Abstract
Background: Otic involvement is common in children during acute infectious diseases, and is an important cause of morbidity and health service utilization. Methods: We performed a retrospective analysis of pediatric cases hospitalized in the largest infectious disease hospital in Romania between 2018 and 2023, with the aim of quantifying the incidence and impact of acute otitis (AO) according to pediatric age subgroups. Results: A total of 1118 cases diagnosed with AO were eligible and included in the analysis. Acute congestive otitis media was the most common subtype, identified in 53.3% of cases, followed by acute purulent otitis media (APOM) in 26.7% of children. The majority of AO cases (69.9%) were diagnosed in the pre-pandemic period (2018–2019), and infants (10.6%), toddlers (49.4%), and preschoolers (29.2%) were the most affected age groups. A viral infection associated with the AO episode was documented in 49.6% of cases. Influenza viruses were most commonly reported (20.5%), followed by SARS-CoV-2 (5.8%), and adenovirus (4.9%). A total of 38 cases of AO were identified in children with measles. In 15.9% of APOM cases, Streptococcus pneumoniae was isolated by culture from otic secretions. The duration of hospitalization was longer in children with APOM and acute otitis externa compared to the other subtypes of AO (p < 0.001). Conclusions: Our study highlights the importance of ENT (ear, nose, and throat) monitoring in children hospitalized for acute infectious diseases, as the majority of AO cases occur in the context of a viral infection. These findings emphasize the necessity for tailored assessment and intervention in suspected cases of AO, especially in young children under 5 years of age.
1. Introduction
Otic involvement is commonly observed in children during acute infectious disease and is an important cause of morbidity and healthcare service use [1]. Acute otitis (AO) occurs commonly during or after an upper respiratory tract infection [2], either as a result of direct viral action, inflammation, or poor drainage of secretions, or as a result of bacterial superinfection [3]. The occurrence of AO is greater in the pediatric population than in adults. This is attributed to a number of anatomical, immunological, and behavioral factors unique to the pediatric age group [4,5]. In total, over 80% of children experience at least one episode of AO, with 51% of cases reported in children under the age of five [1].
AO is also a significant contributor to antibiotic prescribing in the pediatric population, although a significant proportion of cases can and should be managed without antimicrobial treatment. Analgesic therapy is the preferred treatment option, while antibiotic treatment may be delayed in children two years of age and older, or in those with mild symptoms [6]. Thus, otic involvement should be carefully assessed by the otolaryngologist (ENT specialist) to reduce unnecessary antibiotic consumption in the pediatric age group.
The aim of this study was to identify the specific characteristics of pediatric patients with AO according to the type of otitis, their age, and the underlying etiology. These data, derived from actual clinical practice, will contribute to the global data on otic involvement in children in the context of acute infectious diseases.
2. Materials and Methods
We conducted a retrospective study of pediatric cases (under 18 years of age) hospitalized at the National Institute of Infectious Diseases “Prof. Dr. Matei Balș” (NIID) who were diagnosed with AO. The NIID, situated in Bucharest, is the largest hospital in Romania dedicated to the management and treatment of patients with infectious diseases. The hospital has six wards and an emergency room for the care of children of all ages.
All consecutive hospitalized cases with a primary or secondary diagnosis of AO from January 2018 to December 2023 were eligible to be included in the analysis. Patient identification was performed using the following ICD-10 diagnosis codes: H60, H62, H65, H66, and H67.
The inclusion criteria for the study were as follows:
- Patient being under 18 years of age;
- An ear condition as determined by an ENT examination;
- Complete medical records;
- Patient records, including ENT evaluations, reviewed by an ENT physician on the study team to confirm inclusion and to classify the type of otic involvement.
Cases without an ENT examination in the medical records or those with incomplete data were excluded from the analysis.
We classified AO cases into acute otitis externa (AOE), acute congestive otitis media (ACOM), acute otitis media with effusion (AOME), and acute purulent otitis media (APOM). Cases showing involvement of the external ear canal with inflammation and edema, without involvement of the tympanic membrane or middle ear, were classified as AOE. Cases were included in the ACOM group if the tympanic membrane was congested, with no accumulation of secretions in the middle ear. Cases were classified as AOME if secretions accumulated in the middle ear without any bulging or tympanic membrane involvement, while cases were classified as APOM if secretions accumulated in the middle ear with bulging or pulsatility of the tympanic membrane, or tympanic perforation and purulent secretions.
For each patient, we collected general data (age, sex), clinical data (signs and symptoms), laboratory data (blood cell count; inflammatory syndrome: fibrinogen, erythrocyte sedimentation rate (ESR), and C-reactive protein (CRP); and culture from ear swab), etiological context (viruses identified by RT-PCR or serology for Epstein–Barr virus, cytomegalovirus, varicella zoster virus, and measles), and length of hospitalization.
Patients were divided into five age groups: infants (0–12 months), toddlers (13–35 months), preschoolers (3–4 years), school children (5–13 years), and adolescents (14–18 years). Any values of laboratory parameters not in the normal range were considered low or high, as appropriate.
Statistical analysis was performed using IBM SPSS version 25 software (IBM Corp., Armonk, NY, USA). After checking the data distribution, continuous variables are reported either as medians, accompanied by the interquartile range (IQR), or as means and standard deviation. The comparison of these variables was performed using the Kruskal–Wallis (H) test. For categorical variables, data are presented as frequencies and percentages, and comparison was performed using the chi-square test. In addition, Cramer’s V (V) coefficient was used to assess effect size. The threshold for statistical significance was set at a level of p < 0.05.
3. Results
3.1. General Characteristics
A total of 1118 children were included in the analysis. Most cases were identified in the pre-pandemic years 2018 and 2019 (69.9%, n = 781, Figure 1). Male patients were more frequent (59.0%, n = 660), while almost half of the cases occurred in young children (49.4%, n = 552, Table 1), with a median age of 2.4 years (IQR: 1.5, 4.0 years).
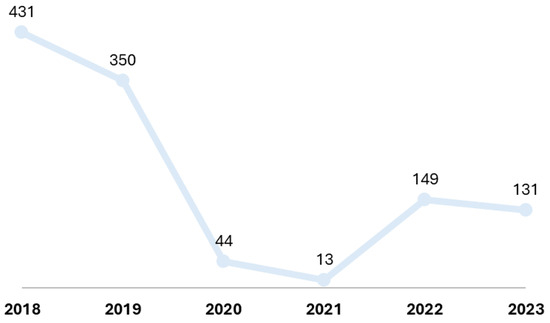
Figure 1.
Distribution of cases by year.

Table 1.
General characteristics of the patients in the study.
3.2. Clinical and Laboratory Aspects in Relation to Age Group
The clinical picture was dominated by fever (88.7%, n = 992), cough (57.5%, n = 643), and nasal congestion (53.0%, n = 592). Among infants, the presence of nasal congestion was significantly associated with otic involvement compared to other age groups (p = 0.001, V = 0.126), while among school children and teenagers, headache (p < 0.001, V = 0.369) and otalgia (p < 0.001, V = 0.255) were significantly more common (Table 2).
Table 2.
Clinical and laboratory characteristics by age group.
Variations in white blood cell counts were observed between age groups (Table 2), and elevated serum CRP levels (74.4%) were more common than increased ESR (66.1%) or increased fibrinogen levels (32.4%).
The median duration from the onset of symptoms until hospital presentation was 4 days (IQR: 2, 6 days), with no significant variation between age groups (p > 0.05 for each).
3.3. Type of Otitis and Clinical and Laboratory Features
ACOM (53.3%, n = 596) was the most common type of otitis identified in patients in the study. Over a quarter of children (27.6%, n = 309) had typical APOM changes, and 18.1% (n = 202) were classified as having AOME. Only 11 (1.0%) children had AOE (Figure 2). The median age was significantly higher among children with AOE (4.5 years (IQR: 1.2, 7.3 years)) compared to the other types of AO (Table 3).
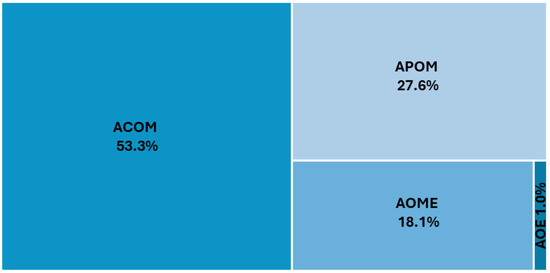
Figure 2.
Distribution of otitis types in the study. AOE—acute otitis externa; ACOM—acute congestive otitis media; AOME—acute otitis media with effusion; APOM—acute purulent otitis media.
Table 3.
Clinical and laboratory characteristics according to the type of acute otitis.
Otalgia was significantly more common in children with APOM (55.3%) and AOE (81.8%, p < 0.001, V = 0.185), while sore throat was reported more often in children with ACOM (29.9%) and AOME (28.7%, p < 0.001, V = 0.194).
APOM was associated with increases in white blood cells (p < 0.001, V = 0.185), neutrophils (p = 0.001, V = 0.120) and inflammatory markers such as fibrinogen (p = 0.002, V = 0.116), ESR (p = 0.019, V = 0.182), and CRP (p = 0.003, V = 0.159).
3.4. Type of Otitis and Clinical and Laboratory Features
In 555 cases (49.6%), a viral infection associated with the episode of AO was documented. Most commonly reported were influenza viruses (20.5%, n = 229), followed by SARS-CoV-2 (5.8%, n = 65) and adenovirus (4.9%, n = 55) (Table 4). A total of 38 cases of AO were identified in children with measles. AOE was only identified in the context of Epstein–Barr virus and varicella zoster virus infection. In 49 cases (15.9%, 49/309) of APOM, Streptococcus pneumoniae was isolated in the culture from otic secretion. In 31 of the 49 cases, tympanocentesis was performed, while in the other 18 cases, Streptococcus pneumoniae was identified from spontaneous otorrhea.
Table 4.
Etiological context according to the type of otitis.
The length of hospitalization was significantly longer in children with AOE (6 days (IQR: 3, 8 days)) and APOM (6 days (IQR: 4, 7 days)) compared to ACOM (5 days (IQR: 4, 6 days)) and AOME (5 days (IQR: 4, 6 days)) (p < 0.001; H = 38.142). The length of hospitalization by age group and type of otitis did not vary significantly from these values for all patients (Table 5, p > 0.05 for each).
Table 5.
Median length of hospital stay (50th percentile) by age group and type of otitis.
4. Discussion
This study identified that the majority of cases of otic involvement in children hospitalized for an acute infectious disease were ACOM (53.3%), followed by APOM (27.6%). These occurred mainly in infants, toddlers, and preschoolers. It is well established that AO is a frequent condition among children up to the age of five [7]. The concentration of a high number of cases in a relatively small population in terms of age range is not a mere coincidence. Rather, a number of anatomical, behavioral, and immunological factors predispose pediatric patients to the development of this condition. First, the anatomical features of the upper respiratory tract of children are directly implicated in the development of AO. The connection between the middle ear, which is an air-filled cavity, and the nasopharynx is via the Eustachian tube (ET), which regulates the drainage of secretions and pressure from the middle ear. The anatomy of the ET differs in infants and young children from that of adults. The shorter, narrower tube with a more horizontal pathway is more prone to inefficient drainage and provides easy access for pathogens, creating an environment that facilitates fluid stagnation and superinfection [8]. Second, the immaturity of children’s immune systems frequently results in their being affected by acute upper respiratory tract infections, which in turn often lead to otic complications [9]. Third, children’s hygiene measures are not always strictly observed, which serves to facilitate the spread of pathogens. Furthermore, breastfeeding in the supine position, the use of pacifiers, and exposure to passive smoking have also been identified as risk factors that can contribute to the development of acute otitis media.
We have shown that the number of cases of AO dropped dramatically during the COVID-19 pandemic, from 431 cases in 2018 and 350 cases in 2019 to 44 cases in 2020 and 13 cases in 2021. This significant reduction in the number of AO cases after the installation of lockdown measures was recently reported by Warner et al. [10] in a meta-analysis on studies from 11 countries. An overall decrease in all ENT pathologies was also reported during the COVID-19 pandemic [11]. It should also be noted that most of our cases in 2020–2021 were in the context of SARS-CoV-2 infection. This finding is not surprising given the decline in the circulation of other respiratory viruses in the first two years of the pandemic [12,13]. Ear pain, ear pressure, hearing loss, and dizziness have been reported in patients with COVID-19 [14]. SARS-CoV-2 has also been isolated in middle-ear fluid, showing direct involvement in the pathogenesis of AO [15]. In addition, during the COVID-19 pandemic, an increase in the incidence of AOE was reported [16]. In our analysis, we did not identify an increase in the number of AOE cases in the pediatric population associated with SARS-CoV-2 infection. The lower number of AO cases in the 2022–2023 period compared to the pre-pandemic period in our study may be artefactual, or due to the implementation of more widespread etiological testing through RT-PCR of pediatric cases hospitalized for influenza-like respiratory illness. Thus, etiology identification can warrant appropriate earlier management with a reduced likelihood of progression towards otic involvement.
The clinical picture dominated by fever (88.7%), cough (57.5%), and nasal congestion (53.0%) shows that most cases of AO occured in the context of viral upper respiratory tract infection. A study by Heikkinen and Chonmaitree [17] found that viral upper respiratory tract infections are involved in more than 70% of cases of childhood AO. Also, a cohort study conducted in Finland [18] showed that fever is a common symptom in children with acute otitis, being present in more than 80% of the cases studied, thus supporting the data obtained in our study. The identification and recognition of the typical symptoms of viral upper respiratory tract infections are crucial for the early diagnosis and effective management of acute otitis in children. It is imperative that all children hospitalized with upper respiratory tract symptoms undergo an evaluation by an ENT specialist. This specialist assessment allows for the early identification of signs of AO, thus facilitating the prompt initiation of appropriate treatment. In the context of hospitalization, the continuous monitoring of pediatric patients by ENT specialists can prevent the negative progression of the condition and ensure a personalized therapeutic approach tailored to the individual needs of each child.
In our study, we identified that, unsurprisingly, increased white blood cell counts, particularly increased neutrophil counts, along with increased ESR and CRP, are more commonly associated with APOM compared to other types of otitis. Evaluation by blood tests is essential in patients in whom a bacterial etiology of the otic involvement is suspected. Changes in white blood cell count may suggest viral or bacterial etiology, and inflammatory markers are useful in quantifying the body’s response to infection, as well as monitoring response to treatment.
In our analysis, 49.6% of cases exhibited a viral etiological context. In the development of acute otitis, influenza viruses were identified as the causative agent with the highest prevalence. The incidence of influenza in the pediatric population is high each season [19,20], and the risk of AO can increase 1.54 times during an influenza episode [21]. Furthermore, influenza vaccination in children has been shown to reduce the number of cases of AO in the pediatric population. Nevertheless, the rates of influenza vaccination, particularly among children, remain low in Romania. Recent data indicate that a relatively low percentage of the pediatric population is vaccinated against influenza each year [22]. To enhance influenza vaccination rates among children, it is imperative to implement efficacious information campaigns that underscore the safety and significance of vaccination. This is becoming increasingly important for Romania now that authorities ensure a better availability of vaccines and facilitate access to them through full reimbursement.
We identified a total of 38 cases of AO in children with measles. In the United States, AO is the most common complication of measles, with an incidence of more than 14% in children under 5 years of age, with lower rates seen with increasing age [23]. In addition, as with other viruses, rubella virus has been isolated from the middle-ear fluid of infants with acute otitis media [24], thereby demonstrating it can also have a direct involvement in the development of acute otitis media. Unfortunately, due to low measles, mumps, and rubella (MMR) vaccination rates in Romania [25], large measles epidemics have been ongoing in our country from 2016 to 2019 [25,26] and again since 2023, resulting in a high number of pediatric hospitalizations, many of which have been complicated by conditions beyond the field of AO.
Among the bacterial pathogens responsible for AO, notable species include Streptococcus pneumoniae, Moraxella catarrhalis, Haemophilus influenzae, Staphylococcus aureus, and Streptococcus pyogenes. Of these, pneumococcus is the predominant causative agent, accounting for more than 50% of cases of acute otitis, regardless of age [27,28]. This highlights the significant role of pneumococcus in the etiology of this condition, making it a critical target for both preventive and therapeutic strategies [29,30]. Non-typable Haemophilus influenzae is next in terms of isolation rate in cultures, being identified in up to 20% of cases occurring in children under six years of age [31]. Moraxella catarrhalis is detected in 10–15% of cases and is notably associated with recurrent infections due to its resistance to beta-lactam antibiotics, which are frequently employed as an empirical treatment for AO [32]. Also, group A streptococci, although not very frequently isolated in otic cultures, are responsible for cases occurring in older children, or those complicated with tympanic perforation or mastoiditis [33]. This spectrum of pathogens underscores the need for accurate diagnosis and targeted antibiotic therapy to effectively manage AO and mitigate complications. In our study, Streptococcus pneumoniae was isolated in 49 of the otic cultures from patients with APOM (31 by tympanocentesis and 18 by spontaneous otorrhea). Data on antimicrobial resistance or pneumococcal vaccination history were not available in this study due to its retrospective nature. The pneumococcal vaccine was widely introduced in the Romanian National Immunization Program for more than seven years, but nevertheless, more efforts are needed to ensure optimal vaccine uptake, and in the meantime invasive pneumococcal disease continues to remain a challenge in the country [34].
The main limitation of our study is the retrospective nature of the data, which made it impossible to fully monitor viral and bacterial etiologies. In addition, a proportion of the patient records had incomplete or brief ENT consultation data, or the type of AO was difficult to determine, so a proportion of cases had to be excluded from the analysis. Also, other data such as vaccine history or antimicrobial resistance of Streptococcus pneumoniae were not available for analysis. Nevertheless, the number of cases is high, and the 6-year duration of the study, including the pre-pandemic period, provides a comprehensive picture of the impact of AO on the pediatric population hospitalized in an infectious diseases hospital.
5. Conclusions
Our study highlights the importance of ENT monitoring in children hospitalized with acute infectious diseases, especially those presenting with fever, cough, and nasal congestion. The majority of AO cases were associated with viral infections, some of which were vaccine-preventable. Children under 5 years of age accounted for the majority of cases, and tympanic congestion was the most common finding. These data underscore the need for prompt evaluation and intervention in suspected cases of AO to prevent complications and reduce unwarranted antibiotic use.
Author Contributions
Conceptualization, V.Ș.P. and O.S.; methodology, A.D.P. and A.S.-C.; software, V.Ș.P.; validation, O.S. and A.S.-C.; formal analysis, A.C.D. and A.D.P.; investigation, V.Ș.P., R.H., A.C.D., O.S., A.S.-C. and A.D.P.; data curation, O.S. and A.C.D.; writing—original draft preparation, V.Ș.P. and A.S.-C.; writing—review and editing, A.D.P., A.S.-C. and O.S.; supervision, O.S. and A.D.P. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki and was approved by the Institutional Review Board, number C12855/27.10.2023. The approval date was 27 October 2023.
Informed Consent Statement
The study was with a waiver for informed consent given the retrospective nature of the data and Ethics committee waived informed consent.
Data Availability Statement
The data are available through reasonable request to the corresponding author. The data are not publicly available due to restrictions.
Acknowledgments
Publication of this paper was supported by the Carol Davila University of Medicine and Pharmacy through the institutional program Publish not Perish.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Monasta, L.; Ronfani, L.; Marchetti, F.; Montico, M.; Brumatti, L.V.; Bavcar, A.; Grasso, D.; Barbiero, C.; Tamburlini, G. Burden of disease caused by otitis media: Systematic review and global estimates. PLoS ONE 2012, 7, e36226. [Google Scholar] [CrossRef]
- Nokso-Koivisto, J.; Marom, T.; Chonmaitree, T. Importance of viruses in acute otitis media. Curr. Opin. Pediatr. 2015, 27, 110–115. [Google Scholar] [CrossRef]
- Ngo, C.C.; Massa, H.M.; McMonagle, B.A.; Perry, C.F.; Nissen, M.D.; Sloots, T.P.; Thornton, R.B.; Cripps, A.W. Predominant Bacterial and Viral Otopathogens Identified Within the Respiratory Tract and Middle Ear of Urban Australian Children Experiencing Otitis Media Are Diversely Distributed. Front. Cell. Infect. Microbiol. 2022, 12, 775535. [Google Scholar] [CrossRef]
- Usonis, V.; Jackowska, T.; Petraitiene, S.; Sapala, A.; Neculau, A.; Stryjewska, I.; Devadiga, R.; Tafalla, M.; Holl, K. Incidence of acute otitis media in children below 6 years of age seen in medical practices in five East European countries. BMC Pediatr. 2016, 16, 108. [Google Scholar] [CrossRef]
- Schilder, A.G.; Chonmaitree, T.; Cripps, A.W.; Rosenfeld, R.M.; Casselbrant, M.L.; Haggard, M.P.; Venekamp, R.P. Otitis media. Nat. Rev. Dis. Primers 2016, 2, 16063. [Google Scholar] [CrossRef]
- Harmes, K.M.; Blackwood, R.A.; Burrows, H.L.; Cooke, J.M.; Harrison, R.V.; Passamani, P.P. Otitis media: Diagnosis and treatment. Am. Fam. Physician 2013, 88, 435–440. [Google Scholar]
- Jamal, A.; Alsabea, A.; Tarakmeh, M.; Safar, A. Etiology, Diagnosis, Complications, and Management of Acute Otitis Media in Children. Cureus 2022, 14, e28019. [Google Scholar] [CrossRef]
- Fireman, P. Otitis media and eustachian tube dysfunction: Connection to allergic rhinitis. J. Allergy Clin. Immunol. 1997, 99, S787–S797. [Google Scholar] [CrossRef]
- Chonmaitree, T.; Revai, K.; Grady, J.J.; Clos, A.; Patel, J.A.; Nair, S.; Fan, J.; Henrickson, K.J. Viral upper respiratory tract infection and otitis media complication in young children. Clin. Infect. Dis. 2008, 46, 815–823. [Google Scholar] [CrossRef]
- Warner, B.K.; Durrant, F.G.; Nguyen, S.A.; Meyer, T.A. Global Otitis Media Incidence Changes During the COVID Pandemic: Systematic Review and Meta-Analysis. Laryngoscope 2024, 134, 2028–2037. [Google Scholar] [CrossRef]
- Gazzini, L.; Fazio, E.; Dallari, V.; Accorona, R.; Abousiam, M.; Nebiaj, A.; Giorgetti, G.; Girolami, I.; Vittadello, F.; Magnato, R.; et al. Impact of the COVID-19 pandemic on head and neck cancer diagnosis: Data from a single referral center, South Tyrol, northern Italy. Eur. Arch. Otorhinolaryngol. 2022, 279, 3159–3166. [Google Scholar] [CrossRef]
- Sandulescu, M.; Sandulescu, O. Changing clinical patterns and ear-nose-throat complications of seasonal viral respiratory tract infections. Germs 2023, 13, 311–313. [Google Scholar] [CrossRef]
- Tarzjani, S.D.; Kamalzadeh, S.; Moghadam, M.T.; Ashoobi, M.T. Clinical challenge of co-infection of SARS-CoV-2 with influenza during the influenza circulation season: Suggestions for prevention. Germs 2023, 13, 188–191. [Google Scholar] [CrossRef]
- Maharaj, S.; Bello Alvarez, M.; Mungul, S.; Hari, K. Otologic dysfunction in patients with COVID-19: A systematic review. Laryngoscope Investig. Otolaryngol. 2020, 5, 1192–1196. [Google Scholar] [CrossRef]
- Fan, Y.; Gao, R.; Shang, Y.; Tian, X.; Zhao, Y.; Chen, X. Presence of SARS-CoV-2 in middle ear fluid and characterization of otitis media with effusion in patients with COVID-19. Int. J. Infect. Dis. 2023, 136, 44–48. [Google Scholar] [CrossRef]
- Mady, O.M.; El-Ozairy, H.S.; Wady, E.M. Increased incidence of otitis externa in COVID-19 patients. Am. J. Otolaryngol. 2021, 42, 102672. [Google Scholar] [CrossRef]
- Heikkinen, T.; Chonmaitree, T. Importance of respiratory viruses in acute otitis media. Clin. Microbiol. Rev. 2003, 16, 230–241. [Google Scholar]
- Ruohola, A.; Meurman, O.; Nikkari, S.; Skottman, T.; Salmi, A.; Waris, M.; Österback, R.; Eerola, E.; Allander, T.; Niesters, H.; et al. Microbiology of acute otitis media in children with tympanostomy tubes: Prevalences of bacteria and viruses. Clin. Infect. Dis. 2006, 43, 1417–1422. [Google Scholar] [CrossRef]
- Drăgănescu, A.C.; Miron, V.D.; Streinu-Cercel, A.; Florea, D.; Vlaicu, O.; Bilaşco, A.; Oţelea, D.; Luminos, M.L.; Piţigoi, D.; Streinu-Cercel, A.; et al. Circulation of influenza A viruses among patients hospitalized for severe acute respiratory infection in a tertiary care hospital in Romania in the 2018/19 season: Results from an observational descriptive epidemiological study. Medicine 2021, 100, e28460. [Google Scholar] [CrossRef]
- Miron, V.D.; Bănică, L.; Săndulescu, O.; Paraschiv, S.; Surleac, M.; Florea, D.; Vlaicu, O.; Milu, P.; Streinu-Cercel, A.; Bilașco, A.; et al. Clinical and molecular epidemiology of influenza viruses from Romanian patients hospitalized during the 2019/20 season. PLoS ONE 2021, 16, e0258798. [Google Scholar] [CrossRef] [PubMed]
- Hoy, G.; Kuan, G.; López, R.; Sánchez, N.; López, B.; Ojeda, S.; Maier, H.; Patel, M.; Wraith, S.; Meyers, A.; et al. The Spectrum of Influenza in Children. Clin. Infect. Dis. 2023, 76, e1012–e1020. [Google Scholar] [CrossRef]
- Miron, V.D.; Toma, A.R.; Filimon, C.; Bar, G.; Craiu, M. Optional Vaccines in Children-Knowledge, Attitudes, and Practices in Romanian Parents. Vaccines 2022, 10, 404. [Google Scholar] [CrossRef]
- Perry, R.T.; Halsey, N.A. The clinical significance of measles: A review. J. Infect. Dis. 2004, 189 (Suppl. S1), S4–S16. [Google Scholar]
- Yano, H.; Suetake, M.; Endo, H.; Takayanagi, R.; Numata, M.; Ohyama, K.; Sagai, S.; Okitsu, N.; Okamoto, M.; Nishimura, H.; et al. Isolation of measles virus from middle ear fluid of infants with acute otitis media. J. Infect. 2005, 51, e237–e240. [Google Scholar] [CrossRef]
- Centrul Național de Supraveghere și Control al Bolilor Transmisibile, Analiza Evoluției Bolilor Transmisibile Aflate în Supraveghere-Raport Pentru Anul 2022. Available online: https://insp.gov.ro/centrul-national-de-supraveghere-si-control-al-bolilor-transmisibile-cnscbt/rapoarte-anuale/ (accessed on 14 June 2024).
- Pițigoi, D.; Săndulescu, O.; Crăciun, M.D.; Drăgănescu, A.; Jugulete, G.; Streinu-Cercel, A.; Vișan, A.; Rîciu, C.; Rafila, A.; Aramă, V.; et al. Measles in Romania-clinical and epidemiological characteristics of hospitalized measles cases during the first three years of the 2016-ongoing epidemic. Virulence 2020, 11, 686–694. [Google Scholar] [CrossRef]
- Arrieta, A.; Singh, J. Management of recurrent and persistent acute otitis media: New options with familiar antibiotics. Pediatr. Infect. Dis. J. 2004, 23 (Suppl. 2), S115–S124. [Google Scholar] [CrossRef]
- Paudel, G.; Amatya, N.; Saud, B.; Wagle, S.; Shrestha, V.; Adhikari, B. Nasal colonization by potential bacterial pathogens in healthy kindergarten children of Nepal: A prevalence study. Germs 2022, 12, 86–98. [Google Scholar] [CrossRef]
- Scelfo, C.; Menzella, F.; Fontana, M.; Ghidoni, G.; Galeone, C.; Facciolongo, N.C. Pneumonia and Invasive Pneumococcal Diseases: The Role of Pneumococcal Conjugate Vaccine in the Era of Multi-Drug Resistance. Vaccines 2021, 9, 420. [Google Scholar] [CrossRef]
- Oligbu, G.; Fry, N.K.; Ladhani, S.N. The Pneumococcus and Its Critical Role in Public Health. Methods Mol. Biol. 2019, 1968, 205–213. [Google Scholar] [PubMed]
- Rosenblut, A.; Napolitano, C.; Pereira, A.; Moreno, C.; Kolhe, D.; Lepetic, A.; Ortega-Barria, E. Etiology of acute otitis media and serotype distribution of Streptococcus pneumoniae and Haemophilus influenzae in Chilean children <5 years of age. Medicine 2017, 96, e5974. [Google Scholar] [PubMed]
- Broides, A.; Dagan, R.; Greenberg, D.; Givon-Lavi, N.; Leibovitz, E. Acute otitis media caused by Moraxella catarrhalis: Epidemiologic and clinical characteristics. Clin. Infect. Dis. 2009, 49, 1641–1647. [Google Scholar] [CrossRef] [PubMed]
- Ramakrishnan, K.; Sparks, R.A.; Berryhill, W.E. Diagnosis and treatment of otitis media. Am. Fam. Physician 2007, 76, 1650–1658. [Google Scholar] [PubMed]
- Ceyhan, M.; Dagan, R.; Sayiner, A.; Chernyshova, L.; Dinleyici, E.Ç.; Hryniewicz, W.; Kulcsár, A.; Mad’arová, L.; Pazdiora, P.; Sidorenko, S.; et al. Surveillance of pneumococcal diseases in Central and Eastern Europe. Hum. Vaccin. Immunother. 2016, 12, 2124–2134. [Google Scholar] [CrossRef] [PubMed]
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).