
School Readiness in 4-Year-Old Very Preterm Children

 , , , ,
, , , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Sample
2.2. Procedures and Measures
2.3. Analysis
3. Results
3.1. Group Differences in Continuous Measures of Readiness
3.2. Group Differences in Rates of Deficits
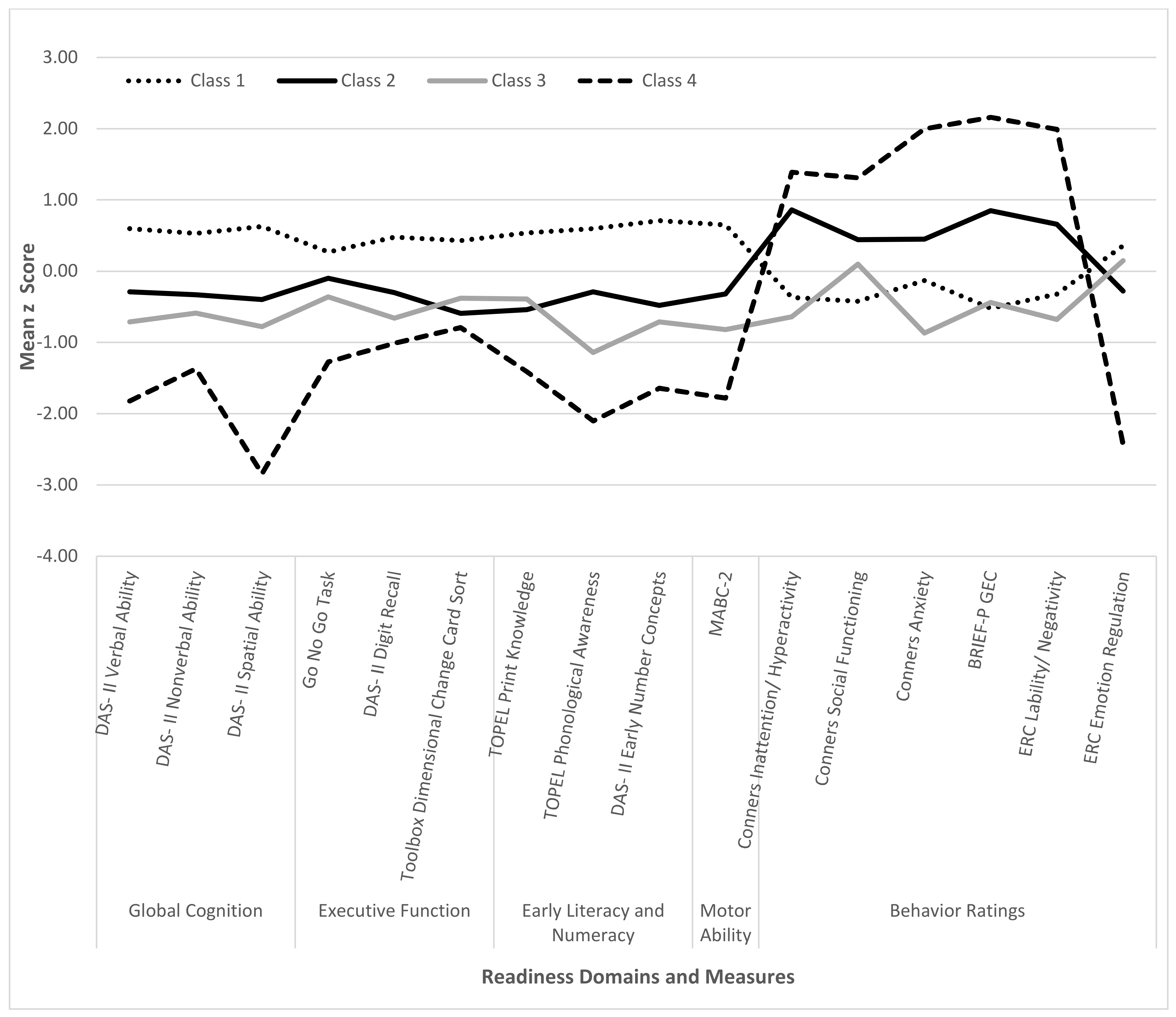
3.3. Readiness Profiles
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Johnson, S.; Wolke, D.; Hennessy, E.; Marlow, N. Educational Outcomes in Extremely Preterm Children: Neuropsychological Correlates and Predictors of Attainment. Dev. Neuropsychol. 2011, 36, 74–95. [Google Scholar] [CrossRef] [PubMed]
- Pritchard, V.E.; Clark, C.A.; Liberty, K.; Champion, P.R.; Wilson, K.; Woodward, L.J. Early school-based learning difficulties in children born very preterm. Early Hum. Dev. 2009, 85, 215–224. [Google Scholar] [CrossRef] [PubMed]
- Aylward, G.P. Neurodevelopmental outcomes of infants born prematurely. J. Dev. Behav. Pediatr. 2014, 35, 394–407. [Google Scholar] [CrossRef] [PubMed]
- Pritchard, V.E.; Bora, S.; Austin, N.C.; Levin, K.J.; Woodward, L.J. Identifying very preterm children at educational risk using a school readiness framework. Pediatrics 2014, 134, e825–e832. [Google Scholar] [CrossRef] [Green Version]
- Shah, P.E.; Kaciroti, N.; Richards, B.; Lumeng, J.C. Gestational age and kindergarten school readiness in a national sample of preterm infants. J. Pediatr. 2016, 178, 61–67. [Google Scholar] [CrossRef] [Green Version]
- Taylor, H.G.; Klein, N.; Anselmo, M.G.; Minich, N.; Espy, K.A.; Hack, M. Learning problems in kindergarten students with extremely preterm birth. Arch. Pediatr. Adolesc. Med. 2011, 165, 819–825. [Google Scholar] [CrossRef] [Green Version]
- High, P.C.; The Pediatrics Committee on Early Childhood, Adoption and Dependent Care and Council on School Health. School readiness. Pediatrics 2008, 121, e1008–e1015. [Google Scholar] [CrossRef] [Green Version]
- Williams, P.G.; Lerner, M.A.; Council On Early Childhood; Council On School Health; Sells, J.; Alderman, S.L.; Hashikawa, A.; Mendelsohn, M.A.; Mc Fadden, T.; Navsaria, D.; et al. School readiness. Pediatrics 2019, 144, e20191766. [Google Scholar] [CrossRef] [Green Version]
- Pan, Q.; Trang, K.T.; Love, H.R.; Templin, J. School readiness profiles and growth in academic achievement. Front. Educ. 2019, 4, 127. [Google Scholar] [CrossRef]
- Roberts, G.; Lim, J.; Doyle, L.W.; Anderson, P.J. High rates of school readiness difficulties at 5 years of age in very preterm infants compared with term controls. J. Dev. Behav. Pediatr. 2011, 32, 117–124. [Google Scholar] [CrossRef]
- Baron, I.S.; Erickson, K.; Ahronovich, M.D.; Baker, R.; Litman, F.R. Neuropsychological and behavioral outcomes of extremely low birth weight at age three. Dev. Neuropsychol. 2011, 36, 5–21. [Google Scholar] [CrossRef]
- Baron, I.S.; Kerns, K.A.; Muller, U.; Ahronovich, M.D.; Litman, F.R. Executive functions in extremely low birth weight and late-preterm preschoolers: Effects on working memory and response inhibition. Child Neuropsychol. 2012, 18, 586–599. [Google Scholar] [CrossRef]
- Blair, C.; Raver, C.C. School readiness and self-regulation: A developmental psychobiological approach. Annu. Rev. Psychol. 2015, 66, 711–731. [Google Scholar] [CrossRef] [Green Version]
- Clark, C.A.C.; Pritchard, V.E.; Woodward, L.J. Preschool executive functioning abilities predict early mathematics achievement. Dev. Psychol. 2010, 46, 1176–1191. [Google Scholar] [CrossRef]
- Foster-Cohen, S.H.; Friesen, M.D.; Champion, P.R.; Woodward, L.J. High prevalence/low severity language delay in preschool children born very preterm. J. Dev. Behav. Pediatr. 2010, 31, 658–667. [Google Scholar] [CrossRef]
- Hasler, H.M.; Akshoomoff, N. Mathematics ability and related skills in preschoolers born very preterm. Child Neuropsychol. 2019, 25, 162–178. [Google Scholar] [CrossRef]
- Jones, K.M.; Champion, P.R.; Woodward, L.J. Social competence of preschool children born very preterm. Early Hum. Dev. 2013, 89, 795–802. [Google Scholar] [CrossRef] [Green Version]
- Taylor, H.G.; Klein, N.; Espy, K.A.; Schluchter, M.; Minich, N.; Stilp, R.; Hack, M. Effects of extreme prematurity and kindergarten neuropsychological skills on early academic progress. Neuropsychology 2018, 32, 809–821. [Google Scholar] [CrossRef]
- Woodward, L.J.; Lu, Z.; Morris, A.; Healey, D. Self regulatory skills during early childhood are associated with later mental health and educational achievement in very preterm and typically developing children. Clin. Neuropsychol. 2017, 31, 404–422. [Google Scholar] [CrossRef]
- Anderson, P.J. Neuropsychological outcomes of children born very preterm. Semin. Fetal Neonatal Med. 2014, 19, 90–96. [Google Scholar] [CrossRef]
- Anderson, P.J.; Doyle, L.W. Cognitive and educational deficits in children born extremely preterm. Semin. Perinatol. 2008, 32, 51–58. [Google Scholar] [CrossRef] [PubMed]
- Woodward, L.J.; Moor, S.; Hood, K.M.; Champion, P.R.; Foster-Cohen, S.; Inder, T.E.; Austin, N.C. Very preterm children show impairments across multiple neurodevelopmental domains by age 4 years. Arch. Dis. Child Fetal Neonatal Ed. 2009, 94, F339–F344. [Google Scholar] [CrossRef]
- Hair, E.; Halle, T.; Terry-Humen, E.; Lavelle, B.; Calkins, J. Children’s school readiness in the ECLS-K: Predictions to academic, health, and social outcomes in first grade. Early Child. Res. Q. 2006, 21, 431–454. [Google Scholar] [CrossRef]
- Konold, T.R.; Pianta, R.C. Empirically-derived, person-oriented patterns of school readiness in typically-developing children: Description and prediction to first-grade achievement. Appl. Dev. Sci. 2005, 9, 174–187. [Google Scholar] [CrossRef]
- Burnett, A.C.; Youssef, G.; Anderson, P.J.; Duff, J.; Doyle, L.W.; Cheong, J.L.Y.; Victorian Infant Collaborative Study Group. Exploring the “preterm behavioral phenotype” in children born extremely preterm. J. Dev. Behav. Pediatr. 2019, 40, 200–207. [Google Scholar] [CrossRef]
- Twilhaar, E.S.; Pierrat, V.; Marchand-Martin, L.; Benhammou, V.; Kaminski, M.; Ancel, P.Y. Profiles of functioning in 5.5-year-old very preterm born children in france: The EPIPAGE-2 study. J. Am. Acad. Child Adolesc. Psychiatry 2021. [Google Scholar] [CrossRef]
- Lean, R.E.; Lessov-Shlaggar, C.N.; Gerstein, E.D.; Smyser, T.A.; Paul, R.A.; Smyser, C.D.; Rogers, C.E. Maternal and family factors differentiate profiles of psychiatric impairments in very preterm children at age 5-years. J. Child Psychol. Psychiatry 2020, 61, 157–166. [Google Scholar] [CrossRef]
- Alduncin, N.; Huffman, L.C.; Feldman, H.M.; Loe, I.M. Executive function is associated with social competence in preschool-aged children born preterm or full term. Early Hum. Dev. 2014, 90, 299–306. [Google Scholar] [CrossRef] [Green Version]
- Delobel-Ayoub, M.; Arnaud, C.; White-Koning, M.; Casper, C.; Pierrat, V.; Garel, M.; Burguet, A.; Roze, J.C.; Matis, J.; Picaud, J.C.; et al. Behavioral problems and cognitive performance at 5 years of age after very preterm birth: The EPIPAGE Study. Pediatrics 2009, 123, 1485–1492. [Google Scholar] [CrossRef]
- Witt, A.; Theurel, A.; Tolsa, C.B.; Lejeune, F.; Fernandes, L.; de Jonge, L.; Monnier, M.; Bickle Graz, M.; Barisnikov, K.; Gentaz, E.; et al. Emotional and effortful control abilities in 42-month-old very preterm and full-term children. Early Hum. Dev. 2014, 90, 565–569. [Google Scholar] [CrossRef]
- De Silva, A.; Neel, M.L.; Maitre, N.; Busch, T.; Taylor, H.G. Resilience and vulnerability in very preterm 4-year-olds. Clin. Neuropsychol. 2021, 35, 904–924. [Google Scholar] [CrossRef]
- Neel, M.L.; de Silva, A.; Taylor, H.G.; Benninger, K.; Busch, T.; Hone, E.; Moore-Clingenpeel, M.; Pietruszewski, L.; Maitre, N.L. Exceeding expectations after perinatal risks for poor development: Associations in term- and preterm-born preschoolers. J. Perinatol. 2021. [Google Scholar] [CrossRef]
- Orchinik, L.J.; Taylor, H.G.; Espy, K.A.; Minich, N.; Klein, N.; Sheffield, T.; Hack, M. Cognitive outcomes for extremely preterm/extremely low birth weight children in kindergarten. J. Int. Neuropsychol. Soc. 2011, 17, 1067–1079. [Google Scholar] [CrossRef] [Green Version]
- Mohammad, K.; Scott, J.N.; Leijser, L.M.; Zein, H.; Afifi, J.; Piedboeuf, B.; de Vries, L.S.; van Wezel-Meijler, G.; Lee, S.K.; Shah, P.S. Consensus Approach for Standardizing the Screening and Classification of Preterm Brain Injury Diagnosed with Cranial Ultrasound: A Canadian Perspective. Front. Pediatr. 2021, 9, 618236. [Google Scholar] [CrossRef]
- Papile, L.A.; Burstein, J.; Burstein, R.; Koffler, H. Incidence and evolution of subependymal and intraventricular hemorrhage: A study of infants with birth weights less than 1500 gm. J. Pediatr. 1978, 92, 529–534. [Google Scholar] [CrossRef]
- Conners, C.K. Conners Early Childhood.; Multi-Health Systems, Inc.: Toronto, ON, Canada, 2009. [Google Scholar]
- Johnson, S.; Marlow, N. Preterm birth and childhood psychiatric disorders. Pediatr. Res. 2011, 69, 11R–18R. [Google Scholar] [CrossRef]
- Lamm, C.; Walker, O.L.; Degnan, K.A.; Henderson, H.A.; Pine, D.S.; McDermott, J.M.; Fox, N.A. Cognitive control moderates early childhood temperament in predicting social behavior in 7-year-old children: An ERP study. Dev. Sci. 2012, 17, 667–681. [Google Scholar] [CrossRef]
- Shields, A.; Cicchetti, D. Emotion regulation among school-age children: The development and validation of a new criterion Q-sort scale. Dev. Psychol. 1997, 33, 906–916. [Google Scholar] [CrossRef]
- Griffiths, A.; Morgan, P.; Anderson, P.J.; Doyle, L.W.; Lee, K.J.; Spittle, A.J. Predictive value of the movement assessment battery for children—Second Edition at 4 years, for motor impairment at 8 years in children born preterm. Dev. Med. Child Neurol. 2017, 59, 490–496. [Google Scholar] [CrossRef] [Green Version]
- Taylor, H.G.; Minich, N.; Schluchter, M.; Espy, K.A.; Klein, N. Resilience in Extremely preterm/extremely low birth weight kindergarten children. J. Int. Neuropsychol. Soc. 2019, 25, 362–374. [Google Scholar] [CrossRef]
- Wiley, C.P.; Wedeking, T.; Galindo, A.M. Test review: C.K. Test Review: CK Conners. Conners early childhood manual. J. Psychoeduc. Assess. 2013, 31, 606–610. [Google Scholar] [CrossRef]
- Zelazo, P.D.; Muller, U.; Frye, D.; Marcovitch, S.; Argitis, G.; Boseovski, J.; Chiang, J.K.; Hongwanishkul, D.; Schuster, B.V.; Sutherland, A. The development of executive function in early childhood. Monogr. Soc. Res. Child Dev. 2003, 68, vii-137. [Google Scholar] [CrossRef] [PubMed]
- Elliot, C.D. Differential Ability Scales, 2nd ed.; Harcourt Assessment: San Antonio, TX, USA, 2007. [Google Scholar]
- Casaletto, K.B.; Umlauf, A.; Beaumont, J.; Gershon, R.; Slotkin, J.; Akshoomoff, N.; Heaton, R.K. Demographically corrected normative standards for the English version of the NIH Toolbox Cognition Battery. J. Int. Neuropsychol. Soc. 2015, 21, 378–391. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wagner, R.; Torgensen, J.; Rashotte, C.; Pearson, N. Comprehensive Test of Phonological Processing, 2nd ed.; PRO-ED: Austin, TX, USA, 2013. [Google Scholar]
- Henderson, S.E.; Sugden, D.A.; Barnett, A. Movement Assessment Battery for Children (Movement ABC-2): Examiner’s Manual, 2nd ed.; Harcourt Assessment: London, UK, 2007. [Google Scholar]
- Lonigan, C.J.; Wagner, R.K.; Torgensen, J.K.; Rashotte, C.A. TOPEL: Test of Preschool Early Literacy; Pro-Ed: Austin, TX, USA, 2007. [Google Scholar]
- Wilson, S.B.; Lonigan, C.J. An evaluation of two emergent literacy screening tools for preschool children. Ann. Dyslexia 2009, 59, 115–131. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gioia, G.A.; Espy, K.A.; Esquith, P.K. BRIEF-P: Behavior Rating Inventory of Executive Function—Preschool Version; Psychological Assessment Resources: Lutz, FL, USA, 2003. [Google Scholar]
- Cohen, J. A power primer. Psychol. Bull. 1992, 112, 155–159. [Google Scholar] [CrossRef]
- Pitchford, N.; Johnson, S.; Scerif, G.; Marlow, N. Early indications of delayed cognitive development in preschool children born very preterm: Evidence from domain-general and domain-specific tasks. Infant Child Dev. 2011, 20, 400–422. [Google Scholar] [CrossRef]
- Baron, I.S.; Brandt, J.; Ahronovich, M.D.; Baker, R.; Erickson, K.; Litman, F.R. Selective deficit in spatial location memory in extremely low birth weight children at age six: The PETIT study. Child Neuropsychol. 2012, 18, 299–311. [Google Scholar] [CrossRef]
- Larson, J.C.G.; Barson, I.S.; Erickson, K.; Ahronovich, M.D.; Baker, R.; Litman, F.R. Neuromotor outcomes at school age after extremely low birth weight: Early detection of subtle signs. Neuropsychology 2011, 25, 66–75. [Google Scholar] [CrossRef]
- Scott, M.N.; Taylor, H.G.; Fristad, M.A.; Klein, N.; Espy, K.A.; Minich, N.; Hack, M. Behavior disorders in extremely preterm/extremely low birth weight children in kindergarten. J. Dev. Behav. Pediatr. 2012, 33, 202–213. [Google Scholar] [CrossRef] [Green Version]
- Taylor, H.G. Neurodevelopmental origins of social competence in very preterm children. Semin. Fetal Neonatal. Med. 2020, 25, 101108. [Google Scholar] [CrossRef]
- Taylor, H.G.; Clark, C.A.C. Executive function in children born preterm: Risk factors and implications for outcome. Semin. Perinatol. 2016, 40, 520–529. [Google Scholar] [CrossRef] [Green Version]
- O’Driscoll, D.N.; McGovern, M.; Greene, C.M.; Molloy, E.J. Gender disparities in preterm neonatal outcomes. Acta Paediatr. 2018, 107, 1494–1499. [Google Scholar] [CrossRef] [Green Version]
- Underwood, M.K.; Galen, B.R.; Paquette, J.A. Top ten challenges for understanding gender and aggression in children: Why can’t we all just get along? Soc. Dev. 2001, 10, 248–266. [Google Scholar] [CrossRef]
- Najman, J.M.; Williams, G.M.; Nikles, J.; Spence, S.; Bor, W.; O’Callaghan, M.; Le Brocque, R.; Andersen, M.J.; Shuttlewood, G.J. Bias influencing maternal reports of child behaviour and emotional state. Soc. Psychiatry Psychiatr. Epidemiol. 2001, 36, 186–194. [Google Scholar] [CrossRef]
- Jaekel, J.; Pluess, M.; Belsky, J.; Wolke, D. Effects of maternal sensitivity on low birth weight children’s academic achievement: A test of differential susceptibility versus diathesis stress. J. Child Psychol. Psychiatry 2015, 56, 693–701. [Google Scholar] [CrossRef]
- Spittle, A.J.; Treyvaud, K.; Lee, K.J.; Anderson, P.J.; Doyle, L.W. The role of social risk in an early preventative care programme for infants born very preterm: A randomized controlled trial. Dev. Med. Child Neurol. 2018, 60, 54–62. [Google Scholar] [CrossRef]
- Benavente-Fernandez, I.; Synnes, A.; Grunau, R.E.; Chau, V.; Ramraj, C.; Glass, T.; Cayam-Rand, D.; Siddiqi, A.; Miller, S.P. Association of socioeconomic status and brain injury with neurodevelopmental outcomes of very preterm children. JAMA Netw. Open 2019, 2, e192914. [Google Scholar] [CrossRef]
- Duncan, A.F.; Bann, C.M.; Maitre, N.L.; Peralta-Carcelen, M.; Hintz, S.R.; Eunice Kennedy Shriver National Institute of Child Health; Development Neonatal Research Network. Hand function at 18–22 months is associated with school-age manual dexterity and motor performance in children born extremely preterm. J. Pediatr. 2020, 225, 51–57. [Google Scholar] [CrossRef]
- Johnson, S.; Waheed, G.; Manktelow, B.N.; Field, D.J.; Marlow, N.; Draper, E.S.; Boyle, E.M. Differentiating the preterm phenotype: Distinct profiles of cognitive and behavioral development following late and moderately preterm birth. J. Pediatr. 2018, 193, 85–92. [Google Scholar] [CrossRef] [Green Version]
- Weller, B.E.; Bowen, N.K.; Faubert, S.J. Latent class analysis: A guide to best practice. J. Black Psychol. 2020, 46, 287–311. [Google Scholar] [CrossRef]
- Wurpts, I.C.; Geiser, C. Is adding more indicators to a latent class analysis beneficial or detrimental? Results of a monte-carlo study. Front. Psychol. 2014, 5, 920. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chung, P.J.; Opipari, V.P.; Koolwijk, I. Executive function and extremely preterm children. Pediatr. Res. 2017, 82, 565–566. [Google Scholar] [CrossRef] [PubMed]
- Chen, J.H.; Claessens, A.; Msall, M.E. Prematurity and school readiness in a nationally representative sample of Australian children: Does typically occurring preschool moderate the relationship? Early Hum. Dev. 2014, 90, 73–79. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Doyle, L.W.; Cheong, J.L.; Burnett, A.; Roberts, G.; Lee, K.J.; Anderson, P.J.; Victorian Infant Collaborative Study, G. Biological and social influences on outcomes of extreme-preterm/low-birth weight adolescents. Pediatrics 2015, 136, e1513–e1520. [Google Scholar] [CrossRef] [Green Version]

{kind=link}
| Characteristic | Group | |
|---|---|---|
| VPT (n = 53) | FT (n = 38) | |
| Neonatal and early developmental status: | ||
| Child age, mean (SD) | 4.7 (0.29) | 4.6 (0.29) |
| Gestational age, mean in weeks (SD, range) a,b | 27.3 (1.9, 23–30) | 39.1 (1.1, 37–41) |
| Birth weight in grams, mean (SD, range) a,b | 944 (270, 369–1644) | 3249 (435, 2325–4167) |
| Multiple birth c, n (%) | 10 (45) | 2 (11) |
| Medical complications | ||
| Grade III-IVH or PVHI d, n (%) | 6 (11.32) | - |
| Periventricular leukomalacia e, n (%) | 10 (18.9) | - |
| Bronchopulmonary dysplasia requiring home oxygen, n (%) | 16 (30.2) | - |
| Intrauterine growth restriction (IUGR), n (%) | 7 (13.2) | - |
| Culture-positive sepsis, n (%) | 14 (26.4) | - |
| Necrotizing enterocolitis (NEC) f, n (%) | 6 (11.3) | - |
| Retinopathy of prematurity (ROP) requiring laser surgery, n (%) | 4 (7.5) | - |
| Family demographic characteristics: | ||
| Child sex: male, n (%) | 27 (50.9) | 18 (47.4) |
| Child race: | ||
| White, n (%) | 35 (66) | 28 (73.7) |
| Black/African American, n (%) | 10 (18.9) | 3 (7.9) |
| Asian, n (%) | 1 (1.9) | 1 (2.6) |
| More than one race, n (%) | 7 (13.2) | 6 (15.8) |
| Child enrolled in preschool, n (%) | 46 (86.8) | 32 (84.2) |
| zSES Composite, mean (SD) a | −0.25 (0.73) | 0.35 (0.59) |
| Domain/Measure | Reference | Description | Score |
|---|---|---|---|
| Global cognitive ability (DAS-II): | [44] | Standard Scores | |
| DAS-II General Conceptual Ability | Global ability composite | ||
| DAS-II Verbal Ability | Verbal comprehension and naming | ||
| DAS-II Nonverbal Ability | Nonverbal reasoning | ||
| DAS-II Spatial Ability | Perceptual motor skills | ||
| Executive function and processing speed: | |||
| NIH Toolbox Dimensional Change Card Sort | [45] | Cognitive ability/rule shifting | T-score a |
| DAS-II Recall of Digits—Forward | [44] | Verbal working memory | T-score |
| Zoo Game Go No Go Task b | [38] | Attention and inhibition | Proportion correct |
| CTOPP-2 Rapid Symbolic Naming c | [46] | Speed of naming | Standard score |
| Motor skills (MABC-2): | [47] | Scaled scores | |
| Total | Composite of motor skills | ||
| Manual Dexterity | Fine motor skills | ||
| Balance | Gross motor balance | ||
| Aiming and Catching | Eye–hand coordination | ||
| Early literacy and numeracy: | |||
| TOPEL Print Knowledge | [48,49] | Letter names and sounds | Standard score |
| TOPEL Phonological Awareness | Ability to identify phonemes | Standard score | |
| DAS-II Early Number Concepts | [44] | Counting and math problem solving | T-score |
| Behavior ratings: | |||
| Conners EC-P Total Problems, Inattention/Hyperactivity, Anxiety, Social Functioning | [36,42] | Symptoms of overall problems and in areas of attention, externalizing, and socialization | T-scores |
| BRIEF-P Global Executive Composite, Inhibitory Self-Control Index, Flexibility Index, Emergent Metacognition Index | [50] | Behavior symptoms of executive dysfunction | T-scores |
| ERC Lability/Negativity, Emotion Regulation | [39] | Symptoms of mood lability and ability to regulate emotions | Raw scores |
| VPT Group | FT Group | ||||
|---|---|---|---|---|---|
| School Readiness Measure | M (SE) | M (SE) | β | p | Cohen’s d |
| Global/cognitive ability (DAS-II): | |||||
| General Conceptual Ability | 92.17 (1.88) | 108.97 (2.08) | −16.80 | <0.001 | −1.29 |
| Verbal Ability | 97.17 (1.97) | 107.12 (2.21) | −9.95 | 0.002 | −0.72 |
| Nonverbal Ability | 95.63 (2.02) | 108.29 (2.22) | −12.66 | <0.001 | −0.92 |
| Spatial Ability | 90.08 (1.88) | 106.03 (2.05) | −15.95 | <0.001 | −1.23 |
| Executive function and processing speed: | |||||
| DCCS Age Corrected | 94.53 (2.15) | 100.05 (2.10) | −5.52 | 0.078 | −0.42 |
| DAS-II Recall of Digits-Forward | 43.94 (1.77) | 56.75 (1.98) | −12.81 | <0.001 | −1.22 |
| Go No Go | 0.62 (0.03) | 0.75 (0.03) | −0.13 | 0.003 | −0.70 |
| CTOPP−2 Rapid Symbolic Naming a | 96.15 (2.80) | 105.67 (2.77) | −16.68 | 0.031 | −0.57 |
| Motor skills (MABC−2): | |||||
| Total | 5.52 (0.42) | 8.91 (0.45) | −3.39 | <0.001 | −1.18 |
| Manual Dexterity | 4.90 (0.42) | 8.29 (0.47) | −3.40 | <0.001 | −1.16 |
| Balance | 6.92 (0.40) | 9.61 (0.46) | −2.69 | <0.001 | −0.96 |
| Aiming and Catching b | 8.59 (0.43) | 10.46 (0.51) | 1.93 | 0.043 | −0.79 |
| Early literacy and numeracy: | |||||
| TOPEL Print Knowledge | 96.80 (2.22) | 107.26 (2.39) | −10.46 | 0.003 | −0.69 |
| TOPEL Phonological Awareness | 92.37 (2.08) | 106.53 (2.31) | −14.16 | <0.001 | −1.00 |
| DAS-II Early Number Concepts | 45.29 (1.27) | 55.89 (1.49) | −10.60 | <0.001 | −1.31 |
| Behavior ratings: | |||||
| Conners EC-P Global Index Total | 56.23 (1.69) | 55.23 (1.88) | 1.00 | 0.702 | 0.09 |
| Conners EC-P Inattention/Hyperactivity | 55.81 (1.72) | 56.42 (1.97) | −0.61 | 0.822 | −0.05 |
| Conners EC-P Anxiety | 56.88 (1.74) | 55.46 (1.93) | 1.42 | 0.598 | 0.13 |
| Conners EC-P Social Functioning c | 53.73 (1.29) | 47.68 (1.48) | −12.61 | 0.001 | 0.64 |
| BRIEF-P GEC | 58.55 (1.66) | 51.31 (1.91) | 7.24 | 0.007 | 0.61 |
| BRIEF-P Inhibitory Self-Control Index | 56.60 (1.76) | 51.89 (2.00) | 4.71 | 0.092 | 0.38 |
| BRIEF-P Flexibility Index | 54.67 (1.53) | 50.04 (1.73) | 4.63 | 0.056 | 0.43 |
| BRIEF-P Emergent Metacognition Index | 60.18 (1.59) | 51.42 (1.91) | 8.77 | 0.001 | 0.76 |
| ERC Lability/Negativity | 27.74 (0.95) | 26.58 (1.10) | 1.15 | 0.447 | 0.17 |
| ERC Emotion Regulation d | 26.31 (0.40) | 28.39 (0.48) | 3.57 | 0.003 | −0.60 |
| VPT Group (n = 53) | FT Group (n = 38) | |||
|---|---|---|---|---|
| Area of Deficit | N (%) | N (%) | p | OR (95% CI) |
| Global/cognitive ability (DAS-II): | ||||
| General Conceptual Ability | 16 (31) | 0 (0) | 0.017 | 31.85 (1.85, 548.40) |
| Verbal Ability | 9 (18) | 0 (0) | 0.037 | 20.84 (1.21, 358.86) |
| Nonverbal Ability | 10 (20) | 1 (3) | 0.021 | 10.96 (1.43, 83.82) |
| Spatial Ability | 20 (42) | 1 (3) | 0.014 | 14.10 (1.73, 115.11) |
| Executive function and processing speed: | ||||
| DCCS Age Corrected | 11 (26) | 3 (8) | 0.040 | 5.00 (1.07, 23.29) |
| DAS-II Recall of Digits, Forward | 14 (28) | 1 (3) | 0.007 | 15.43 (2.09, 113.90) |
| Go No Go | 16 (37) | 2 (6) | 0.013 | 6.67 (1.49, 29.86) |
| CTOPP-2 Rapid Symbolic Naming | 6 (18) | 3 (9) | 0.654 | 1.39 (0.33, 5.91) |
| Motor skills (MABC-2): | ||||
| Total | 33 (62) | 6 (16) | <0.001 | 1.61 (1.31, 1.98) |
| Manual Dexterity | 39 (74) | 9 (24) | <0.001 | 1.58 (1.27, 1.97) |
| Balance | 18 (34) | 6 (16) | 0.050 | 1.22 (1.00, 1.48) |
| Aiming and Catching | 17 (32) | 2 (5) | 0.003 | 1.25 (1.08, 1.45) |
| Early literacy and numeracy: | ||||
| TOPEL Print Knowledge | 14 (28) | 1 (3) | 0.043 | 10.08 (1.08, 94.43) |
| TOPEL Phonological Awareness | 13 (26) | 0 (0) | 0.031 | 22.87 (1.33, 394.68) |
| DAS-II Early Number Concepts | 12 (24) | 0 (0) | 0.039 | 20.00 (1.17, 342.69) |
| Behavior problems: | ||||
| Conners EC-P Global Index Total | 16 (30) | 8 (21) | 0.888 | 0.92 (0.28, 3.04) |
| Conners EC-P Inattention/Hyperactivity | 20 (38) | 10 (26) | 0.666 | 1.25 (0.46, 3.38) |
| Conners EC-P Anxiety | 19 (36) | 9 (24) | 0.442 | 1.53 (0.52, 4.47) |
| Conners EC-P Social Functioning | 17 (32) | 1 (3) | 0.033 | 14.77 (1.24, 176.29) |
| BRIEF-P GEC | 28 (53) | 4 (11) | 0.001 | 6.90 (2.10, 22.72) |
| BRIEF-P Inhibitory Self-Control Index | 25 (47) | 6 (16) | 0.039 | 3.34 (1.07, 10.48) |
| BRIEF-P Flexibility Index | 18 (34) | 4 (11) | 0.146 | 2.63 (0.71, 9.69) |
| BRIEF-P Emergent Metacognition Index | 30 (57) | 3 (8) | <0.001 | 12.81 (3.70, 44.33) |
| ERC Lability/Negativity | 12 (23) | 5 (13) | 0.577 | 1.45 (0.39, 5.42) |
| ERC Emotion Regulation | 13 (25) | 1 (3) | 0.002 | 1.22 (1.08, 1.39) |
| Multiple Deficits: | 44 (83) | 12 (32) | 0.001 | 1.42 (1.15, 1.76) |
| Fit Statistics | Class 1 | Class 2 | Class 3 | Class 4 | Class 5 |
|---|---|---|---|---|---|
| AIC | 8224.109 | 7972.723 | 7890.293 | 7843.928 | 7807.723 |
| BIC | 8298.268 | 8086.28 | 8043.248 | 8036.28 | 8039.472 |
| SSA-BIC | 8197.413 | 7931.845 | 7835.233 | 7774.686 | 7724.298 |
| Entropy | - | 0.944 | 0.963 | 0.966 | 0.958 |
| LMR | - | 285.385 | 116.43 | 80.365 | 65.277 |
| p-value (LMR) | - | 0.01 | 0.27 | 0.57 | 0.77 |
| BLRT | - | 285.385 | 116.43 | 80.365 | 65.277 |
| p-value (BLRT) | - | <0.0001 | <0.0001 | <0.0001 | <0.0001 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Taylor, H.G.; Vrantsidis, D.M.; Neel, M.L.; Benkart, R.; Busch, T.A.; de Silva, A.; Udaipuria, S.; Maitre, N.L. School Readiness in 4-Year-Old Very Preterm Children. Children 2022, 9, 323. https://doi.org/10.3390/children9030323
Taylor HG, Vrantsidis DM, Neel ML, Benkart R, Busch TA, de Silva A, Udaipuria S, Maitre NL. School Readiness in 4-Year-Old Very Preterm Children. Children. 2022; 9(3):323. https://doi.org/10.3390/children9030323
Chicago/Turabian StyleTaylor, H. Gerry, Daphne M. Vrantsidis, Mary Lauren Neel, Rebekah Benkart, Tyler A. Busch, Aryanne de Silva, Shivika Udaipuria, and Nathalie L. Maitre. 2022. "School Readiness in 4-Year-Old Very Preterm Children" Children 9, no. 3: 323. https://doi.org/10.3390/children9030323