
Tracheal Tube Misplacement after Emergency Intubation in Pediatric Trauma Patients: A Retrospective, Exploratory Study

 ,
, 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
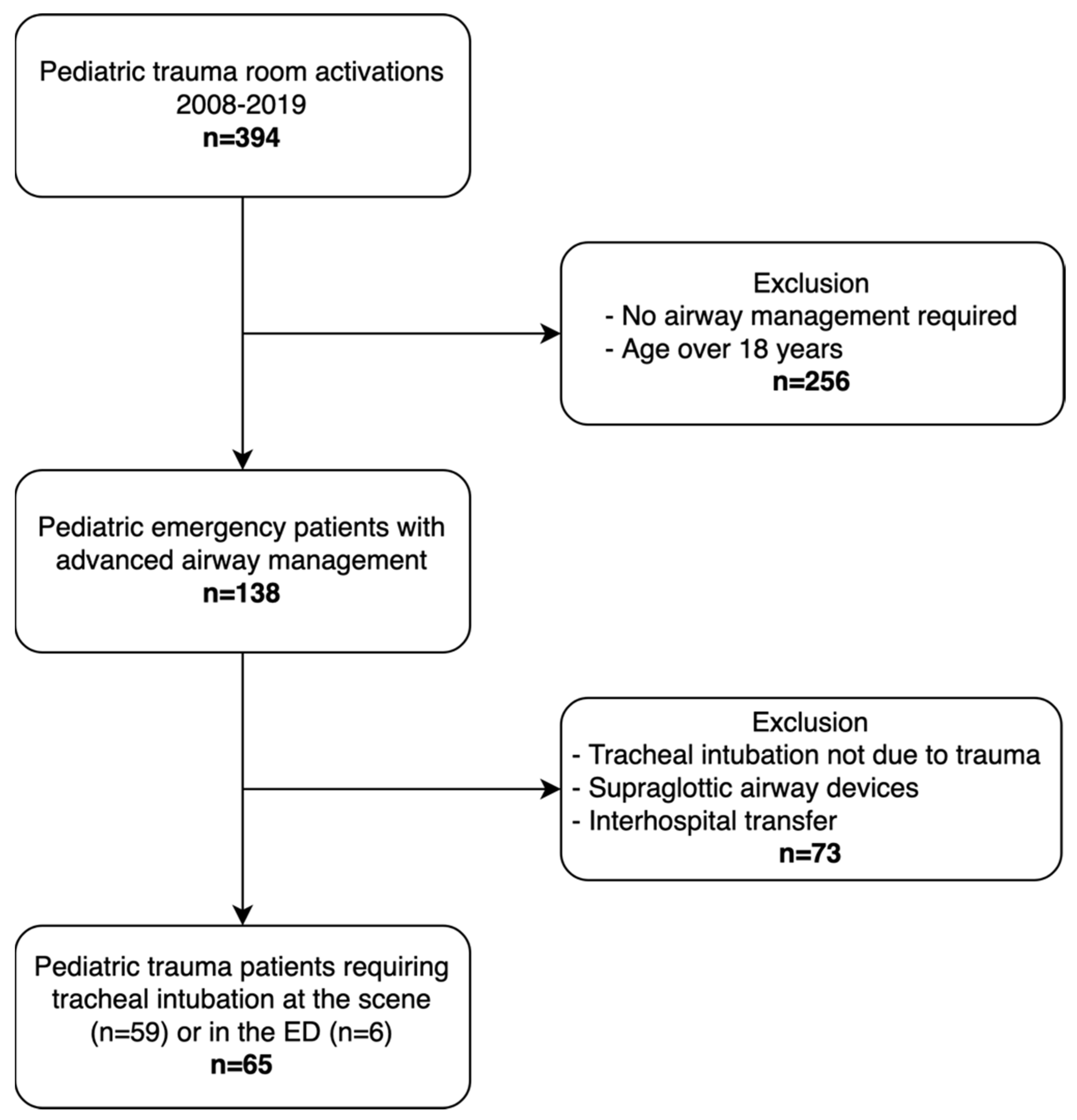
2.2. Patient Enrollment
2.3. General Management
2.4. Statistical Analysis
3. Results
3.1. Baseline Characteristics
3.2. Tracheal Intubation
3.3. Risk Factors Associated with Tracheal Tube Misplacement
3.4. Characteristics of Helicopter EMS and Ground EMS
3.5. Clinical Consequences of Tracheal Tube Misplacement
4. Discussion
Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Carlson, J.N.; Gannon, E.; Mann, N.C.; Jacobson, K.E.; Dai, M.; Colleran, C.; Wang, H.E. Pediatric Out-of-Hospital Critical Procedures in the United States. Pediatr. Crit. Care Med. 2015, 16, e260–e267. [Google Scholar] [CrossRef] [PubMed]
- Hansen, M.; Lambert, W.; Guise, J.M.; Warden, C.R.; Mann, N.C.; Wang, H. Out-of-hospital pediatric airway management in the United States. Resuscitation 2015, 90, 104–110. [Google Scholar] [CrossRef] [Green Version]
- Eich, C.; Roessler, M.; Nemeth, M.; Russo, S.G.; Heuer, J.F.; Timmermann, A. Characteristics and outcome of prehospital paediatric tracheal intubation attended by anaesthesia-trained emergency physicians. Resuscitation 2009, 80, 1371–1377. [Google Scholar] [CrossRef]
- Rodríguez, J.J.; Higuita-Gutiérrez, L.F.; Carrillo Garcia, E.A.; Castaño Betancur, E.; Luna Londoño, M.; Restrepo Vargas, S. Meta-Analysis of Failure of Prehospital Endotracheal Intubation in Pediatric Patients. Emerg. Med. Int. 2020, 2020, 7012508. [Google Scholar] [CrossRef] [PubMed]
- Garner, A.A.; Bennett, N.; Weatherall, A.; Lee, A. Success and complications by team composition for prehospital paediatric intubation: A systematic review and meta-analysis. Crit. Care 2020, 24, 149. [Google Scholar] [CrossRef] [Green Version]
- Garner, A.A.; Bennett, N.; Weatherall, A.; Lee, A. Physician-staffed helicopter emergency medical services augment ground ambulance paediatric airway management in urban areas: A retrospective cohort study. Emerg. Med. J. 2019, 36, 678–683. [Google Scholar] [CrossRef] [PubMed]
- Bläsius, F.M.; Horst, K.; Brokmann, J.C.; Lefering, R.; Andruszkow, H.; Hildebrand, F.; TraumaRegister Dgu. Helicopter Emergency Medical Service and Hospital Treatment Levels Affect Survival in Pediatric Trauma Patients. J. Clin. Med. 2021, 10, 837. [Google Scholar] [CrossRef] [PubMed]
- Nevin, D.G.; Green, S.J.; Weaver, A.E.; Lockey, D.J. An observational study of paediatric pre-hospital intubation and anaesthesia in 1933 children attended by a physician-led, pre-hospital trauma service. Resuscitation 2014, 85, 189–195. [Google Scholar] [CrossRef]
- Gerritse, B.M.; Draaisma, J.M.; Schalkwijk, A.; van Grunsven, P.M.; Scheffer, G.J. Should EMS-paramedics perform paediatric tracheal intubation in the field? Resuscitation 2008, 79, 225–229. [Google Scholar] [CrossRef] [PubMed]
- Lohser, J.; Slinger, P. Lung Injury after One-Lung Ventilation: A Review of the Pathophysiologic Mechanisms Affecting the Ventilated and the Collapsed Lung. Anesth. Analg. 2015, 121, 302–318. [Google Scholar] [CrossRef] [PubMed]
- Heyne, G.; Ewens, S.; Kirsten, H.; Fakler, J.K.M.; Özkurtul, O.; Hempel, G.; Krämer, S.; Struck, M.F. Risk factors and outcomes of unrecognised endobronchial intubation in major trauma patients. Emerg. Med. J. 2021. [Google Scholar] [CrossRef] [PubMed]
- Simons, T.; Söderlund, T.; Handolin, L. Radiological evaluation of tube depth and complications of prehospital endotracheal intubation in pediatric trauma: A descriptive study. Eur. J. Trauma Emerg. Surg. 2017, 43, 797–804. [Google Scholar] [CrossRef]
- Tarpgaard, M.; Hansen, T.M.; Rognås, L. Anaesthetist-provided pre-hospital advanced airway management in children: A descriptive study. Scand. J. Trauma Resusc. Emerg. Med. 2015, 23, 61. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Burns, B.J.; Watterson, J.B.; Ware, S.; Regan, L.; Reid, C. Analysis of Out-of-Hospital Pediatric Intubation by an Australian Helicopter Emergency Medical Service. Ann. Emerg. Med. 2017, 70, 773–782.e4. [Google Scholar] [CrossRef]
- Schmidt, A.R.; Ulrich, L.; Seifert, B.; Albrecht, R.; Spahn, D.R.; Stein, P. Ease and difficulty of pre-hospital airway management in 425 paediatric patients treated by a helicopter emergency medical service: A retrospective analysis. Scand. J. Trauma Resusc. Emerg. Med. 2016, 24, 22. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- To, Y.H.; Ong, Y.G.; Chong, S.L.; Ang, P.H.; Bte Zakaria, N.D.; Lee, K.P.; Pek, J.H. Differences in intubation outcomes for pediatric patients between pediatric and general Emergency Departments. Paediatr. Anaesth. 2021, 31, 713–719. [Google Scholar] [CrossRef] [PubMed]
- Easley, R.B.; Segeleon, J.E.; Haun, S.E.; Tobias, J.D. Prospective study of airway management of children requiring endotracheal intubation before admission to a pediatric intensive care unit. Crit. Care Med. 2000, 28, 2058–2063. [Google Scholar] [CrossRef]
- Sagarin, M.J.; Chiang, V.; Sakles, J.C.; Barton, E.D.; Wolfe, R.E.; Vissers, R.J.; Walls, R.M.; National Emergency Airway Registry (NEAR) investigators. Rapid sequence intubation for pediatric emergency airway management. Pediatr. Emerg. Care 2002, 18, 417–423. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Matettore, A.; Ramnarayan, P.; Jones, A.; Randle, E.; Lutman, D.; O’Connor, M.; Chigaru, L. Adverse Tracheal Intubation-Associated Events in Pediatric Patients at Nonspecialist Centers: A Multicenter Prospective Observational Study. Pediatr. Crit. Care Med. 2019, 20, 518–526. [Google Scholar] [CrossRef] [PubMed]
- Miller, K.A.; Kimia, A.; Monuteaux, M.C.; Nagler, J. Factors Associated with Misplaced Endotracheal Tubes during Intubation in Pediatric Patients. J. Emerg. Med. 2016, 51, 9–18. [Google Scholar] [CrossRef] [PubMed]
- Bai, W.; Golmirzaie, K.; Burke, C.; Van Veen, T.; Christensen, R.; Voepel-Lewis, T.; Malviya, S. Evaluation of emergency pediatric tracheal intubation by pediatric anesthesiologists on inpatient units and the emergency department. Paediatr. Anaesth. 2016, 26, 384–391. [Google Scholar] [CrossRef] [PubMed]
- Deutsche Deutsche Gesellschaft für Kinderchirurgie e.V. (DGKCH). Polytraumaversorgung im Kindesalter. AWMF-Register-Nr. 006-120, Klasse S2k. 2020. Available online: https://www.awmf.org/uploads/tx_szleitlinien/006-120k_S2k_Polytraumaversorgung-im-Kindesalter_2020-12.pdf (accessed on 19 January 2022).
- Deutsche Gesellschaft für Unfallchirurgie e.V. (DGU). Polytrauma/Schwerverletzten-Behandlung. AWMF-Register Nr. 012/019, Klasse: S3. 2016. Available online: http://www.awmf.org/uploads/tx_szleitlinien/012-019l_S3_Polytrauma_Schwerverletzten-Behandlung_2016-09.pdf (accessed on 19 January 2022).
- Volsko, T.A.; McNinch, N.L.; Prough, D.S.; Bigham, M.T. Adherence to Endotracheal Tube Depth Guidelines and Incidence of Malposition in Infants and Children. Respir. Care 2018, 63, 1111–1117. [Google Scholar] [CrossRef] [PubMed]
- Sunde, G.A.; Kottmann, A.; Heltne, J.K.; Sandberg, M.; Gellerfors, M.; Krüger, A.; Lockey, D.; Sollid, S.J.M. Standardised data reporting from pre-hospital advanced airway management—A nominal group technique update of the Utstein-style airway template. Scand. J. Trauma Resusc. Emerg. Med. 2018, 26, 46. [Google Scholar] [CrossRef]
- Yan, S.; Zhang, H. Impact of changes in head position during head and neck surgery on the depth of tracheal tube intubation in anesthetized children. BMC Anesthesiol. 2020, 20, 124. [Google Scholar] [CrossRef] [PubMed]
- Kim, J.T.; Kim, H.J.; Ahn, W.; Kim, H.S.; Bahk, J.H.; Lee, S.C.; Kim, C.S.; Kim, S.D. Head rotation, flexion, and extension alter endotracheal tube position in adults and children. Can. J. Anaesth. 2009, 56, 751–756. [Google Scholar] [CrossRef] [Green Version]
- Weiss, M.; Knirsch, W.; Kretschmar, O.; Dullenkopf, A.; Tomaske, M.; Balmer, C.; Stutz, K.; Gerber, A.C.; Berger, F. Tracheal tube-tip displacement in children during head-neck movement—A radiological assessment. Br. J. Anaesth. 2006, 96, 486–491. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Herway, S.T.; Benumof, J.L. The tracheal accordion and the position of the endotracheal tube. Anaesth. Intensive Care 2017, 45, 177–188. [Google Scholar] [CrossRef] [PubMed]
- Jain, A.; Wadhwa, B.; Saxena, K.N. Preventing inadvertent Endobronchial intubation: Upper incisor to manubriosternal joint length as a predictor of airway length in children. Paediatr. Anaesth. 2020, 30, 1240–1244. [Google Scholar] [CrossRef] [PubMed]
- Lee, B.J.; Yi, J.W.; Chung, J.Y.; Kim, D.O.; Kang, J.M. Bedside prediction of airway length in adults and children. Anesthesiology 2009, 111, 556–560. [Google Scholar] [CrossRef] [Green Version]
- Koshy, T.; Misra, S.; Chatterjee, N.; Dharan, B.S. Accuracy of a Chest X-Ray-Based Method for Predicting the Depth of Insertion of Endotracheal Tubes in Pediatric Patients Undergoing Cardiac Surgery. J. Cardiothorac. Vasc. Anesth. 2016, 30, 947–953. [Google Scholar] [CrossRef] [PubMed]
- Lee, S.U.; Jung, J.Y.; Kim, D.K.; Kwak, Y.H.; Kwon, H.; Cho, J.H.; Park, J.W.; Choi, Y.J. New decision formulas for predicting endotracheal tube depth in children: Analysis of neck CT images. Emerg. Med. J. 2018, 35, 303–308. [Google Scholar] [CrossRef]
- Phipps, L.M.; Thomas, N.J.; Gilmore, R.K.; Raymond, J.A.; Bittner, T.R.; Orr, R.A.; Robertson, C.L. Prospective assessment of guidelines for determining appropriate depth of endotracheal tube placement in children. Pediatr. Crit. Care Med. 2005, 6, 519–522. [Google Scholar] [CrossRef]
- Lau, N.; Playfor, S.D.; Rashid, A.; Dhanarass, M. New formulae for predicting tracheal tube length. Paediatr. Anaesth. 2006, 16, 1238–1243. [Google Scholar] [CrossRef] [PubMed]
- Weiss, M.; Gerber, A.C.; Dullenkopf, A. Appropriate placement of intubation depth marks in a new cuffed paediatric tracheal tube. Br. J. Anaesth. 2005, 94, 80–87. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Elonheimo, L.; Ljungqvist, H.; Harve-Rytsälä, H.; Jäntti, H.; Nurmi, J. Frequency, indications and success of out-of-hospital intubations in Finnish children. Acta Anaesthesiol. Scand. 2021, 66, 125–131. [Google Scholar] [CrossRef] [PubMed]
- Oude Alink, M.B.; Moors, X.R.J.; Karrar, S.; Houmes, R.J.; Hartog, D.D.; Stolker, R.J. Characteristics, management and outcome of prehospital pediatric emergencies by a Dutch HEMS. Eur. J. Trauma Emerg. Surg. 2021. [Google Scholar] [CrossRef]
- Brown, J.B.; Leeper, C.M.; Sperry, J.L.; Peitzman, A.B.; Billiar, T.R.; Gaines, B.A.; Gestring, M.L. Helicopters and injured kids: Improved survival with scene air medical transport in the pediatric trauma population. J. Trauma Acute Care Surg. 2016, 80, 702–710. [Google Scholar] [CrossRef] [Green Version]
- Renberg, M.; Hertzberg, D.; Kornhall, D.; Günther, M.; Gellerfors, M. Pediatric Prehospital Advanced Airway Management by Anesthesiologist and Nurse Anesthetist Staffed Critical Care Teams. Prehosp. Disaster Med. 2021, 36, 547–552. [Google Scholar] [CrossRef]
- Duffens, A.; Grigorian, A.; de Virgilio, C.; Chin, T.; Kim, D.; Lekawa, M.; Schubl, S.D.; Nahmias, J. Association of Risk of Mortality in Pediatric Patients Transferred from Scene by Helicopter with Major but Not Minor Injuries. Pediatr. Emerg. Care 2020, 38, e287–e291. [Google Scholar] [CrossRef] [PubMed]
- Enomoto, Y.; Tsuchiya, A.; Tsutsumi, Y.; Ishigami, K.; Osone, J.; Togo, M.; Yasuda, S.; Inoue, Y. Association between physician-staffed helicopter versus ground emergency medical services and mortality for pediatric trauma patients: A retrospective nationwide cohort study. PLoS ONE 2020, 15, e0237192. [Google Scholar] [CrossRef] [PubMed]
- Ramsingh, D.; Ghazal, E.; Gordon, B.; Ross, P.; Goltiao, D.; Alschuler, M.; Pugh, J.; Holsclaw, M.; Mason, L. Relationship Between Evaluations of Tracheal Tube Position Using Ultrasound and Fluoroscopy in an Infant and Pediatric Population. J. Clin. Med. 2020, 9, 1707. [Google Scholar] [CrossRef]
- Van de Voorde, P.; Turner, N.M.; Djakow, J.; de Lucas, N.; Martinez-Mejias, A.; Biarent, D.; Bingham, R.; Brissaud, O.; Hoffmann, F.; Johannesdottir, G.B.; et al. European Resuscitation Council Guidelines 2021: Paediatric Life Support. Resuscitation 2021, 161, 327–387. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Overall | Tracheal Tube Position Correct | Tracheal Tube Misplacement | p | |
|---|---|---|---|---|
| n (%) | 65 (100) | 48 (73.8) | 17 (26.2) | |
| Age (years) | 14.0 (8.5) | 16 (4) | 9 (7.5) | <0.001 |
| Male, n (%) | 40 (62) | 31 (65) | 9 (53) | 0.404 |
| Height (cm) | 165 (48) | 170 (22) | 127 (42) | <0.001 |
| Weight (kg) | 51.2 (25.1) | 59.2 (23.5) | 28.7 (13.1) | <0.001 |
| BMI | 20.4 (4.7) | 21.5 (4.8) | 17.7 (2) | <0.001 |
| GCS | 8 (8) | 8 (10.5) | 4 (7) | 0.317 |
| SBP (mmHg) | 100 (85.5) | 100 (78.5) | 90 (110) | 0.208 |
| HR (min−1) | 100 (37.5) | 102.5 (44.5) | 98 (77) | 0.153 |
| SpO2 (%) | 95 (18) | 93 (17.3) | 97 (52) | 0.116 |
| ISS | 29 (21) | 26 (19.5) | 29 (27) | 0.373 |
| RTA, n (%) | 40 (61.5) | 30 (62.5) | 10 (58.8) | 0.781 |
| Fall from height, n (%) | 15 (23.1) | 11 (22.9) | 4 (23.5) | 1 |
| Other cause n (%) | 10 (15.4) | 7 (14.6) | 3 (17.6) | 0.713 |
| Helicopter EMS ETI, n (%) | 30 (46.2) | 26 (54.2) | 4 (23.5) | 0.046 |
| Ground EMS ETI, n (%) | 29 (44.6) | 18 (37.5) | 11 (64.7) | 0.087 |
| ED ETI, n (%) | 6 (9.2) | 4 (8.3) | 2 (11.8) | 0.648 |
| CPR prior ED, n (%) | 19 (29) | 13 (27) | 6 (35) | 0.546 |
| WBCT, n (%) | 43 (66.2) | 33 (68.8) | 10 (58.8) | 0.554 |
| CCT only | 10 (15.3) | 6 (12.5) | 4 (23.5) | 0.434 |
| No CT | 12 (18.5) | 8 (16.7) | 4 (23.5) | 0.713 |
| Emergency surgery, n (%) | 46 (70.8) | 37 (66.7) | 9 (52.9) | 0.071 |
| Ventilator (days) | 1.0 (5) | 1.0 (5) | 1 (6) | 0.596 |
| PICU (days) | 5.0 (11.5) | 5.0 (11.5) | 6 (12) | 0.611 |
| 24 h mortality, n (%) | 8 (12.3) | 5 (10.4) | 3 (17.6) | 0.421 |
| 30-day mortality, n (%) | 18 (27.7) | 12 (25.0) | 6 (35.3) | 0.529 |
| Predictor | Univariable OR (95% CI) | p |
|---|---|---|
| Age | 0.81 (0.71–0.90) | <0.001 |
| Height | 0.96 (0.94–0.98) | <0.001 |
| Weight | 0.94 (0.90–0.97) | <0.001 |
| BMI | 0.75 (0.61–0.89) | 0.003 |
| Helicopter EMS ETI | 0.26 (0.06–0.85) | 0.035 |
| Predictor | Multivariable OR (95% CI) | p |
|---|---|---|
| Weight | 0.86 (0.76–0.99) | 0.032 |
| Helicopter EMS ETI | 0.20 (0.04–0.97) | 0.036 |
| Helicopter EMS ETI | Ground EMS ETI | p | |
|---|---|---|---|
| n (%) | 30 (56.2) | 29 (44.6) | |
| Age (years) | 14.5 (6) | 16 (8) | 0.681 |
| Male, n (%) | 19 (63.3) | 19 (65.5) | 1 |
| Height (cm) | 155.7 (27.2) | 152.8 (31.3) | 0.968 |
| Weight (kg) | 52.6 (21.8) | 54.6 (27.7) | 0.652 |
| BMI | 20 (5) | 21 (8) | 0.575 |
| GCS | 8 (11) | 5 (7) | 0.043 |
| ISS | 25 (18) | 34 (20) | 0.034 |
| SBP (mmHg) | 111 (52) | 80 (110) | 0.003 |
| HR (min−1) | 108.5 (35) | 98 (59) | 0.067 |
| SpO2 (%) | 94.5 (10) | 94 (77) | 0.435 |
| ETI misplacement, n (%) | 4 (13.3) | 11 (37.9) | 0.039 |
| CPR prior ED, n (%) | 6 (20) | 11 (37.9) | 0.158 |
| 24 h mortality, n (%) | 2 (6.7) | 5 (17.2) | 0.254 |
| 30-day mortality, n (%) | 5 (16.7) | 12 (41.4) | 0.047 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rost, F.; Donaubauer, B.; Kirsten, H.; Schwarz, T.; Zimmermann, P.; Siekmeyer, M.; Gräfe, D.; Ebel, S.; Kleber, C.; Lacher, M.; et al. Tracheal Tube Misplacement after Emergency Intubation in Pediatric Trauma Patients: A Retrospective, Exploratory Study. Children 2022, 9, 289. https://doi.org/10.3390/children9020289
Rost F, Donaubauer B, Kirsten H, Schwarz T, Zimmermann P, Siekmeyer M, Gräfe D, Ebel S, Kleber C, Lacher M, et al. Tracheal Tube Misplacement after Emergency Intubation in Pediatric Trauma Patients: A Retrospective, Exploratory Study. Children. 2022; 9(2):289. https://doi.org/10.3390/children9020289
Chicago/Turabian StyleRost, Franziska, Bernd Donaubauer, Holger Kirsten, Thomas Schwarz, Peter Zimmermann, Manuela Siekmeyer, Daniel Gräfe, Sebastian Ebel, Christian Kleber, Martin Lacher, and et al. 2022. "Tracheal Tube Misplacement after Emergency Intubation in Pediatric Trauma Patients: A Retrospective, Exploratory Study" Children 9, no. 2: 289. https://doi.org/10.3390/children9020289
APA StyleRost, F., Donaubauer, B., Kirsten, H., Schwarz, T., Zimmermann, P., Siekmeyer, M., Gräfe, D., Ebel, S., Kleber, C., Lacher, M., & Struck, M. F. (2022). Tracheal Tube Misplacement after Emergency Intubation in Pediatric Trauma Patients: A Retrospective, Exploratory Study. Children, 9(2), 289. https://doi.org/10.3390/children9020289