
Hypomineralized Primary Teeth in Preterm Low Birth Weight Children and Its Association with Molar Incisor Hypomineralization—A 3-Year-Prospective Study

Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Population, Design and Sampling Procedure
- Sociodemographic details: age, gender, parental education, family income.
- Prenatal history: mothers’ medical history, infection during pregnancy, medication history, vitamin D deficiency or hypocalcemia, gestational diabetes, hypertension, pre-eclampsia.
- Perinatal history: Type of delivery (vaginal or caesarean section), premature birth, birth weight, prolonged delivery (perinatal information taken from hospital records).
- Postnatal history: Childhood infection and illness (asthma, urinary tract infection, otitis media, chickenpox, respiratory tract infection, rubella, tonsillitis, high fever, allergies, epilepsy, renal failure, cardiac problems), antibiotic usage, breastfeeding history during the first four years of life.
2.2. Oral Examination
2.3. Followup Examination
2.4. Exclusion Criteria
2.5. Birth Weight and Birth Type
2.6. Socioeconomic Status
2.7. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Seow, W.K. Developmental defects of enamel and dentine: Challenges for basic science research and clinical management. Aust. Dent. J. 2014, 59, 143–154. [Google Scholar] [CrossRef]
- Seow, W.K.; Ford, D.; Kazoullis, S.; Newman, B.; Holcombe, T. Comparison of Enamel Defects in the Primary and Permanent Dentitions of Children from a Low-fluoride District in Australia. Pediatr. Dent. 2011, 33, 207–212. [Google Scholar]
- Tkachenko, T.B.; Savushkina, N.A.; Karpova, L.S. Acquired malformations of hard dental tissue: Molar-Incisor-Hipomineralisation (review of literature). Sci. Notes Pavlov Univ. 2020, 26, 18–22. [Google Scholar] [CrossRef]
- Masumo, R.; Bardsen, A.; Astrom, A.N. Developmental defects of enamel in primary teeth and association with early life course events: A study of 6–36 month old children in Manyara, Tanzania. BMC Oral Health 2013, 13, 21. [Google Scholar] [CrossRef] [Green Version]
- Cruvinel, V.R.; Gravina, D.B.; Azevedo, T.D.; Rezende, C.S.; Bezerra, A.C.; Toledo, O.A. Prevalence of enamel defects and associated risk factors in both dentitions in preterm and fullterm born children. J. Appl. Oral Sci. 2012, 20, 310–317. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Olczak-Kowalczyk, D.; Danko, M.; Banaś, E.; Gozdowski, D.; Popińska, K.; Krasuska-Sławińska, E.; Książyk, J. Parenteral nutrition in childhood and consequences for dentition and gingivae. Eur. J. Paediatr. Dent. 2017, 18, 69–76. [Google Scholar] [PubMed]
- Silva, M.J.; Scurrah, K.J.; Craig, J.M.; Manton, D.J.; Kilpatrick, N. Etiology of molar incisor hypomineralization—A systematic review. Community Dent. Oral Epidemiol. 2016, 44, 342–353. [Google Scholar] [CrossRef]
- Butera, A.; Maiorani, C.; Morandini, A.; Simonini, M.; Morittu, S.; Barbieri, S.; Bruni, A.; Sinesi, A.; Ricci, M.; Trombini, J.; et al. Assessment of Genetical, Pre, Peri and Post Natal Risk Factors of Deciduous Molar Hypomineralization (DMH), Hypomineralized Second Primary Molar (HSPM) and Molar Incisor Hypomineralization (MIH): A Narrative Review. Children 2021, 8, 432. [Google Scholar] [CrossRef] [PubMed]
- Alhowaish, L.; Baidas, L.; Aldhubaiban, M.; Bello, L.L.; Al-Hammad, N. Etiology of Molar-Incisor Hypomineralization (MIH): A Cross-Sectional Study of Saudi Children. Children 2021, 8, 466. [Google Scholar] [CrossRef]
- Massignan, C.; Ximenes, M.; da Silva Pereira, C.; Dias, L.; Bolan, M.; Cardoso, M. Prevalence of enamel defects and association with dental caries in preschool children. Eur. Arch. Paediatr. Dent. 2016, 17, 461–466. [Google Scholar] [CrossRef]
- Gambetta-Tessini, K.; Mariño, R.; Ghanim, A.; Calache, H.; Manton, D.J. The impact of MIH/HSPM on the carious lesion severity of schoolchildren from Talca, Chile. Eur. Arch. Paediatr. Dent. 2019, 20, 417–423. [Google Scholar] [CrossRef]
- Padavala, S.; Sukumaran, G. Molar Incisor Hypomineralization and Its Prevalence. Contemp. Clin. Dent. 2018, 9, S246–S250. [Google Scholar] [PubMed]
- Portella, P.D.; Menoncin, B.L.V.; de Souza, J.F.; de Menezes, J.V.N.B.; Fraiz, F.C.; Assunção, L.R.D.S. Impact of molar incisor hypomineralization on quality of life in children with early mixed dentition: A hierarchical approach. Int. J. Paediatr. Dent. 2019, 29, 496–506. [Google Scholar] [CrossRef]
- Folayan, M.O.; Chukwumah, N.M.; Popoola, B.O.; Temilola, D.O.; Onyejaka, N.K.; Oyedele, T.A.; Lawal, F.B. Developmental defects of the enamel and its impact on the oral health quality of life of children resident in Southwest Nigeria. BMC Oral Health 2018, 18, 160. [Google Scholar] [CrossRef] [PubMed]
- Robles, M.J.; Ruiz, M.; Bravo-Perez, M.; González, E.; Peñalver, M.A. Prevalence of enamel defects in primary and permanent teeth in a group of schoolchildren from Granada (Spain). Med. Oral Patol. Oral Cir. Bucal. 2013, 18, e187–e193. [Google Scholar] [CrossRef]
- Alshehhi, A.; Al Halabi, M.; Hussein, I.; Salami, A.; Hassan, A.; Kowash, M. Enamel defects and caries prevalence in preterm children aged 5–10 years in Dubai. Libyan J. Med. 2020, 15, 1705633. [Google Scholar] [CrossRef] [Green Version]
- Rai, A.; Singh, A.; Menon, I.; Singh, J.; Rai, V.; Aswal, G.S. Molar Incisor Hypomineralization: Prevalence and Risk Factors Among 7–9 Years Old School Children in Muradnagar, Ghaziabad. Open Dent. J. 2018, 12, 714–722. [Google Scholar] [CrossRef]
- Koruyucu, M.; Özel, S.; Tuna, E.B. Prevalence and etiology of molar-incisor hypomineralization (MIH) in the city of Istanbul. J. Dent. Sci. 2018, 13, 318–328. [Google Scholar] [CrossRef] [PubMed]
- Jacobsen, P.E.; Haubek, D.; Henriksen, T.B.; Ostergaard, J.R.; Poulsen, S. Developmental enamel defects in children born preterm: A systematic review. Eur. J. Oral Sci. 2014, 122, 7–14. [Google Scholar] [CrossRef]
- Wu, X.; Wang, J.; Li, Y.H.; Yang, Z.Y.; Zhou, Z. Association of molar incisor hypomineralization with premature birth or low birth weight: Systematic review and meta-analysis. J. Matern. Fetal Neonatal Med. 2020, 33, 1700–1708. [Google Scholar] [CrossRef]
- Bensi, C.; Costacurta, M.; Belli, S.; Paradiso, D.; Docimo, R. Relationship between preterm birth and developmental defects of enamel: A systematic review and meta-analysis. Int. J. Paediatr. Dent. 2020, 30, 676–686. [Google Scholar] [CrossRef] [PubMed]
- da Silva Figueiredo Sé, M.J.; Ribeiro, A.P.D.; Dos Santos-Pinto, L.A.M.; de Cassia Loiola Cordeiro, R.; Cabral, R.N.; Leal, S.C. Are Hypomineralized Primary Molars and Canines Associated with Molar-Incisor Hypomineralization? Pediatr. Dent. 2017, 39, 445–449. [Google Scholar]
- Mittal, N.; Sharma, B.B. Hypomineralised second primary molars: Prevalence, defect characteristics and possible association with Molar Incisor Hypomineralisation in Indian children. Eur. Arch. Paediatr. Dent. 2015, 16, 441–447. [Google Scholar] [CrossRef]
- Mittal, R.; Chandak, S.; Chandwani, M.; Singh, P.; Pimpale, J. Assessment of association between molar incisor hypomineralization and hypomineralized second primary molar. J. Int. Soc. Prev. Community Dent. 2016, 6, 34–39. [Google Scholar] [PubMed] [Green Version]
- Garot, E.; Denis, A.; Delbos, Y.; Manton, D.; Silva, M.; Rouas, P. Are hypomineralised lesions on second primary molars (HSPM) a predictive sign of molar incisor hypomineralisation (MIH)? A systematic review and a meta-analysis. J. Dent. 2018, 72, 8–13. [Google Scholar] [CrossRef]
- A review of the developmental defects of enamel index (DDE Index): Commission on Oral Health, Research & Epidemiology. Report of an FDI Working Group. Int. Dent. J. 1992, 42, 411–426.
- Weerheijm, K.L.; Duggal, M.; Mejàre, I.; Papagiannoulis, L.; Koch, G.; Martens, L.C.; Hallonsten, A.L. Judgment criteria for molar incisor hypomineralization (MIH) in epidemiologic studies: A summary of the European meeting on MIH held in Athens, 2003. Eur. J. Paediatr. Dent. 2003, 4, 110–113. [Google Scholar]
- World Health Organization. Oral Health Surveys: Basic Methods, 5th ed.; World Health Organization: Geneva, Switzerland, 2013. [Google Scholar]
- Leone, C.R.; Sadeck, L.S.; Vaz, F.A. Brazilian Neonatal Research Network (BNRN): Very low birth weight infant (VLBW) infant morbidity and mortality. Pediatr. Res. 2001, 49, 405. [Google Scholar]
- Sharma, R. Revision of Prasad’s social classification and provision of an online tool for real-time updating. South Asian J. Cancer 2013, 2, 157. [Google Scholar] [CrossRef]
- Neggers, Y.H. The relationship between preterm birth and underweight in Asian women. Reprod. Toxicol. 2015, 56, 170–174. [Google Scholar] [CrossRef] [PubMed]
- Christian, P.; Lee, S.E.; Angel, M.D.; Adair, L.S.; Arifeen, S.; Ashorn, P.; Barros, F.C.; Fall, C.; Fawzi, W.W.; Hao, W.; et al. Risk of childhood undernutrition related to small-for-gestational age and preterm birth in low- and middle-income countries. Int. J. Epidemiol. 2013, 42, 1340–1355. [Google Scholar] [CrossRef]
- Tourino, L.F.P.; Zarzar, P.M.; Corrêa-Faria, P.; Paiva, S.M.; Vale, M.P.P. Prevalence and factors associated with enamel defects among preschool children from a southeastern city in Brazil. Ciênc. Saúde Coletiva 2018, 23, 1667–1674. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Merglova, V.; Dort, J. Developmental enamel defects of primary incisors in preterm infants with very low and extremely low birthweight. A case- control study. Eur. J. Paediatr. Dent. 2020, 21, 318–322. [Google Scholar] [PubMed]
- Basha, S.; Mohamed, R.N.; Swamy, H.S. Prevalence and associated factors to developmental defects of enamel in primary and permanent dentition. Oral Health Dent. Manag. 2014, 13, 588–594. [Google Scholar] [PubMed]



{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variables | Study Group n = 287 | % or Range | Control Group n = 290 | % or Range |
|---|---|---|---|---|
| Gender | ||||
| Boys | 124 | 43.2 | 130 | 44.8 |
| Girls | 163 | 56.8 | 160 | 55.2 |
| Chi-squared p value | 0.12 | |||
| Birth weight | ||||
| VLBW | 37 | 12.9 | 0 | 0 |
| LBW | 250 | 87.1 | 0 | 0 |
| NBW | 0 | 0 | 290 | 100 |
| Mean birth weight in kg | 1.65 ± 0.1 | 1050–1830 g | 2.84 ± 1.2 | 2720–3900 g |
| Gestational age | ||||
| <34 weeks | 11 | 3.8 | 0 | 0 |
| 34 weeks to <37 weeks | 212 | 73.9 | 0 | 0 |
| >37 weeks | 64 | 22.3 | 290 | 100 |
| Mean gestational age in weeks | 35.1 ± 2.1 | 26–36 | 39.5 ± 2.2 | 37–42 |
| SES | ||||
| Upper class | 11 | 3.8 | 23 | 7.9 |
| Middle class | 113 | 39.4 | 98 | 33.8 |
| Lowe class | 163 | 56.8 | 169 | 58.3 |
| Kruskal–Wallis p value | 0.18 | |||
| Prenatal history | ||||
| Yes | 123 | 42.9 | 63 | 21.7 |
| No | 164 | 57.1 | 227 | 78.3 |
| Chi-squared p value | 0.03 | |||
| Postnatal History/Childhood Infection | ||||
| Yes | 135 | 47 | 179 | 61.7 |
| No | 152 | 53 | 111 | 38.3 |
| Chi-squared p value | 0.07 | |||
| Variables | EH Yes (%) | EH No (%) | MIH Yes (%) | MIH No (%) |
|---|---|---|---|---|
| Gender | ||||
| Boys (n = 254) | 111 (43.7) | 143 (56.3) | 92 (36.2) | 162 (63.8) |
| Girls (n = 323) | 168 (52.0) | 155 (48.0) | 115 (35.6) | 208 (64.4) |
| Chi-Square, p value | 0.135 | 0.126 | ||
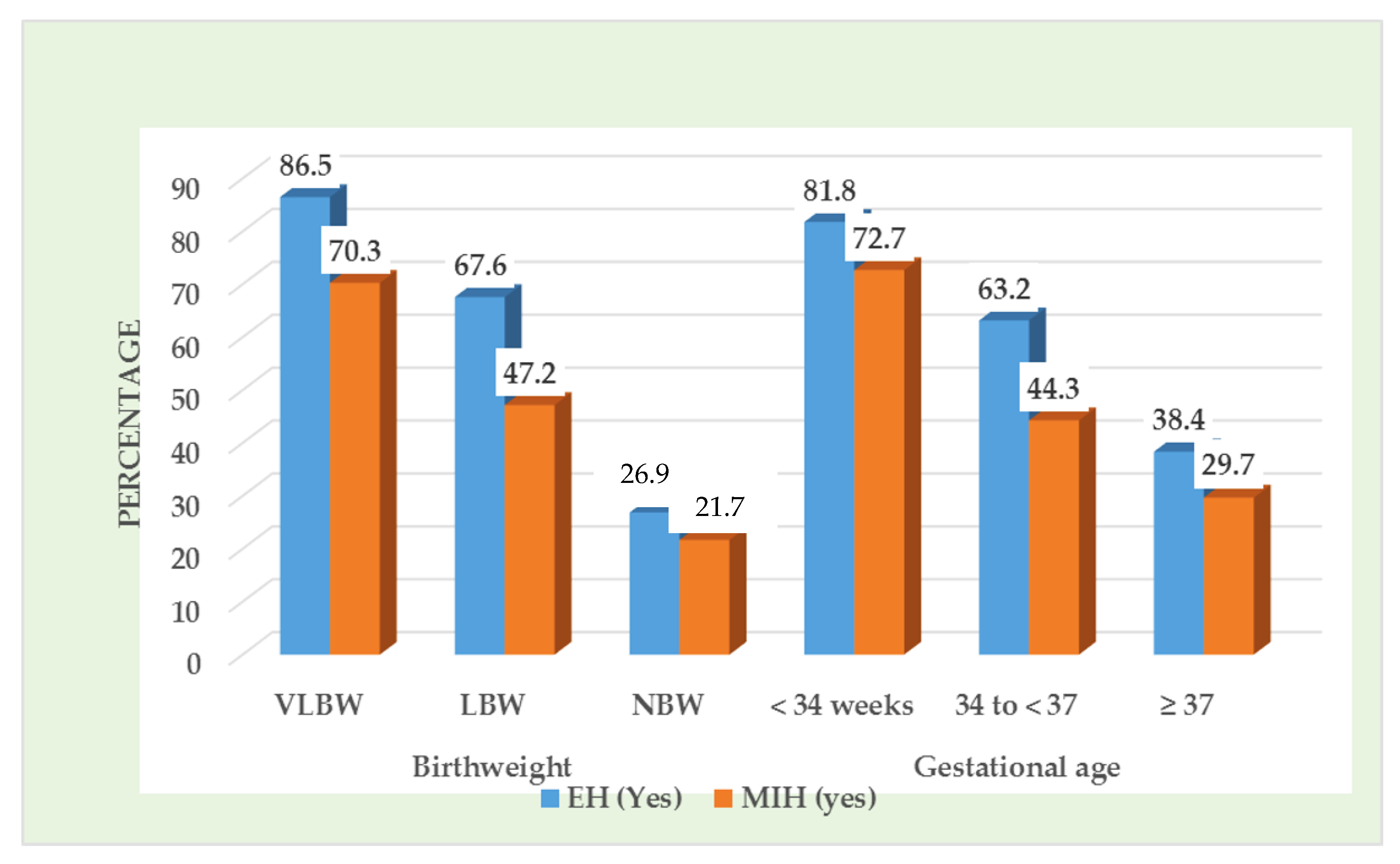
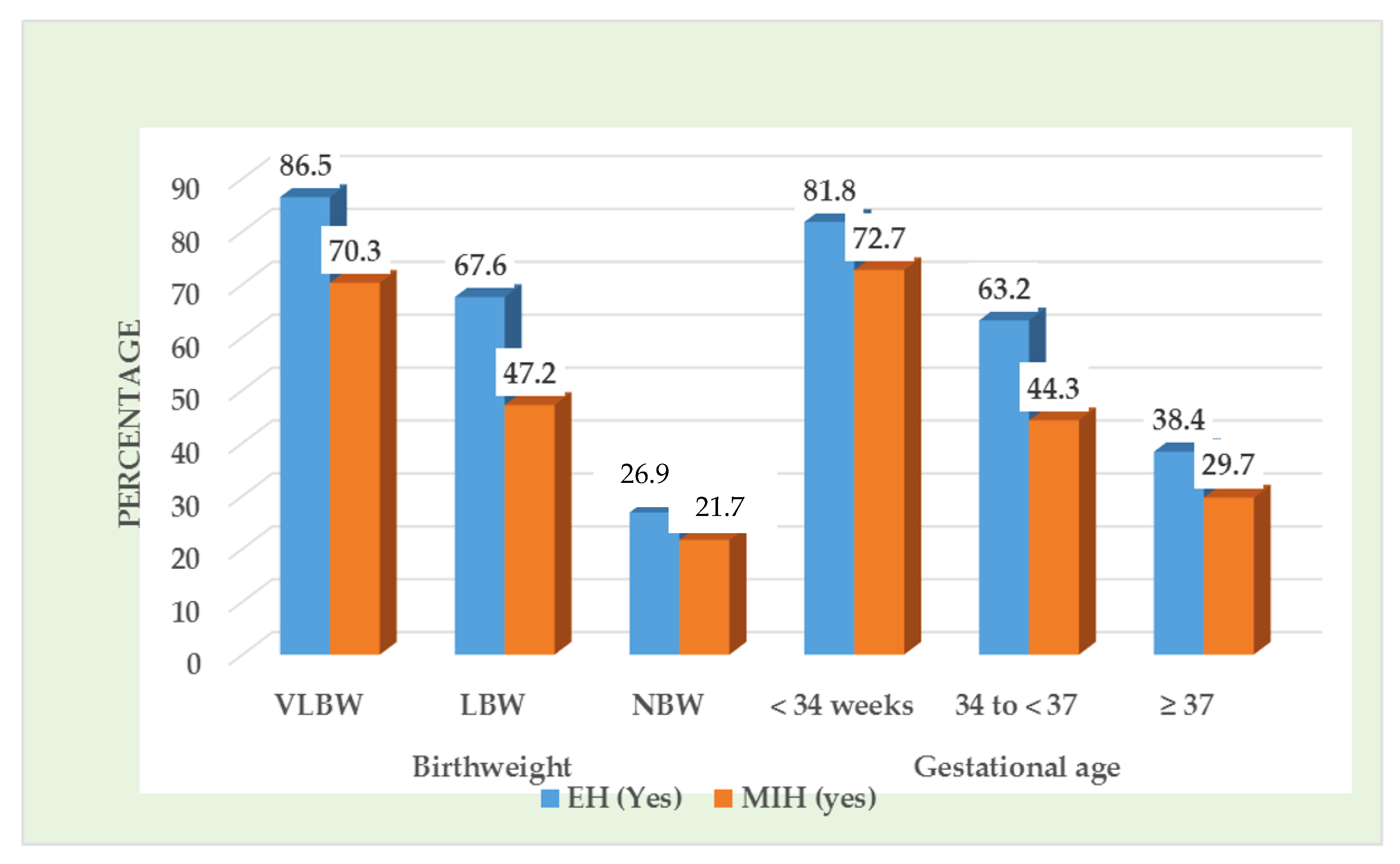
| Birth weight | ||||
| VLBW a (n = 37) | 32 (86.5) | 5 (13.5) | 26 (70.3) | 11 (29.7) |
| LBW b (n = 250) | 169 (67.6) | 81 (32.4) | 118 (47.2) | 132 (52.8) |
| NBW c (n = 290) | 78 (26.9) | 212 (73.1) | 63 (21.7) | 227 (78.3) |
| Kruskal–Wallis, p | 0.001 | 0.03 | ||
| Mann–Whitney U | a > b (U = 118, p = 0.031) a > c (U = 124, p = 0.001) b > c (U = 116, p = 0.022) | a > b (U = 98, p = 0.042) a > c (U = 112, p = 0.021) b > c (U = 102, p = 0.031) | ||
| Gestational age | ||||
| <34 weeks d (n = 11) | 9 (81.8) | 2 (18.2) | 8 (72.7) | 3 (27.3) |
| 34 to <37 e (n = 212) | 134 (63.2) | 78 (36.8) | 94 (44.3) | 118 (55.7) |
| ≥37 f (n = 354) | 136 (38.4) | 218 (61.6) | 105 (29.7) | 249 (70.3) |
| Kruskal–Wallis, p | 0.04 | 0.03 | ||
| Mann–Whitney U | d > f (U = 114, p = 0.036) e > f (U = 96, p = 0.042) | d > e (U = 92, p = 0.041) d > f (U = 112, p = 0.023) e > f (U = 94, p = 0.041) | ||
| SES | ||||
| Upper (n = 34) | 7 (20.6) | 27 (79.4) | 6 (17.6) | 28 (82.4) |
| Middle (n = 211) | 86 (40.8) | 125 (59.2) | 72 (34.1) | 139 (65.9) |
| Lower (n = 332) | 186 (56.0) | 146 (44.0) | 129 (38.9) | 203 (61.1) |
| Kruskal–Wallis H, p | 0.05 | 0.06 | ||
| Prenatal history | ||||
| Yes (n = 186) | 57 (30.6) | 129 (69.4) | 42 (22.6) | 144 (77.4) |
| No (n = 391) | 222 (56.8) | 169 (43.2) | 165 (42.2) | 226 (57.8) |
| Chi-squared, p | 0.03 | 0.04 | ||
| Postnatal History/Childhood Infection | ||||
| Yes (n = 314) | 202 (64.3) | 112 (35.7) | 142 (45.2) | 172 (54.8) |
| No (n = 263) | 77 (29.3) | 186 (70.7) | 65 (24.7) | 198 (75.3) |
| Chi-squared, p | 0.002 | 0.03 | ||
| Subjects with Hypomineralized Primary Second Molars | ||||
| Yes (n = 176) | NA | 135 (76.7) | 41 (23.3) | |
| No (n = 401) | NA | 72(18.0) | 329 (82.0) | |
| Chi-squared, p | 0.001 | |||
| Study Group with Teeth | EH in Primary Teeth n (%) | MIH n (%) |
|---|---|---|
| PT-LBW | ||
| Incisor | 209/2061 (10.1) | 97/2218 (4.4) |
| Canine | 63/1011(6.2) | NA |
| Molar | 334/2033 (16.4) | 152/1139 (13.3) |
| FTNBW | ||
| Incisor | 79/2190 (3.6) | 33/2308 (1.4) |
| Canine | 20/1029 (1.9) | NA |
| Molar | 144/2288 (6.3) | 94/1153 (8.2) |
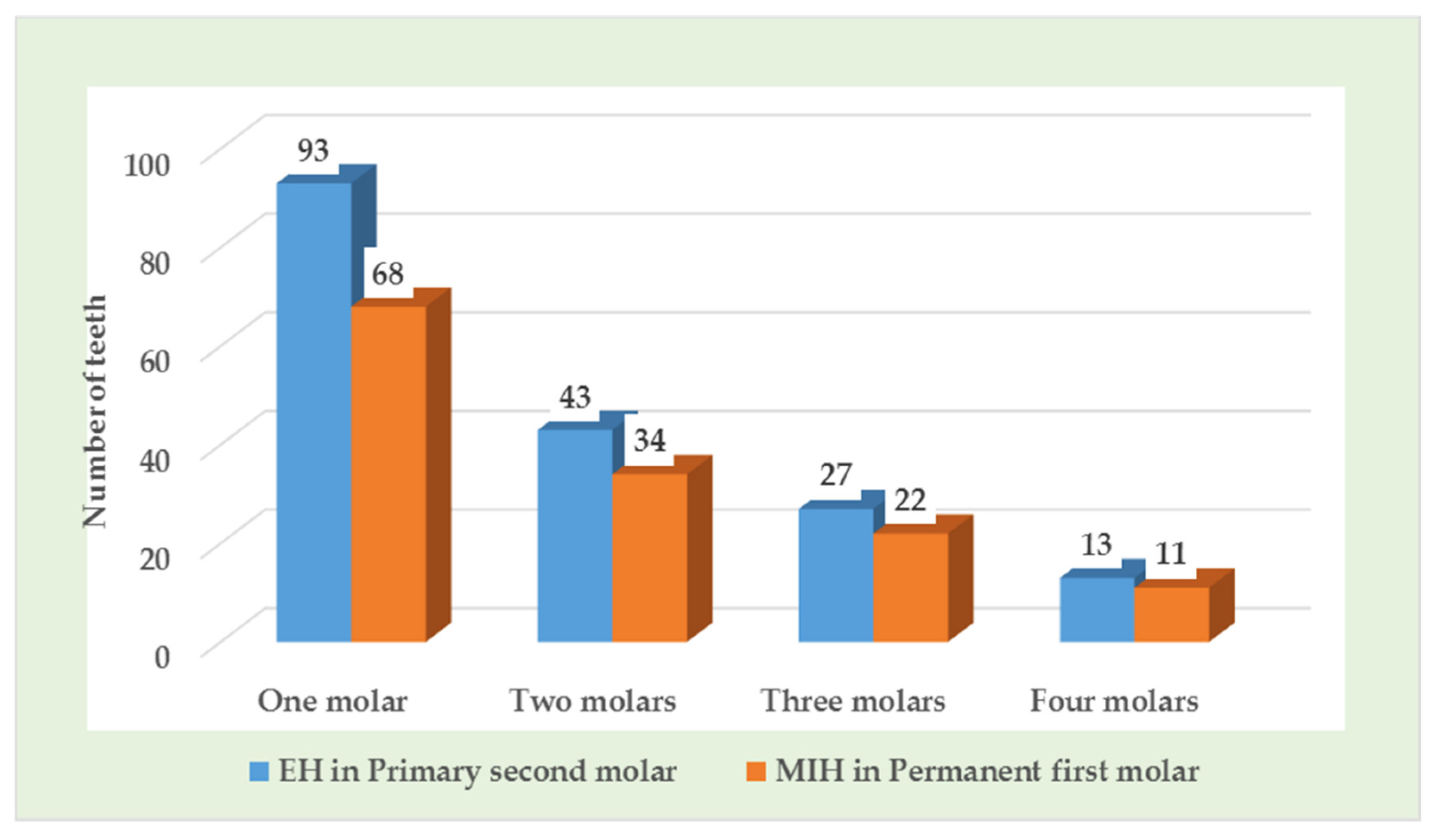
| Number of SPM/PFMs Affected/Child | ||
| One molar | 93 (52.8) | 68 (50.3) |
| Two molars | 43 (24.4) | 34 (25.2) |
| Three molars | 27 (15.3) | 22 (16.3) |
| Four molars | 13 (7.4) | 11 (8.1) |
| Total | 176 | 135 |
| Mean (SD) affected molars | 2.3 (1.1) | 2.1 (0.9) |
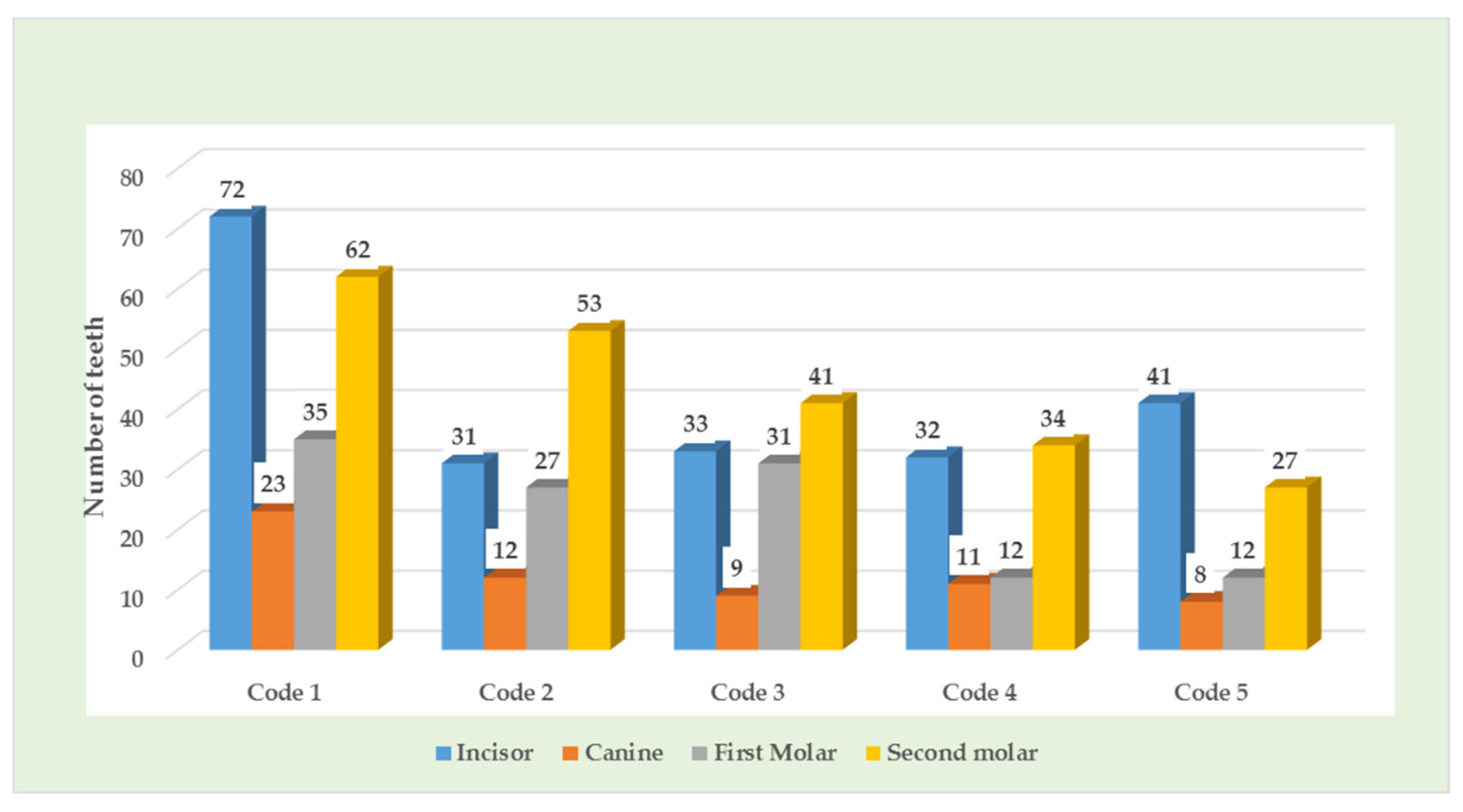
| Study Group with Teeth | Modified DDE Index by FDI, n (%) | |||||
|---|---|---|---|---|---|---|
| Code 1 | Code 2 | Code 3 | Code 4 | Code 5 | No DDE | |
| PTLBW | ||||||
| Incisor (n = 2061) | 72 (3.5) | 31 (1.5) | 33 (1.6) | 32 (1.5) | 41 (2.0) | 1852 (89.9) |
| Canine (n = 1011) | 23 (2.3) | 12 (1.2) | 9 (0.9) | 11 (1.1) | 8 (0.8) | 948 (93.7) |
| First molar (n = 924) | 35 (3.8) | 27 (2.9) | 31 (3.4) | 12 (1.3) | 12 (1.3) | 807 (87.3) |
| Second molar (n = 1109) | 62 (5.6) | 53 (4.8) | 41 (3.7) | 34 (3.1) | 27 (2.4) | 892 (80.4) |
| Kruskal–Wallis, p value | 0.143 | |||||
| FTNBW | ||||||
| Incisor (n = 2190) | 23 (1.0) | 13 (0.6) | 11 (0.5) | 17 (0.8) | 15 (0.7) | 2111 (96.4) |
| Canine (n = 1029) | 6 (0.6) | 4 (0.4) | 0 | 2 (0.2) | 8 (0.8) | 1009 (98.0) |
| First molar (n = 1138) | 10 (0.9) | 9 (0.8) | 12 (1.0) | 11 (1.0) | 7 (0.6) | 1089 (95.7) |
| Second molar (n = 1150) | 19 (1.6) | 25 (2.2) | 17 (1.5) | 16 (1.4) | 18 (1.6) | 1055 (91.7) |
| Kruskal–Wallis | 0.162 | |||||
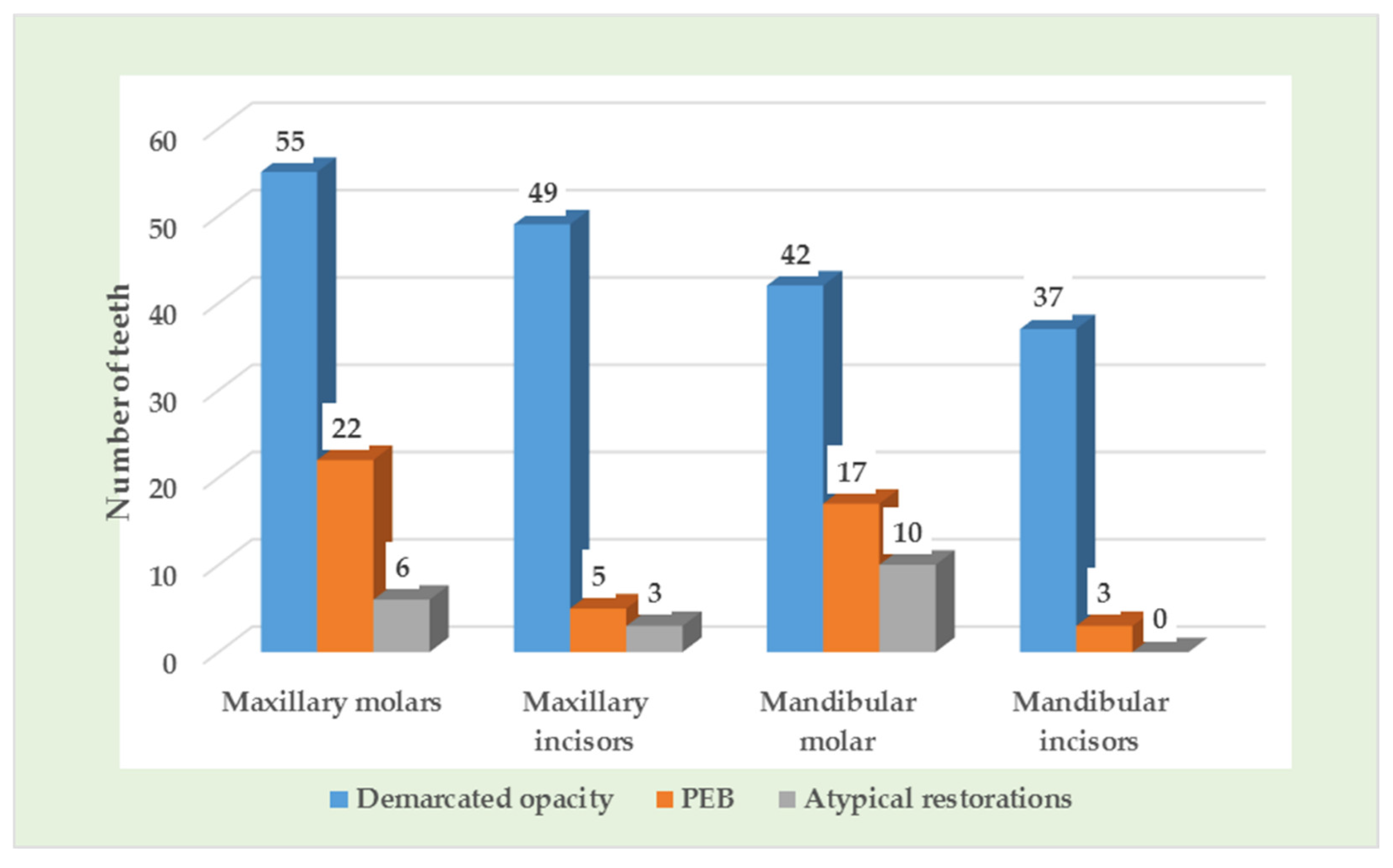
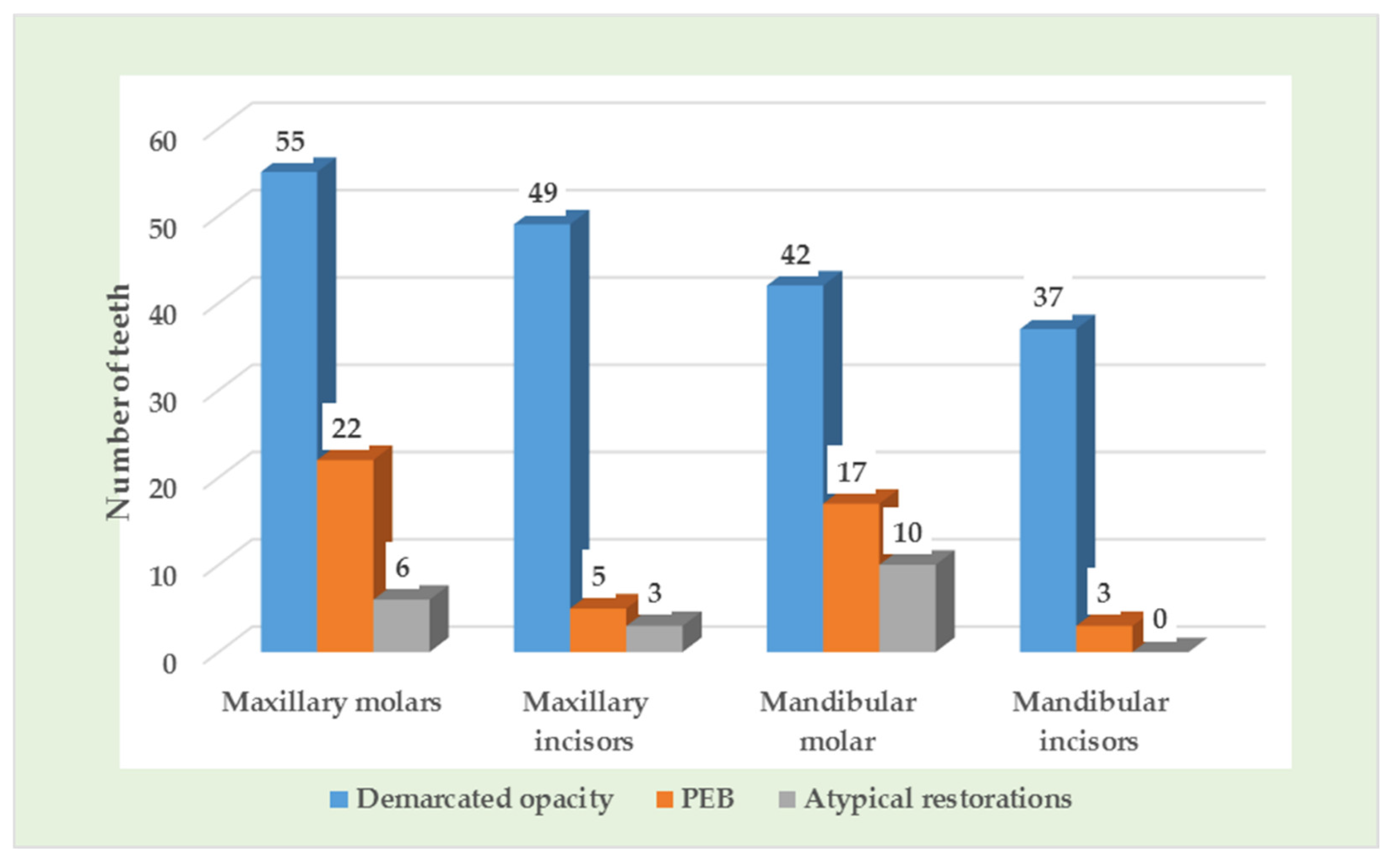
| Study Group with Teeth | MIH Category According to EAPD, n (%) | ||||
|---|---|---|---|---|---|
| Demarcated OPACITY | PEB | Atypical Restorations | Tooth Loss due to MIH | Tooth without MIH | |
| PTLBW | |||||
| Maxillary molars (n = 568) | 55 (9.7) | 22 (3.9) | 6 (1.0) | 0 | 485 (85.4) |
| Maxillary incisors (n = 1106) | 49 (4.4) | 5 (0.5) | 3 (0.3) | 0 | 1049 (94.8) |
| Mandibular molar (n = 571) | 42 (7.4) | 17 (3.0) | 10 (1.7) | 0 | 502 (87.9) |
| Mandibular incisors (n = 1112) | 37 (3.3) | 3 (0.3) | 0 | 0 | 1072 (96.4) |
| FTNBW | |||||
| Maxillary molars (n = 577) | 42 (7.3) | 4 (0.7) | 2 (0.3) | 0 | 529 (91.7) |
| Maxillary incisors (n = 1152) | 18 (1.6) | 0 | 0 | 0 | 1134 (98.4) |
| Mandibular molar (n = 576) | 37 (6.4) | 4 (0.7) | 5 (0.9) | 0 | 530 (9.2) |
| Mandibular incisors (n = 1156) | 15 (1.3) | 0 | 0 | 0 | 1141 (98.7) |
| Variable | Odds Ratio (95% CI) | R2 | p Value |
|---|---|---|---|
| PT-LBW | 2.11 (0.97–4.08) | 0.18 | 0.005 |
| Subjects with primary second molar hypomineralization | 2.13 (0.98–4.19) | 0.19 | 0.005 |
| Adjusted for childhood infection | 2.32 (0.98–4.26) | 0.22 | 0.005 |
| Adjusted for childhood infection and prenatal history | 2.37 (0.96–4.37) | 0.24 | 0.005 |
| Adjusted for childhood infection, prenatal history, and presence of hypomineralized second primary molar | 3.02 (1.01–5.94) | 0.31 | 0.005 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Noor Mohamed, R.; Basha, S.; Virupaxi, S.G.; Idawara Eregowda, N.; Parameshwarappa, P. Hypomineralized Primary Teeth in Preterm Low Birth Weight Children and Its Association with Molar Incisor Hypomineralization—A 3-Year-Prospective Study. Children 2021, 8, 1111. https://doi.org/10.3390/children8121111
Noor Mohamed R, Basha S, Virupaxi SG, Idawara Eregowda N, Parameshwarappa P. Hypomineralized Primary Teeth in Preterm Low Birth Weight Children and Its Association with Molar Incisor Hypomineralization—A 3-Year-Prospective Study. Children. 2021; 8(12):1111. https://doi.org/10.3390/children8121111
Chicago/Turabian StyleNoor Mohamed, Roshan, Sakeenabi Basha, Shruti Girish Virupaxi, Neena Idawara Eregowda, and Poornima Parameshwarappa. 2021. "Hypomineralized Primary Teeth in Preterm Low Birth Weight Children and Its Association with Molar Incisor Hypomineralization—A 3-Year-Prospective Study" Children 8, no. 12: 1111. https://doi.org/10.3390/children8121111
APA StyleNoor Mohamed, R., Basha, S., Virupaxi, S. G., Idawara Eregowda, N., & Parameshwarappa, P. (2021). Hypomineralized Primary Teeth in Preterm Low Birth Weight Children and Its Association with Molar Incisor Hypomineralization—A 3-Year-Prospective Study. Children, 8(12), 1111. https://doi.org/10.3390/children8121111