


Study on Nocturnal Infant Crying Evaluation (NICE) and Reflux Disease (RED)


 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Population
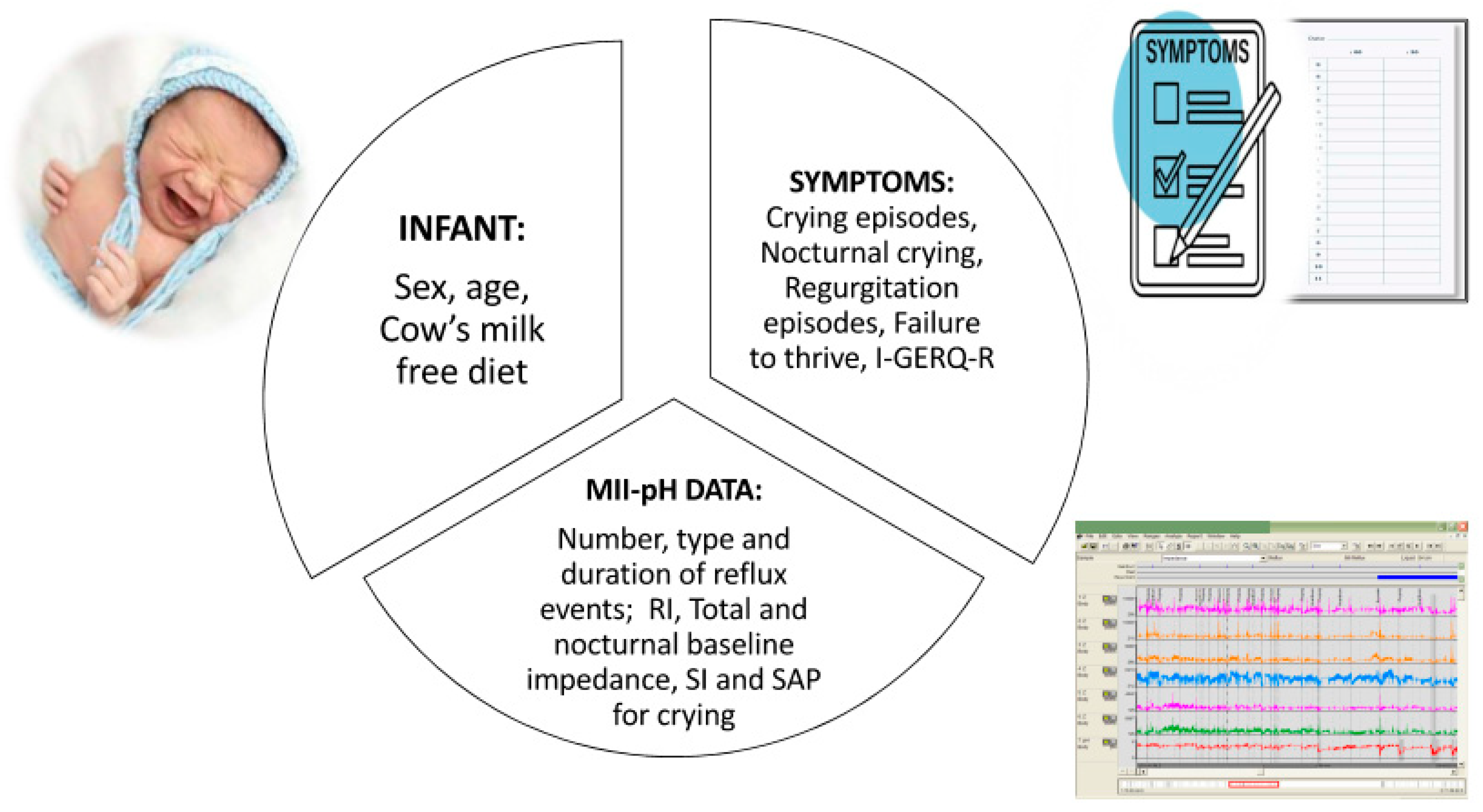
2.2. Procedures
2.2.1. Infant Symptom Recording
2.2.2. GERD Investigation
2.2.3. Interpretation of MII-pH Results
2.2.4. Treatment
2.3. Statistical Analysis
Sample Size
3. Results
3.1. Symptoms and GERD
3.2. Results of Laryngoscopy and Polysomnography
3.3. Effect of Treatment and Follow-Up Data
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Vandenplas, Y.; Rudolph, C.D.; Di Lorenzo, C.; Hassall, E.; Liptak, G.; Mazur, L.; Sondheimer, J.; Staiano, A.; Thomson, M.; Veereman-Wauters, G.; et al. Pediatric gastroesophageal reflux clinical practice guidelines: Joint recommendations of the North American Society of Pediatric Gastroenterology, Hepatology, and Nutrition and the European Society of Pediatric Gastroenterology, Hepatology, and Nutrition. J. Pediatr. Gastroenterol. Nutr. 2009, 49, 498–547. [Google Scholar] [CrossRef]
- Rosen, R.; Vandenplas, Y.; Singendonk, M.; Cabana, M.; DiLorenzo, C.; Gottrand, F.; Gupta, S.; Langendam, M.; Staiano, A.; Thapar, N.; et al. Pediatric Gastroesophageal Reflux Clinical Practice Guidelines: Joint Recommendations of the North American Society for Pediatric Gastroenterology, Hepatology, and Nutrition and the European Society for Pediatric Gastroenterology, Hepatology, and Nutrition. J. Pediatr. Gastroenterol. Nutr. 2018, 66, 516–554. [Google Scholar] [CrossRef]
- Sherman, P.M.; Hassall, E.; Fagundes-Neto, U.; Gold, B.D.; Kato, S.; Koletzko, S.; Orenstein, S.; Rudolph, C.; Vakil, N.; Vandenplas, Y. A global, evidence-based consensus on the definition of gastroesophageal reflux disease in the pediatric population. Am. J. Gastroenterol. 2009, 104, 1278–1295. [Google Scholar] [CrossRef]
- National Institute for Health and Care Excellence (NICE). GORD: Recognition, Diagnosis and Management in Children and Young People. (Clinical Guideline 193). 2015. Available online: http://www.nice.org.uk/guidance/NG1 (accessed on 30 April 2015).
- Salvatore, S.; Abkari, A.; Cai, W.; Catto-Smith, A.; Cruchet, S.; Gottrand, F.; Hegar, B.; Lifschitz, C.; Ludwig, T.; Shah, N.; et al. Review shows that parental reassurance and nutritional advice help to optimise the management of functional gastrointestinal disorders in infants. Acta Paediatr. 2018, 107, 1512–1520. [Google Scholar] [CrossRef]
- Heine, R.G.; Jaquiery, A.; Lubitz, L.; Cameron, D.J.; Catto-Smith, A.G. Role of gastro-oesophageal reflux in infant irritability. Arch. Dis. Child. 1995, 73, 121–125. [Google Scholar] [CrossRef]
- Tighe, M.P.; Andrews, E.; Liddicoat, I.; Afzal, N.A.; Hayen, A.; Beattie, R.M. Pharmacological treatment of gastro-oesophageal reflux in children. Cochrane Database Syst. Rev. 2023, 8, CD008550. [Google Scholar]
- Gieruszczak-Białek, D.; Konarska, Z.; Skórka, A.; Vandenplas, Y.; Szajewska, H. No effect of proton pump inhibitors on crying and irritability in infants: Systematic review of randomized controlled trials. J. Pediatr. 2015, 166, 767–770.e3. [Google Scholar] [CrossRef]
- Salvatore, S.; Pagliarin, F.; Huysentruyt, K.; Bosco, A.; Fumagalli, L.; Van De Maele, K.; Agosti, M.; Vandenplas, Y. Distress in Infants and Young Children: Don’t Blame Acid Reflux. J. Pediatr. Gastroenterol. Nutr. 2020, 71, 465–469. [Google Scholar] [CrossRef]
- Levy, E.I.; Salvatore, S.; Vandenplas, Y.; de Winter, J.P. Prescription of acid inhibitors in infants: An addiction hard to break. Eur. J. Pediatr. 2020, 179, 1957–1961. [Google Scholar] [CrossRef]
- Kołodziej, M.; Gieruszczak-Białek, D.; Pieścik-Lech, M.; Skórka, A.; Vandenplas, Y.; Szajewska, H. Overuse continues despite no new evidence on the efficacy of proton pump inhibitors for crying and irritability in infants. Acta Paediatr. 2022, 111, 682–683. [Google Scholar] [CrossRef]
- Malchodi, L.; Wagner, K.; Susi, A.; Gorman, G.; Hisle-Gorman, E. Early Acid Suppression Therapy Exposure and Fracture in Young Children. Pediatrics 2019, 144, e20182625. [Google Scholar] [CrossRef]
- Orel, R.; Benninga, M.A.; Broekaert, I.J.; Gottrand, F.; Papadopoulou, A.; Ribes-Koninckx, C.; Thomson, M.; Wilschanski, M.; Thapar, N. Drugs in Focus: Proton Pump Inhibitors. J. Pediatr. Gastroenterol. Nutr. 2021, 72, 645–653. [Google Scholar] [CrossRef]
- Dipasquale, V.; Cicala, G.; Spina, E.; Romano, C. A Narrative Review on Efficacy and Safety of Proton Pump Inhibitors in Children. Front. Pharmacol. 2022, 13, 839972. [Google Scholar] [CrossRef]
- Wolf, E.R.; Sabo, R.T.; Lavallee, M.; French, E.; Schroeder, A.R.; Huffstetler, A.N.; Schefft, M.; Krist, A.H. Overuse of Reflux Medications in Infants. Pediatrics 2023, 151, e2022058330. [Google Scholar] [CrossRef]
- Orenstein, S.R.; Hassall, E.; Furmaga-Jablonska, W.; Atkinson, S.; Raanan, M. Multicenter, double-blind, randomized, placebo-controlled trial assessing the efficacy and safety of proton pump inhibitor lansoprazole in infants with symptoms of gastroesophageal reflux disease. J. Pediatr. 2009, 154, 514–520.e4. [Google Scholar] [CrossRef]
- Lee, A.L.H.; Varjavandi, V.; Lemberg, D.A.; Ooi, C.Y.; Gupta, N.; Krishnan, U. Does Combined Multichannel Intraluminal Impedance and pH (MII-pH) Testing Improve Clinical Outcomes in Children with Gastroesophageal Reflux Disease? J. Pediatr. Gastroenterol. Nutr. 2020, 71, 596–603. [Google Scholar] [CrossRef]
- Salvatore, S.; Ripepi, A.; Huysentruyt, K.; van de Maele, K.; Nosetti, L.; Agosti, M.; Salvatoni, A.; Vandenplas, Y. The Effect of Alginate in Gastroesophageal Reflux in Infants. Paediatr. Drugs. 2018, 20, 575–583. [Google Scholar] [CrossRef]
- Kleinman, L.; Rothman, M.; Strauss, R.; Orenstein, S.R.; Nelson, S.; Vandenplas, Y.; Cucchiara, S.; Revicki, D.A. The infant gastroesophageal reflux questionnaire revised: Development and validation as an evaluative instrument. Clin. Gastroenterol. Hepatol. 2006, 4, 588–596. [Google Scholar] [CrossRef]
- Salvatore, S.; Hauser, B.; Vandemaele, K.; Novario, R.; Vandenplas, Y. Gastroesophageal reflux disease in infants: How much is predictable with questionnaires, pH-metry, endoscopy and histology? J. Pediatr. Gastroenterol. Nutr. 2005, 40, 210–215. [Google Scholar]
- Gatrad, A.R.; Sheikh, A. Persistent crying in babies. BMJ 2004, 328, 330. [Google Scholar] [CrossRef]
- Akhnikh, S.; Engelberts, A.C.; van Sleuwen, B.E.; L’Hoir, M.P.; Benninga, M.A. The excessively crying infant: Etiology and treatment. Pediatr. Ann. 2014, 43, e69–e75. [Google Scholar] [CrossRef]
- Muller, I.; Ghio, D.; Mobey, J.; Jones, H.; Hornsey, S.; Dobson, A.; Maund, E.; Santer, M. Parental perceptions and experiences of infant crying: A systematic review and synthesis of qualitative research. J. Adv. Nurs. 2023, 79, 403–417. [Google Scholar] [CrossRef]
- Whittall, H.; Kahn, M.; Pillion, M.; Gradisar, M. Parents matter: Barriers and solutions when implementing behavioural sleep interventions for infant sleep problems. Sleep Med. 2021, 84, 244–252. [Google Scholar] [CrossRef]
- Gordon, M.; Gohil, J.; Banks, S.S. Parent training programmes for managing infantile colic. Cochrane Database Syst. Rev. 2019, 12, CD012459. [Google Scholar] [CrossRef]
- Montazeri, R.; Hasanpour, S.; Mirghafourvand, M.; Gharehbaghi, M.M.; Tehrani, M.M.G.; Rezaei, S.M. The effect of behavioral therapy based counseling with anxious mothers on their infants’ colic: A randomized controlled clinical trial. BMC Pediatr. 2022, 22, 645. [Google Scholar] [CrossRef]
- Byars, K.C.; Yolton, K.; Rausch, J.; Lanphear, B.; Beebe, D.W. Prevalence, patterns, and persistence of sleep problems in the first 3 years of life. Pediatrics 2012, 129, e276–e284. [Google Scholar] [CrossRef]
- Thabet, F.; Tabarki, B. Common sleep disorders in children: Assessment and treatment. Neurosciences 2023, 28, 85–90. [Google Scholar] [CrossRef]
- Wenzl, T.G.; Benninga, M.A.; Loots, C.M.; Salvatore, S.; Vandenplas, Y.; ESPGHAN EURO-PIG Working Group. Indications, methodology, and interpretation of combined esophageal impedance-pH monitoring in children: ESPGHAN EURO-PIG standard protocol. J. Pediatr. Gastroenterol. Nutr. 2012, 55, 230–234. [Google Scholar] [CrossRef]
- Quitadamo, P.; Tambucci, R.; Mancini, V.; Cristofori, F.; Baldassarre, M.; Pensabene, L.; Francavilla, R.; Di Nardo, G.; Caldaro, T.; Rossi, P.; et al. Esophageal pH-impedance monitoring in children: Position paper on indications, methodology and interpretation by the SIGENP working group. Dig. Liver Dis. 2019, 51, 1522–1536. [Google Scholar] [CrossRef] [PubMed]
- Cresi, F.; Cester, E.A.; Salvatore, S.; De Rose, D.U.; Ripepi, A.; Magistà, A.M.; Fontana, C.; Maggiora, E.; Coscia, A.; Francavilla, R.; et al. Multichannel Intraluminal Impedance and pH Monitoring: A Step towards Pediatric Reference Values. J. Neurogastroenterol. Motil. 2020, 26, 370–377. [Google Scholar] [CrossRef] [PubMed]
- Olsen, E.M.; Petersen, J.; Skovgaard, A.M.; Weile, B.; Jørgensen, T.; Wright, C.M. Failure to thrive: The prevalence and concurrence of anthropometric criteria in a general infant population. Arch. Dis. Child. 2007, 92, 109–114. [Google Scholar] [CrossRef] [PubMed]
- Shields, B.; Wacogne, I.; Wright, C.M. Weight faltering and failure to thrive in infancy and early childhood. BMJ 2012, 345, e5931. [Google Scholar] [CrossRef] [PubMed]
- Strobel, C.T.; Byrne, W.J.; Ament, M.E.; Euler, A.R. Correlation of esophageal lengths in children with height: Application to the tuttle test without prior esophageal manometry. J. Pediatr. 1979, 94, 81–84. [Google Scholar] [CrossRef] [PubMed]
- Salvatore, S.; Hauser, B.; Devreker, T.; Arrigo, S.; Marino, P.S.; Citro, C.; Salvatoni, A.; Vandenplas, Y. Esophageal Impedance and Esophagitis in Children: Any Correlation? J. Pediatr. Gastroenterol. Nutr. 2009, 49, 566–570. [Google Scholar] [CrossRef] [PubMed]
- Pilic, D.; Hankel, S.; Koerner-Rettberg, C.; Hamelmann, E.; Schmidt-Choudhury, A. The role of baseline impedance as a marker of mucosal integrity in children with gastro esophageal reflux disease. Scand. J. Gastroenterol. 2013, 48, 785–793. [Google Scholar] [CrossRef] [PubMed]
- Salvatore, S.; Salvatoni, A.; Van Steen, K.; Ummarino, D.; Hauser, B.; Vandenplas, Y. Behind the (impedance) baseline in children. Dis. Esophagus. 2014, 27, 726–731. [Google Scholar] [CrossRef] [PubMed]
- Tambucci, R.; Thapar, N.; Saliakellis, E.; Pescarin, M.; Quitadamo, P.; Cristofori, F.; Lindley, K.J.; Borrelli, O. Clinical relevance of esophageal baseline impedance measurement: Just an innocent bystander. J. Pediatr. Gastroenterol. Nutr. 2015, 60, 776–782. [Google Scholar] [CrossRef] [PubMed]
- Patel, A.; Wang, D.; Sainani, N.; Sayuk, G.S.; Gyawali, C.P. Distal mean nocturnal baseline impedance on pH-impedance monitoring predicts reflux burden and symptomatic outcome in gastro-oesophageal reflux disease. Aliment. Pharmacol. Ther. 2016, 44, 890–898. [Google Scholar] [CrossRef] [PubMed]
- Rengarajan, A.; Savarino, E.; Della Coletta, M.; Ghisa, M.; Patel, A.; Gyawali, C.P. Mean Nocturnal Baseline Impedance Correlates with Symptom Outcome When Acid Exposure Time Is Inconclusive on Esophageal Reflux Monitoring. Clin. Gastroenterol. Hepatol. 2020, 18, 589–595. [Google Scholar] [CrossRef] [PubMed]
- Wu, Y.; Guo, Z.; Zhang, C.; Zhan, Y. Mean nocturnal baseline impedance, a novel metric of multichannel intraluminal impedance-pH monitoring in diagnosing gastroesophageal reflux disease. Therap. Adv. Gastroenterol. 2022, 15, 17562848221105195. [Google Scholar] [CrossRef]
- Salvatore, S.; Salvatoni, A.; Van Berkel, M.; Van Steen, K.; Unmarino, D.; Ghanma, A.; Hauser, B.; Vandenplas, Y. Esophageal impedance baseline is age dependent. J. Pediatr. Gastroenterol. Nutr. 2013, 57, 506–513. [Google Scholar] [CrossRef] [PubMed]
- Hawkins, D.B.; Clark, R.W. Flexible laryngoscopy in neonates, infants, and young children. Ann. Otol. Rhinol. Laryngol. 1987, 96 Pt 1, 81–85. [Google Scholar] [CrossRef]
- Horne, R.S.; Nixon, G.M. The role of physiological studies and apnoea monitoring in infants. Paediatr. Respir. Rev. 2014, 15, 312–318. [Google Scholar] [CrossRef] [PubMed]
- Douglas, P.; Hill, P. Managing infants who cry excessively in the first few months of life. BMJ 2011, 343, d7772. [Google Scholar] [CrossRef] [PubMed]
- Douglas, P.S. Excessive crying and gastro-oesophageal reflux disease in infants: Misalignment of biology and culture. Med. Hypotheses. 2005, 64, 887–898. [Google Scholar] [CrossRef] [PubMed]
- Sung, V. Infantile colic. Aust. Prescr. 2018, 41, 105–110. [Google Scholar] [CrossRef] [PubMed]
- Steutel, N.F.; Zeevenhooven, J.; Scarpato, E.; Vandenplas, Y.; Tabbers, M.M.; Staiano, A.; Benninga, M.A. Prevalence of Functional Gastrointestinal Disorders in European Infants and Toddlers. J. Pediatr. 2020, 221, 107–114. [Google Scholar] [CrossRef] [PubMed]
- Beser, O.F.; Cullu Cokugras, F.; Dogan, G.; Akgun, O.; Elevli, M.; Yilmazbas, P.; Ocal, M.; Bayrak, N.A.; Sezer Yamanel, R.G.; Bozaykut, A.; et al. The frequency of and factors affecting functional gastrointestinal disorders in infants that presented to tertiary care hospitals. Eur. J. Pediatr. 2021, 180, 2443–2452. [Google Scholar] [CrossRef] [PubMed]
- Vandenplas, Y.; Benninga, M.; Broekaert, I.; Falconer, J.; Gottrand, F.; Guarino, A.; Lifschitz, C.; Lionetti, P.; Orel, R.; Papadopoulou, A.; et al. Functional gastro-intestinal disorder algorithms focus on early recognition, parental reassurance and nutritional strategies. Acta Paediatr. 2016, 105, 244–252. [Google Scholar] [CrossRef]
- Reuter, A.; Silfverdal, S.A.; Lindblom, K.; Hjern, A. A systematic review of prevention and treatment of infant behavioural sleep problems. Acta Paediatr. 2020, 109, 1717–1732. [Google Scholar] [CrossRef]
- Sette, S.; Baumgartner, E.; Ferri, R.; Bruni, O. Predictors of sleep disturbances in the first year of life: A longitudinal study. Sleep Med. 2017, 36, 78–85. [Google Scholar] [CrossRef]
- Bruni, O.; Baumgartner, E.; Sette, S.; Ancona, M.; Caso, G.; Di Cosimo, M.E.; Mannini, A.; Ometto, M.; Pasquini, A.; Ulliana, A.; et al. Longitudinal study of sleep behavior in normal infants during the first year of life. J. Clin. Sleep Med. 2014, 10, 1119–1127. [Google Scholar] [CrossRef] [PubMed]
- Sadeh, A.; Juda-Hanael, M.; Livne-Karp, E.; Kahn, M.; Tikotzky, L.; Anders, T.F.; Calkins, S.; Sivan, Y. Low parental tolerance for infant crying: An underlying factor in infant sleep problems? J. Sleep Res. 2016, 25, 501–507. [Google Scholar] [CrossRef]
- Salvatore, S.; Hauser, B.; Vandenplas, Y. The natural course of gastro-oesophageal reflux. Acta Paediatr. 2004, 93, 1063–1069. [Google Scholar] [CrossRef]
- Singendonk, M.M.J.; Rexwinkel, R.; Steutel, N.F.; Gottrand, F.; McCall, L.; Orsagh-Yentis, D.K.; Rosen, R.; Strisciuglio, C.; Thapar, N.; Vandenplas, Y.; et al. Development of a Core Outcome Set for Infant Gastroesophageal Reflux Disease. J. Pediatr. Gastroenterol. Nutr. 2019, 68, 655–661. [Google Scholar] [CrossRef]
- Steutel, N.F.; Benninga, M.A.; Langendam, M.W.; Korterink, J.J.; Indrio, F.; Szajewska, H.; Tabbers, M.M. Developing a core outcome set for infant colic for primary, secondary and tertiary care settings: A prospective study. BMJ Open 2017, 7, e015418. [Google Scholar] [CrossRef]
- Ghaem, M.; Armstrong, K.L.; Trocki, O.; Cleghorn, G.J.; Patrick, M.K.; Shepherd, R.W. The sleep patterns of infants and young children with gastro-oesophageal reflux. J. Paediatr. Child Health 1998, 34, 160–163. [Google Scholar] [CrossRef] [PubMed]
- Harris, P.; Brockmann, P.; Muñoz, C.; Mobarec, S.; Mesa, T.; Sánchez, I. Alteraciones polisomnográficas en lactantes con reflujo gastroesofágico [Polysomnographic abnormalities in infants with gastroesophageal reflux]. Rev. Med. Chil. 2003, 131, 1143–1150. [Google Scholar] [CrossRef]
- Hegar, B.; Rantos, R.; Firmansyah, A.; De Schepper, J.; Vandenplas, Y. Natural evolution of infantile regurgitation versus the efficacy of thickened formula. J. Pediatr. Gastroenterol. Nutr. 2008, 47, 26–30. [Google Scholar] [CrossRef] [PubMed]
- Cresi, F.; Locatelli, E.; Maggiora, E.; Di Nicola, P.; Cester, E.; Sabatino, G.; Martano, C.; Giuliani, F.; Bertino, E. Relationship between sleep/wakefulness and gastroesophageal reflux in symptomatic newborns. J. Biol. Regul. Homeost. Agents 2012, 26 (Suppl. S3), 83–85. [Google Scholar]
- Machado, R.; Woodley, F.W.; Skaggs, B.; Di Lorenzo, C.; Splaingard, M.; Mousa, H. Gastroesophageal reflux causing sleep interruptions in infants. J. Pediatr. Gastroenterol. Nutr. 2013, 56, 431–435. [Google Scholar] [CrossRef] [PubMed]
- Sankaran, J.; Qureshi, A.H.; Woodley, F.; Splaingard, M.; Jadcherla, S.R. Effect of Severity of Esophageal Acidification on Sleep vs. Wake Periods in Infants Presenting with Brief Resolved Unexplained Events. J. Pediatr. 2016, 179, 42–48.e1. [Google Scholar] [CrossRef] [PubMed]
- Pappa, A.; Muschaweck, M.; Wenzl, T.G. Change of Sleep Stage during Gastroesophageal Reflux in Infants. Children 2023, 10, 836. [Google Scholar] [CrossRef] [PubMed]
- Aizlewood, E.G.; Jones, F.W.; Whatmough, R.M. Paediatric gastroesophageal reflux disease and parental mental health: Prevalence and predictors. Clin. Child Psychol. Psychiatry. 2023, 28, 1024–1037. [Google Scholar] [CrossRef] [PubMed]
- Tikotzky, L.; Shaashua, L. Infant sleep and early parental sleep-related cognitions predict sleep in pre-school children. Sleep Med. 2012, 13, 185–192. [Google Scholar] [CrossRef] [PubMed]
- Francavilla, R.; Magistà, A.M.; Bucci, N.; Villirillo, A.; Boscarelli, G.; Mappa, L.; Leone, G.; Fico, S.; Castellaneta, S.; Indrio, F.; et al. Comparison of esophageal pH and multichannel intraluminal impedance testing in pediatric patients with suspected gastroesophageal reflux. J. Pediatr. Gastroenterol. Nutr. 2010, 50, 154–160. [Google Scholar] [CrossRef] [PubMed]
- Loots, C.M.; Benninga, M.A.; Davidson, G.P.; Omari, T.I. Addition of pH-impedance monitoring to standard pH monitoring increases the yield of symptom association analysis in infants and children with gastroesophageal reflux. J. Pediatr. 2009, 154, 248–252. [Google Scholar] [CrossRef] [PubMed]
- Cresi, F.; Locatelli, E.; Marinaccio, C.; Grasso, G.; Coscia, A.; Bertino, E. Prognostic values of multichannel intraluminal impedance and pH monitoring in newborns with symptoms of gastroesophageal reflux disease. J. Pediatr. 2013, 162, 770–775. [Google Scholar] [CrossRef] [PubMed]
- Rosen, R.; Hart, K.; Nurko, S. Does reflux monitoring with multichannel intraluminal impedance change clinical decision making? J. Pediatr. Gastroenterol. Nutr. 2011, 52, 404–407. [Google Scholar] [CrossRef] [PubMed]
- Kaditis, A.; Gozal, D. Sleep Studies for Clinical Indications during the First Year of Life: Infants Are Not Small Children. Children 2022, 9, 523. [Google Scholar] [CrossRef]
- Wise, M.S.; Nichols, C.D.; Grigg-Damberger, M.M.; Marcus, C.L.; Witmans, M.B.; Kirk, V.G.; D’Andrea, L.A.; Hoban, T.F. Executive summary of respiratory indications for polysomnography in children: An evidence-based review. Sleep 2011, 34, 389–398AW. [Google Scholar] [CrossRef] [PubMed]
- Lechien, J.R. Pediatric Laryngopharyngeal Reflux: An Evidence-Based Review. Children 2023, 10, 583. [Google Scholar] [CrossRef] [PubMed]
- Mantegazza, C.; Mallardo, S.; Rossano, M.; Meneghin, F.; Ricci, M.; Rossi, P.; Capra, G.; Latorre, P.; Schindler, A.; Isoldi, S.; et al. Laryngeal signs and pH-multichannel intraluminal impedance in infants and children: The missing ring: LPR and MII-pH in children. Dig. Liver Dis. 2020, 52, 1011–1016. [Google Scholar] [CrossRef] [PubMed]
- Singendonk, M.M.; Pullens, B.; van Heteren, J.A.; de Gier, H.H.; Hoeve, H.L.; König, A.M.; van der Schroeff, M.P.; Hoekstra, C.E.; Veder, L.L.; van der Pol, R.J.; et al. Reliability of the reflux finding score for infants in flexible versus rigid laryngoscopy. Int. J. Pediatr. Otorhinolaryngol. 2016, 86, 37–42. [Google Scholar] [CrossRef]
- Rosen, R.; Mitchell, P.D.; Amirault, J.; Amin, M.; Watters, K.; Rahbar, R. The Edematous and Erythematous Airway Does Not Denote Pathologic Gastroesophageal Reflux. J. Pediatr. 2017, 183, 127–131. [Google Scholar] [CrossRef]


{kind=link}
| MII-pH | ||||
|---|---|---|---|---|
| Total | Abnormal | Normal | ||
| Total number (n) of infants | 50 | 20 | 30 | |
| Sex, n (% of infants) | Female | 26 (52.0) | 8 (40.0) | 18 (60.0) |
| Male | 24 (48.0) | 12 (60.0) | 12 (40.0) | |
| Age (months) | Mean (SD) | 4.0 (2.4) | 3.6 (2.7) | 4.2 (2.2) |
| Median (IQR) | 3.5 (2.0–6.0) | 2.0 (2.0–5.0) | 4.0 (3.0–6.0) | |
| Min-max | 1.0–11.0 | 1.0–11.0 | 1.0–10.0 | |
| Class of age, n (%) | 0–1 month | 5 (10.0) | 2 (40.0) | 3 (60.0) |
| 2–6 months | 39 (78.0) | 16 (41.0) | 23 (59.0) | |
| >6 months | 6 (12.0) | 2 (33.3) | 4 (66.7) | |
| Failure to thrive, n (%) | 11 (22.0) | 3 (27.3) | 8 (72.7) | |
| Regurgitation, episodes n/day (%) | 0–2 | 34 (68.0) | 13 (38.2) | 21 (61.7) |
| 3–10 | 9 (18.0) | 4 (44.4) | 5 (55.6) | |
| >10 | 7 (14.0) | 3 (42.9) | 4 (57.1) | |
| Nocturnal crying/sleep disturbance, n (%) | 26 (52.0) | 10 (38.5) | 16 (61.5) | |
| Abnormal I-GERQ-R, n (%) | 33 (66.0) | 12 (36.4) | 21 (63.6) | |
| Cow’s milk-free diet, n (%) | 29 (58.0) | 10 (34.5) | 19 (65.5) | |
| Variable | OR | 95%CI | p-Value | |
|---|---|---|---|---|
| Sex | Female | 1 | Reference | |
| Male | 2.25 | 0.71–7.14 | 0.17 | |
| Age (continuous) | 0.89 | 0.69–1.14 | 0.63 | |
| Class of age | 0–1 month | 0.96 | 0.14–6.40 | 0.97 |
| 2–6 months | 1 | Reference | ||
| >6 months | 0.72 | 0.12–4.41 | 0.72 | |
| Failure to thrive, n (%) | No | 1 | Reference | |
| Yes | 0.49 | 0.11–2.11 | 0.34 | |
| Regurgitation, n of episodes (% of infants) | 0 | 1 | Reference | |
| 3–10 | 1.29 | 0.29–5.71 | 0.74 | |
| >10 | 1.21 | 0.23–6.30 | 0.82 | |
| Nocturnal crying/sleep disturbance, n (%) | No | 1 | Reference | |
| Yes | 0.88 | 0.28–2.72 | 0.82 | |
| I-GERQ-R score | Normal | 1 | Reference | |
| Abnormal | 0.64 | 0.20–2.11 | 0.47 | |
| Cow’s milk-free diet, n (%) | No | 1 | Reference | |
| Yes | 0.58 | 0.18–1.83 | 0.35 |
| Abnormal MII-pH | OR | 95% CI | p-Value | |
|---|---|---|---|---|
| Univariate Logistic Regression | ||||
| Distal Baseline Impedance | Normal | 1.0 | Reference | |
| Abnormal | 13.38 | 1.46–122.68 | 0.02 | |
| Nocturnal Distal Baseline | Normal | 1.0 | Reference | |
| Abnormal | 3.65 | 1.06–12.56 | 0.04 | |
| Multivariable Logistic Regression | ||||
| Distal Baseline Impedance | Normal | 1.0 | Reference | |
| Abnormal | 8.20 | 0.84–80.51 | 0.07 | |
| Nocturnal Distal Baseline | Normal | 1.0 | Reference | |
| Abnormal | 2.62 | 0.67–10.25 | 0.17 | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Carabelli, G.; Binotto, I.; Armano, C.; Bertù, L.; Luini, C.; Nosetti, L.; Agosti, M.; Salvatore, S. Study on Nocturnal Infant Crying Evaluation (NICE) and Reflux Disease (RED). Children 2024, 11, 450. https://doi.org/10.3390/children11040450
Carabelli G, Binotto I, Armano C, Bertù L, Luini C, Nosetti L, Agosti M, Salvatore S. Study on Nocturnal Infant Crying Evaluation (NICE) and Reflux Disease (RED). Children. 2024; 11(4):450. https://doi.org/10.3390/children11040450
Chicago/Turabian StyleCarabelli, Greta, Ivan Binotto, Chiara Armano, Lorenza Bertù, Chiara Luini, Luana Nosetti, Massimo Agosti, and Silvia Salvatore. 2024. "Study on Nocturnal Infant Crying Evaluation (NICE) and Reflux Disease (RED)" Children 11, no. 4: 450. https://doi.org/10.3390/children11040450
APA StyleCarabelli, G., Binotto, I., Armano, C., Bertù, L., Luini, C., Nosetti, L., Agosti, M., & Salvatore, S. (2024). Study on Nocturnal Infant Crying Evaluation (NICE) and Reflux Disease (RED). Children, 11(4), 450. https://doi.org/10.3390/children11040450