
Adaptation and Validation of the MapMe Body Image Scales in Spanish Parents of Schoolchildren
 , , , and
, , , and
Abstract
1. Introduction
- -
- The correlation between the parental perception of their child’s weight status using the adapted MapMe BIS and the objective measures of child weight status (BMI, Body Fat Percentage (BFP) and Waist Circumference (WC)) will be high.
- -
- This correlation will be greater than between the other perception questions (verbal and analogical) and these weight status variables.
- -
- Parental perception of their child’s weight status using the adapted BIS will be more strongly correlated with the objective measures of child weight status than parental satisfaction with their child’s weight status.
2. Materials and Methods
2.1. Study Design
2.2. Participants
- -
- A total of 4 individuals were excluded from the study due to being outside of this age group, one for not being able to be measured due to a mobility problem.
- -
- A total of 117 children did not provide signed parental consent.
- -
- A total of 41 parents did not complete the questionnaire or answered only some of the questions.
2.3. Procedure
2.4. Instruments
2.4.1. Anthropometric Measures
- Weight: In kilograms, using a TANITA® BC-418 MA bioimpedance scale.
- Height: In centimetres was measured using a SECA® 222 wall height rod.
- Weight status: based on BMI as per the IOTF criteria.
2.4.2. Gold Standard Measures for Validation
- BMI: Calculated as “weight (kg)/(height (m)2)”
- BFP: determined by TANITA® BC-418 MA bioimpedance scale.
- WC: Measured using a flexible tape at the midpoint between the iliac crest and the last rib.
2.4.3. Parental Questionnaire
- Adapted MapMe BIS: it was based on the original body images of children created by Jones et al. [31] using British growth reference (UK90) criteria. These body stimuli were based an analysis of 388 3D scans of children aged 4–5 and 10–11, to produced anatomically accurate illustrations of UK child weight categories [31]. For the validation in Spain, the images were modified to illustrate the IOTF criteria, a measure used worldwide to determine child weight status [34]. For the creation of the original tool in the UK, a total of 12 qualitative sessions were held with parents and childhood obesity health professionals. The result was a sex- and age-specific BIS from two angles: front and profile. Following the format of the original BIS [31], the adapted MapMe BIS was composed of seven different bodies which correspond to seven weight categories: (A) underweight; (B) lower-healthy weight; (C) mid-healthy weight; (D) upper-healthy weight; (E) overweight, (F) lower-very overweight and (G) upper-very overweight. For the analysis, these categories were grouped into four subcategories as per the IOTF: A and B for underweight, C and D for healthy weight, E and F for overweight, and G for obesity.
- Question referred to adapted MapMe BIS: in the first question, called visual perception scale, parents had to choose which of the body shapes best represented their child; the second question, called visual satisfaction scale, analysed satisfaction or dissatisfaction, by asking the parents which image they would like their child to look like/to resemble/seem. These two questions create two variables: perception, that could be correct (if the weight category of the figure coincides with the child’s objectively measured real weight status measured by us) or incorrect (if the weight category of the figure does not coincide with the child’s objectively measured weight status); and satisfaction, that could be satisfied (if the figure chosen coincides with the figure chosen for the visual perception scale of perception), or unsatisfied (if the figure chosen does not coincide with the figure chosen for the visual perception scale if the figure is over or below the perception’s figure).
- Perception based on categorical question: This perception question, with four categorical response options, asked the following question: “How would you describe your child’s current weight at the moment?: underweight, normal weight, overweight or obese” [38].
- Perception based on visual analogue scale: The other perception question had a visual analogue scale response option, consisting of a 10 cm line with one aspect being ‘extremely underweight’, and the other aspect being ‘extremely overweight’. Parents had to specify the position along the line which best described their child’s weight.
2.4.4. Transcultural Adaptation of the Questionnaire
- The inverse translation method was applied to the questions used to assess the impact of the MapMe intervention by specialised English translators. Two bilingual specialists translated the parental questionnaire into Spanish and a native English speaker with Spanish language knowledge carried out an inverse translation. The three translators compared the inverse translation with the original version to determine the degree of semantic and cultural equivalence. Content validity was assessed using the Delphi method, by a team of experts which was composed of 2 paediatricians, 3 paediatric nurses, 1 school nurse, and 2 child psychologists.
- The final version of the questionnaire (adapted BIS and additional questions) was administered to 10 mothers as a pilot comprehension test of the instrument, and no problems were reported. No one proposed any changes, all agreed with the figures of the scale (hair, eye, and skin colour) and considered that it correctly represented the BMI.
2.5. Statistical Analysis
3. Results
3.1. Test-Retest Reliability
3.2. Criterion Validity
3.3. Concurrent Validity
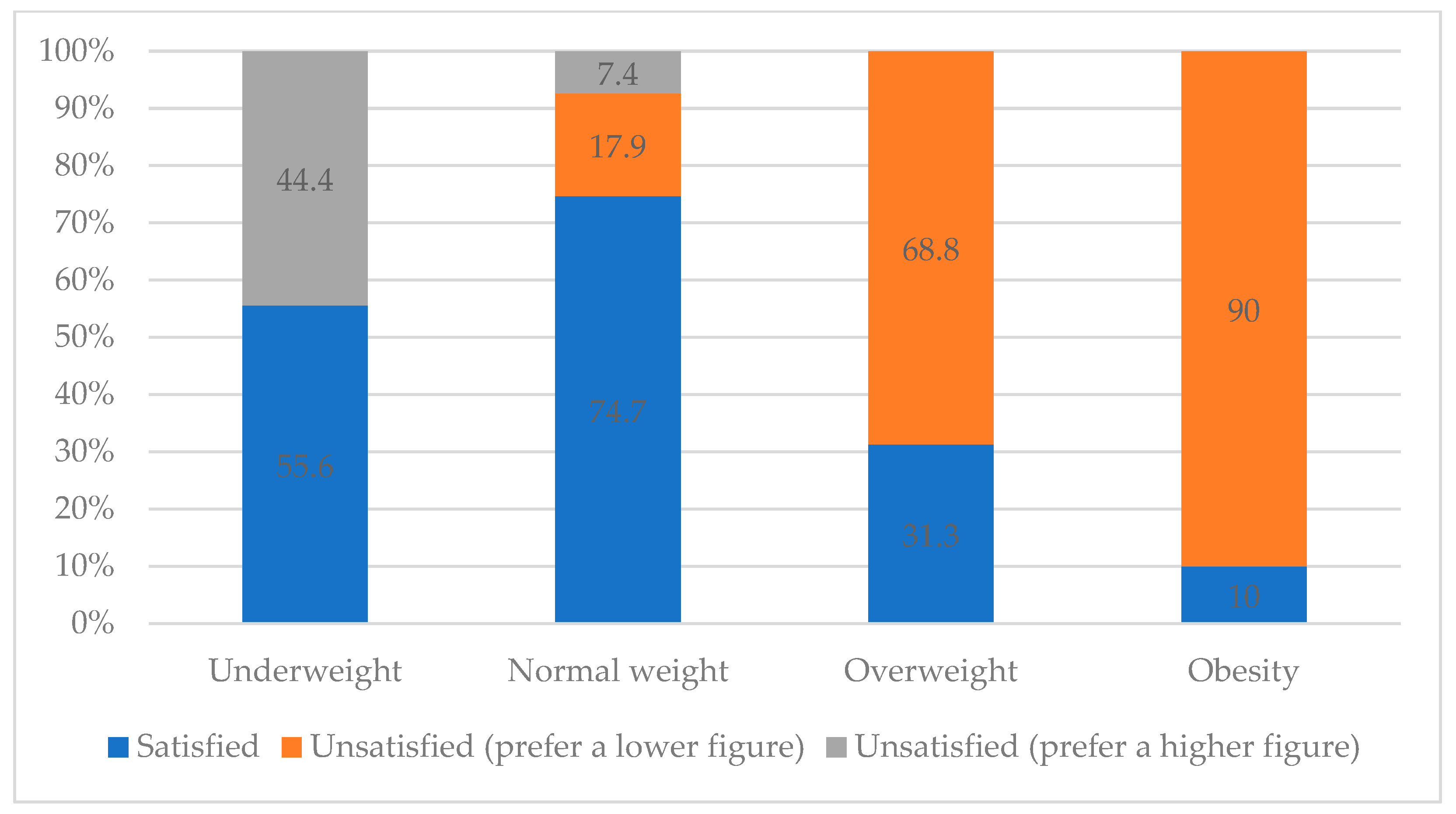
3.4. Satisfaction Visual Scale
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Canals-Sans, J.; Blanco-Gómez, A.; Luque, V.; Ferré, N.; Ferrando, P.J.; Gispert-Llauradó, M.; Escribano, J.; Closa-Monasterolo, R. Validation of the Child Feeding Questionnaire in Spanish Parents of Schoolchildren. J. Nutr. Educ. Behav. 2016, 48, 383–391.e1. [Google Scholar] [CrossRef] [PubMed]
- Garrido-Miguel, M.; Oliveira, A.; Cavero-Redondo, I.; Álvarez-Bueno, C.; Pozuelo-Carrascosa, D.; Soriano-Cano, A.; Martínez-Vizcaíno, V. Prevalence of Overweight and Obesity among European Preschool Children: A Systematic Review and Meta-Regression by Food Group Consumption. Nutrients 2019, 11, 1698. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Report of the Commision on: Ending Childhood Obesity; World Health Organization: Geneva, Switzerland, 2016; ISBN 978-92-4-151006-6. [Google Scholar]
- Ames, H.; Mosdøl, A.; Blaasvær, N.; Nøkleby, H.; Berg, R.C.; Langøien, L.J. Communication of children’s weight status: What is effective and what are the children’s and parents’ experiences and preferences? A mixed methods systematic review. BMC Public Health 2020, 20, 574. [Google Scholar] [CrossRef]
- World Health Organization. Obesity and Overweight: Key Facts. Available online: https://www.who.int/news-room/fact-sheets/detail/obesity-and-overweight (accessed on 4 December 2022).
- AESAN. Informe Breve Sobre la Alimentación, Desarrollo Infantil y Obesidad en España (ALADINO 2019); AESAN: Madrid, Spain, 2020.
- Fan, H.; Zhang, X. Recent trends in overweight and obesity in adolescents aged 12 to 15 years across 21 countries. Pediatr. Obes. 2021, 17, e12839. [Google Scholar] [CrossRef]
- Almoosawi, S.; Jones, A.R.; Parkinson, K.N.; Pearce, M.S.; Collins, H.; Adamson, A.J. Parental Perception of Weight Status: Influence on Children’s Diet in the Gateshead Millennium Study. PLoS ONE 2016, 11, e0144931. [Google Scholar] [CrossRef]
- Ortiz-Pinto, M.A.; Ortiz-Marrón, H.; Rodríguez-Rodríguez, A.; Casado-Sánchez, L.; Cuadrado-Gamarra, J.I.; Galán, I. Parental perception of child health status and quality of life associated with overweight and obesity in early childhood. Qual. Life Res. 2020, 29, 163–170. [Google Scholar] [CrossRef] [PubMed]
- Mareno, N. Parental perception of child weight: A concept analysis. J. Adv. Nurs. 2014, 70, 34–45. [Google Scholar] [CrossRef] [PubMed]
- Garrido-Miguel, M.; Cavero-Redondo, I.; Álvarez-Bueno, C.; Rodríguez-Artalejo, F.; Moreno, L.A.; Ruiz, J.R.; Ahrens, W.; Martínez-Vizcaíno, V. Prevalence and Trends of Overweight and Obesity in European Children from 1999 to 2016: A Systematic Review and Meta-analysis. JAMA Pediatr. 2019, 173, e192430. [Google Scholar] [CrossRef]
- Parkinson, K.N.; Jones, A.R.; Tovee, M.J.; Ells, L.J.; Pearce, M.S.; Araujo-Soares, V.; Adamson, A.J. A cluster randomised trial testing an intervention to improve parents’ recognition of their child’s weight status: Study protocol. BMC Public Health 2015, 15, 549. [Google Scholar] [CrossRef]
- Warkentin, S.; Mais, L.A.; Latorre, M.D.R.; Carnell, S.; Taddei, J.A.A. Factors associated with parental underestimation of child’s weight status. J. Pediatr. 2018, 94, 162–169. [Google Scholar] [CrossRef]
- Warkentin, S.; Henriques, A.; Oliveira, A. Parents’ perceptions and dissatisfaction with child silhouette: Associated factors among 7-year-old children of the Generation XXI birth cohort. Eat. Weight. Disord. 2021, 26, 1595–1607. [Google Scholar] [CrossRef] [PubMed]
- Hahn, S.L.; Barry, M.R.; Weeks, H.M.; Miller, A.L.; Lumeng, J.C.; Sonneville, K.R. Parental perceptions of actual and ideal body weight in early childhood prospectively predict adolescent perceptions of actual and ideal body weight among a low-income population. Eat. Weight. Disord. 2021, 26, 2371–2379. [Google Scholar] [CrossRef]
- Jones, A.R.; Mann, K.D.; Cutler, L.R.; Pearce, M.S.; Tovée, M.J.; Ells, L.J.; Araujo-Soares, V.; Arnott, B.; Harris, J.M.; Adamson, A.J. A Randomised Control Trial Investigating the Efficacy of the MapMe Intervention on Parental Ability to Correctly Categorise Overweight in Their Child and the Impact on Child BMI Z-Score Change at 1 Year. Children 2023, 10, 1577. [Google Scholar] [CrossRef] [PubMed]
- Meredith-jones, K.; Williams, S.; Taylor, R. Agreement between parental perception of child weight status and actual weight status is similar across different ethnic groups in New Zealand. J. Prim. Health Care 2016, 8, 316–324. [Google Scholar] [CrossRef]
- Kelleher, E.; Millar, S.; Shiely, F.; Perry, I.; Harrington, J. RF34 Parent and child misperception of child weight status: A cross-sectional analysis of the cork children’s lifestyle study (CCLaS). J. Epidemiol. Community Health 2018, 72, A59. [Google Scholar] [CrossRef]
- AlHasan, D.M.; Breneman, C.B.; Lynes, C.L.; Callahan-Myrick, K. Factors that Influence Parental Misperception of Their Child’s Actual Weight Status in South Carolina. Matern. Child Health J. 2018, 22, 1077–1084. [Google Scholar] [CrossRef] [PubMed]
- Rodrigues, D.; Machado-Rodrigues, A.M.; Padez, C. Parental misperception of their child’s weight status and how weight underestimation is associated with childhood obesity. Am. J. Hum. Biol. 2020, 32, e23393. [Google Scholar] [CrossRef] [PubMed]
- Hong, S.A.; Peltzer, K.; Jalayondeja, C. Parental misperception of child’s weight and related factors within family norms. Eat. Weight. Disord. 2019, 24, 557–564. [Google Scholar] [CrossRef]
- Ramiro-González, M.D.; Sanz-Barbero, B.; Royo-Bordonada, M.Á. Childhood Excess Weight in Spain From 2006 to 2012. Determinants and Parental Misperception. Rev. Española Cardiol. 2017, 70, 656–663. [Google Scholar] [CrossRef]
- Hager, E.R.; Candelaria, M.; Latta, L.W.; Hurley, K.M.; Wang, Y.; Caulfield, L.E.; Black, M.M. Maternal Perceptions of Toddler Body Size. Arch. Pediatr. Adolesc. Med. 2012, 166, 417. [Google Scholar] [CrossRef]
- Cash, T.F. Body image: Past, present, and future. Body Image 2004, 1, 1–5. [Google Scholar] [CrossRef] [PubMed]
- Blowers, L.C.; Loxton, N.J.; Grady-Flesser, M.; Occhipinti, S.; Dawe, S. The relationship between sociocultural pressure to be thin and body dissatisfaction in preadolescent girls. Eat. Behav. 2003, 4, 229–244. [Google Scholar] [CrossRef] [PubMed]
- Reel, J.; Voelker, D.; Greenleaf, C. Weight status and body image perceptions in adolescents: Current perspectives. Adolesc. Health Med. Ther. 2015, 2015, 149–158. [Google Scholar] [CrossRef]
- Rodgers, R.; Chabrol, H. Parental attitudes, body image disturbance and disordered eating amongst adolescents and young adults: A review. Eur. Eat. Disord. Rev. 2009, 17, 137–151. [Google Scholar] [CrossRef] [PubMed]
- Helfert, S.; Warschburger, P. A prospective study on the impact of peer and parental pressure on body dissatisfaction in adolescent girls and boys. Body Image 2011, 8, 101–109. [Google Scholar] [CrossRef] [PubMed]
- Schur, E.A.; Sanders, M.; Steiner, H. Body dissatisfaction and dieting in young children. Int. J. Eat. Disord. 2000, 27, 74–82. [Google Scholar] [CrossRef]
- Neves, C.M.; Cipriani, F.M.; Meireles, J.F.F.; Da Rocha Morgado, F.F.; Ferreira, M.E.C. Body image in childhood: An integrative literature review. Rev. Paul. Pediatr. 2017, 35, 331–339. [Google Scholar] [CrossRef]
- Jones, A.R.; Tovée, M.J.; Cutler, L.R.; Parkinson, K.N.; Ells, L.J.; Araujo-Soares, V.; Pearce, M.S.; Mann, K.D.; Scott, D.; Harris, J.M.; et al. Development of the MapMe intervention body image scales of known weight status for 4–5 and 10–11 year old children. J. Public Health 2017, 40, 582–590. [Google Scholar] [CrossRef] [PubMed]
- Pallan, M.J.; Hiam, L.C.; Duda, J.L.; Adab, P. Body image, body dissatisfaction and weight status in south asian children: A cross-sectional study. BMC Public Health 2011, 11, 21. [Google Scholar] [CrossRef]
- Salcedo, V.; Gutiérrez-Fisac, J.L.; Guallar-Castillón, P.; Rodríguez-Artalejo, F. Trends in overweight and misperceived overweight in Spain from 1987 to 2007. Int. J. Obes. 2010, 34, 1759–1765. [Google Scholar] [CrossRef]
- Cole, T.; Lobstein, T. Extended international (IOTF) body mass index cut-offs for thinness, overweight and obesity. Pediatr. Obes. 2012, 7, 284–294. [Google Scholar] [CrossRef]
- Ministerio de Sanidad Consumo y Bienestar Social, G. Encuesta Nacional de Salud. España 2017; Ministerio de Sanidad Consumo y Bienestar Social: Madrid, Spain, 2018.
- Agencia Española de Seguridad Alimentaria y Nutrición. Estudio ALADINO 2019: Surveillance Study on Nutrition, Physical Activity, Child Development and Obesity. 2020. Available online: https://www.aesan.gob.es/AECOSAN/docs/documentos/nutricion/observatorio/Brief_report_ALADINO_2019_NAOS.pdf (accessed on 3 February 2023).
- Rodríguez-Martin, A.; Novalbos-Ruiz, J.P.; Villagran-Perez, S.; Martínez-Nieto, J.M.; Lechuga-Campoy, J.L. Parents perception of childhood overweight and obesity and eating behaviors, physical activity and sedentary lifestyle of their children. Rev. Esp. Salud Publica 2012, 86, 483–494. [Google Scholar] [PubMed]
- Carnell, S.; Edwards, C.; Croker, H.; Boniface, D.; Wardle, J. Parental perceptions of overweight in 3–5 y olds. Int. J. Obes. 2005, 29, 353–355. [Google Scholar] [CrossRef]
- Koo, T.K.; Li, M.Y. A Guideline of Selecting and Reporting Intraclass Correlation Coefficients for Reliability Research. J. Chiropr. Med. 2016, 15, 155–163. [Google Scholar] [CrossRef] [PubMed]
- Landis, J.R.; Koch, G.G. Landis amd Koch1977—Agreement of categorical data. Biometrics 1977, 33, 159–174. [Google Scholar] [CrossRef] [PubMed]
- Terwee, C.B.; Bot, S.D.M.; de Boer, M.R.; van der Windt, D.A.W.M.; Knol, D.L.; Dekker, J.; Bouter, L.M.; de Vet, H.C.W. Quality criteria were proposed for measurement properties of health status questionnaires. J. Clin. Epidemiol. 2007, 60, 34–42. [Google Scholar] [CrossRef] [PubMed]
- Wright, C.M.; Booth, I.W.; Buckler, J.M.H.; Cameron, N.; Cole, T.J.; Healy, M.J.R.; Hulse, J.A.; Preece, M.A.; Reilly, J.J.; Williams, A.F. Growth reference charts for use in the United Kingdom. Arch. Dis. Child. 2002, 86, 11–14. [Google Scholar] [CrossRef]
- Manios, Y.; Kondaki, K.; Kourlaba, G.; Vasilopoulou, E.; Grammatikaki, E. Maternal perceptions of their child’s weight status: The GENESIS study. Public Health Nutr. 2009, 12, 1099–1105. [Google Scholar] [CrossRef]
- Towns, N.; D’Auria, J. Parental Perceptions of Their Child’s Overweight: An Integrative Review of the Literature. J. Pediatr. Nurs. 2009, 24, 115–130. [Google Scholar] [CrossRef]
- Berenson, G.S. Health Consequences of Obesity. Pediatr. Blood Cancer 2012, 58, 117–121. [Google Scholar] [CrossRef]
- White, M. Sample size in quantitative instrument validation studies: A systematic review of articles published in Scopus, 2021. Heliyon 2022, 8, e12223. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| n | % | ||
|---|---|---|---|
| Age (years) | 10 | 87 | 56.1 |
| 11 | 68 | 43.9 | |
| Sex | Male | 77 | 49.7 |
| Female | 78 | 50.3 | |
| Weight status | Underweight | 18 | 11.6 |
| Healthy weight | 95 | 61.3 | |
| Overweight | 32 | 20.6 | |
| Obese | 10 | 6.5 | |
| Total | 155 |
| Male | Female | Total | Sig | ||||
|---|---|---|---|---|---|---|---|
| Age (years) | 10 | 46 | 41 | 87 | 0.371 | ||
| 11 | 31 | 37 | 68 | ||||
| Weight status | 0.528 | ||||||
| Underweight | 12 | 6 | 18 | ||||
| Healthy weight | 45 | 50 | 95 | ||||
| Overweight | 14 | 18 | 32 | ||||
| Obese | 6 | 4 | 10 | ||||
| Mean | SD | Mean | SD | ||||
| BMI | 18.91 | 3.68 | 18.73 | 3.27 | 0.750 | ||
| Body fat percentage | 19.33 | 7.41 | 22.78 | 7.65 | 0.005 * | ||
| Waist circumference | 67.75 | 8.75 | 65.06 | 7.69 | 0.044 * | ||
| Visual Parents Perception of Their Children Body Weight | Objective Weight Status | ||||
|---|---|---|---|---|---|
| Underweight | Normal Weight | Overweight | Obese | Total | |
| Underweight | 12 | 13 | 0 | 0 | 25 |
| 66.7 | 13.7 | 0 | 0 | 16.1 | |
| Normal weight | 5 | 57 | 3 | 0 | 65 |
| 27.8 | 60.0 | 9.4 | 0 | 41.9 | |
| Overweight | 1 | 25 | 23 | 4 | 53 |
| 5.6 | 26.3 | 71.9 | 40 | 34.2 | |
| Obese | 0 | 0 | 6 | 6 | 12 |
| 0 | 0 | 18.8 | 60 | 7.7 | |
| Total | 18 | 95 | 32 | 10 | 155 |
| 100 | 100 | 100 | 100 | 100 | |
| Male | Female | |||||
|---|---|---|---|---|---|---|
| BMI | BFP | WC | BMI | BFP | WC | |
| Underweight | 14.37 | 10.96 | 59.51 | 14.26 | 10.57 | 56.46 |
| Healthy weight | 17.89 | 17.49 | 65.09 | 17.38 | 20.24 | 61.87 |
| Overweight | 22.77 | 26.37 | 76.62 | 22.28 | 30.71 | 73.91 |
| Obese | 26.66 | 33.40 | 83.42 | 26.34 | 37.21 | 77.92 |
| Categorical Question | Visual Analogue Scale Question | Visual Question | Satisfaction Question | BMI | BFP | WC | Weight Status | |
|---|---|---|---|---|---|---|---|---|
| Categorical question | 1.000 | 0.561 | 0.673 | 0.256 | 0.724 | 0.676 | 0.682 | 0.705 |
| Visual analogue scale question | 0.561 | 1.000 | 0.461 | 0.229 | 0.431 | 0.393 | 0.429 | 0.398 |
| Visual question | 0.673 | 0.461 | 1.000 | 0.582 | 0.776 | 0.792 | 0.747 | 0.717 |
| Satisfaction question | 0.256 | 0.229 | 0.582 | 1.000 | 0.417 | 0.434 | 0.423 | 0.407 |
| BMI | 0.724 | 0.431 | 0.776 | 0.417 | 1.000 | 0.921 | 0.909 | 0.903 |
| BFP | 0.676 | 0.393 | 0.792 | 0.434 | 0.921 | 1.000 | 0.870 | 0.827 |
| WC | 0.682 | 0.429 | 0.747 | 0.423 | 0.909 | 0.870 | 1.000 | 0.784 |
| Weight status | 0.705 | 0.398 | 0.717 | 0.407 | 0.903 | 0.827 | 0.784 | 1.000 |
| % Correct Perception | Underweight | Healthy Weight | Overweight | Obese |
|---|---|---|---|---|
| Categorical question | 50.0 | 90.5 | 59.4 | 10 |
| Visual analogue scale question | 33.3 | 92.6 | 28.1 | 10 |
| Visual perception question (adapted MapMe BIS) | 66.7 | 60 | 71.9 | 60 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Inclan-Lopez, P.; Martinez-Andres, M.; Jones, A.R.; Tovée, M.J.; Adamson, A.J.; Bartolome-Gutierrez, R. Adaptation and Validation of the MapMe Body Image Scales in Spanish Parents of Schoolchildren. Children 2024, 11, 448. https://doi.org/10.3390/children11040448
Inclan-Lopez P, Martinez-Andres M, Jones AR, Tovée MJ, Adamson AJ, Bartolome-Gutierrez R. Adaptation and Validation of the MapMe Body Image Scales in Spanish Parents of Schoolchildren. Children. 2024; 11(4):448. https://doi.org/10.3390/children11040448
Chicago/Turabian StyleInclan-Lopez, Patricia, Maria Martinez-Andres, Angela R. Jones, Martin J. Tovée, Ashley J. Adamson, and Raquel Bartolome-Gutierrez. 2024. "Adaptation and Validation of the MapMe Body Image Scales in Spanish Parents of Schoolchildren" Children 11, no. 4: 448. https://doi.org/10.3390/children11040448
APA StyleInclan-Lopez, P., Martinez-Andres, M., Jones, A. R., Tovée, M. J., Adamson, A. J., & Bartolome-Gutierrez, R. (2024). Adaptation and Validation of the MapMe Body Image Scales in Spanish Parents of Schoolchildren. Children, 11(4), 448. https://doi.org/10.3390/children11040448