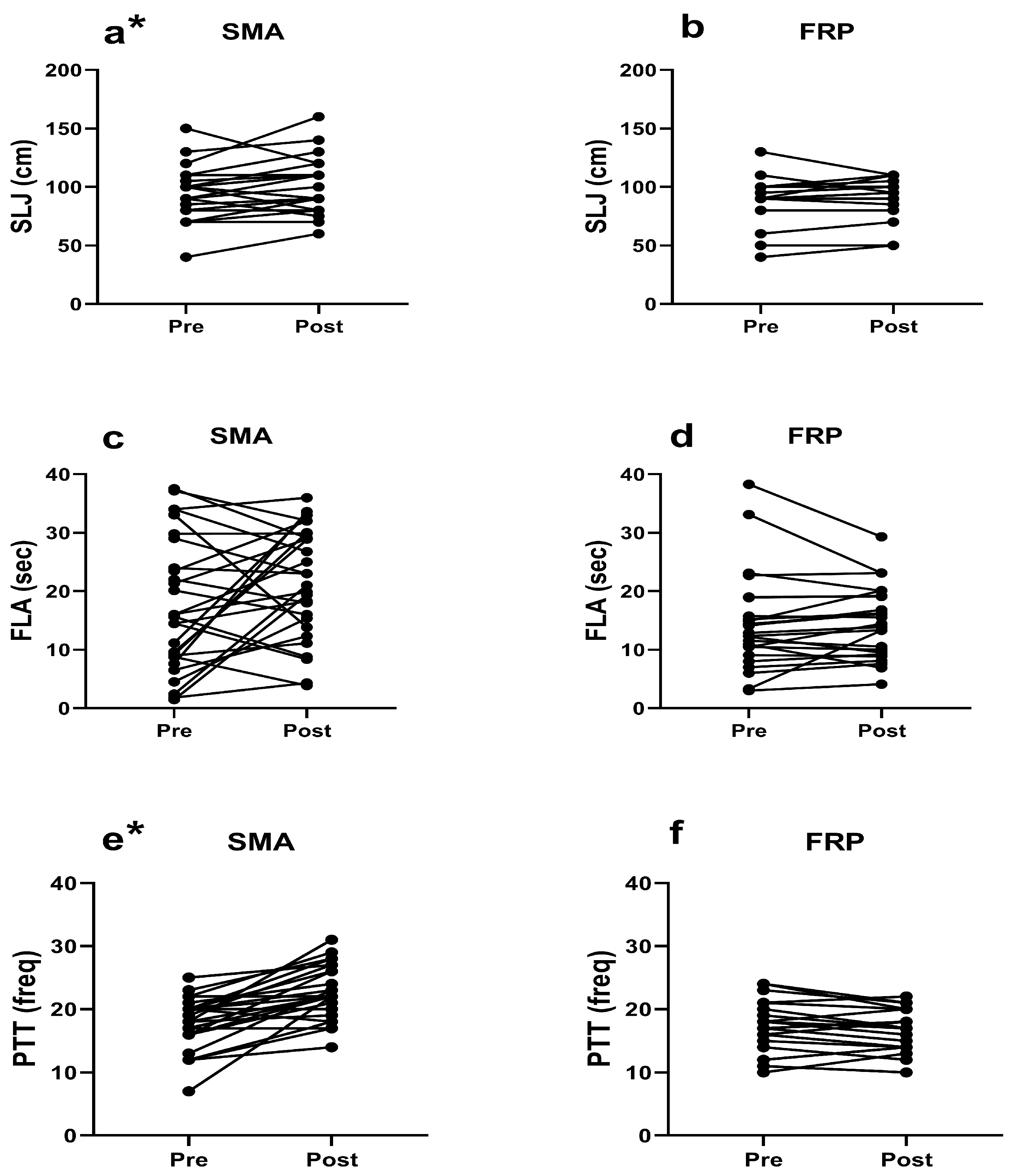
| SLJ | 94.11 ± 21.35 | 100.58 ± 22.69 | 89.40 ± 20.02 | 90.60 ± 17.81 | 0.052 | 3.966 |
| FLA | 17.65 ± 11.29 | 21.49 ± 9.34 | 14.44 ± 8.21 | 14.60 ± 6.01 | 0.005 * | 8.717 |
| PTT | 17.96 ± 3.95 | 23.25 ± 4.42 | 16.76 ± 4.04 | 16.28 ± 3.37 | 0.000 * | 52.414 |
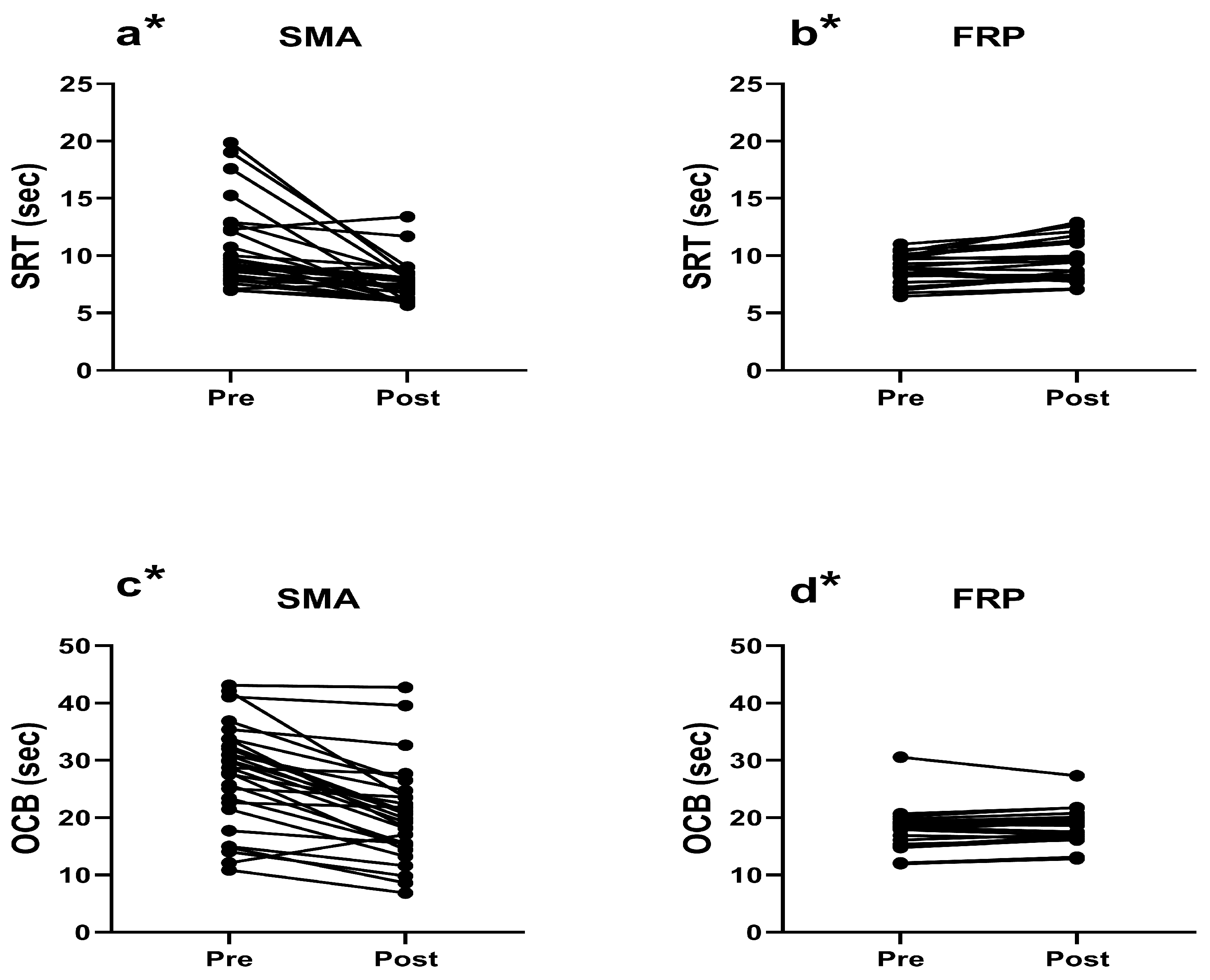
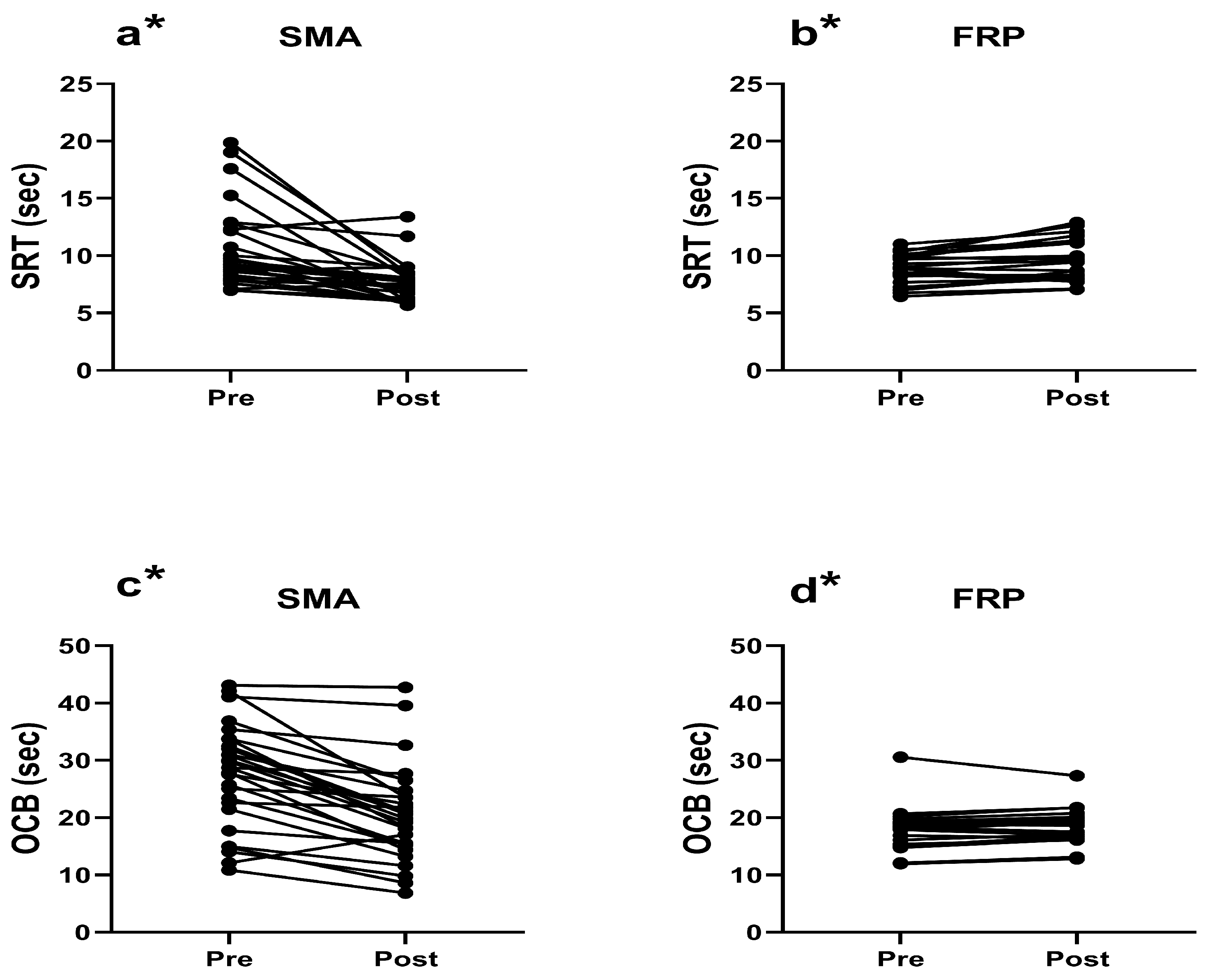
| SRT | 10.54 ± 3.55 # | 3.55± 1.73 | 8.86 ± 1.30 | 9.54 ± 1.79 | 0.000 * | 24.417 |
| OCB | 28.04 ± 10.36 # | 21.18 ± 9.96 | 17.66 ± 3.83 | 18.17 ± 3.27 | 0.000 * | 21.709 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kojić, F.; Arsenijević, R.; Grujić, G.; Toskić, L.; Šimenko, J. Effects of Structured Physical Activity on Motor Fitness in Preschool Children. Children 2024, 11, 433. https://doi.org/10.3390/children11040433
Kojić F, Arsenijević R, Grujić G, Toskić L, Šimenko J. Effects of Structured Physical Activity on Motor Fitness in Preschool Children. Children. 2024; 11(4):433. https://doi.org/10.3390/children11040433
Chicago/Turabian StyleKojić, Filip, Radenko Arsenijević, Gabrijela Grujić, Lazar Toskić, and Jožef Šimenko. 2024. "Effects of Structured Physical Activity on Motor Fitness in Preschool Children" Children 11, no. 4: 433. https://doi.org/10.3390/children11040433
APA StyleKojić, F., Arsenijević, R., Grujić, G., Toskić, L., & Šimenko, J. (2024). Effects of Structured Physical Activity on Motor Fitness in Preschool Children. Children, 11(4), 433. https://doi.org/10.3390/children11040433