
Assessment of Autoregulation of the Cerebral Circulation during Acute Lung Injury in a Neonatal Porcine Model

 , ,
, ,
Abstract
1. Introduction
2. Materials and Methods
2.1. Data Analysis
2.2. Statistical Analysis
3. Results
3.1. Hemodynamics
3.2. Indices of Lung Injury
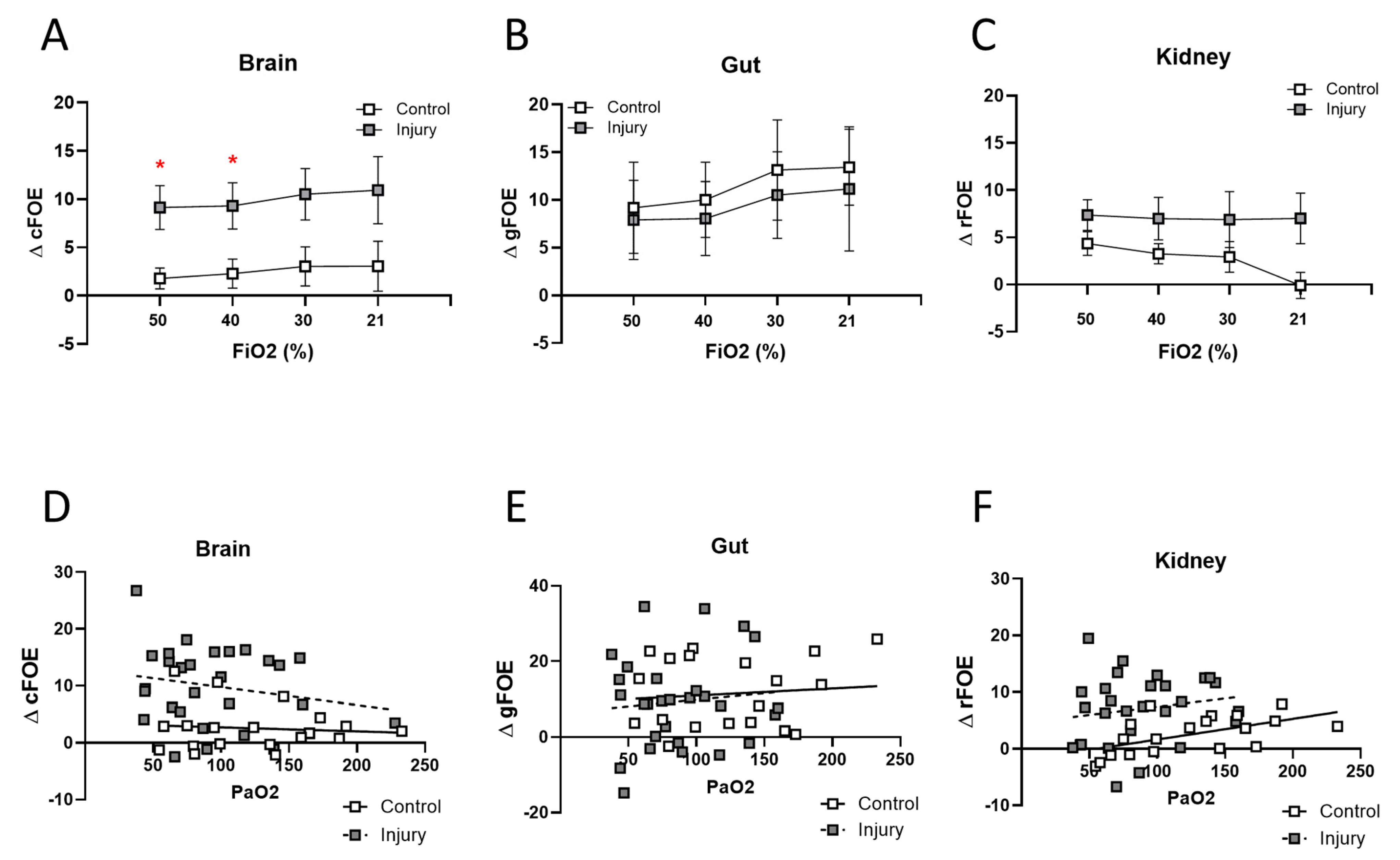
3.3. NIRS Assessment
4. Discussion
4.1. Oleic Acid Lung Injury Model
4.2. NIRS Data
4.3. Autoregulation
4.4. Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- De Luca, D.; van Kaam, A.H.; Tingay, D.G.; Courtney, S.E.; Danhaive, O.; Carnielli, V.P.; Zimmermann, L.J.; Kneyber, M.C.J.; Tissieres, P.; Brierley, J.; et al. The Montreux definition of neonatal ARDS: Biological and clinical background behind the description of a new entity. Lancet Respir. Med. 2017, 5, 657–666. [Google Scholar] [CrossRef]
- Verheijen, A.C.; Janssen, E.E.R.; van der Putten, M.E.; van Horck, M.W.P.; van Well, G.T.J.; Van Loo, I.H.M.; Hutten, M.C.; Van Mechelen, K. Management of severe neonatal respiratory distress due to vertical transmission of severe acute respiratory syndrome coronavirus 2: A case report. J. Med. Case Rep. 2022, 16, 140. [Google Scholar] [CrossRef]
- Saugstad, O.D. The role of oxygen in neonatal resuscitation. Clin. Perinatol. 2004, 31, 431–443. [Google Scholar] [CrossRef]
- Cummings, J.J.; Polin, R.A. Oxygen Targeting in Extremely Low Birth Weight Infants. Pediatrics 2016, 138, e20161576. [Google Scholar] [CrossRef]
- Kayton, A.; Timoney, P.; Vargo, L.; Perez, J.A. A Review of Oxygen Physiology and Appropriate Management of Oxygen Levels in Premature Neonates. Adv. Neonatal Care Off. J. Natl. Assoc. Neonatal Nurses 2018, 18, 98–104. [Google Scholar] [CrossRef]
- Sweet, D.G.; Carnielli, V.; Greisen, G.; Hallman, M.; Ozek, E.; Te Pas, A.; Plavka, R.; Roehr, C.C.; Saugstad, O.D.; Simeoni, U.; et al. European Consensus Guidelines on the Management of Respiratory Distress Syndrome—2019 Update. Neonatology 2019, 115, 432–450. [Google Scholar] [CrossRef]
- Elsayed, Y.N.; Fraser, D. Integrated Evaluation of Neonatal Hemodynamics Program Optimizing Organ Perfusion and Performance in Critically Ill Neonates, Part 1: Understanding Physiology of Neonatal Hemodynamics. Neonatal Netw. NN 2016, 35, 143–150. [Google Scholar] [CrossRef]
- Weber, F.; Scoones, G.P. A practical approach to cerebral near-infrared spectroscopy (NIRS) directed hemodynamic management in noncardiac pediatric anesthesia. Paediatr. Anaesth. 2019, 29, 993–1001. [Google Scholar] [CrossRef]
- Elsayed, Y.N.; Hinton, M.; Graham, R.; Dakshinamurti, S. Lung ultrasound predicts histological lung injury in a neonatal model of acute respiratory distress syndrome. Pediatr. Pulmonol. 2020, 55, 2913–2923. [Google Scholar] [CrossRef]
- Moodley, Y.; Sturm, M.; Shaw, K.; Shimbori, C.; Tan, D.B.; Kolb, M.; Graham, R. Human mesenchymal stem cells attenuate early damage in a ventilated pig model of acute lung injury. Stem Cell Res. 2016, 17, 25–31. [Google Scholar] [CrossRef]
- Matute-Bello, G.; Downey, G.; Moore, B.B.; Groshong, S.D.; Matthay, M.A.; Slutsky, A.S.; Kuebler, W.M. An official American Thoracic Society workshop report: Features and measurements of experimental acute lung injury in animals. Am. J. Respir. Cell Mol. Biol. 2011, 44, 725–738. [Google Scholar] [CrossRef]
- Sidorenko, I.; Turova, V.; Botkin, N.; Eckardt, L.; Alves-Pinto, A.; Felderhoff-Muser, U.; Rieger-Fackeldey, E.; Kovtanyuk, A.; Lampe, R. Modeling Cerebral Blood Flow Dependence on Carbon Dioxide and Mean Arterial Blood Pressure in the Immature Brain With Accounting for the Germinal Matrix. Front. Neurol. 2018, 9, 812. [Google Scholar] [CrossRef]
- Elsayed, Y.N.; Dakshinamurti, S. Titration of inspired oxygen in preterm infants with hypoxemic respiratory failure using near-infrared spectroscopy and pulse oximetry: A new approach. Pediatr. Pulmonol. 2021, 56, 3870–3878. [Google Scholar] [CrossRef]
- Alderliesten, T.; Dix, L.; Baerts, W.; Caicedo, A.; van Huffel, S.; Naulaers, G.; Groenendaal, F.; van Bel, F.; Lemmers, P. Reference values of regional cerebral oxygen saturation during the first 3 days of life in preterm neonates. Pediatr. Res. 2016, 79, 55–64. [Google Scholar] [CrossRef]
- Zubrow, A.B.; Hulman, S.; Kushner, H.; Falkner, B. Determinants of blood pressure in infants admitted to neonatal intensive care units: A prospective multicenter study. Philadelphia Neonatal Blood Pressure Study Group. J. Perinatol. Off. J. Calif. Perinat. Assoc. 1995, 15, 470–479. [Google Scholar]
- Altaany, D.; Natarajan, G.; Gupta, D.; Zidan, M.; Chawla, S. Severe Intraventricular Hemorrhage in Extremely Premature Infants: Are high Carbon Dioxide Pressure or Fluctuations the Culprit? Am. J. Perinatol. 2015, 32, 839–844. [Google Scholar] [CrossRef]
- Amer, R.; Kalash, R.; Seshia, M.M.; Elsayed, Y.N. The Impact of Integrated Evaluation of Hemodynamics on Management of Preterm Infants with Late-Onset Compromised Systemic Circulation. Am. J. Perinatol. 2017, 34, 1011–1019. [Google Scholar] [CrossRef]
- Matute-Bello, G.; Frevert, C.W.; Martin, T.R. Animal models of acute lung injury. Am. J. Physiol. Lung Cell. Mol. Physiol. 2008, 295, L379–L399. [Google Scholar] [CrossRef]
- Tisoncik, J.R.; Korth, M.J.; Simmons, C.P.; Farrar, J.; Martin, T.R.; Katze, M.G. Into the eye of the cytokine storm. Microbiol. Mol. Biol. Rev. MMBR 2012, 76, 16–32. [Google Scholar] [CrossRef]
- Graham, M.R.; Gulati, H.; Kha, L.; Girling, L.G.; Goertzen, A.; Mutch, W.A. Resolution of pulmonary edema with variable mechanical ventilation in a porcine model of acute lung injury. Can. J. Anaesth.=J. Can. D’Anesth. 2011, 58, 740–750. [Google Scholar] [CrossRef]
- Gulasti, F.; Gulasti, S.; Sari, S. Tricuspid annular plane systolic excursion to predict arterial hypotension caused by general anesthesia induction. Minerva Anestesiol. 2023, 89, 265–272. [Google Scholar] [CrossRef]
- Giovanardi, P.; Tincani, E.; Maioli, M.; Tondi, S. The Prognostic Importance of TAPSE in Early and in Stable Cardiovascular Diseases. J. Cardiovasc. Dev. Dis. 2020, 7, 4. [Google Scholar] [CrossRef]
- Kamuf, J.; Garcia-Bardon, A.; Ziebart, A.; Thomas, R.; Folkert, K.; Frauenknecht, K.; Thal, S.C.; Hartmann, E.K. Lung injury does not aggravate mechanical ventilation-induced early cerebral inflammation or apoptosis in an animal model. PLoS ONE 2018, 13, e0202131. [Google Scholar] [CrossRef]
- Hou, X.; Ding, H.; Teng, Y.; Zhou, C.; Tang, X.; Li, S. Research on the relationship between brain anoxia at different regional oxygen saturations and brain damage using near-infrared spectroscopy. Physiol. Meas. 2007, 28, 1251–1265. [Google Scholar] [CrossRef]
- Kurth, C.D.; McCann, J.C.; Wu, J.; Miles, L.; Loepke, A.W. Cerebral oxygen saturation-time threshold for hypoxic-ischemic injury in piglets. Anesth. Analg. 2009, 108, 1268–1277. [Google Scholar] [CrossRef]
- Ringer, S.K.; Clausen, N.G.; Spielmann, N.; Weiss, M. Effects of moderate and severe hypocapnia on intracerebral perfusion and brain tissue oxygenation in piglets. Paediatr. Anaesth. 2019, 29, 1114–1121. [Google Scholar] [CrossRef]
- Silvera, F.; Gagliardi, T.; Vollono, P.; Fernandez, C.; Garcia-Bayce, A.; Berardi, A.; Badia, M.; Beltran, B.; Cabral, T.; Abella, P.; et al. Study of the relationship between regional cerebral saturation and pCO2 changes during mechanical ventilation to evaluate modifications in cerebral perfusion in a newborn piglet model. Braz. J. Med. Biol. Res.=Rev. Bras. Pesqui. Medicas Biol. 2022, 55, e11543. [Google Scholar] [CrossRef]
- Chen, M.W.; Reyes, M.; Kulikowicz, E.; Martin, L.; Hackam, D.J.; Koehler, R.C.; Lee, J.K. Abdominal near-infrared spectroscopy in a piglet model of gastrointestinal hypoxia produced by graded hypoxia or superior mesenteric artery ligation. Pediatr. Res. 2018, 83, 1172–1181. [Google Scholar] [CrossRef]
- Heuer, J.F.; Pelosi, P.; Hermann, P.; Perske, C.; Crozier, T.A.; Bruck, W.; Quintel, M. Acute effects of intracranial hypertension and ARDS on pulmonary and neuronal damage: A randomized experimental study in pigs. Intensive Care Med. 2011, 37, 1182–1191. [Google Scholar] [CrossRef]
- McNeill, S.; Gatenby, J.C.; McElroy, S.; Engelhardt, B. Normal cerebral, renal and abdominal regional oxygen saturations using near-infrared spectroscopy in preterm infants. J. Perinatol. Off. J. Calif. Perinat. Assoc. 2011, 31, 51–57. [Google Scholar] [CrossRef]
- Montaldo, P.; De Leonibus, C.; Giordano, L.; De Vivo, M.; Giliberti, P. Cerebral, renal and mesenteric regional oxygen saturation of term infants during transition. J. Pediatr. Surg. 2015, 50, 1273–1277. [Google Scholar] [CrossRef]
- Holler, N.; Urlesberger, B.; Mileder, L.; Baik, N.; Schwaberger, B.; Pichler, G. Peripheral Muscle Near-Infrared Spectroscopy in Neonates: Ready for Clinical Use? A Systematic Qualitative Review of the Literature. Neonatology 2015, 108, 233–245. [Google Scholar] [CrossRef]
- Rhee, C.J.; da Costa, C.S.; Austin, T.; Brady, K.M.; Czosnyka, M.; Lee, J.K. Neonatal cerebrovascular autoregulation. Pediatr. Res. 2018, 84, 602–610. [Google Scholar] [CrossRef]
- Mardimae, A.; Balaban, D.Y.; Machina, M.A.; Battisti-Charbonney, A.; Han, J.S.; Katznelson, R.; Minkovich, L.L.; Fedorko, L.; Murphy, P.M.; Wasowicz, M.; et al. The interaction of carbon dioxide and hypoxia in the control of cerebral blood flow. Pflug. Arch. Eur. J. Physiol. 2012, 464, 345–351. [Google Scholar] [CrossRef]
- Soul, J.S.; Hammer, P.E.; Tsuji, M.; Saul, J.P.; Bassan, H.; Limperopoulos, C.; Disalvo, D.N.; Moore, M.; Akins, P.; Ringer, S.; et al. Fluctuating pressure-passivity is common in the cerebral circulation of sick premature infants. Pediatr. Res. 2007, 61, 467–473. [Google Scholar] [CrossRef]
- Pryds, O.; Edwards, A.D. Cerebral blood flow in the newborn infant. Arch. Dis. Child. Fetal Neonatal Ed. 1996, 74, F63–F69. [Google Scholar] [CrossRef]
- Pezzato, S.; Govindan, R.B.; Bagnasco, F.; Panagopoulos, E.M.; Robba, C.; Beqiri, E.; Smielewski, P.; Munoz, R.A.; d’Udekem, Y.; Moscatelli, A.; et al. Cerebral autoregulation monitoring using the cerebral oximetry index after neonatal cardiac surgery: A single-center retrospective cohort study. J. Thorac. Cardiovasc. Surg. 2023. [Google Scholar] [CrossRef]
- Kooi, E.M.W.; Verhagen, E.A.; Elting, J.W.J.; Czosnyka, M.; Austin, T.; Wong, F.Y.; Aries, M.J.H. Measuring cerebrovascular autoregulation in preterm infants using near-infrared spectroscopy: An overview of the literature. Expert Rev. Neurother. 2017, 17, 801–818. [Google Scholar] [CrossRef]
- Michelet, D.; Arslan, O.; Hilly, J.; Mangalsuren, N.; Brasher, C.; Grace, R.; Bonnard, A.; Malbezin, S.; Nivoche, Y.; Dahmani, S. Intraoperative changes in blood pressure associated with cerebral desaturation in infants. Paediatr. Anaesth. 2015, 25, 681–688. [Google Scholar] [CrossRef]
- Ringer, S.K.; Clausen, N.G.; Spielmann, N.; Ohlerth, S.; Schwarz, A.; Weiss, M. Effects of moderate and severe arterial hypotension on intracerebral perfusion and brain tissue oxygenation in piglets. Br. J. Anaesth. 2018, 121, 1308–1315. [Google Scholar] [CrossRef] [PubMed]
- Hahn, G.H.; Heiring, C.; Pryds, O.; Greisen, G. Cerebral vascular effects of hypovolemia and dopamine infusions: A study in newborn piglets. Acta Paediatr. 2012, 101, 736–742. [Google Scholar] [CrossRef]
- Ringer, S.K.; Ohlerth, S.; Carrera, I.; Mauch, J.; Spielmann, N.; Bettschart-Wolfensberger, R.; Weiss, M. Effects of hypotension and/or hypocapnia during sevoflurane anesthesia on perfusion and metabolites in the developing brain of piglets-a blinded randomized study. Paediatr. Anaesth. 2016, 26, 909–918. [Google Scholar] [CrossRef]
- Rhondali, O.; Andre, C.; Pouyau, A.; Mahr, A.; Juhel, S.; De Queiroz, M.; Rhzioual-Berrada, K.; Mathews, S.; Chassard, D. Sevoflurane anesthesia and brain perfusion. Paediatr. Anaesth. 2015, 25, 180–185. [Google Scholar] [CrossRef]
- Ziaka, M.; Exadaktylos, A. ARDS associated acute brain injury: From the lung to the brain. Eur. J. Med. Res. 2022, 27, 150. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Control | Injury | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Baseline | 1 h Post | 40% FiO2 | 30% FiO2 | 21% FiO2 | Baseline | 1 h Post | 40% FiO2 | 30% FiO2 | 21% FiO2 | ||
| weight | mean | 2.13 | 2.177 | ||||||||
| SE | 0.09 | 0.146 | |||||||||
| HR | mean | 155.7 | 155.5 | 157.8 | 154.8 | 171.2 | 157.9 | 154.4 | 162.0 | 161.0 | 187.6 |
| SE | 14.3 | 14.3 | 17.1 | 21.0 | 25.7 | 5.0 | 10.7 | 10.7 | 15.7 | 18.0 | |
| BP | mean | 84.3 | 81.7 | 78.8 | 74.8 | 74.0 | 77.3 | 70.7 | 68.4 | 71.6 | 70.3 |
| SE | 4.3 | 4.8 | 5.4 | 5.5 | 7.1 | 3.3 | 3.0 | 3.3 | 5.6 | 7.1 | |
| Systolic BP | mean | 113.2 | 109.7 | 106.5 | 101.6 | 101.0 | 102.3 | 94.9 * | 94.4 | 92.9 | 93.6 |
| SE | 5.6 | 5.1 | 5.1 | 5.2 | 7.8 | 4.2 | 3.2 | 4.9 | 5.3 | 7.2 | |
| Diastolic BP | mean | 65.3 | 64.7 | 62.2 | 59.6 | 58.4 | 59.9 | 54.1 | 55.6 | 56.9 | 54.7 |
| SE | 3.1 | 5.6 | 6.2 | 6.7 | 7.5 | 2.6 | 2.8 | 5.5 | 5.7 | 7.0 | |
| CVP | mean | 7.7 | 7.5 | 7.3 | 7.2 | 7.2 | 6.4 | 6.1 | 5.9 | 5.9 | 5.9 |
| SE | 0.6 | 0.3 | 0.4 | 0.5 | 0.6 | 0.5 | 0.4 | 0.4 | 0.4 | 0.4 | |
| temp | mean | 36.7 | 37.9 | 37.5 | 37.4 | 37.1 | 36.7 | 37.7 | 37.7 | 37.6 | 37.5 |
| SE | 0.2 | 0.3 | 0.2 | 0.2 | 0.2 | 0.2 | 0.3 | 0.2 | 0.2 | 0.2 | |
| PI | mean | 0.72 | 0.80 | 0.80 | 0.79 | 0.81 | 0.90 | 0.56 | 0.72 | 0.56 | 0.57 |
| SE | 0.11 | 0.14 | 0.13 | 0.15 | 0.15 | 0.14 | 0.07 | 0.09 | 0.06 | 0.08 | |
| rcSO2 | rgSO2 | rrSO2 | ||||
|---|---|---|---|---|---|---|
| FiO2 | Control | OA | Control | OA | Control | OA |
| Baseline 50% | 50.4 (2.7) | 54.6 (2.6) | 66.5 (6.2) | 61.9 (4.4) | 47.7 (6.0) | 60.6 (5.0) |
| 1 h 50% | 48.3 (2.6) | 44.9 (1.4) | 57.8 (7.4) | 53.3 (2.7) | 48.6 (2.7) | 52.6 (5.7) |
| 40% | 47.5 (2.5) | 42.6 (0.7) | 57.7 (5.8) | 50.6 (2.0) | 49.6 (2.4) | 50.4 (4.2) |
| 30% | 46.3 (2.6) | 38.4 (1.0) | 53.5 (4.1) | 44.7 (2.3) | 48.6 (2.5) | 47.0 (4.0) |
| 21% | 41.2 (3.2) | 27.9 (2.6) ** | 46.5 (4.7) | 32.0 (2.5) | 45.4 (2.8) | 34.0 (3.2) |
| SaO2 Range (Post Injury or Sham) | N | rcSO2 Post Injury | rcSO2 > 20% Decrease | |||
|---|---|---|---|---|---|---|
| C | OA | C | OA | C | OA | |
| 95–100% | 17 | 11 | 48.5 (1.6) | 44.1(1.0) | 1 ( 5%) | 7 (64%) |
| 90–95% | 3 | 5 | 47.3 (3.5) | 40.8 (0.8) | 0 (0%) | 4 (80%) |
| 85–90% | 1 | 3 | 37 (0) | 35.5 (1.2) | 1 (100%) | 3 (100%) |
| <85% | 3 | 9 | 36.6 (2.7) | 30.1 (2.6) | 2 (67%) | 8 (89%) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Memisoglu, A.; Hinton, M.; Elsayed, Y.; Graham, R.; Dakshinamurti, S. Assessment of Autoregulation of the Cerebral Circulation during Acute Lung Injury in a Neonatal Porcine Model. Children 2024, 11, 611. https://doi.org/10.3390/children11050611
Memisoglu A, Hinton M, Elsayed Y, Graham R, Dakshinamurti S. Assessment of Autoregulation of the Cerebral Circulation during Acute Lung Injury in a Neonatal Porcine Model. Children. 2024; 11(5):611. https://doi.org/10.3390/children11050611
Chicago/Turabian StyleMemisoglu, Asli, Martha Hinton, Yasser Elsayed, Ruth Graham, and Shyamala Dakshinamurti. 2024. "Assessment of Autoregulation of the Cerebral Circulation during Acute Lung Injury in a Neonatal Porcine Model" Children 11, no. 5: 611. https://doi.org/10.3390/children11050611
APA StyleMemisoglu, A., Hinton, M., Elsayed, Y., Graham, R., & Dakshinamurti, S. (2024). Assessment of Autoregulation of the Cerebral Circulation during Acute Lung Injury in a Neonatal Porcine Model. Children, 11(5), 611. https://doi.org/10.3390/children11050611