
Sleep-Disordered Breathing and Associated Comorbidities among Preschool-Aged Children with Down Syndrome

 ,
,  ,
, 


Abstract
1. Introduction
2. Methods
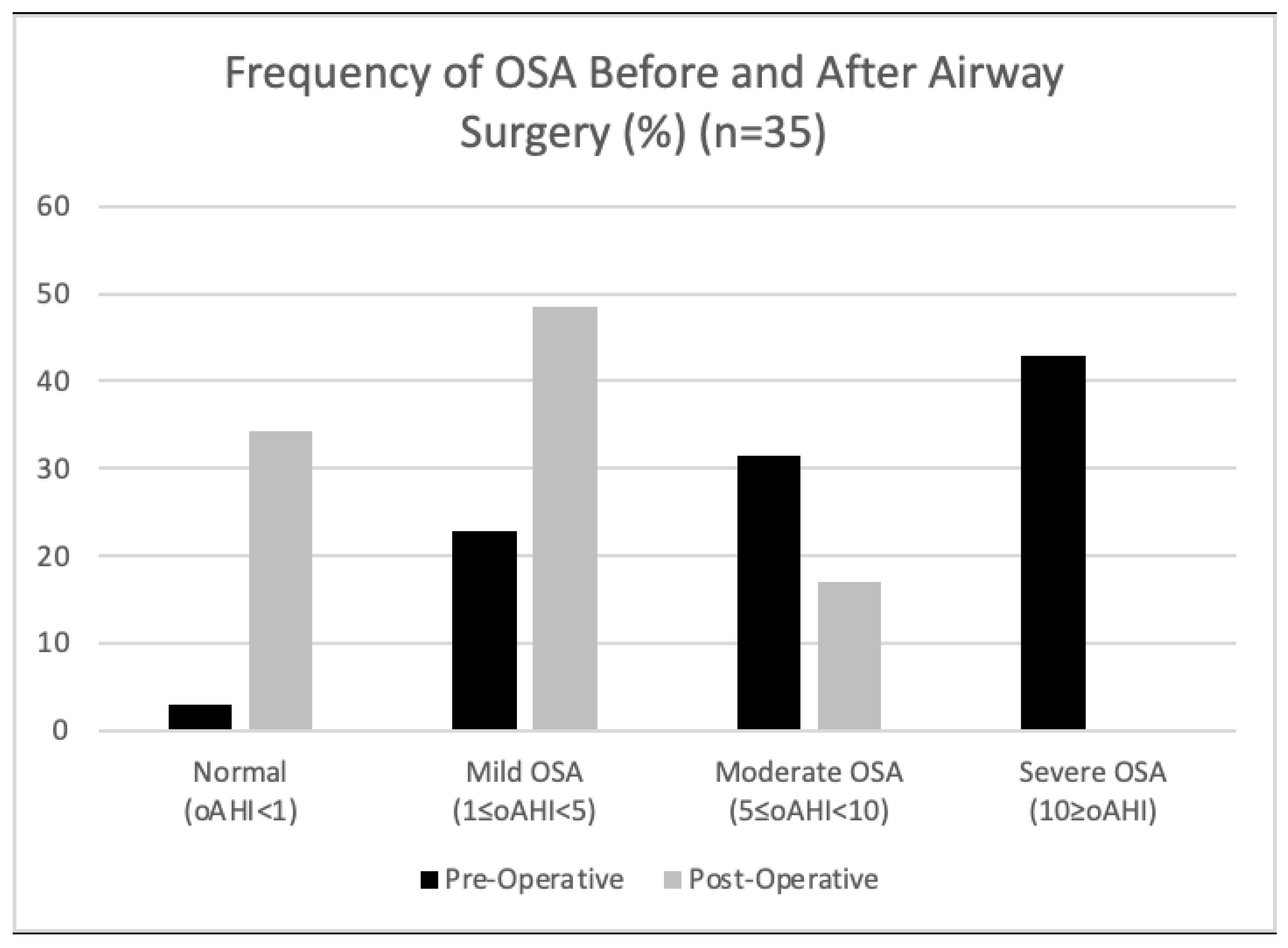
3. Results
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Parker, S.E.; Mai, C.T.; Canfield, M.A.; Rickard, R.; Wang, Y.; Meyer, R.E.; Anderson, P.; Mason, C.A.; Collins, J.S.; Kirby, R.S.; et al. National Birth Defects Prevention Network. Updated National Birth Prevalence estimates for selected birth defects in the United States, 2004–2006. Birth Defects Res. A Clin. Mol. Teratol. 2010, 88, 1008–1016. [Google Scholar] [CrossRef]
- Weijerman, M.E.; de Winter, J.P. Clinical practice. The care of children with Down syndrome. Eur. J. Pediatr. 2010, 169, 1445–1452. [Google Scholar] [CrossRef]
- Gastelum, E.; Cummins, M.; Singh, A.; Montoya, A.; Urbano, G.L.; Tablizo, M.A. Treatment Considerations for Obstructive Sleep Apnea in Pediatric Down Syndrome. Children 2021, 8, 1074. [Google Scholar] [CrossRef] [PubMed]
- Lee, C.-F.; Lee, C.-H.; Hsueh, W.-Y.; Lin, M.-T.; Kang, K.-T. Prevalence of Obstructive Sleep Apnea in Children with Down Syndrome: A Meta-Analysis. J. Clin. Sleep Med. 2018, 14, 867–875. [Google Scholar] [CrossRef]
- Qubty, W.F.; Mrelashvili, A.; Kotagal, S.; Lloyd, R.M. Comorbidities in infants with obstructive sleep apnea. J. Clin. Sleep Med. 2014, 10, 1213–1216. [Google Scholar] [CrossRef]
- Lumeng, J.C.; Chervin, R.D. Epidemiology of pediatric obstructive sleep apnea. Proc. Am. Thorac. Soc. 2008, 5, 242–252. [Google Scholar] [CrossRef]
- Maris, M.; Verhulst, S.; Wojciechowski, M.; Van de Heyning, P.; Boudewyns, A. Prevalence of Obstructive Sleep Apnea in Children with Down Syndrome. Sleep 2016, 39, 699–704. [Google Scholar] [CrossRef]
- Bull, M.J. Health supervision for children with Down syndrome. Pediatrics 2011, 128, 393–406. [Google Scholar] [CrossRef]
- Esbensen, A.J.; Beebe, D.W.; Byars, K.C.; Hoffman, E.K. Use of sleep evaluations and treatments in children with down syndrome. J. Dev. Behav. Pediatr. 2016, 37, 629–636. [Google Scholar] [CrossRef]
- Bassell, J.L.; Phan, H.; Leu, R.; Kronk, R.; Visootsak, J. Sleep profiles in children with Down syndrome. Am. J. Med. Genet. Part A 2015, 167, 1830–1835. [Google Scholar] [CrossRef]
- Breslin, J.; Spanò, G.; Bootzin, R.; Anand, P.; Nadel, L.; Edgin, J. Obstructive sleep apnea syndrome and cognition in down syndrome. Dev. Med. Child Neurol. 2014, 56, 657–664. [Google Scholar] [CrossRef] [PubMed]
- Capdevila, O.S.; Kheirandish-Gozal, L.; Dayyat, E.; Gozal, D. Pediatric obstructive sleep apnea: Complications, management, and long-term outcomes. Proc. Am. Thorac. Soc. 2008, 5, 274–282. [Google Scholar] [CrossRef] [PubMed]
- Lal, C.; White, D.R.; Joseph, J.E.; van Bakergem, K.; LaRosa, A. Sleep-disordered breathing in Down syndrome. Chest 2015, 147, 570–579. [Google Scholar] [CrossRef] [PubMed]
- Simpson, R.; Oyekan, A.A.; Ehsan, Z.; Ingram, D.G. Obstructive sleep apnea in patients with Down syndrome: Current perspectives. Nat. Sci. Sleep 2018, 10, 287–293. [Google Scholar] [CrossRef]
- Anand, V.; Shukla, G.; Gupta, N.; Gupta, A.; Sapra, S.; Gulati, S.; Pandey, R.M.; Pandey, S.; Kabra, M. Association of Sleep Apnea with Development and Behavior in Down Syndrome: A Prospective Clinical and Polysomnographic Study. Pediatr. Neurol. 2021, 116, 7–13. [Google Scholar] [CrossRef] [PubMed]
- Lee, N.C.; Hsu, W.C.; Chang, L.M.; Chen, Y.C.; Huang, P.T.; Chien, C.C.; Chien, Y.H.; Chen, C.L.; Hwu, W.L.; Lee, P.L. REM sleep and sleep apnea are associated with language function in Down syndrome children: An analysis of a community sample. J. Formos. Med. Assoc. 2020, 119 Pt 3, 516–523. [Google Scholar] [CrossRef] [PubMed]
- Joyce, A.; Elphick, H.; Farquhar, M.; Gringras, P.; Evans, H.; Bucks, R.S.; Kreppner, J.; Kingshott, R.; Martin, J.; Reynolds, J.; et al. Obstructive Sleep Apnoea Contributes to Executive Function Impairment in Young Children with Down Syndrome. Behav. Sleep Med. 2020, 18, 611–621. [Google Scholar] [CrossRef] [PubMed]
- Farhood, Z.; Isley, J.W.; Ong, A.A.; Nguyen, S.A.; Camilon, T.J.; LaRosa, A.C.; White, D.R. Adenotonsillectomy outcomes in patients with Down syndrome and obstructive sleep apnea. Laryngoscope 2017, 127, 1465–1470. [Google Scholar] [CrossRef] [PubMed]
- Jeans, W.D.; Fernando, D.C.; Maw, A.R.; Leighton, B.C. Along itudinal study of the growth of the nasopharynx and its contents in normal children. Br. J. Radiol. 1981, 54, 117–121. [Google Scholar] [CrossRef]
- Song, S.A.; Tolisano, A.M.; Cable, B.B.; Camacho, M. Neurocognitive outcomes after pediatric adenotonsillectomy for obstructive sleep apnea: A systematic review and meta-analysis. Int. J. Pediatr. Otorhinolaryngol. 2016, 83, 205–210. [Google Scholar] [CrossRef]
- Di Sessa, A.; Messina, G.; Bitetti, I.; Falanga, C.; Farello, G.; Verrotti, A.; Carotenuto, M. Cardiometabolic risk profile in non-obese children with obstructive sleep apnea syndrome. Eur. J. Pediatr. 2022, 181, 1689–1697. [Google Scholar] [CrossRef] [PubMed]
- Berry, R.B.; Budhiraja, R.; Gottlieb, D.J.; Gozal, D.; Iber, C.; Kapur, V.K.; Marcus, C.L.; Mehra, R.; Parthasarathy, S.; Quan, S.F.; et al. Rules for scoring respiratory events in sleep: Update of the 2007 AASM Manual for the scoring of sleep and associated events. J. Clin. Sleep Med. 2012, 08, 597–619. [Google Scholar] [CrossRef] [PubMed]
- Richard, N.; Beydon, N.; Berdah, L.; Corvol, H.; Aubertin, G.; Taytard, J. Nocturnal hypoventilation in Down syndrome children with or without sleep apnea. Pediatr. Pulmonol. 2020, 55, 1246–1253. [Google Scholar] [CrossRef] [PubMed]
- Trucco, F.; Chatwin, M.; Semple, T.; Rosenthal, M.; Bush, A.; Tan, H.L. Sleep disordered breathing and ventilatory support in children with Down syndrome. Pediatr. Pulmonol. 2018, 53, 1414–1421. [Google Scholar] [CrossRef] [PubMed]
- Fan, Z.; Ahn, M.; Roth, H.L.; Li, L.; Vaughn, B.V. Sleep apnea and hypoventilation in patients with Down syndrome: Analysis of 144 polysomnogram studies. Children 2017, 4, 55. [Google Scholar] [CrossRef] [PubMed]
- Suri, S.; Tompson, B.D.; Cornfoot, L. Cranial base, maxillary and mandibular morphology in Down syndrome. Angle Orthod. 2010, 80, 861–869. [Google Scholar] [CrossRef] [PubMed]
- Takahashi, T.; Sakai, N.; Iwasaki, T.; Doyle, T.C.; Mobley, W.C.; Nishino, S. Detailed evaluation of the upper airway in the Dp(16)1Yey mouse model of Down syndrome. Sci. Rep. 2020, 10, 21323. [Google Scholar] [CrossRef] [PubMed]
- De Lausnay, M.; Verhulst, S.; Van Hoorenbeeck, K.; Boudewyns, A. Obstructive Sleep Disorders in Down Syndrome’s Children with and without Lower Airway Anomalies. Children 2021, 8, 693. [Google Scholar] [CrossRef] [PubMed]
- Romero-Corral, A.; Caples, S.M.; Lopez-Jimenez, F.; Somers, V.K. Interactions between obesity and obstructive sleep apnea: Implications for treatment. Chest 2010, 137, 711–719. [Google Scholar] [CrossRef]
- Van Gameren-Oosterom, H.B.; van Dommelen, P.; Schönbeck, Y.; Oudesluys-Murphy, A.M.; van Wouwe, J.P.; Buitendijk, S.E. Prevalence of overweight in Dutch children with Down syndrome. Pediatrics 2012, 130, e1520–e1526. [Google Scholar] [CrossRef]
- Yu, W.; Sarber, K.M.; Howard, J.J.M.; Huang, G.; Hossain, M.M.; Heubi, C.H.; Lu, X.; Simakajornboon, N. Children with Down syndrome and mild OSA: Treatment with medication versus observation. J. Clin. Sleep Med. 2020, 16, 899–906. [Google Scholar] [CrossRef] [PubMed]
- Cho, Y.; Kwon, Y.; DelRosso, L.; Sobremonte-King, M. Dysphagia severity is associated with worse sleep-disordered breathing in infants with Down Syndrome. J. Clin. Sleep Med. 2023, 19, 883–887. [Google Scholar] [CrossRef] [PubMed]
- Connolly, H.V.; Tomaselli, L.T.; McKenna, B.M.K. Adenotonsillectomy for Pediatric Obstructive Sleep Apnea: How to Predict Those at Risk for Postoperative Complications. J. Clin. Sleep Med. 2020, 16, 3–4. [Google Scholar] [CrossRef] [PubMed]
- Rayasam, S.; Johnson, R.; Lenahan, D.; Abijay, C.; Mitchell, R.B. Obstructive Sleep Apnea in Children Under 3 Years of Age. Laryngoscope 2021, 131, E2603–E2608. [Google Scholar] [CrossRef] [PubMed]
- Maris, M.; Verhulst, S.; Wojciechowski, M.; Van de Heyning, P.; Boudewyns, A. Outcome of adenotonsillectomy in children with Down syndrome and obstructive sleep apnoea. Arch. Dis. Child. 2017, 102, 331–336. [Google Scholar] [CrossRef] [PubMed]
- Nerfeldt, P.; Sundelin, A. Obstructive sleep apnea in children with Down Syndrome—Prevalence and evaluation of surgical treatment. Int. J. Pediatr. Otorhinolaryngol. 2020, 133, 109968. [Google Scholar] [CrossRef] [PubMed]
- Ingram, D.G.; Amanda, G.; Ruiz, D.G.; Norman, R.F. Success of Tonsillectomy for Obstructive Sleep Apnea in Children with Down Syndrome. J. Clin. Sleep Med. JCSM Off. Publ. Am. Acad. Sleep Med. 2017, 13, 975–980. [Google Scholar] [CrossRef] [PubMed]
- Sudarsan, S.S.; Vijaya, K.P.; Senthil, V.A.; Sathiya, M.; Mohan, K. Comparison of Treatment Modalities in Syndromic Children with Obstructive Sleep Apnea—A Randomized Cohort Study. Int. J. Pediatr. Otorhinolaryngol. 2014, 78, 1526–1533. [Google Scholar] [CrossRef]
- Shete, M.M.; Stocks, R.M.S.; Sebelik, M.E.; Schoumacher, R.A. Effects of Adeno-Tonsillectomy on Polysomnography Patterns in Down Syndrome Children with Obstructive Sleep Apnea: A Comparative Study with Children without Down Syndrome. Int. J. Pediatr. Otorhinolaryngol. 2010, 74, 241–244. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Race | % |
| American Indian | 0.0 |
| Asian | 13.3 |
| Black or African American | 1.3 |
| Native Hawaiian or Other Pacific Islander | 1.3 |
| White | 54.7 |
| Other or multiple races | 24.0 |
| Declined to answer | 5.3 |
| Ethnicity | % |
| Hispanic | 20.0 |
| Non-Hispanic | 74.7 |
| Declined to answer | 5.3 |
| Mean (SD) | n | |
|---|---|---|
| Sleep efficiency (%) | 85.2% (8.68) | 75 |
| Total sleep time (min) | 481.2 (79.92) | 75 |
| Stage N1 % of sleep time | 8.4% (6.74) | 75 |
| Stage N2 % of sleep time | 42.5% (8.1) | 74 |
| Stage N3 % of sleep time | 29.9% (7.22) | 75 |
| Stage REM % of sleep time | 21.5% (14.93) | 75 |
| Total arousal index | 13.1 (4.74) | 75 |
| Respiratory Parameters | Mean (SD) | n |
|---|---|---|
| Total AHI | 10.30 (10.20) | 75 |
| OAHI | 7.9 (9.40) | 75 |
| CAI | 2.40 (2.40) | 75 |
| REM AHI | 19.8 (20.36) | 74 |
| NREM AHI | 8.6 (9.56) | 73 |
| Mean O2 saturation during sleep | 96.9% (1.92) | 75 |
| Nadir O2 saturation during sleep | 87.6% (5.48) | 75 |
| % Total sleep time O2 < 88% | 0.8% (6.16) | 75 |
| Oxygen desaturation index | 7.03 (7.65) | 75 |
| % Total sleep time ETCO2 > 50 mmHg | 7.9% (18.2) | 48 |
| % Total sleep time TcCO2 > 50 mmHg | 17.9% (24.46) | 45 |
| Respiratory Parameters | Pre-Surgery Mean (SD) | Post-Surgery Mean (SD) | * p Value (95% CI) | n |
|---|---|---|---|---|
| Total AHI | 14.9 (12.63) | 7.4 (5.42) | 0.0014 (−11.98, −3.143) | 35 |
| OAHI | 12.1 (11.99) | 4.8 (3.72) | 0.001 (−11.52, −3.18) | 35 |
| CAI | 2.8 (2.69) | 2.6 (2.49) | 0.63 (−1.07, 0.66) | 35 |
| REM AHI | 28.8 (26) | 12.2 (8.57) | 0.0007 (−25.64, −7.58) | 34 |
| NREM AHI | 12.0 (11.63) | 6.5 (5.15) | 0.013 (−9.70, −1.24) | 34 |
| Mean O2 saturation | 96.2% (2.43) | 96.9% (1.37) | 0.15 (−0.23, 0.9) | 35 |
| O2 saturation nadir | 85.4% (5.91) | 88.4% (3.97) | 0.009 (0.78, 5.14) | 35 |
| % Sleep time O2 < 88% | 1.6% (9.01) | 0.02% (0.05) | 0.3 (−4.68, 1.5) | 35 |
| ODI | 10.4 (9.59) | 5.3 (4.84) | 0.006 (−8.68, −1.6) | 35 |
| % Sleep time ETCO2 > 50 mmHg | 12.9% (27.33) | 7.2% (17.41) | 0.34 (−18.38, 6.88) | 14 |
| % Sleep time TcCO2 > 50 mmHg | 16.7% (22.4) | 12.2% (23.97) | 0.58 (−21.36, 12.27) | 19 |
| Sleep Parameters | Pre-Surgery Mean (SD) | Post Surgery Mean (SD) | * p Value (95% CI) | n |
|---|---|---|---|---|
| Sleep efficiency (%) | 86.1% (6.69) | 85.5% (8.31) | 0.013 (−3.49, 2.24) | 35 |
| Total sleep rime (min) | 469.5 (89.36) | 515.03 (54.59) | 0.013 (10.39, 80.6) | 35 |
| Stage N1 % of sleep time | 9.8% (7.19) | 7.7% (6.02) | 0.17 (−5.1, 0.96) | 35 |
| Stage N2 % of sleep time | 42.0% (9.3) | 43.3% (8.59) | 0.49 (−2.49, 5.11) | 34 |
| Stage N3 % of sleep time | 30.5% (8.74) | 29.1% (9.99) | 0.53 (−5.48, 2.85) | 35 |
| Stage REM % of sleep time | 20.5% (14.35) | 19.4% (6.48) | 0.005 (−6.65, 4.40) | 35 |
| Total arousal index | 14.7 (4.84) | 12.5 (4.80) | 0.014 (−3.94, −0.47) | 35 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kolstad, T.K.; DelRosso, L.M.; Tablizo, M.A.; Witmans, M.; Cho, Y.; Sobremonte-King, M. Sleep-Disordered Breathing and Associated Comorbidities among Preschool-Aged Children with Down Syndrome. Children 2024, 11, 651. https://doi.org/10.3390/children11060651
Kolstad TK, DelRosso LM, Tablizo MA, Witmans M, Cho Y, Sobremonte-King M. Sleep-Disordered Breathing and Associated Comorbidities among Preschool-Aged Children with Down Syndrome. Children. 2024; 11(6):651. https://doi.org/10.3390/children11060651
Chicago/Turabian StyleKolstad, Tessa K., Lourdes M. DelRosso, Mary Anne Tablizo, Manisha Witmans, Yeilim Cho, and Michelle Sobremonte-King. 2024. "Sleep-Disordered Breathing and Associated Comorbidities among Preschool-Aged Children with Down Syndrome" Children 11, no. 6: 651. https://doi.org/10.3390/children11060651
APA StyleKolstad, T. K., DelRosso, L. M., Tablizo, M. A., Witmans, M., Cho, Y., & Sobremonte-King, M. (2024). Sleep-Disordered Breathing and Associated Comorbidities among Preschool-Aged Children with Down Syndrome. Children, 11(6), 651. https://doi.org/10.3390/children11060651