Acceptability and Feasibility of Single-Component Primary School Physical Activity Interventions to Inform the AS:Sk Project

 ,
, 

Abstract
1. Introduction
2. Materials and Methods
2.1. Participants and Recruitment
2.2. Intervention Components
2.2.1. Active Breaks Intervention
2.2.2. Born to Move Videos Intervention
2.2.3. Playground Intervention
2.3. Measures
2.3.1. Qualitative Data
2.3.2. Quantitative Data
2.4. Data Analysis
2.4.1. Qualitative Data
2.4.2. Quantitative Data
3. Results
3.1. Qualitative Data
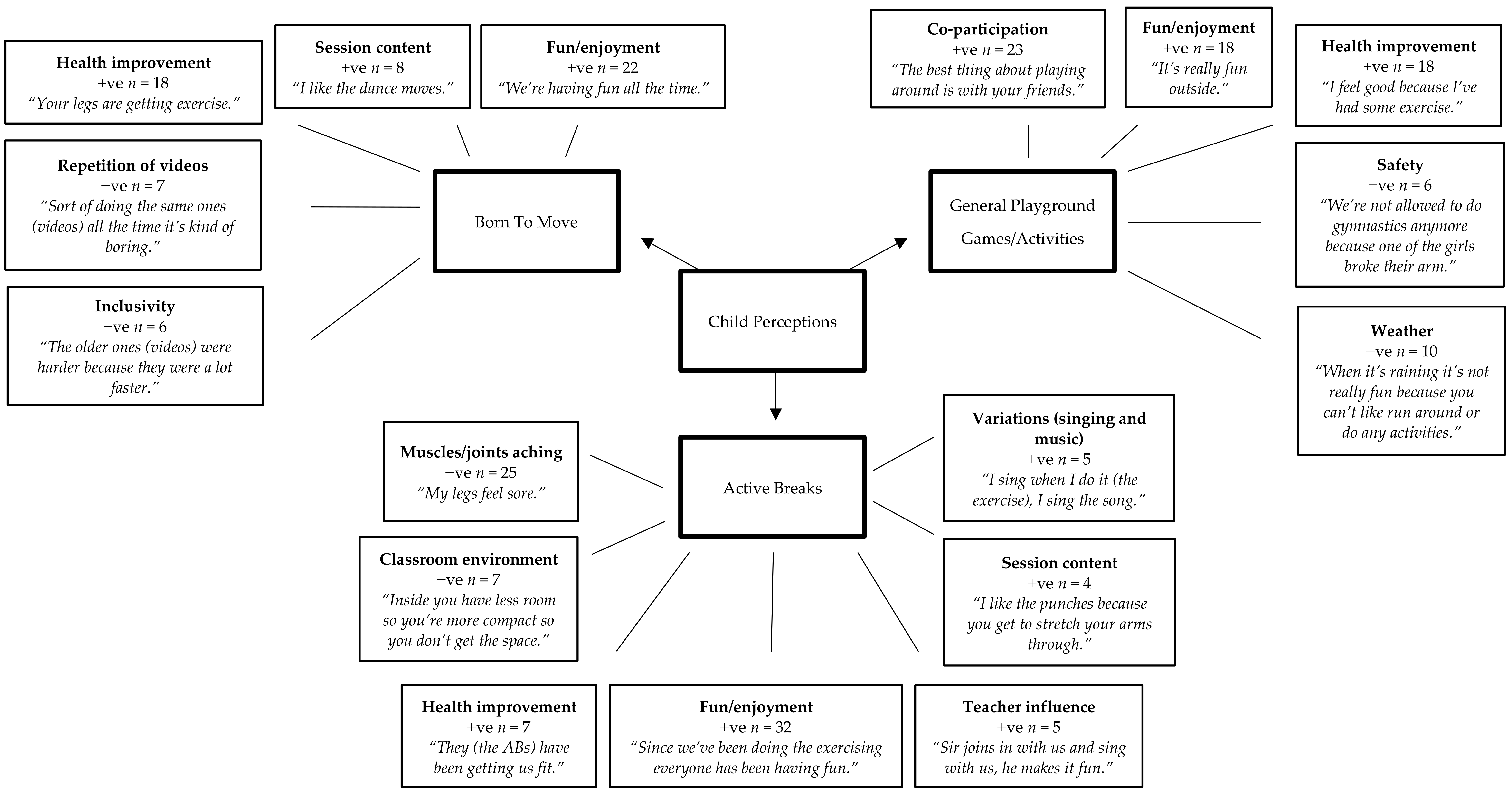
3.1.1. Child Perceptions
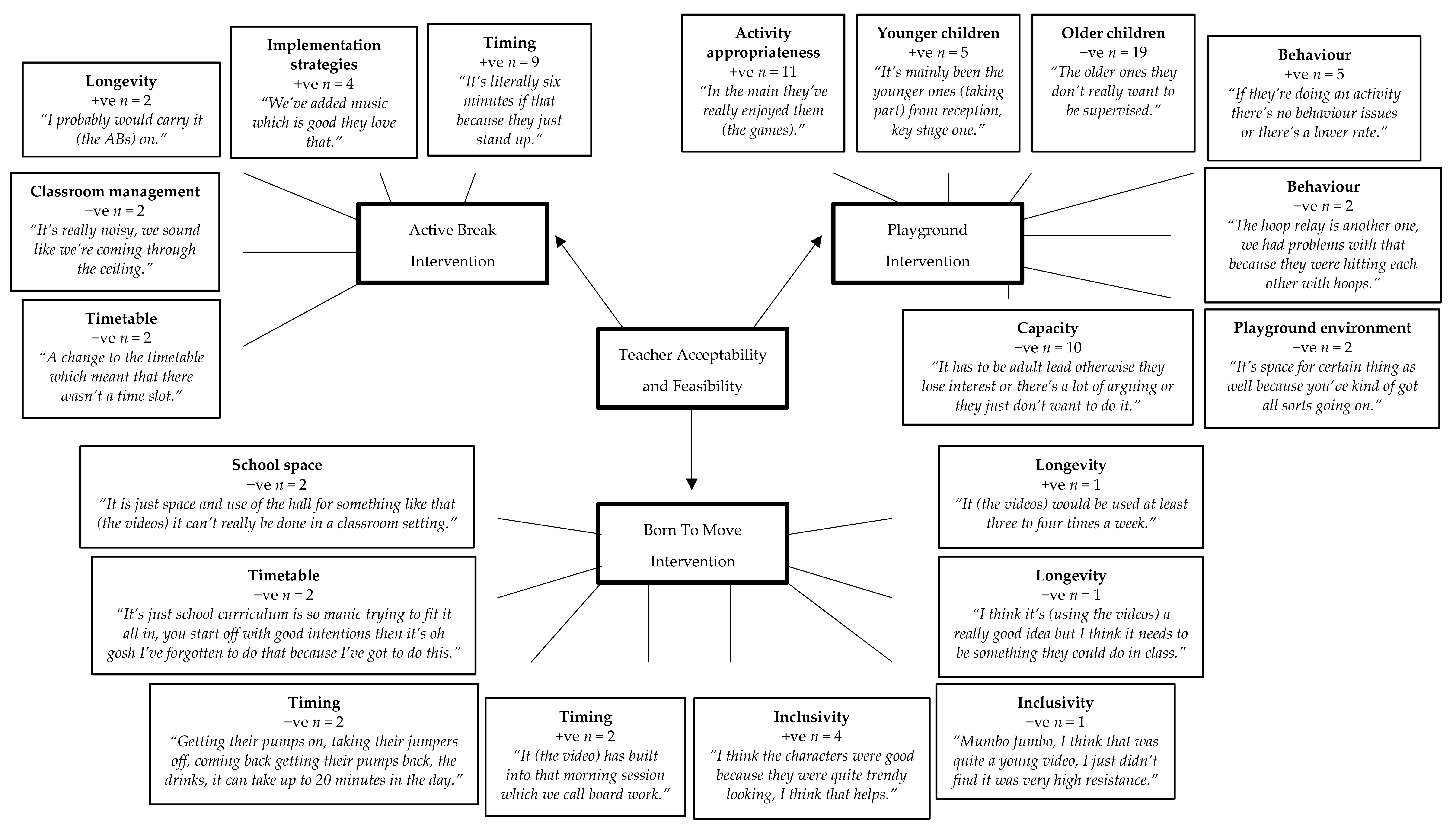
3.1.2. Teacher Perceptions
3.1.3. Teacher Reported Implementation
3.2. Quantitative Data
3.2.1. Active Break Intervention
3.2.2. Born to Move Intervention
3.2.3. Playground Intervention
4. Discussion
4.1. Acceptability and Feasibility
4.2. Moderate to Vigorous Physical Activity and Sedentary Time
4.3. Strengths and Limitations
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Andersen, L.B.; Riddoch, C.; Kriemler, S.; Hills, A.P. Physical activity and cardiovascular risk factors in children. Br. J. Sports Med. 2011, 45, 871–876. [Google Scholar] [CrossRef] [PubMed]
- Reddon, H.; Meyre, D.; Cairney, J. Physical Activity and Global Self-worth in a Longitudinal Study of Children. Med. Sci. Sports Exerc. 2017, 49, 1606–1613. [Google Scholar] [CrossRef] [PubMed]
- Lubans, D.; Richards, J.; Hillman, C.; Faulkner, G.; Beauchamp, M.; Nilsson, M.; Kelly, P.; Smith, J.; Raine, L.; Biddle, S. Physical Activity for Cognitive and Mental Health in Youth: A Systematic Review of Mechanisms. Pediatrics 2016, 138, e20161642. [Google Scholar] [CrossRef] [PubMed]
- Chief Medical Officer Department of Health. Start Active, Stay Active: A Report on Physical Activity from the four Home Countries’; Department of Health: London, UK, 2011. [Google Scholar]
- Cooper, A.R.; Goodman, A.; Page, A.S.; Sherar, L.B.; Esliger, D.W.; van Sluijs, E.M.; Andersen, L.B.; Anderssen, S.; Cardon, G.; Davey, R.; et al. Objectively measured physical activity and sedentary time in youth: The International children’s accelerometry database (ICAD). Int. J. Behav. Nutr. Phys. Act. 2015, 12, 113. [Google Scholar] [CrossRef] [PubMed]
- Carson, V.; Hunter, S.; Kuzik, N.; Gray, C.E.; Poitras, V.J.; Chaput, J.P.; Saunders, T.J.; Katzmarzyk, P.T.; Okely, A.D.; Connor Gorber, S. Systematic review of sedentary behaviour and health indicators in school-aged children and youth: An update. Appl. Physiol. Nutr. Metab. 2016, 41, S240–S265. [Google Scholar] [CrossRef] [PubMed]
- Pearson, N.; Haycraft, E.; Johnston, J.P.; Atkin, A.J. Sedentary behaviour across the primary-secondary school transition: A systematic review. Prev. Med. 2017, 94, 40–47. [Google Scholar] [CrossRef] [PubMed]
- Burns, R.D.; Fu, Y.; Podlog, L.W. School-based physical activity interventions and physical activity enjoyment: A meta-analysis. Prev. Med. 2017, 103, 84–90. [Google Scholar] [CrossRef] [PubMed]
- Kohl, H.W., III; Cook, H.D. (Eds.) Educating the Student Body: Taking Physical Activity and Physical Education to School; The National Academies Press: Washington, DC, USA, 2013; ISBN 978-0-309-28313-7. [Google Scholar]
- Van Stralen, M.M.; Yıldırım, M.; Wulp, A.; te Velde, S.J.; Verloigne, M.; Doessegger, A.; Androutsos, O.; Kovács, É.; Brug, J.; Chinapaw, M.J.M. Measured sedentary time and physical activity during the school day of European 10- to 12-year-old children: The ENERGY project. J. Sci. Med. Sport 2014, 17, 201–206. [Google Scholar] [CrossRef] [PubMed]
- Fox, K.R.; Cooper, A.; McKenna, J. The School and Promotion of Children’s Health-Enhancing Physical Activity: Perspectives from the United Kingdom. J. Teach. Phys. Educ. 2004, 23, 338–358. [Google Scholar] [CrossRef]
- Erwin, H.; Beighle, A.; Carson, R.L.; Castelli, D.M. Comprehensive School-Based Physical Activity Promotion: A Review. Quest 2013, 65, 412–428. [Google Scholar] [CrossRef]
- Russ, L.B.; Webster, C.A.; Beets, M.W.; Phillips, D.S. Systematic Review and Meta-Analysis of Multi-Component Interventions Through Schools to Increase Physical Activity. J. Phys. Act. Health 2015, 12, 1436–1446. [Google Scholar] [CrossRef] [PubMed]
- Naylor, P.J.; Macdonald, H.M.; Reed, K.E.; McKay, H.A. Action Schools! BC: A Socioecological Approach to Modifying Chronic Disease Risk Factors in Elementary School Children. Prev. Chronic Dis. 2006, 3, A60. [Google Scholar]
- Naylor, P.J.; Macdonald, H.M.; Warburton, D.E.R.; Reed, K.E.; McKay, H.A. An active school model to promote physical activity in elementary schools: Action schools! BC. Br. J. Sports Med. 2008, 42, 338. [Google Scholar] [CrossRef] [PubMed]
- Naylor, P.J.; Macdonald, H.M.; Zebedee, J.A.; Reed, K.E.; McKay, H.A. Lessons learned from Action Schools! BC—An ‘active school’ model to promote physical activity in elementary schools. J. Sci. Med. Sport 2006, 9, 413–423. [Google Scholar] [CrossRef] [PubMed]
- Okely, A.D.; Lubans, D.R.; Morgan, P.J.; Cotton, W.; Peralta, L.; Miller, J.; Batterham, M.; Janssen, X. Promoting physical activity among adolescent girls: The Girls in Sport group randomized trial. Int. J. Behav. Nutr. Phys. Act. 2017, 14, 81. [Google Scholar] [CrossRef] [PubMed]
- Beets, M.W.; Okely, A.; Weaver, R.G.; Webster, C.; Lubans, D.; Brusseau, T.; Carson, R.; Cliff, D.P. The theory of expanded, extended, and enhanced opportunities for youth physical activity promotion. Int. J. Behav. Nut. Phys. Act. 2016, 13, 120. [Google Scholar] [CrossRef] [PubMed]
- Craig, P.; Dieppe, P.; Macintyre, S.; Michie, S.; Nazareth, I.; Petticrew, M. Developing and evaluating complex interventions: The new Medical Research Council guidance. BMJ 2008, 337, a1655. [Google Scholar] [CrossRef] [PubMed]
- Weatherson, K.A.; McKay, R.; Gainforth, H.L.; Jung, M.E. Barriers and facilitators to the implementation of a school-based physical activity policy in Canada: Application of the theoretical domains framework. BMC Public Health 2017, 17, 835. [Google Scholar] [CrossRef] [PubMed]
- Van den Berg, V.; Salimi, R.; de Groot, R.H.M.; Jolles, J.; Chinapaw, M.J.M.; Singh, A.S. “It’s a Battle… You Want to Do It, but How Will You Get It Done?”: Teachers’ and Principals’ Perceptions of Implementing Additional Physical activity in School for Academic Performance. Int. J. Environ. Res. Public Health 2017, 14, 1160. [Google Scholar] [CrossRef] [PubMed]
- Moore, G.F.; Audrey, S.; Barker, M.; Bond, L.; Bonell, C.; Hardeman, W. Process evaluation of complex interventions: Medical Research Council guidance. BMJ 2015, 350, h1258. [Google Scholar] [CrossRef] [PubMed]
- Laine, H.; Araujo-Soares, V.; Haukkala, A.; Hankonen, N. Acceptability of Strategies to Reduce Student Sitting: A Mixed-Methods Study with College Teachers. Health Promot. Pract. 2017, 18, 44–53. [Google Scholar] [CrossRef] [PubMed]
- Naylor, P.J.; Nettlefold, L.; Race, D.; Hoy, C.; Ashe, M.C.; Wharf Higgins, J.; McKay, H.A. Implementation of school based physical activity interventions: A systematic review. Prev. Med. 2015, 72, 95–115. [Google Scholar] [CrossRef] [PubMed]
- Burns, R.D.; Brusseau, T.A.; Fu, Y. Moderators of School-Based Physical Activity Interventions on Cardiorespiratory Endurance in Primary School-Aged Children: A Meta-Regression. Int. J. Environ. Res. Public Health 2018, 15, 1764. [Google Scholar] [CrossRef] [PubMed]
- Taylor, S.L.; Curry, W.B.; Knowles, Z.R.; Noonan, R.J.; McGrane, B.; Fairclough, S.J. Predictors of Segmented School Day Physical Activity and Sedentary Time in Children from a Northwest England Low-Income Community. Int. J. Environ. Res. Public Health 2017, 14, 534. [Google Scholar] [CrossRef] [PubMed]
- Taylor, S.L.; Noonan, R.J.; Knowles, Z.R.; Owen, M.B.; McGrane, B.; Curry, W.B.; Fairclough, S.J. Evaluation of a Pilot School-Based Physical Activity Clustered Randomised Controlled Trial-Active Schools: Skelmersdale. Int. J. Environ. Res. Public Health 2018, 15, 1011. [Google Scholar] [CrossRef] [PubMed]
- Collins, S. Seven Wards: A Focus on Skelmersdale; Lancashire County Council: Preston, UK, 2015. [Google Scholar]
- Eldridge, S.M.; Lancaster, G.A.; Campbell, M.J.; Thabane, L.; Hopewell, S.; Coleman, C.L.; Bond, C.M. Defining Feasibility and Pilot Studies in Preparation for Randomised Controlled Trials: Development of a Conceptual Framework. PLoS ONE 2016, 11, e0150205. [Google Scholar] [CrossRef] [PubMed]
- Watson, A.; Timperio, A.; Brown, H.; Hesketh, K.D. A primary school active break programme (ACTI-BREAK): Study protocol for a pilot cluster randomised controlled trial. Trials 2017, 18, 433. [Google Scholar] [CrossRef] [PubMed]
- Watson, A.J.L.; Timperio, A.; Brown, H.; Hesketh, K.D. A pilot primary school active break program (ACTI-BREAK): Effects on academic and physical activity outcomes for students in Years 3 and 4. J. Sci. Med. Sport 2018. [Google Scholar] [CrossRef] [PubMed]
- Watson, A.; Timperio, A.; Brown, H.; Best, K.; Hesketh, K.D. Effect of classroom-based physical activity interventions on academic and physical activity outcomes: A systematic review and meta-analysis. Int. J. Behav. Nutr. Phys. Act. 2017, 14, 114. [Google Scholar] [CrossRef] [PubMed]
- Fairclough, S.J.; McGrane, B.; Sanders, G.; Taylor, S.; Owen, M.; Curry, W. A non-equivalent group pilot trial of a school-based physical activity and fitness intervention for 10-11 year old english children: Born to move. BMC Public Health 2016, 16, 861. [Google Scholar] [CrossRef] [PubMed]
- Till, J.; Ferkins, L.; Handcock, P. Physical activity based professional development for teachers: The importance of whole school involvement. Health Educ. J. 2011, 70, 225–235. [Google Scholar] [CrossRef]
- Coe, R.; Waring, M.; Hedges, L.V.; Arthur, J. Research Methods and Methodologies in Education, 2nd ed.; SAGE Publications: London, UK, 2017; ISBN 9781473969803. [Google Scholar]
- Nyumba, T.O.; Wilson, K.; Derrick, C.J.; Mukherjee, N. The use of focus group discussion methodology: Insights from two decades of application in conservation. Methods Ecol. Evol. 2018, 9, 20–32. [Google Scholar] [CrossRef]
- Fairclough, S.J.; Noonan, R.; Rowlands, A.V.; Van Hees, V.; Knowles, Z.; Boddy, L.M. Wear Compliance and Activity in Children Wearing Wrist- and Hip-Mounted Accelerometers. Med. Sci. Sports Exerc. 2016, 48, 245–253. [Google Scholar] [CrossRef] [PubMed]
- Rowlands, A.V.; Mirkes, E.M.; Yates, T.; Clemes, S.; Davies, M.; Khunti, K.; Edwardson, C.L. Accelerometer-assessed Physical Activity in Epidemiology: Are Monitors Equivalent? Med. Sci. Sports Exerc. 2018, 50, 257–265. [Google Scholar] [CrossRef] [PubMed]
- Van Hees, V.T.; Gorzelniak, L.; Dean Leon, E.C.; Eder, M.; Pias, M.; Taherian, S.; Ekelund, U.; Renstrom, F.; Franks, P.W.; Horsch, A.; et al. Separating movement and gravity components in an acceleration signal and implications for the assessment of human daily physical activity. PLoS ONE 2013, 8, e61691. [Google Scholar] [CrossRef] [PubMed]
- Van Hees, V.T.; Fang, Z.; Langford, J.; Assah, F.; Mohammad, A.; da Silva, I.C.M.; Trenell, M.I.; White, T.; Wareham, N.J.; Brage, S. Autocalibration of accelerometer data for free-living physical activity assessment using local gravity and temperature: An evaluation on four continents. J. Appl. Physiol. 2014, 117, 738–744. [Google Scholar] [CrossRef] [PubMed]
- Nettlefold, L.; McKay, H.A.; Warburton, D.E.R.; McGuire, K.A.; Bredin, S.S.D.; Naylor, P.J. The challenge of low physical activity during the school day: At recess, lunch and in physical education. Br. J. Sports Med. 2011, 45, 813. [Google Scholar] [CrossRef] [PubMed]
- Mooses, K.; Pihu, M.; Riso, E.M.; Hannus, A.; Kaasik, P.; Kull, M. Physical Education Increases Daily Moderate to Vigorous Physical Activity and Reduces Sedentary Time. J. Sch. Health 2017, 87, 602–607. [Google Scholar] [CrossRef] [PubMed]
- Hildebrand, M.; Van Hees, V.T.; Hansen, B.H.; Ekelund, U.L.F. Age Group Comparability of Raw Accelerometer Output from Wrist- and Hip-Worn Monitors. Med. Sci. Sports Exerc. 2014, 46, 1816–1824. [Google Scholar] [CrossRef] [PubMed]
- Hildebrand, M.; Hansen, B.H.; van Hees, V.T.; Ekelund, U. Evaluation of raw acceleration sedentary thresholds in children and adults. Scand. J. Med. Sci. Sports 2017, 27, 1814–1823. [Google Scholar] [CrossRef] [PubMed]
- Braun, V.; Clarke, V. Using thematic analysis in psychology. Qual. Res. Psychol. 2006, 3, 77–101. [Google Scholar] [CrossRef]
- Mackintosh, K.A.; Knowles, Z.R.; Ridgers, N.D.; Fairclough, S.J. Using formative research to develop CHANGE!: A curriculum-based physical activity promoting intervention. BMC Public Health 2011, 11, 831. [Google Scholar] [CrossRef] [PubMed]
- Knowles, Z.R.; Parnell, D.; Stratton, G.; Ridgers, N.D. Learning from the experts: Exploring playground experience and activities using a write and draw technique. J. Phys. Act. Health 2013, 10, 406–415. [Google Scholar] [CrossRef] [PubMed]
- Noonan, R.J.; Boddy, L.M.; Fairclough, S.J.; Knowles, Z.R. Write, draw, show, and tell: A child-centred dual methodology to explore perceptions of out-of-school physical activity. BMC Public Health 2016, 16, 326. [Google Scholar] [CrossRef] [PubMed]
- Berliner, D.C. Comment: Educational Research: The Hardest Science of All. Educ. Res. 2002, 31, 18–20. [Google Scholar] [CrossRef]
- Ridgers, N.D.; Salmon, J.; Parrish, A.-M.; Stanley, R.M.; Okely, A.D. Physical Activity During School Recess: A Systematic Review. Am. J. Prev. Med. 2012, 43, 320–328. [Google Scholar] [CrossRef] [PubMed]
- Parrish, A.M.; Yeatman, H.; Iverson, D.; Russell, K. Using interviews and peer pairs to better understand how school environments affect young children’s playground physical activity levels: A qualitative study. Health Educ. Res. 2012, 27, 269–280. [Google Scholar] [CrossRef] [PubMed]
- Gebremariam, M.K.; Bergh, I.H.; Andersen, L.F.; Ommundsen, Y.; Bjelland, M.; Lien, N. Stability and change in potential correlates of physical activity and association with pubertal status among Norwegian children in the transition between childhood and adolescence. Int. J. Behav. Nutr. Phys. Act. 2012, 9, 56. [Google Scholar] [CrossRef] [PubMed]
- Best, K.; Ball, K.; Zarnowiecki, D.; Stanley, R.; Dollman, J. In Search of Consistent Predictors of Children’s Physical Activity. Int. J. Environ. Res. Public Health 2017, 14, 1258. [Google Scholar] [CrossRef] [PubMed]
- Teixeira, P.J.; Carraça, E.V.; Markland, D.; Silva, M.N.; Ryan, R.M. Exercise, physical activity, and self-determination theory: A systematic review. Int. J. Behav. Nutr. Phys. Act. 2012, 9, 78. [Google Scholar] [CrossRef] [PubMed]
- Martin, R.; Murtagh, E.M. Teachers’ and students’ perspectives of participating in the ‘Active Classrooms’ movement integration programme. Teach. Teach. Educ. 2017, 63, 218–230. [Google Scholar] [CrossRef]
- Welk, G.J. The Youth Physical Activity Promotion Model: A Conceptual Bridge Between Theory and Practice. Quest 1999, 51, 5–23. [Google Scholar] [CrossRef]
- McMullen, J.; Kulinna, P.; Cothran, D. Physical Activity Opportunities During the School Day: Classroom Teachers’ Perceptions of Using Activity Breaks in the Classroom. J. Teach. Phys. Educ. 2014, 33, 511–527. [Google Scholar] [CrossRef]
- Webster, C.A.; Zarrett, N.; Cook, B.S.; Egan, C.; Nesbitt, D.; Weaver, R.G. Movement integration in elementary classrooms: Teacher perceptions and implications for program planning. Eval. Program Plan. 2017, 61, 134–143. [Google Scholar] [CrossRef] [PubMed]
- Carlson, J.A.; Engelberg, J.K.; Cain, K.L.; Conway, T.L.; Mignano, A.M.; Bonilla, E.A.; Geremia, C.; Sallis, J.F. Implementing classroom physical activity breaks: Associations with student physical activity and classroom behavior. Prev. Med. 2015, 81, 67–72. [Google Scholar] [CrossRef] [PubMed]
- Ridgers, N.D.; Fairclough, S.J.; Stratton, G. Variables associated with children’s physical activity levels during recess: The A-CLASS project. Int. J. Behav. Nutr. Phys. Act. 2010, 7, 74. [Google Scholar] [CrossRef] [PubMed]
- Dumuid, D.; Stanford, T.E.; Pedišić, Ž.; Maher, C.; Lewis, L.K.; Martín-Fernández, J.-A.; Katzmarzyk, P.T.; Chaput, J.-P.; Fogelholm, M.; Standage, M.; et al. Adiposity and the isotemporal substitution of physical activity, sedentary time and sleep among school-aged children: A compositional data analysis approach. BMC Public Health 2018, 18, 311. [Google Scholar] [CrossRef] [PubMed]
- Fairclough, S.J.; Dumuid, D.; Taylor, S.; Curry, W.; McGrane, B.; Stratton, G.; Maher, C.; Olds, T. Fitness, fatness and the reallocation of time between children’s daily movement behaviours: An analysis of compositional data. Int. J. Behav. Nutr. Phys. Act. 2017, 14, 64. [Google Scholar] [CrossRef] [PubMed]
- Fairclough, S.J.; Dumuid, D.; Mackintosh, K.A.; Stone, G.; Dagger, R.; Stratton, G.; Davies, I.; Boddy, L.M. Adiposity, fitness, health-related quality of life and the reallocation of time between children’s school day activity behaviours: A compositional data analysis. Prev. Med. Rep. 2018, 11, 254–261. [Google Scholar] [CrossRef] [PubMed]
- Erwin, H.E.; Ickes, M.; Ahn, S.; Fedewa, A. Impact of Recess Interventions on Children’s Physical Activity—A Meta-Analysis. Am. J. Health Promot. 2014, 28, 159–167. [Google Scholar] [CrossRef] [PubMed]
- Chin, J.J.; Ludwig, D. Increasing children’s physical activity during school recess periods. Am. J. Public Health 2013, 103, 1229–1234. [Google Scholar] [CrossRef] [PubMed]
- Howe, C.A.; Freedson, P.S.; Alhassan, S.; Feldman, H.A.; Osganian, S.K. A recess intervention to promote moderate-to-vigorous physical activity. Pediatr. Obes. 2012, 7, 82–88. [Google Scholar] [CrossRef] [PubMed]
- Haapala, H.L.; Hirvensalo, M.H.; Kulmala, J.; Hakonen, H.; Kankaanpää, A.; Laine, K.; Laakso, L.; Tammelin, T.H. Changes in physical activity and sedentary time in the Finnish Schools on the Move program: A quasi-experimental study. Scand. J. Med. Sci. Sports 2017, 27, 1442–1453. [Google Scholar] [CrossRef] [PubMed]
- Thomas, J.R.; Silverman, S.; Nelson, J. Research Methods in Physical Activity, 7th ed.; Human Kinetics: Champaign, IL, USA, 2015; ISBN 9781450470445. [Google Scholar]



{kind=link}
{kind=link}
| AB Intervention (n = 101) | BTM Intervention (n = 43) | Playground Intervention (n = 51) | AB vs. BTM | AB vs. PI | BTM vs. PI | |
|---|---|---|---|---|---|---|
| ST (minutes) | 259.9 (30.6) | 237.0 (33.4) | 232.9 (25.7) | p < 0.001 d = 0.7 | p < 0.001 d = 1.0 | p = 0.8 d = 0.1 |
| MVPA (minutes) | 32.3 (13.0) | 45.7 (15.6) | 37.0 (14.2) | p < 0.001 d = −0.9 | p = 0.8 d = −0.3 | p = 0.007 d = 0.6 |
| AB | Usual Practice Pre/Post AB | p | d | BTM | Usual Practice Pre/Post BTM | p | d | |
|---|---|---|---|---|---|---|---|---|
| ST (minutes) | 20.3 (5.4) | 25.3 (4.4) | 0.009 | −1.0 | 12.5 (5.2) | 21.3 (4.7) | 0.003 | −1.8 |
| MVPA (minutes) | 4.8 (2.5) | 0.9 (1.1) | <0.001 | 2.2 | 8.6 (4.0) | 1.8 (2.6) | 0.002 | 2.1 |
| Playground Intervention Schools (n = 2) | Other Schools (n = 5) | p | d | |
|---|---|---|---|---|
| Playground %ST | 35.4 (9.1) | 43.8 (16.2) | <0.001 | −0.7 |
| Playground %MVPA | 17.2 (7.5) | 14.6 (9.5) | 0.08 | 0.3 |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Taylor, S.L.; Noonan, R.J.; Knowles, Z.R.; McGrane, B.; Curry, W.B.; Fairclough, S.J. Acceptability and Feasibility of Single-Component Primary School Physical Activity Interventions to Inform the AS:Sk Project. Children 2018, 5, 171. https://doi.org/10.3390/children5120171
Taylor SL, Noonan RJ, Knowles ZR, McGrane B, Curry WB, Fairclough SJ. Acceptability and Feasibility of Single-Component Primary School Physical Activity Interventions to Inform the AS:Sk Project. Children. 2018; 5(12):171. https://doi.org/10.3390/children5120171
Chicago/Turabian StyleTaylor, Sarah L., Robert J. Noonan, Zoe R. Knowles, Bronagh McGrane, Whitney B. Curry, and Stuart J. Fairclough. 2018. "Acceptability and Feasibility of Single-Component Primary School Physical Activity Interventions to Inform the AS:Sk Project" Children 5, no. 12: 171. https://doi.org/10.3390/children5120171
APA StyleTaylor, S. L., Noonan, R. J., Knowles, Z. R., McGrane, B., Curry, W. B., & Fairclough, S. J. (2018). Acceptability and Feasibility of Single-Component Primary School Physical Activity Interventions to Inform the AS:Sk Project. Children, 5(12), 171. https://doi.org/10.3390/children5120171