
Predictive Value of Red Blood Cell Distribution Width, Mean Platelet Volume and Platelet Distribution Width in Children with Acute Appendicitis

Abstract
:
1. Introduction
2. Materials and Methods
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Almaramhy, H.H. Acute appendicitis in young children less than 5 years: Review article. Acute appendicitis in young children less than 5 years: Review article. Ital. J. Pediatr. 2017, 43, 15. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Galai, T.; Beloosesky, O.Z.; Scolnik, D.; Rimon, A.; Glatstein, M. Misdiagnosis of acute appendicitis in children attending the Emergency Department: The experience of a large, tertiary care pediatric hospital. Eur. J. Pediatr. Surg. 2017, 27, 138–141. [Google Scholar] [CrossRef] [PubMed]
- Maloney, C.; Edelman, M.C.; Bolognese, A.C.; Lipskar, A.M.; Rich, B.S. The Impact of Pathological Criteria on Pediatric Negative Appendectomy Rate. J. Pediatr. Surg. 2019, 54, 1794–1799. [Google Scholar] [CrossRef]
- Maita, S.; Andersson, B.; Svensson, J.F.; Wester, T. Nonoperative treatment for nonperforated appendicitis in children: A systematic review and meta-analysis. Pediatr. Surg. Int. 2020, 36, 261–269. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dinc, B.; Oskay, A.; Dinc, S.E.; Bas, B.; Tekin, S. New parameter in diagnosis of acute appendicitis: Platelet distribution width. World J. Gastroenterol. 2015, 21, 1821–1826. [Google Scholar] [CrossRef] [PubMed]
- Rastgoo Haghi, A.; Pourmohammad, P.; Seyf Rabiee, M.A. Accuracy of Mean Platelet Volume (MPV) and Red Cell Distribution Width (RDW) for the Diagnosis of Acute Appendicitis: Evaluation of Possible New Biomarkers. Adv. J. Emerg. Med. 2020, 4, e20. [Google Scholar]
- Narci, H.; Turk, E.; Karagulle, E.; Togan, T.; Karabulut, K. The role of red cell distribution width in the diagnosis of acute appendicitis: A retrospective case-controlled study. World J. Emerg. Surg. 2013, 8, 46–51. [Google Scholar] [CrossRef] [Green Version]
- Bozlu, G.; Taskinlar, H.; Unal, S.; Alakaya, M.; Nayci, A.; Kuyucu, N. Diagnostic value of red blood cell distribution width in children with acute appendicitis. Pediatrics Int. 2016, 58, 202–205. [Google Scholar] [CrossRef]
- Kumar, M.S.V.; Tiwari, M.K.; Singh, J.; Malik, A. Plasma Fibrinogen: An Independent Predictor of Pediatric Appendicitis. J. Indian Assoc. Pediatr. Surg. 2021, 26, 240–245. [Google Scholar] [CrossRef]
- Bosak Versic, A.; Glavan, N.; Bukvic, N.; Tomasic, Z.; Nikolic, H. Does elevated urinary 5-hydroxyindole acetic acid level predict acute appendicitis in children? Emerg. Med. J. 2016, 33, 848–852. [Google Scholar] [CrossRef] [Green Version]
- Pogorelić, Z.; Lukšić, B.; Ninčević, S.; Lukšić, B.; Polašek, O. Hyponatremia as a predictor of perforated acute appendicitis in pediatric population: A prospective study. J. Pediatr. Surg. 2021, 56, 1816–1821. [Google Scholar] [CrossRef] [PubMed]
- Andersson, M.; Ruber, M.; Ekerfelt, C.; Hallgren, H.B.; Olaison, G.; Andersson, R.E. Can new inflammatory markers improve the diagnosis of acute appendicitis? World J. Surg. 2014, 38, 2777–2783. [Google Scholar] [CrossRef]
- Destek, S.; Gül, V.O.; Menteş, M.Ö.; Çiçek, A.F. Diagnostic efficacy of serum procalcitonin, IL-6, IL-2, and D-dimer levels in an experimental acute appendicitis model. Turk. J. Gastroenterol. 2019, 30, 641–647. [Google Scholar] [CrossRef]
- Rivera-Chavez, F.A.; Wheeler, H.; Lindberg, G.; Munford, R.S.; O’Keefe, G.E. Regional and systemic cytokine responses to acute inflammation of the vermiform appendix. Ann. Surg. 2003, 237, 408–416. [Google Scholar] [CrossRef] [PubMed]
- Karacan, C.D.; Tuygun, N. Utility of biomarkers in predicting complicated appendicitis: Can immature granulocyte percentage and C-reactive protein be used? Postgrad. Med. 2021, 133, 817–821. [Google Scholar]
- Pogorelić, Z.; Lukšić, A.M.; Mihanović, J.; Đikić, D.; Balta, V. Hyperbilirubinemia as an Indicator of Perforated Acute Appendicitis in Pediatric Population: A Prospective Study. Surg. Infect. 2021. ahead of print. [Google Scholar] [CrossRef] [PubMed]
- Tullavardhana, T.; Sanguanlosit, S.; Chartkitchareon, A. Role of platelet indices as a biomarker for the diagnosis of acute appendicitis and as a predictor of complicated appendicitis: A meta-analysis. Ann. Med. Surg. 2021, 66, 102448. [Google Scholar] [CrossRef]
- Uyanik, B.; Kavalci, C.; Arslan, E.D.; Yilmaz, F.; Aslan, O.; Dede, S.; Bakir, F. Role of mean platelet volume in diagnosis of childhood acute appendicitis. Emerg. Med. Int. 2012, 4, 823095. [Google Scholar] [CrossRef] [Green Version]
- Nissen, M.; Tröbs, R.B. Levels of C-Reactive Protein and Sodium May Differentiate a Perforated Appendix from a Nonperforated Appendix in Children. BioMed Res. Int. 2021, 2021, 9957829. [Google Scholar] [CrossRef]
- Gelpke, K.; Hamminga, J.; Bastelaar, J.; de Vos, B.; Bodegom, M.; Heineman, E.; Hofker, H.S.; El Moumni, M.; Haveman, J.W. Reducing the negative appendectomy rate with the laparoscopic appendicitis score; a multicenter prospective cohort and validation study. Int. J. Surg. 2020, 79, 257–264. [Google Scholar] [CrossRef]
- Dubrovsky, G.; Rouch, J.; Huynh, N.; Freidlander, S.; Lu, Y.; Lee, S. Clinical and socioeconomic factors associated with negative pediatric appendicitis. J. Surg. Res. 2017, 218, 322–328. [Google Scholar] [CrossRef]
- Howell, E.C.; Dubina, E.D.; Lee, S.L. Perforation risk in pediatric appendicitis: Assessment and management. Pediatric. Health Med. Ther. 2018, 9, 135–145. [Google Scholar] [CrossRef] [Green Version]
- Beltran, M.A.; Almonacid, J.; Vicencio, A.; Gutierrez, J.; Cruces, K.S.; Cumsille, M.A. Predictive value of white blood cell count and C-reactive protein in children with appendicitis. J. Pediatr. Surg. 2007, 42, 1208–1214. [Google Scholar] [CrossRef]
- Bux Broh, L.; Mooghal, M.; Ahmed, H.; Khan, W.A.; Malik, J.; Mahmood, T. Diagnostic Precision of C-Reactive Protein Levels, Neutrophil Count and Total Leukocyte Count in Identifying Acute Appendicitis Clinically. J. Surg. Res. 2021, 4, 441–449. [Google Scholar]
- Chiang, J.J.Y.; Angus, M.I.; Nah, S.A.; Jacobsen, A.S.; Low, Y.; Choo, C.S.; Yap, T.L.; Chen, Y. Time course response of inflammatory markers in pediatric appendicitis. Pediatr. Surg. Int. 2020, 36, 493–500. [Google Scholar] [CrossRef]
- Akturk, O.M.; Cakir, M.; Yildirim, D.; Akinci, M. C-reactive protein and red cell distribution width as indicators of complications in patients with acute appendicitis. Arch. Clin. Exp. Med. 2019, 4, 76–80. [Google Scholar] [CrossRef] [Green Version]
- Cetinkaya, E.; Erdogan, A.; Akgul, O.; Celik, C.; Tez, M. High serum cancer antigen 125 level indicates perforation in acute appendicitis. Am. J. Emerg. Med. 2015, 33, 1465–1467. [Google Scholar] [CrossRef] [PubMed]
- Tanrikulu, C.S.; Tanrikulu, Y.; Sabuncuoglu, M.Z.; Karamercan, M.A.; Akkapulu, N.; Coskun, F. Mean Platelet Volume and Red Cell Distribution Width as a Diagnostic Marker in Acute Appendicitis. Iran. Red. Crescent Med. J. 2014, 16, e10211. [Google Scholar] [CrossRef] [Green Version]
- Gasparyan, A.Y.; Ayvazyan, L.; Mikhailidis, D.P.; Kitas, G.D. Mean platelet volume: A link between thrombosis and inflammation? Curr. Pharm. Des. 2011, 17, 47–58. [Google Scholar] [CrossRef]
- Benito, J.; Acedo, Y.; Medrano, L.; Barcena, E.; Garay, R.P.; Arri, E.A. Usefulness of new and traditional serum biomarkers in children with suspected appendicitis. Am. J. Emerg. Med. 2016, 34, 871–876. [Google Scholar] [CrossRef] [PubMed]
- Oktay, M.M.; Boğan, M.; Çolak, S.T.; Sabak, M.; Gümüşboğa, H.; Eren, S.H. Evaluation of the diagnostic value of platelet indices in pediatric acute appendicitis. J. Int. Med. Res. 2020, 48, 300060520946515. [Google Scholar] [CrossRef] [PubMed]
- Bilici, S.; Sekmenli, T.; Goksu, M.; Melek, M.; Avci, V. Mean Platelet volume in diagnosis of acute appendicitis in children. Afr. Health Sci. 2011, 11, 427–432. [Google Scholar] [PubMed]
- Sucu, A.; Tolunay, O.; Cesur, I.B.; Özçelik, Z.; Çelik, T.; Reşitoğlu, S.; Çelik, Ü. Relationship Between Acute Appendicitis and Platelet Indices in Childhood. J. Pediatr. Emerg. Intensive Care Med. 2018, 5, 64–68. [Google Scholar] [CrossRef]
- Daldal, E.; Dagmura, H. The Correlation between Complete Blood Count Parameters and Appendix Diameter for the Diagnosis of Acute Appendicitis. Healthcare 2020, 13, 39. [Google Scholar] [CrossRef] [Green Version]


{kind=link}
{kind=link}
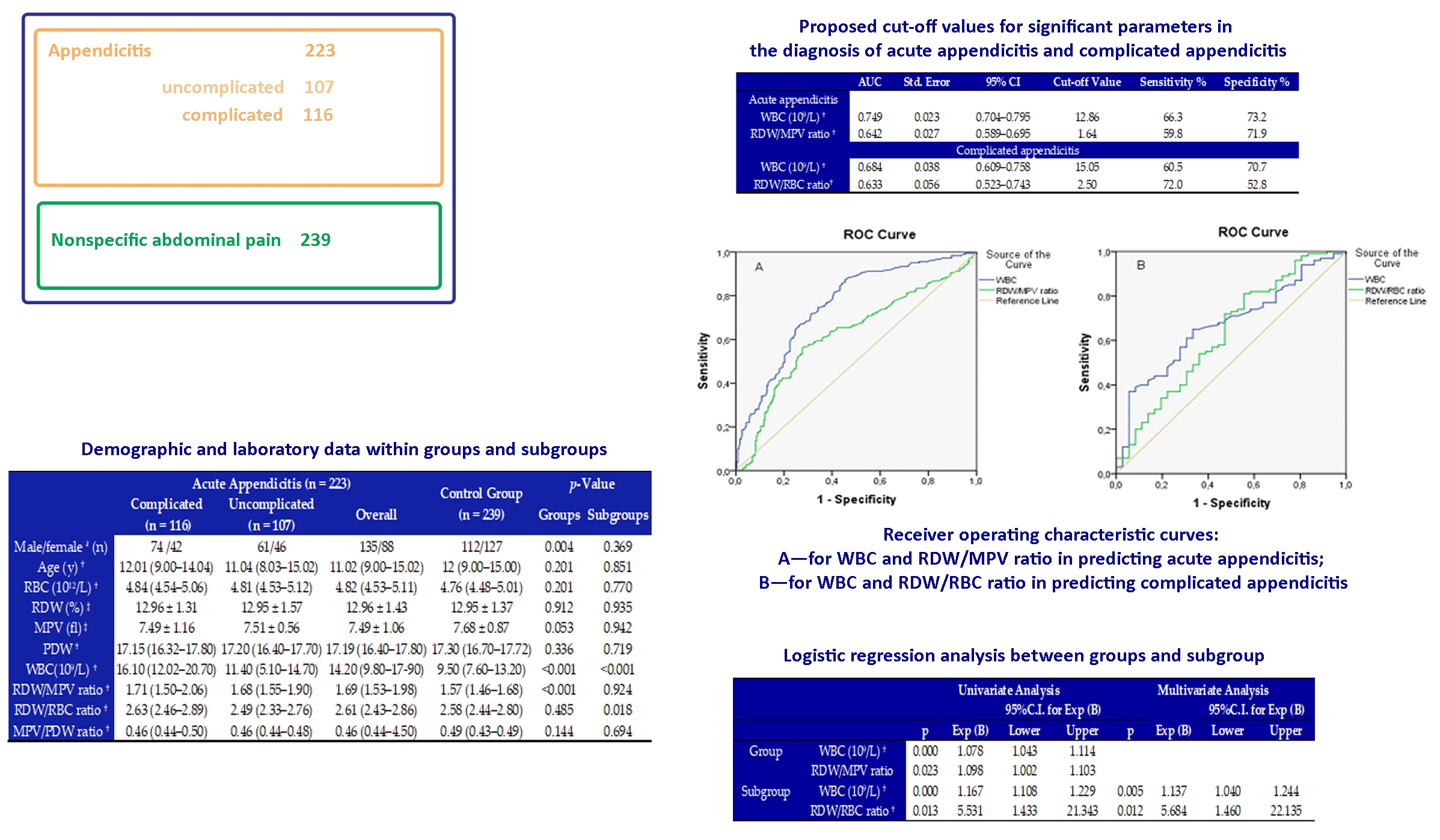
| Acute Appendicitis (n = 223) | Control Group (n = 239) | p-Value | ||||
|---|---|---|---|---|---|---|
| Complicated (n = 116) | Uncomplicated (n = 107) | Overall | Groups | Subgroups | ||
| Male/female # (n) | 74 /42 | 61/46 | 135/88 | 112/127 | 0.004 | 0.369 |
| Age (y) † | 12.01 (9.00–14.04) | 11.04 (8.03–15.02) | 11.02 (9.00–15.02) | 12 (9.00–15.00) | 0.201 | 0.851 |
| RBC (1012/L) † | 4.84 (4.54–5.06) | 4.81 (4.53–5.12) | 4.82 (4.53–5.11) | 4.76 (4.48–5.01) | 0.201 | 0.770 |
| RDW (%) ‡ | 12.96 ± 1.31 | 12.95 ± 1.57 | 12.96 ± 1.43 | 12.95 ± 1.37 | 0.912 | 0.935 |
| MPV (fl) ‡ | 7.49 ± 1.16 | 7.51 ± 0.56 | 7.49 ± 1.06 | 7.68 ± 0.87 | 0.053 | 0.942 |
| PDW † | 17.15 (16.32–17.80) | 17.20 (16.40–17.70) | 17.19 (16.40–17.80) | 17.30 (16.70–17.72) | 0.336 | 0.719 |
| WBC (109/L) † | 16.10 (12.02–20.70) | 11.40 (5.10–14.70) | 14.20 (9.80–17.90) | 9.50 (7.60–13.20) | <0.001 | <0.001 |
| RDW/MPV ratio † | 1.71 (1.50–2.06) | 1.68 (1.55–1.90) | 1.69 (1.53–1.98) | 1.57 (1.46–1.68) | <0.001 | 0.924 |
| RDW/RBC ratio † | 2.63 (2.46–2.89) | 2.49 (2.33–2.76) | 2.61 (2.43–2.86) | 2.58 (2.44–2.80) | 0.485 | 0.018 |
| MPV/PDW ratio † | 0.46 (0.44–0.50) | 0.46 (0.44–0.48) | 0.46 (0.44–4.50) | 0.49 (0.43–0.49) | 0.144 | 0.694 |
| Univariate Analysis | Multivariate Analysis | ||||||||
|---|---|---|---|---|---|---|---|---|---|
| 95% CI for Exp (B) | 95% CI for Exp (B) | ||||||||
| p | Exp (B) | Lower | Upper | p | Exp (B) | Lower | Upper | ||
| Group | WBC (109/L) † | 0.000 | 1.078 | 1.043 | 1.114 | ||||
| RDW/MPV ratio | 0.023 | 1.098 | 1.002 | 1.103 | |||||
| Subgroup | WBC (109/L) † | 0.000 | 1.167 | 1.108 | 1.229 | 0.005 | 1.137 | 1.040 | 1.244 |
| RDW/RBC ratio † | 0.013 | 5.531 | 1.433 | 21.343 | 0.012 | 5.684 | 1.460 | 22.135 | |
| AUC | Std. Error | 95% CI | Cut-Off Value | Sensitivity % | Specificity % | |
|---|---|---|---|---|---|---|
| Acute appendicitis | ||||||
| WBC (109/L) † | 0.749 | 0.023 | 0.704–0.795 | 12.86 | 66.3 | 73.2 |
| RDW/MPV ratio † | 0.642 | 0.027 | 0.589–0.695 | 1.64 | 59.8 | 71.9 |
| Complicated appendicitis | ||||||
| WBC (109/L) † | 0.684 | 0.038 | 0.609–0.758 | 15.05 | 60.5 | 70.7 |
| RDW/RBC ratio † | 0.633 | 0.056 | 0.523–0.743 | 2.50 | 72.0 | 52.8 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Antić, J.; Jokić, R.; Bukarica, S.; Lukić, I.; Dobrijević, D.; Rakić, G.; Pajić, M.; Trajković, V.; Milenković, M. Predictive Value of Red Blood Cell Distribution Width, Mean Platelet Volume and Platelet Distribution Width in Children with Acute Appendicitis. Children 2021, 8, 1041. https://doi.org/10.3390/children8111041
Antić J, Jokić R, Bukarica S, Lukić I, Dobrijević D, Rakić G, Pajić M, Trajković V, Milenković M. Predictive Value of Red Blood Cell Distribution Width, Mean Platelet Volume and Platelet Distribution Width in Children with Acute Appendicitis. Children. 2021; 8(11):1041. https://doi.org/10.3390/children8111041
Chicago/Turabian StyleAntić, Jelena, Radoica Jokić, Svetlana Bukarica, Ivana Lukić, Dejan Dobrijević, Goran Rakić, Miloš Pajić, Veličko Trajković, and Marina Milenković. 2021. "Predictive Value of Red Blood Cell Distribution Width, Mean Platelet Volume and Platelet Distribution Width in Children with Acute Appendicitis" Children 8, no. 11: 1041. https://doi.org/10.3390/children8111041