

Practices and Trends in the Prescription of Probiotics: A Detailed Analysis in an Eastern European Region




 ,
,  and
and 
Abstract
1. Introduction
2. Materials and Methods
2.1. Data Collection
2.2. Analysis
3. Results
3.1. Distribution of Probiotic Recommendations by Age and Gender
3.2. Diagnostics Associated with Probiotic Recommendation
3.3. Prescribed Probiotic Genera
3.4. Prescribed Probiotic Species
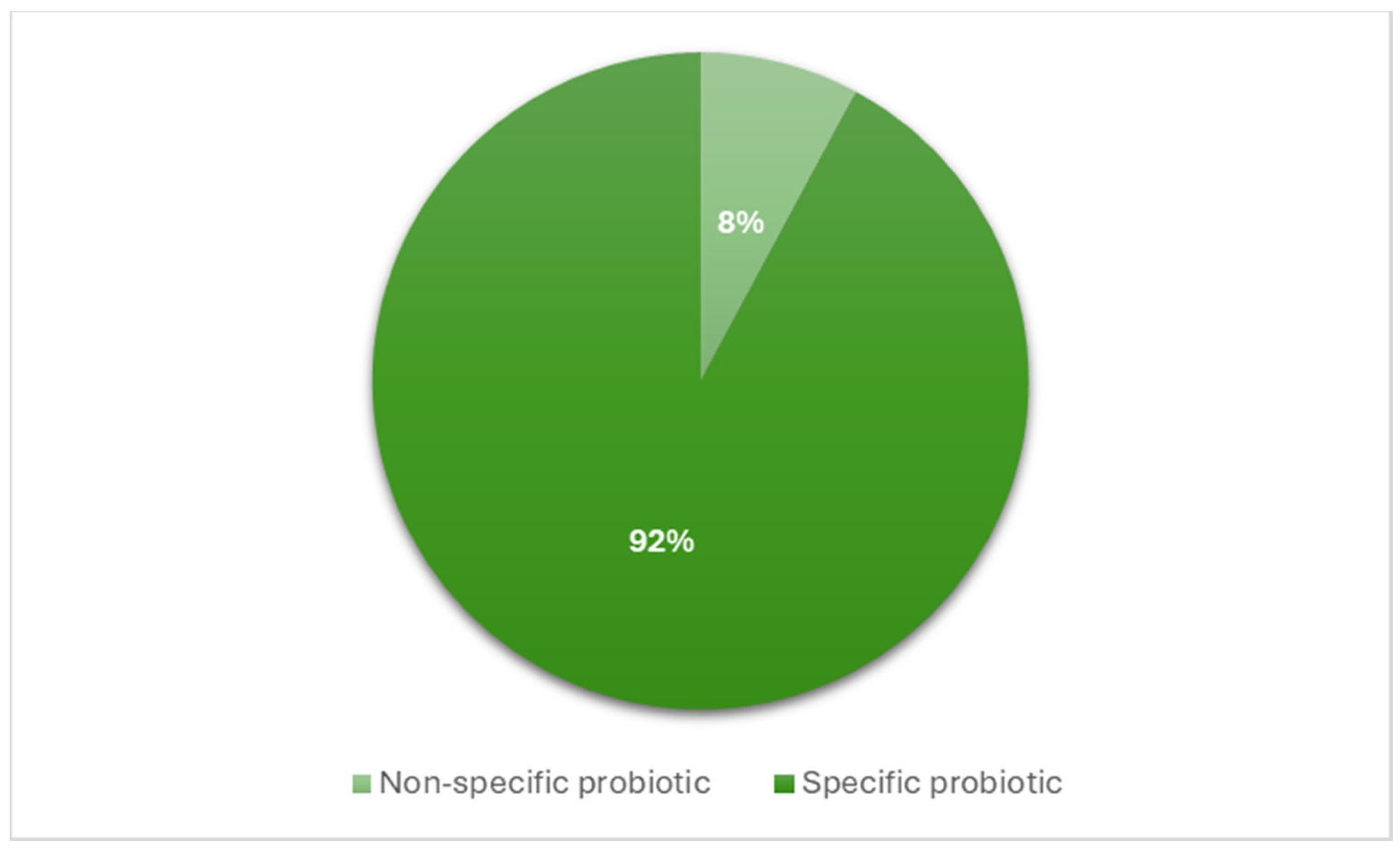
3.5. Physicians’ Approach Regarding the Importance of Probiotic Product Specificity
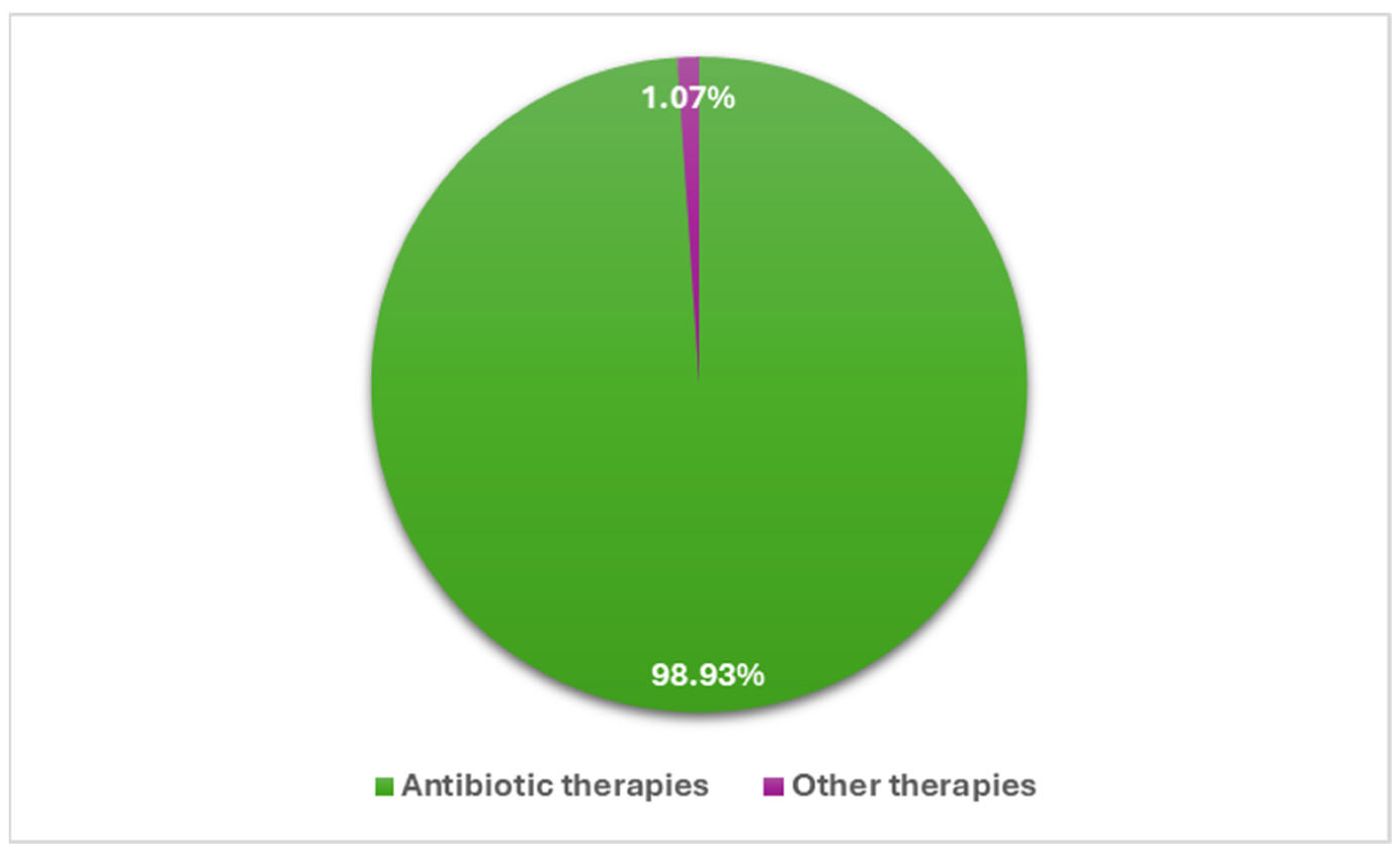
3.6. Analysis of Antibiotic–Probiotic Associations
3.7. Physicians’ Recommendations for Probiotic Genera Associated with Antibiotic Therapy
3.8. Physicians’ Recommendations for Probiotic Species Associated with Antibiotic Therapy
3.9. Diagnoses for Which Probiotics Are Associated with Antibiotics
3.10. Duration of Probiotic Treatment Versus Duration of Antibiotic Therapy
4. Discussions
Strengths and Weaknesses
5. Conclusions
Author Contributions
Funding
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Zavišić, G.; Popović, M.; Stojkov, S.; Medić, D.; Gusman, V.; Jovanović Lješković, N.; Jovanović Galović, A. Antibiotic Resistance and Probiotics: Knowledge Gaps, Market Overview and Preliminary Screening. Antibiotics 2023, 12, 1281. [Google Scholar] [CrossRef]
- Lynch, E.; Troob, J.; Lebwohl, B.; Freedberg, D.E. Who Uses Probiotics and Why? A Survey Study Conducted among General Gastroenterology Patients. BMJ Open Gastroenterol. 2021, 8, e000742. [Google Scholar] [CrossRef] [PubMed]
- European Probiotic Market Insights Update 2022. Available online: https://www.ipaeurope.org/wp-content/uploads/2023/10/202305-EU-MARKET-INSIGHTS-UPDATE-2022.pdf (accessed on 3 March 2024).
- van den Nieuwboer, M.; van de Burgwal, L.H.M.; Claassen, E. A Quantitative Key-Opinion-Leader Analysis of Innovation Barriers in Probiotic Research and Development: Valorisation and Improving the Tech Transfer Cycle. PharmaNutrition 2016, 4, 9–18. [Google Scholar] [CrossRef]
- Day, R.L.; Harper, A.J.; Woods, R.M.; Davies, O.G.; Heaney, L.M. Probiotics: Current Landscape and Future Horizons. Futur. Sci. OA 2019, 5, FSO391. [Google Scholar] [CrossRef] [PubMed]
- Sniffen, J.C.; McFarland, L.V.; Evans, C.T.; Goldstein, E.J.C. Choosing an Appropriate Probiotic Product for Your Patient: An Evidence-Based Practical Guide. PLoS ONE 2018, 13, e0209205. [Google Scholar] [CrossRef]
- World Gastroenterology Organisation Global Guidelines. Available online: https://www.worldgastroenterology.org/UserFiles/file/guidelines/probiotics-and-prebiotics-english-2023.pdf (accessed on 3 March 2024).
- Su, G.L.; Ko, C.W.; Bercik, P.; Falck-Ytter, Y.; Sultan, S.; Weizman, A.V.; Morgan, R.L. AGA Clinical Practice Guidelines on the Role of Probiotics in the Management of Gastrointestinal Disorders. Gastroenterology 2020, 159, 697–705. [Google Scholar] [CrossRef] [PubMed]
- Szajewska, H.; Canani, R.B.; Guarino, A.; Hojsak, I.; Indrio, F.; Kolacek, S.; Orel, R.; Shamir, R.; Vandenplas, Y.; van Goudoever, J.B.; et al. Probiotics for the Prevention of Antibiotic-Associated Diarrhea in Children. J. Pediatr. Gastroenterol. Nutr. 2016, 62, 495–506. [Google Scholar] [CrossRef]
- Draper, K.; Ley, C.; Parsonnet, J. Probiotic Guidelines and Physician Practice: A Cross-Sectional Survey and Overview of the Literature. Benef. Microbes 2017, 8, 507–519. [Google Scholar] [CrossRef]
- Martinez, R.C.R.; Bedani, R.; Saad, S.M.I. Scientific Evidence for Health Effects Attributed to the Consumption of Probiotics and Prebiotics: An Update for Current Perspectives and Future Challenges. Br. J. Nutr. 2015, 114, 1993–2015. [Google Scholar] [CrossRef]
- Ouwehand, A.C.; Invernici, M.M.; Furlaneto, F.A.C.; Messora, M.R. Effectiveness of Multi-Strain Versus Single-Strain Probiotics. J. Clin. Gastroenterol. 2018, 52, S35–S40. [Google Scholar] [CrossRef]
- McFarland, L.V. Efficacy of Single-Strain Probiotics Versus Multi-Strain Mixtures: Systematic Review of Strain and Disease Specificity. Dig. Dis. Sci. 2021, 66, 694–704. [Google Scholar] [CrossRef] [PubMed]
- Sharma, P.; Tomar, S.K.; Goswami, P.; Sangwan, V.; Singh, R. Antibiotic Resistance among Commercially Available Probiotics. Food Res. Int. 2014, 57, 176–195. [Google Scholar] [CrossRef]
- Pais, P.; Almeida, V.; Yılmaz, M.; Teixeira, M.C. Saccharomyces Boulardii: What Makes It Tick as Successful Probiotic? J. Fungi 2020, 6, 78. [Google Scholar] [CrossRef] [PubMed]
- Velescu, B.Ș.; Ilie, M.I.; Amzăr, A.I.; Lupașcu, R.E.; Marandiuc, I.M.; Apetroaei, M.-M.; Arsene, A.L.; Blejan, E.I.; Nedea, O.A.; Fistos, T.; et al. Development and Experimental Evaluation of Some Silver Nanoparticles with Antimicrobial Potential. Processes 2023, 11, 1212. [Google Scholar] [CrossRef]
- Klein, E.Y.; Van Boeckel, T.P.; Martinez, E.M.; Pant, S.; Gandra, S.; Levin, S.A.; Goossens, H.; Laxminarayan, R. Global Increase and Geographic Convergence in Antibiotic Consumption between 2000 and 2015. Proc. Natl. Acad. Sci. USA 2018, 115, E3463–E3470. [Google Scholar] [CrossRef]
- Ouwehand, A.C.; DongLian, C.; Weijian, X.; Stewart, M.; Ni, J.; Stewart, T.; Miller, L.E. Probiotics Reduce Symptoms of Antibiotic Use in a Hospital Setting: A Randomized Dose Response Study. Vaccine 2014, 32, 458–463. [Google Scholar] [CrossRef]
- Kerna, N.A. A Complementary Medicine Approach to Augmenting Antibiotic Therapy: Current Practices in the Use of Probiotics during Antibiotic Therapy. Int. J. Complement. Altern. Med. 2018, 11, 62–66. [Google Scholar] [CrossRef]
- Hickson, M.; D’Souza, A.L.; Muthu, N.; Rogers, T.R.; Want, S.; Rajkumar, C.; Bulpitt, C.J. Use of Probiotic Lactobacillus Preparation to Prevent Diarrhoea Associated with Antibiotics: Randomised Double Blind Placebo Controlled Trial. BMJ 2007, 335, 80. [Google Scholar] [CrossRef]
- FAO/WHO. Health and Nutritional Properties of Probiotics in Food Including Powder Milk with Live Lactic Acid Bacteria. Prevention 2001, 5, 1–10. [Google Scholar]
- Hill, C.; Guarner, F.; Reid, G.; Gibson, G.R.; Merenstein, D.J.; Pot, B.; Morelli, L.; Canani, R.B.; Flint, H.J.; Salminen, S.; et al. The International Scientific Association for Probiotics and Prebiotics Consensus Statement on the Scope and Appropriate Use of the Term Probiotic. Nat. Rev. Gastroenterol. Hepatol. 2014, 11, 506–514. [Google Scholar] [CrossRef]
- Precup, G.; Pocol, C.B.; Teleky, B.-E.; Vodnar, D.C. Awareness, Knowledge, and Interest about Prebiotics—A Study among Romanian Consumers. Int. J. Environ. Res. Public Health 2022, 19, 1208. [Google Scholar] [CrossRef]
- Xiang, H.; Sun-Waterhouse, D.; Waterhouse, G.I.N.; Cui, C.; Ruan, Z. Fermentation-Enabled Wellness Foods: A Fresh Perspective. Food Sci. Hum. Wellness 2019, 8, 203–243. [Google Scholar] [CrossRef]
- Cohen, P.A. Probiotic Safety—No Guarantees. JAMA Intern. Med. 2018, 178, 1577. [Google Scholar] [CrossRef] [PubMed]
- de Simone, C. The Unregulated Probiotic Market. Clin. Gastroenterol. Hepatol. 2019, 17, 809–817. [Google Scholar] [CrossRef] [PubMed]
- How the European Commission Deals with “Health Claims” Concerning Probiotics Included in Foodstuffs. Available online: https://www.ombudsman.europa.eu/en/opening-summary/en/179398 (accessed on 27 June 2024).
- Guarner, F.; Ellen Sanders, M.; Gibson, G.; Klaenhammer, T.; Cabana, M.; Scott, K.; Reid, G.; Delzenne, N.M.; Fahey, G.C.; Hill, C. Probiotic and Prebiotic Claims in Europe: Seeking a Clear Roadmap. Br. J. Nutr. 2011, 106, 1765–1767. [Google Scholar] [CrossRef]
- Agamennone, V.; Krul, C.A.M.; Rijkers, G.; Kort, R. A Practical Guide for Probiotics Applied to the Case of Antibiotic-Associated Diarrhea in The Netherlands. BMC Gastroenterol. 2018, 18, 103. [Google Scholar] [CrossRef]
- Daniali, M.; Nikfar, S.; Abdollahi, M. Antibiotic Resistance Propagation through Probiotics. Expert Opin. Drug Metab. Toxicol. 2020, 16, 1207–1215. [Google Scholar] [CrossRef]
- Palleja, A.; Mikkelsen, K.H.; Forslund, S.K.; Kashani, A.; Allin, K.H.; Nielsen, T.; Hansen, T.H.; Liang, S.; Feng, Q.; Zhang, C.; et al. Recovery of Gut Microbiota of Healthy Adults Following Antibiotic Exposure. Nat. Microbiol. 2018, 3, 1255–1265. [Google Scholar] [CrossRef]
- Isaac, S.; Scher, J.U.; Djukovic, A.; Jiménez, N.; Littman, D.R.; Abramson, S.B.; Pamer, E.G.; Ubeda, C. Short- and Long-Term Effects of Oral Vancomycin on the Human Intestinal Microbiota. J. Antimicrob. Chemother. 2017, 72, 128–136. [Google Scholar] [CrossRef]
- Dethlefsen, L.; Relman, D.A. Incomplete Recovery and Individualized Responses of the Human Distal Gut Microbiota to Repeated Antibiotic Perturbation. Proc. Natl. Acad. Sci. USA 2011, 108, 4554–4561. [Google Scholar] [CrossRef]
- Hutchinson, A.N.; Bergh, C.; Kruger, K.; Sűsserová, M.; Allen, J.; Améen, S.; Tingö, L. The Effect of Probiotics on Health Outcomes in the Elderly: A Systematic Review of Randomized, Placebo-Controlled Studies. Microorganisms 2021, 9, 1344. [Google Scholar] [CrossRef] [PubMed]
- Ale, E.C.; Binetti, A.G. Role of Probiotics, Prebiotics, and Synbiotics in the Elderly: Insights Into Their Applications. Front. Microbiol. 2021, 12, 631254. [Google Scholar] [CrossRef] [PubMed]
- Akagawa, S.; Akagawa, Y.; Yamanouchi, S.; Kimata, T.; Tsuji, S.; Kaneko, K. Development of the Gut Microbiota and Dysbiosis in Children. Biosci. Microbiota Food Health 2021, 40, 12–18. [Google Scholar] [CrossRef] [PubMed]
- Cox, L.M.; Blaser, M.J. Antibiotics in Early Life and Obesity. Nat. Rev. Endocrinol. 2015, 11, 182–190. [Google Scholar] [CrossRef]
- West, C.E.; Jenmalm, M.C.; Prescott, S.L. The Gut Microbiota and Its Role in the Development of Allergic Disease: A Wider Perspective. Clin. Exp. Allergy 2015, 45, 43–53. [Google Scholar] [CrossRef]
- Bertakis, K.D.; Azari, R.; Helms, L.J.; Callahan, E.J.; Robbins, J.A. Gender Differences in the Utilization of Health Care Services. J. Fam. Pract. 2000, 49, 147–152. [Google Scholar]
- Fugh-Berman, A.; Kronenberg, F. Complementary and Alternative Medicine (CAM) in Reproductive-Age Women: A Review of Randomized Controlled Trials. Reprod. Toxicol. 2003, 17, 137–152. [Google Scholar] [CrossRef]
- Flach, J.; Dias, A.S.M.; Rademaker, S.H.M.; van der Waal, M.B.; Claassen, E.; Larsen, O.F.A. Medical Doctors’ Perceptions on Probiotics: Lack of Efficacy Data Hampers Innovation. PharmaNutrition 2017, 5, 103–108. [Google Scholar] [CrossRef]
- van der Geest, A.M.; Flach, J.; Claassen, E.; Sijlmans, A.W.; van de Burgwal, L.H.M.; Larsen, O.F.A. European General Practitioners Perceptions on Probiotics: Results of a Multinational Survey. PharmaNutrition 2020, 11, 100178. [Google Scholar] [CrossRef]
- Fijan, S.; Frauwallner, A.; Varga, L.; Langerholc, T.; Rogelj, I.; Lorber, M.; Lewis, P.; Povalej Bržan, P. Health Professionals’ Knowledge of Probiotics: An International Survey. Int. J. Environ. Res. Public Health 2019, 16, 3128. [Google Scholar] [CrossRef]
- Jordan, D.; Johnson, N.; Thomas, L. Probiotics in Primary Care: A Survey of Health Professionals. Pract. Nurs. 2015, 26, 550–554. [Google Scholar] [CrossRef]
- Neut, C.; Mahieux, S.; Dubreuil, L.J. Antibiotic Susceptibility of Probiotic Strains: Is It Reasonable to Combine Probiotics with Antibiotics? Médecine Mal. Infect. 2017, 47, 477–483. [Google Scholar] [CrossRef] [PubMed]
- Drago, L. Probiotics and Colon Cancer. Microorganisms 2019, 7, 66. [Google Scholar] [CrossRef]
- McFarland, L.V. From Yaks to Yogurt: The History, Development, and Current Use of Probiotics. Clin. Infect. Dis. 2015, 60, S85–S90. [Google Scholar] [CrossRef] [PubMed]
- Hammad, A.M.; Shimamoto, T. Towards a Compatible Probiotic-Antibiotic Combination Therapy: Assessment of Antimicrobial Resistance in the Japanese Probiotics. J. Appl. Microbiol. 2010, 109, 1349–1360. [Google Scholar] [CrossRef] [PubMed]
- Boyanova, L.; Mitov, I. Coadministration of Probiotics with Antibiotics: Why, When and for How Long? Expert Rev. Anti. Infect. Ther. 2012, 10, 407–409. [Google Scholar] [CrossRef]
- Didari, T. Effectiveness of Probiotics in Irritable Bowel Syndrome: Updated Systematic Review with Meta-Analysis. World J. Gastroenterol. 2015, 21, 3072. [Google Scholar] [CrossRef]
- Jakubczyk, D.; Leszczyńska, K.; Górska, S. The Effectiveness of Probiotics in the Treatment of Inflammatory Bowel Disease (IBD)—A Critical Review. Nutrients 2020, 12, 1973. [Google Scholar] [CrossRef]
- Sánchez, B.; Delgado, S.; Blanco-Míguez, A.; Lourenço, A.; Gueimonde, M.; Margolles, A. Probiotics, Gut Microbiota, and Their Influence on Host Health and Disease. Mol. Nutr. Food Res. 2017, 61, 1600240. [Google Scholar] [CrossRef]
- Amzăr, A.I.; Udeanu, D.I.; Pițuru, M.T.; Hîrjău, M.; Popa, D.E.; Velescu, B.Ş.; Arsene, A.L. Signalling through the microbiota-gut-brain triade. Farmacia 2022, 70, 402–409. [Google Scholar] [CrossRef]
- Ojha, S.; Patil, N.; Jain, M.; Kole, C.; Kaushik, P. Probiotics for Neurodegenerative Diseases: A Systemic Review. Microorganisms 2023, 11, 1083. [Google Scholar] [CrossRef] [PubMed]
- Liu, R.T.; Walsh, R.F.L.; Sheehan, A.E. Prebiotics and Probiotics for Depression and Anxiety: A Systematic Review and Meta-Analysis of Controlled Clinical Trials. Neurosci. Biobehav. Rev. 2019, 102, 13–23. [Google Scholar] [CrossRef] [PubMed]
- Suganya, K.; Koo, B.-S. Gut–Brain Axis: Role of Gut Microbiota on Neurological Disorders and How Probiotics/Prebiotics Beneficially Modulate Microbial and Immune Pathways to Improve Brain Functions. Int. J. Mol. Sci. 2020, 21, 7551. [Google Scholar] [CrossRef] [PubMed]
- Oniszczuk, A.; Oniszczuk, T.; Gancarz, M.; Szymańska, J. Role of Gut Microbiota, Probiotics and Prebiotics in the Cardiovascular Diseases. Molecules 2021, 26, 1172. [Google Scholar] [CrossRef]
- Tao, Y.-W.; Gu, Y.-L.; Mao, X.-Q.; Zhang, L.; Pei, Y.-F. Effects of Probiotics on Type II Diabetes Mellitus: A Meta-Analysis. J. Transl. Med. 2020, 18, 30. [Google Scholar] [CrossRef]
- Sivamaruthi, B.S.; Kesika, P.; Suganthy, N.; Chaiyasut, C. A Review on Role of Microbiome in Obesity and Antiobesity Properties of Probiotic Supplements. Biomed Res. Int. 2019, 2019, 1–20. [Google Scholar] [CrossRef]
- Legesse Bedada, T.; Feto, T.K.; Awoke, K.S.; Garedew, A.D.; Yifat, F.T.; Birri, D.J. Probiotics for Cancer Alternative Prevention and Treatment. Biomed. Pharmacother. 2020, 129, 110409. [Google Scholar] [CrossRef]
- Lopez-Santamarina, A.; Gonzalez, E.G.; Lamas, A.; Mondragon, A.D.C.; Regal, P.; Miranda, J.M. Probiotics as a Possible Strategy for the Prevention and Treatment of Allergies. A Narrative Review. Foods 2021, 10, 701. [Google Scholar] [CrossRef]
- Quigley, E.M.M. Prebiotics and Probiotics in Digestive Health. Clin. Gastroenterol. Hepatol. 2019, 17, 333–344. [Google Scholar] [CrossRef]
- Sherman, P.M.; Ossa, J.C.; Johnson-Henry, K. Unraveling Mechanisms of Action of Probiotics. Nutr. Clin. Pract. 2009, 24, 10–14. [Google Scholar] [CrossRef]
- McFarland, L.; Elmer, G. Properties of Evidence-Based Probiotics for Human Health. In Probiotics in Food Safety and Human Health; CRC Press: Boca Raton, FL, USA, 2005; pp. 109–138. [Google Scholar]
- Duysburgh, C.; Van den Abbeele, P.; Morera, M.; Marzorati, M. Lacticaseibacillus Rhamnosus GG and Saccharomyces Cerevisiae Boulardii Supplementation Exert Protective Effects on Human Gut Microbiome Following Antibiotic Administration in Vitro. Benef. Microbes 2021, 12, 365–380. [Google Scholar] [CrossRef]
- Wilkins, T.; Sequoia, J. Probiotics for Gastrointestinal Conditions: A Summary of the Evidence. Am. Fam. Physician 2017, 96, 170–178. [Google Scholar] [PubMed]
- McFarland, L.V. Common Organisms and Probiotics: Saccharomyces Boulardii. In The Microbiota in Gastrointestinal Pathophysiology; Elsevier: Amsterdam, The Netherlands, 2017; pp. 145–164. [Google Scholar]
- Szajewska, H.; Kołodziej, M. Systematic Review with Meta-analysis: Saccharomyces Boulardii in the Prevention of Antibiotic-associated Diarrhoea. Aliment. Pharmacol. Ther. 2015, 42, 793–801. [Google Scholar] [CrossRef]
- Ahmadi, E.; Alizadeh-Navaei, R.; Rezai, M.S. Efficacy of Probiotic Use in Acute Rotavirus Diarrhea in Children: A Systematic Review and Meta-Analysis. Casp. J. Intern. Med. 2015, 6, 187–195. [Google Scholar]
- Szajewska, H.; Kołodziej, M. Systematic Review with Meta-Analysis: Lactobacillus Rhamnosus GG in the Prevention of Antibiotic-Associated Diarrhoea in Children and Adults. Aliment. Pharmacol. Ther. 2015, 42, 1149–1157. [Google Scholar] [CrossRef] [PubMed]
- McFarland, L.V. Antibiotic-Associated Diarrhea: Epidemiology, Trends and Treatment. Future Microbiol. 2008, 3, 563–578. [Google Scholar] [CrossRef]
- Johnston, B.C.; Goldenberg, J.Z.; Vandvik, P.O.; Sun, X.; Guyatt, G.H. Probiotics for the Prevention of Pediatric Antibiotic-Associated Diarrhea. In Cochrane Database of Systematic Reviews; Johnston, B.C., Ed.; John Wiley & Sons, Ltd.: Chichester, UK, 2011. [Google Scholar]
- Goldenberg, J.Z.; Lytvyn, L.; Steurich, J.; Parkin, P.; Mahant, S.; Johnston, B.C. Probiotics for the Prevention of Pediatric Antibiotic-Associated Diarrhea. Cochrane Database Syst. Rev. 2015, 12, CD004827. [Google Scholar] [CrossRef] [PubMed]
- Guo, Q.; Goldenberg, J.Z.; Humphrey, C.; El Dib, R.; Johnston, B.C. Probiotics for the Prevention of Pediatric Antibiotic-Associated Diarrhea. Cochrane Database Syst. Rev. 2019, 4, CD004827. [Google Scholar] [CrossRef]
- Başar Güneş, H.; Bayraktar Ekincioğlu, A.; Karakan, T.; Demirkan, K. Assessment of Knowledge and Attitudes of Physicians and Pharmacists on Probiotics: A Cross-Sectional Survey. Turkish J. Pharm. Sci. 2024, 21, 36–41. [Google Scholar] [CrossRef]
- Oliver, L.; Rasmussen, H.; Gregoire, M.B.; Chen, Y. Health Care Provider’s Knowledge, Perceptions, and Use of Probiotics and Prebiotics. Top. Clin. Nutr. 2014, 29, 139–149. [Google Scholar] [CrossRef]
- Wilson, Z.; Whitehead, K. A Cross Sectional Survey to Assess Healthcare Professionals’ Attitudes to and Understanding of Probiotics. Clin. Nutr. ESPEN 2019, 34, 104–109. [Google Scholar] [CrossRef]
- Singh, T.P.; Natraj, B.H. Next-Generation Probiotics: A Promising Approach towards Designing Personalized Medicine. Crit. Rev. Microbiol. 2021, 47, 479–498. [Google Scholar] [CrossRef] [PubMed]
- Gueimonde, M.; Sánchez, B.; de los Reyes-Gavilán, C.G.; Margolles, A. Antibiotic Resistance in Probiotic Bacteria. Front. Microbiol. 2013, 4, 202. [Google Scholar] [CrossRef]
- Salminen, M.K.; Rautelin, H.; Tynkkynen, S.; Poussa, T.; Saxelin, M.; Valtonen, V.; Jarvinen, A. Lactobacillus Bacteremia, Species Identification, and Antimicrobial Susceptibility of 85 Blood Isolates. Clin. Infect. Dis. 2006, 42, e35–e44. [Google Scholar] [CrossRef]
- Li, S.; Li, Z.; Wei, W.; Ma, C.; Song, X.; Li, S.; He, W.; Tian, J.; Huo, X. Association of Mutation Patterns in GyrA and ParC Genes with Quinolone Resistance Levels in Lactic Acid Bacteria. J. Antibiot. 2015, 68, 81–87. [Google Scholar] [CrossRef] [PubMed]
- Mantegazza, C.; Molinari, P.; D’Auria, E.; Sonnino, M.; Morelli, L.; Zuccotti, G.V. Probiotics and Antibiotic-Associated Diarrhea in Children: A Review and New Evidence on Lactobacillus Rhamnosus GG during and after Antibiotic Treatment. Pharmacol. Res. 2018, 128, 63–72. [Google Scholar] [CrossRef] [PubMed]
- Doron, S.I.; Hibberd, P.L.; Gorbach, S.L. Probiotics for Prevention of Antibiotic-Associated Diarrhea. J. Clin. Gastroenterol. 2008, 42, S58–S63. [Google Scholar] [CrossRef]
- Forssten, S. Influence of a Probiotic Mixture on Antibiotic Induced Microbiota Disturbances. World J. Gastroenterol. 2014, 20, 11878. [Google Scholar] [CrossRef]
- Plummer, S.F.; Garaiova, I.; Sarvotham, T.; Cottrell, S.L.; Le Scouiller, S.; Weaver, M.A.; Tang, J.; Dee, P.; Hunter, J. Effects of Probiotics on the Composition of the Intestinal Microbiota Following Antibiotic Therapy. Int. J. Antimicrob. Agents 2005, 26, 69–74. [Google Scholar] [CrossRef]
- Madden, J.A.J.; Plummer, S.F.; Tang, J.; Garaiova, I.; Plummer, N.T.; Herbison, M.; Hunter, J.O.; Shimada, T.; Cheng, L.; Shirakawa, T. Effect of Probiotics on Preventing Disruption of the Intestinal Microflora Following Antibiotic Therapy: A Double-Blind, Placebo-Controlled Pilot Study. Int. Immunopharmacol. 2005, 5, 1091–1097. [Google Scholar] [CrossRef]
- Voicu, S.N.; Scărlătescu, A.I.; Apetroaei, M.-M.; Nedea, M.I.; Blejan, I.E.; Udeanu, D.I.; Velescu, B.Ș.; Ghica, M.; Nedea, O.A.; Cobelschi, C.P.; et al. Evaluation of Neuro-Hormonal Dynamics after the Administration of Probiotic Microbial Strains in a Murine Model of Hyperthyroidism. Nutrients 2024, 16, 1077. [Google Scholar] [CrossRef]
- King, S.; Glanville, J.; Sanders, M.E.; Fitzgerald, A.; Varley, D. Effectiveness of Probiotics on the Duration of Illness in Healthy Children and Adults Who Develop Common Acute Respiratory Infectious Conditions: A Systematic Review and Meta-Analysis. Br. J. Nutr. 2014, 112, 41–54. [Google Scholar] [CrossRef]
- Villena, J.; Chiba, E.; Tomosada, Y.; Salva, S.; Marranzino, G.; Kitazawa, H.; Alvarez, S. Orally Administered Lactobacillus Rhamnosus Modulates the Respiratory Immune Response Triggered by the Viral Pathogen-Associated Molecular Pattern Poly(I:C). BMC Immunol. 2012, 13, 53. [Google Scholar] [CrossRef] [PubMed]
- Liao, H.; Liu, S.; Wang, H.; Su, H.; Liu, Z. Enhanced Antifungal Activity of Bovine Lactoferrin-Producing Probiotic Lactobacillus Casei in the Murine Model of Vulvovaginal Candidiasis. BMC Microbiol. 2019, 19, 7. [Google Scholar] [CrossRef]
- Reid, G. In Vitro Testing of Lactobacillus Acidophilus NCFMTM as a Possible Probiotic for the Urogenital Tract. Int. Dairy J. 2000, 10, 415–419. [Google Scholar] [CrossRef]
- Falagas, M.E.; Betsi, G.I.; Tokas, T.; Athanasiou, S. Probiotics for Prevention of Recurrent Urinary Tract Infections in Women. Drugs 2006, 66, 1253–1261. [Google Scholar] [CrossRef] [PubMed]
- Akgul, T.; Karakan, T. The Role of Probiotics in Women with Recurrent Urinary Tract Infections. Türk Üroloji Dergisi/Turkish J. Urol. 2018, 44, 377–383. [Google Scholar] [CrossRef] [PubMed]
- Raheem, A.; Liang, L.; Zhang, G.; Cui, S. Modulatory Effects of Probiotics During Pathogenic Infections With Emphasis on Immune Regulation. Front. Immunol. 2021, 12, 616713. [Google Scholar] [CrossRef]
- Chitulea, P.; Gherai, R.; Cheta, C.; Marin Negru, T. The role of intravaginal prebiotics in controlling the evolution of uncomplicated bacterial and fungal vaginal infections. Farmacia 2022, 70, 545–549. [Google Scholar] [CrossRef]
- Vladescu, C.; Scintee, S.G.; Olsavszky, V.; Hernandez-Quevedo, C.; Sagan, A. Romania: Health System Review. Health Syst. Transit. 2016, 18, 1–170. [Google Scholar] [PubMed]












{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Genus | Species | Strain |
|---|---|---|
| Bacillus | B. clausii | N/A |
| B. mesentericus | TO-A | |
| B.coagulans | N/A | |
| Bifidobacterium | B. bifidum | HA-132 |
| BB-01 | ||
| W-23 | ||
| BB-G90 | ||
| B. breve | BR-03 | |
| BB-G95 | ||
| B. infantis | N/A | |
| B. lactis | BL-G101 | |
| DSM 15954 (BB-12) | ||
| BI-04 | ||
| W-52 | ||
| HN-019 | ||
| Lafti B-94 | ||
| B. longum | BB-536 | |
| W-11 | ||
| BL-986 | ||
| N/A | ||
| Clostridium | C.butyricum | TO-A |
| Enterococcus | E. faecium | N/A |
| Lactobacillus | L. acidophillus | LA-G80 |
| LA-14 | ||
| LA-1063 | ||
| LA-02 | ||
| HA-122 | ||
| DSM 13241 (LA-5) | ||
| Rosell-52 | ||
| L. casei | HA-108 | |
| R-0215 | ||
| LC-03 | ||
| L. paracasei | 431 | |
| LPC-12 | ||
| LPC-G110 | ||
| Lafti L-26 | ||
| CNCM I-1572 | ||
| L. fermentum | LF-26 | |
| L. gasseri | LG-G12 | |
| L. helveticus | LH-43 | |
| Lafti L-10 | ||
| Rosell-52 | ||
| L. plantarum | CECT 7484 | |
| CECT 7485 | ||
| R-1012 | ||
| LP-09 | ||
| LP-G18 | ||
| L. reuterii | DSM 17938 | |
| L. rhamnosus | GG | |
| R-0011 | ||
| LR-02 | ||
| LRH-10 | ||
| HN-001 | ||
| LR-G14 | ||
| Rosell-11 | ||
| Lactococcus | L. lactis | LL-02 |
| W-58 | ||
| Pediococcus | P. acidilactici | CECT 7483 |
| Saccharomyces | S. boulardii | CNCM I-745 |
| Lesaffre CNCM I-3799 | ||
| N/A | ||
| S. cerevisiae | CNCM I-3856 | |
| Streptococcus | S. faecalis | T-110 |
| S. salivarius | K-12 | |
| S. thermophilus | TH-4 | |
| ST-30 | ||
| YA-08 |
| Class of Antibiotics | Antibiotics Associated with Probiotics | % |
|---|---|---|
| Penicillins | Amoxicillin/clavulanic acid | 43.1 |
| Amoxicillin | 3.9 | |
| Other penicillins | 0.5 | |
| Cephalosporines | Cefuroxime | 9.5 |
| Cefixime | 4.6 | |
| Other cephalosporines | 0.7 | |
| Macrolides | Azithromycin | 6.1 |
| Clarithromycin | 5.6 | |
| Other macrolides | 0.5 | |
| Fluoroquinolones | Ciprofloxacin | 6.8 |
| Levofloxacin | 5.7 | |
| Other fluoroquinolones | 2.0 | |
| Other classes | Lincosamides | 2.9 |
| Tetracyclines | 2.4 | |
| Nitroimidazoles | 3.2 | |
| Others | 2.7 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Scărlătescu, A.-I.; Velescu, B.Ș.; Apetroaei, M.-M.; Nedea, M.I.; Udeanu, D.I.; Arsene, A.L. Practices and Trends in the Prescription of Probiotics: A Detailed Analysis in an Eastern European Region. Processes 2024, 12, 1856. https://doi.org/10.3390/pr12091856
Scărlătescu A-I, Velescu BȘ, Apetroaei M-M, Nedea MI, Udeanu DI, Arsene AL. Practices and Trends in the Prescription of Probiotics: A Detailed Analysis in an Eastern European Region. Processes. 2024; 12(9):1856. https://doi.org/10.3390/pr12091856
Chicago/Turabian StyleScărlătescu, Anca-Ioana (Amzăr), Bruno Ștefan Velescu, Miruna-Maria Apetroaei, Marina Ionela (Ilie) Nedea, Denisa Ioana Udeanu, and Andreea Letiția Arsene. 2024. "Practices and Trends in the Prescription of Probiotics: A Detailed Analysis in an Eastern European Region" Processes 12, no. 9: 1856. https://doi.org/10.3390/pr12091856
APA StyleScărlătescu, A.-I., Velescu, B. Ș., Apetroaei, M.-M., Nedea, M. I., Udeanu, D. I., & Arsene, A. L. (2024). Practices and Trends in the Prescription of Probiotics: A Detailed Analysis in an Eastern European Region. Processes, 12(9), 1856. https://doi.org/10.3390/pr12091856