
Bracing of Pectus Carinatum in Children: Current Practices

 ,
, 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Recruitment of Participants and Data Collection
2.2. The Questionnaire
2.3. Statistical Data Evaluation
3. Results
3.1. The Experience of the Participating Departments
3.2. Indications and Contraindications for COB
3.3. Diagnostics and In-Treatment Protocol
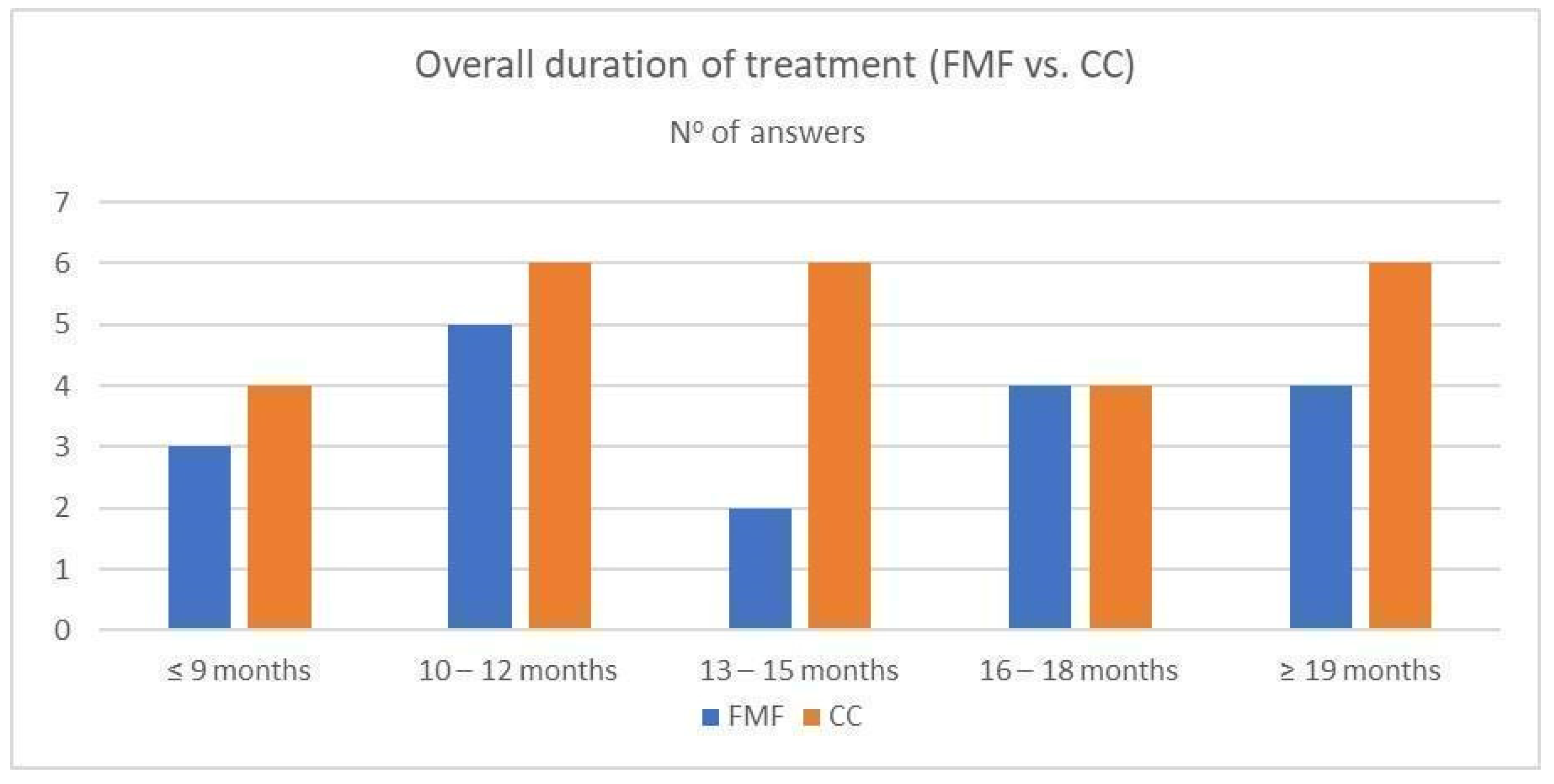
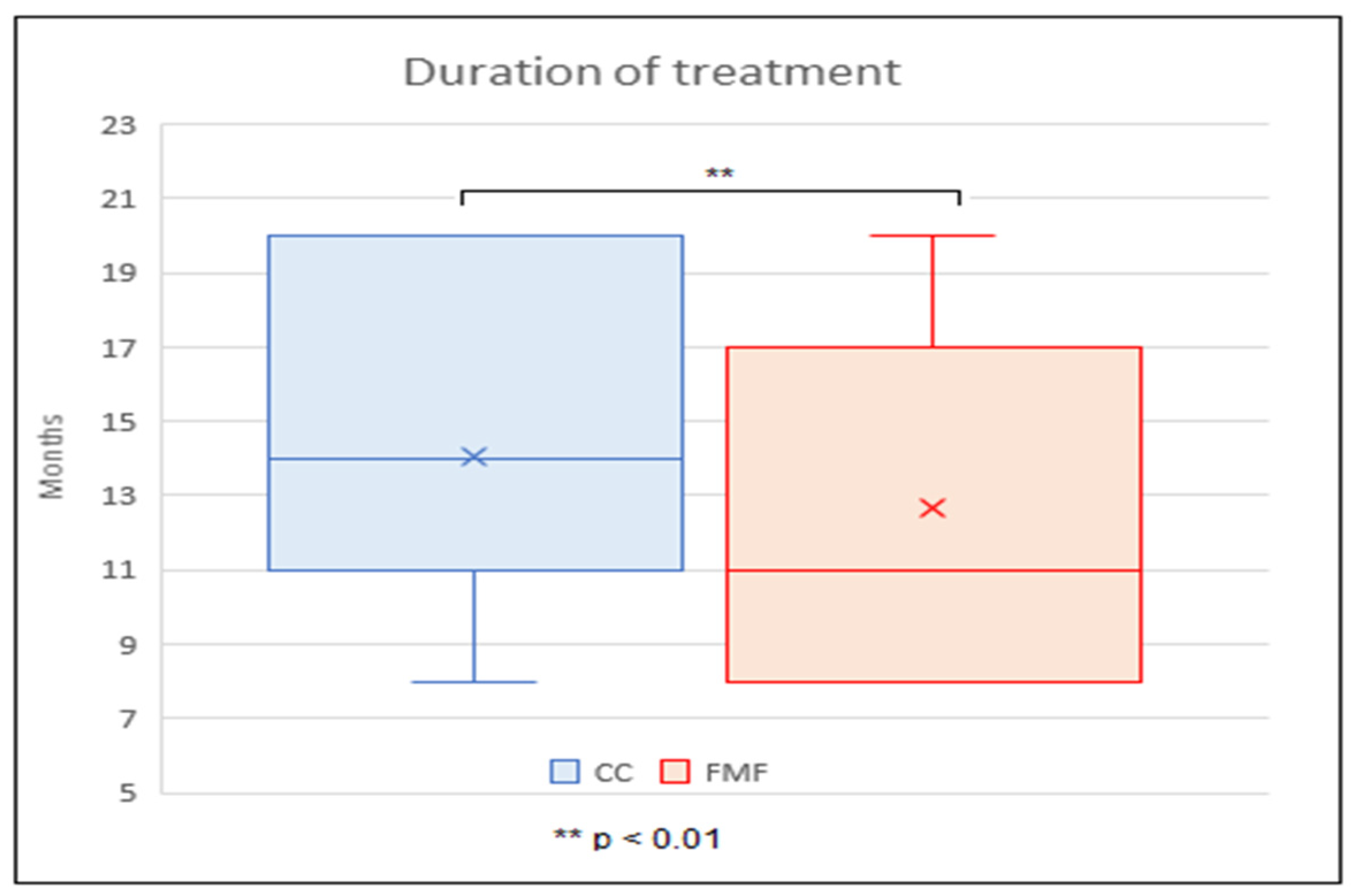
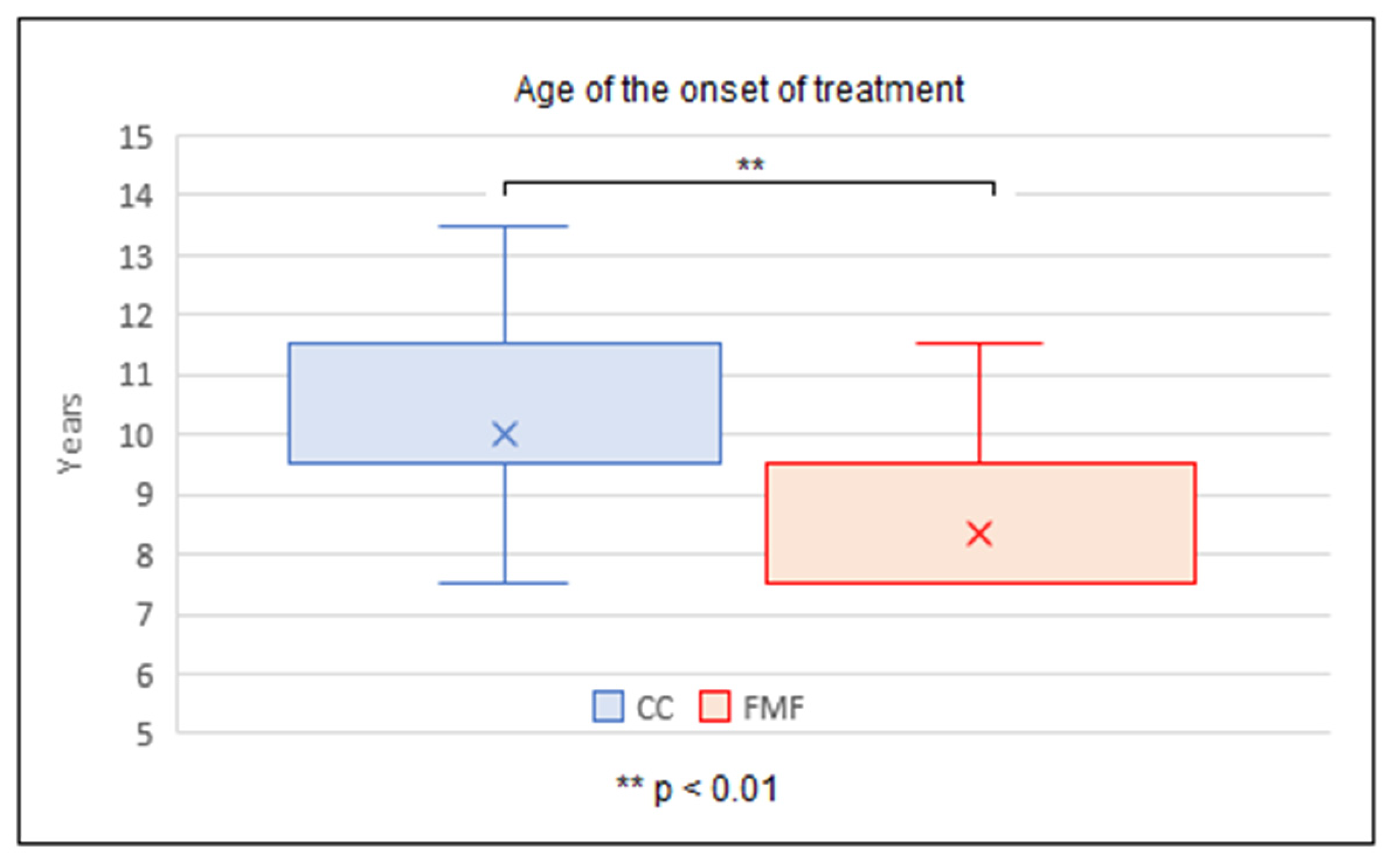
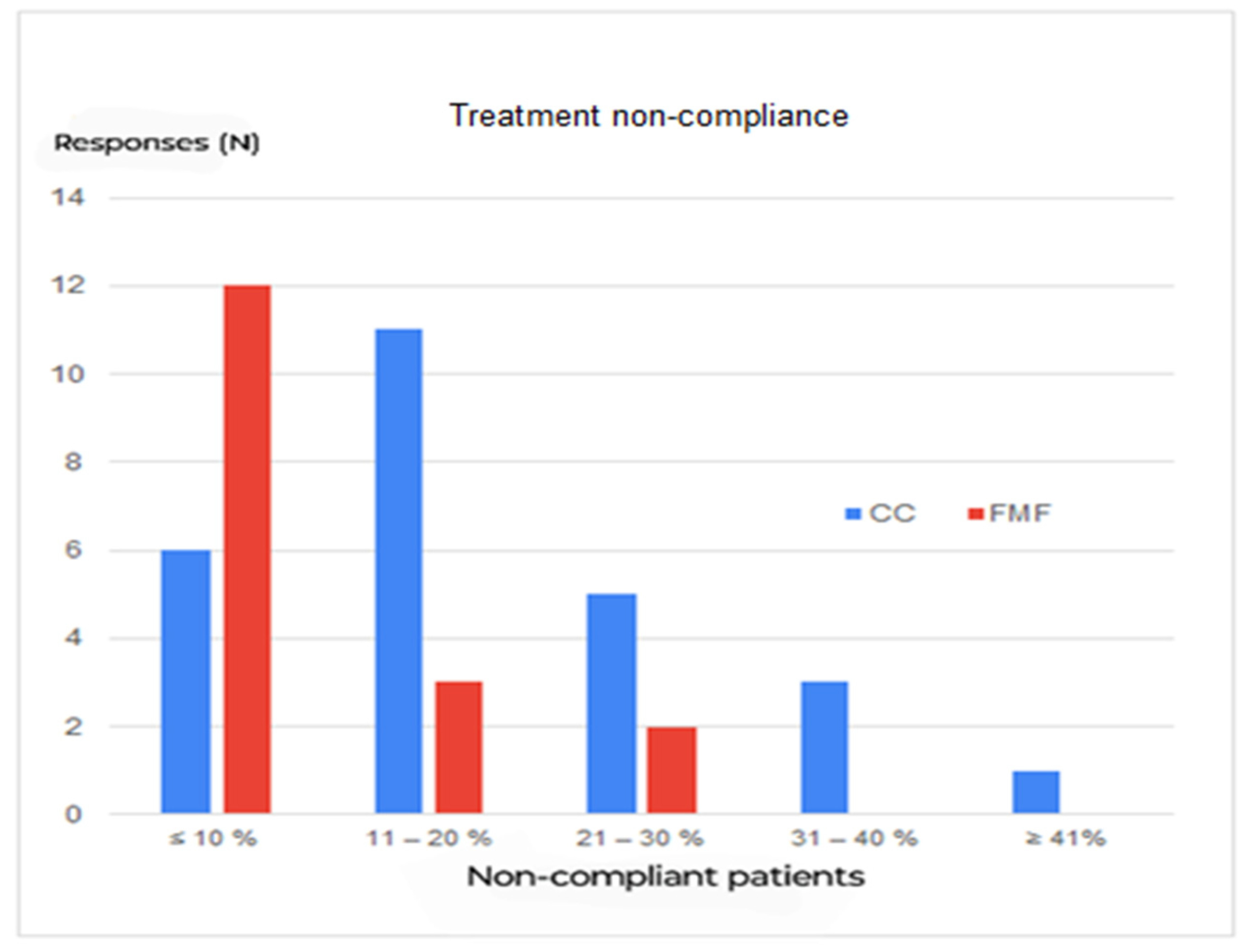
3.4. Treatment Regime and Follow-Up
4. Discussion
5. Limitations
6. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Cohee, A.S.; Lin, J.R.; Frantz, F.W.; Kelly, R.E., Jr. Staged management of pectus carinatum. J. Pediatr. Surg. 2013, 48, 315–320. [Google Scholar] [CrossRef] [PubMed]
- Orrick, B.A.; Pierce, A.L.; McElroy, S.F. Changes in self-image after pectus carinatum brace treatment. J. Pediatr. Surg. 2022, 57, 1579–1583. [Google Scholar] [CrossRef]
- Emil, S.; Sévigny, M.; Montpetit, K.; Baird, R.; Laberge, J.M.; Goyette, J.; Finlay, I.; Courchesne, G. Success and duration of dynamic bracing for pectus carinatum: A four-year prospective study. J. Pediatr. Surg. 2017, 52, 124–129. [Google Scholar] [CrossRef]
- Yuksel, M.; Lacin, T.; Ermerak, N.O.; Sirzai, E.Y.; Sayan, B. Minimally Invasive Repair of Pectus Carinatum. Ann. Thorac. Surg. 2018, 105, 915–923. [Google Scholar] [CrossRef] [PubMed]
- Del Frari, B.; Sigl, S.; Schwabegger, A.H.; Blank, C.; Morawetz, D.; Gassner, E.; Schobersberger, W. Impact of surgical treatment of pectus carinatum on cardiopulmonary function: A prospective study. Eur. J. Cardio-Thorac. Surg. 2021, 59, 382–388. [Google Scholar] [CrossRef] [PubMed]
- Fonkalsrud, E.W.; Beanes, S. Surgical management of pectus carinatum: 30 years’ experience. World J. Surg. 2001, 25, 898–903. [Google Scholar] [CrossRef] [PubMed]
- Wang, L.; Liu, J.; Shen, S.; Li, Y.; Feng, T.; Li, G.; Xiao, H.; Hu, F. Comparison of Outcomes Between Anti-Nuss Operation and Modified Anti-Nuss Operation Using a Flexible Plate for Correcting Pectus Carinatum: A Retrospective Study. Front. Surg. 2021, 7, 600755. [Google Scholar] [CrossRef] [PubMed]
- Haller, J.A., Jr.; Colombani, P.M.; Humphries, C.T.; Azizkhan, R.G.; Loughlin, G.M. Chest wall constriction after too extensive and too early operations for pectus excavatum. Ann. Thorac. Surg. 1996, 61, 1618–1625. [Google Scholar] [CrossRef]
- Haje, S.A.; Raymundo, J.L.P. Considerações sobre deformidades da parede torácica anterior e apresentação de tratamento conservador para as formas com componentes de protrusão. Rev. Bras. Ortop. 1979, 14, 167–178. [Google Scholar]
- Martinez-Ferro, M.; Fraire, C.; Bernard, S. Dynamic compression system for the correction of pectus carinatum. Semin. Pediatr. Surg. 2008, 17, 194–200. [Google Scholar] [CrossRef]
- Abramson, H. Método miniinvasivo para la corrección del pectus carinatum. Comunicación preliminar [A minimally invasive technique to repair pectus carinatum. Preliminary report]. Arch Bronconeumol. 2005, 41, 349–351. [Google Scholar] [CrossRef] [PubMed]
- Chest Wall International Group. Available online: www.cwig.info (accessed on 11 January 2024).
- Altman, D.G. Practical Statistics for Medical Research, 1st ed.; Chapman and Hall/CRC: London, UK, 1990; pp. 85–94. [Google Scholar]
- Port, E.; Hebal, F.; Hunter, C.J.; Malas, B.; Reynolds, M. Measuring the impact of brace intervention on pediatric pectus carinatum using white light scanning. J. Pediatr. Surg. 2018, 53, 2491–2494. [Google Scholar] [CrossRef]
- Bugajski, T.; Murari, K.; Lopushinsky, S.; Schneider, M.; Ronsky, J. Bracing of pectus carinatum: A quantitative analysis. J. Pediatr. Surg. 2018, 53, 1014–1019. [Google Scholar] [CrossRef] [PubMed]
- Ugolini, S.; Mazzocchi, T.; Ghionzoli, M.; Facchini, F.; Ricotti, L.; Ciuti, G.; Menciassi, A.; Messineo, A. Sensorized Orthosis for Non-Operative Treatment of Pectus Carinatum in Pediatric Patients. IEEE Trans. Med. Robot. Bionics 2019, 1, 115–121. [Google Scholar] [CrossRef]
- Skrzypczak, P.; Kasprzyk, M.; Piwkowski, C. The new steel bar in pectus carinatum repair and a review of current methods of correcting chest deformations. J. Thorac. Dis. 2022, 14, 3671–3673. [Google Scholar] [CrossRef]
- American Pediatric Surgical Association. Available online: https://ppfe7e.a2cdn1.secureserver.net/wp-content/uploads/2020/10/Pectus_Carinatum_Guideline_080812-1.pdf?time=1700120584 (accessed on 11 January 2024).
- Giray, E.; Ermerak, N.O.; Bahar-Ozdemir, Y.; Kalkandelen, M.; Yuksel, M.; Gunduz, O.H.; Akyuz, G.A. Comparative Study on Short-Term Effects of Compression Orthosis and Exercises in the Treatment of Pectus Carinatum: A Randomized Controlled Pilot Feasibility Trial. Eur. J. Pediatr. Surg. 2021, 31, 147–156. [Google Scholar] [CrossRef]
- Wahba, G.; Nasr, A.; Bettolli, M. A less intensive bracing protocol for pectus carinatum. J. Pediatr. Surg. 2017, 52, 1795–1799. [Google Scholar] [CrossRef] [PubMed]
- Kang, D.Y.; Jung, J.; Chung, S.; Cho, J.; Lee, S. Factors affecting patient compliance with compressive brace therapy for pectus carinatum. Interact. Cardiovasc. Thorac. Surg. 2014, 19, 900–903. [Google Scholar] [CrossRef]
- Hunt, I.; Patel, A.J. Effectiveness of Compressive External Bracing in Patients with Flexible Pectus Carinatum Deformity: A Review. Thorac. Cardiovasc. Surg. 2020, 68, 72–79. [Google Scholar] [CrossRef]
- Shang, Z.; Hong, C.; Duan, X.; Li, X.; Si, Y. Orthotic Bracing or Minimally Invasive Surgery? A Summary of 767 Pectus Carinatum Cases for 9 Years. BioMed Res. Int. 2021, 2021, 6942329. [Google Scholar] [CrossRef]
- Real, A.; Morais, P.; Oliveira, B.; Torres, H.R.; Vilaça, J.L. Remote Monitoring System of Dynamic Compression Bracing to Correct Pectus Carinatum. Sensors 2023, 23, 4427. [Google Scholar] [CrossRef] [PubMed]
- Kelly, R.E.; Obermeyer, R.J.; Goretsky, M.J.; Kuhn, M.A.; McGuire, M.M.; Duke, D.S.; Pallera, H.K.; Frantz, F.W. Ten-year experience with staged management of pectus carinatum: Results and lessons learned. J. Pediatr. Surg. 2021, 56, 1835–1840. [Google Scholar] [CrossRef]
- de Beer, S.A.; Blom, Y.E.; Lopez, M.; de Jong, J.R. Measured dynamic compression for pectus carinatum: A systematic review. Semin. Pediatr. Surg. 2018, 27, 175–182. [Google Scholar] [CrossRef] [PubMed]
- de Beer, S.; Volcklandt, S.; de Jong, J.; Oomen, M.; Zwaveling, S.; van Heurn, E. Dynamic Compression Therapy for Pectus Carinatum in Children and Adolescents: Factors for Success. J. Pediatr. Surg. 2023, 58, 1440–1445. [Google Scholar] [CrossRef] [PubMed]
- Alaca, N.; Yüksel, M. Comparison of physical functions and psychosocial conditions between adolescents with pectus excavatum, pectus carinatum and healthy controls. Pediatr. Surg. Int. 2021, 37, 765–775. [Google Scholar] [CrossRef] [PubMed]
- Song, S.H.; Kim, C.H.; Moon, D.H.; Lee, S. Usefulness of 3-Dimensional Body Surface Scanning in the Evaluation of Patients with Pectus Carinatum. Korean J. Thorac. Cardiovasc. Surg. 2020, 53, 301–305. [Google Scholar] [CrossRef] [PubMed]
- Guillot, M.S.; Rouchaud, A.; Mounayer, C.; Tricard, J.; Belgacem, A.; Auditeau, E.; Omraam, O.; Fourcade, L.; Ballouhey, Q. X-ray-free protocol for pectus deformities based on magnetic resonance imaging and a low-cost portable three-dimensional scanning device: A preliminary study. Interact. Cardiovasc. Thorac. Surg. 2021, 33, 110–118. [Google Scholar] [CrossRef]
- Kutanzi, K.R.; Lumen, A.; Koturbash, I.; Miousse, I.R. Pediatric Exposures to Ionizing Radiation: Carcinogenic Considerations. Int. J. Environ. Res. Public Health 2016, 13, 1057. [Google Scholar] [CrossRef]
- Daemen, J.H.T.; Loonen, T.G.J.; Lozekoot, P.W.J.; Maessen, J.G.; Maal, T.J.J.; Hulsewé, K.W.E.; Vissers, Y.L.J.; de Loos, E.R. Optical imaging versus CT and plain radiography to quantify pectus severity: A systematic review and meta-analysis. J. Thorac. Dis. 2020, 12, 1475–1487. [Google Scholar] [CrossRef]
- Omaník, P.; Kozlíková, K.; Daumová, N.; Schmidtová, V.; Béder, I. The Role of Anthropologic Measurements in Pectus Carinatum Brace Treatment Evaluation. Meas. Sci. Rev. 2022, 22, 50–57. [Google Scholar] [CrossRef]
- Hussain, A.; Patel, A.; Hunt, I. Are non-radiation-based imaging modalities effective for objectively assessing and monitoring patients with pectus deformities? Interact. Cardiovasc. Thorac. Surg. 2020, 31, 536–539. [Google Scholar] [CrossRef] [PubMed]
- Kelly, R.E., Jr.; Obermeyer, R.J.; Kuhn, M.A.; Frantz, F.W.; Obeid, M.F.; Kidane, N.; McKenzie, F.D. Use of an Optical Scanning Device to Monitor the Progress of Noninvasive Treatments for Chest Wall Deformity: A Pilot Study. Korean J. Thorac. Cardiovasc. Surg. 2018, 51, 390–394. [Google Scholar] [CrossRef] [PubMed]
- Fuentes, S.; Berlioz, M.; Damián, F.; Pradillos, J.M.; Lorenzo, T.; Ardela, E. Patient and healthcare professional satisfaction with 3D imaging new technologies for medical purposes. Satisfacción de pacientes y profesionales con las nuevas tecnologías de imagen tridimensional aplicadas a la medicina. Radiologia 2020, 62, 46–50. [Google Scholar] [CrossRef] [PubMed]
- Sun, J.; Chen, C.; Peng, Y.; Zhang, Y.; Tian, H.; Yu, J.; Cao, J.; Zeng, Q. Comparison of magnetic resonance imaging and computed tomography to measure preoperative parameters of children with pectus excavatum. Pediatr. Investig. 2019, 3, 102–109. [Google Scholar] [CrossRef] [PubMed]
- Sesia, S.B.; Holland-Cunz, S.; Häcker, F.M. Dynamic Compression System: An Effective Nonoperative Treatment for Pectus Carinatum: A Single Center Experience in Basel, Switzerland. Eur. J. Pediatr. Surg. 2016, 26, 481–486. [Google Scholar] [CrossRef] [PubMed]
- de Beer, S.A.; Gritter, M.; de Jong, J.R.; van Heurn, E.L.W. The Dynamic Compression Brace for Pectus Carinatum: Intermediate Results in 286 Patients. Ann. Thorac. Surg. 2017, 103, 1742–1749. [Google Scholar] [CrossRef]
- Fadnes, L.; Taube, A.; Tylleskär, T. The Internet Journal of Epidemiology How to identify information bias due to self-reporting in epidemiological research. Int. J. Epidemiol. 2009, 7, 28–38. [Google Scholar]









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Departments Experience | |
|---|---|
| Question | Answers N (%) |
| Number of new patients with pectus carinatum per year | |
| ≤25 | 15 (34) |
| 26–50 | 16 (37) |
| 51–75 | 5 (11) |
| 76–100 | 4 (9) |
| ≥101 | 4 (9) |
| What is your overall experience with PC external bracing? | |
| ≤3 years | 5 (11) |
| 4–6 years | 11 (25) |
| 7–9 years | 8 (18) |
| ≥10 years | 20 (46) |
| How many patients have you treated with COB successfully so far? | |
| ≤50 | 15 (34) |
| 51–100 | 9 (20) |
| 101–150 | 7 (16) |
| 151–200 | 2 (5) |
| ≥201 | 11 (25) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Omanik, P.; Sesia, S.B.; Kozlikova, K.; Schmidtova, V.; Funakova, M.; Haecker, F.-M. Bracing of Pectus Carinatum in Children: Current Practices. Children 2024, 11, 470. https://doi.org/10.3390/children11040470
Omanik P, Sesia SB, Kozlikova K, Schmidtova V, Funakova M, Haecker F-M. Bracing of Pectus Carinatum in Children: Current Practices. Children. 2024; 11(4):470. https://doi.org/10.3390/children11040470
Chicago/Turabian StyleOmanik, Pavol, Sergio Bruno Sesia, Katarina Kozlikova, Veronika Schmidtova, Miroslava Funakova, and Frank-Martin Haecker. 2024. "Bracing of Pectus Carinatum in Children: Current Practices" Children 11, no. 4: 470. https://doi.org/10.3390/children11040470
APA StyleOmanik, P., Sesia, S. B., Kozlikova, K., Schmidtova, V., Funakova, M., & Haecker, F.-M. (2024). Bracing of Pectus Carinatum in Children: Current Practices. Children, 11(4), 470. https://doi.org/10.3390/children11040470