The Accident Path of Coal Mine Gas Explosion Based on 24Model: A Case Study of the Ruizhiyuan Gas Explosion Accident

Abstract
:1. Introduction
2. Analysis Method
2.1. Traditional Accident Causation Model
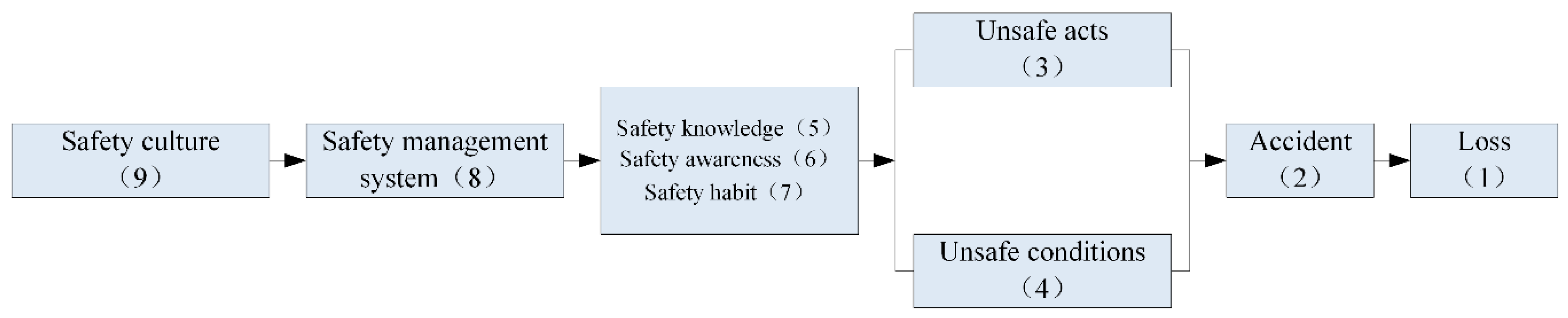
2.2. Development of 24Model
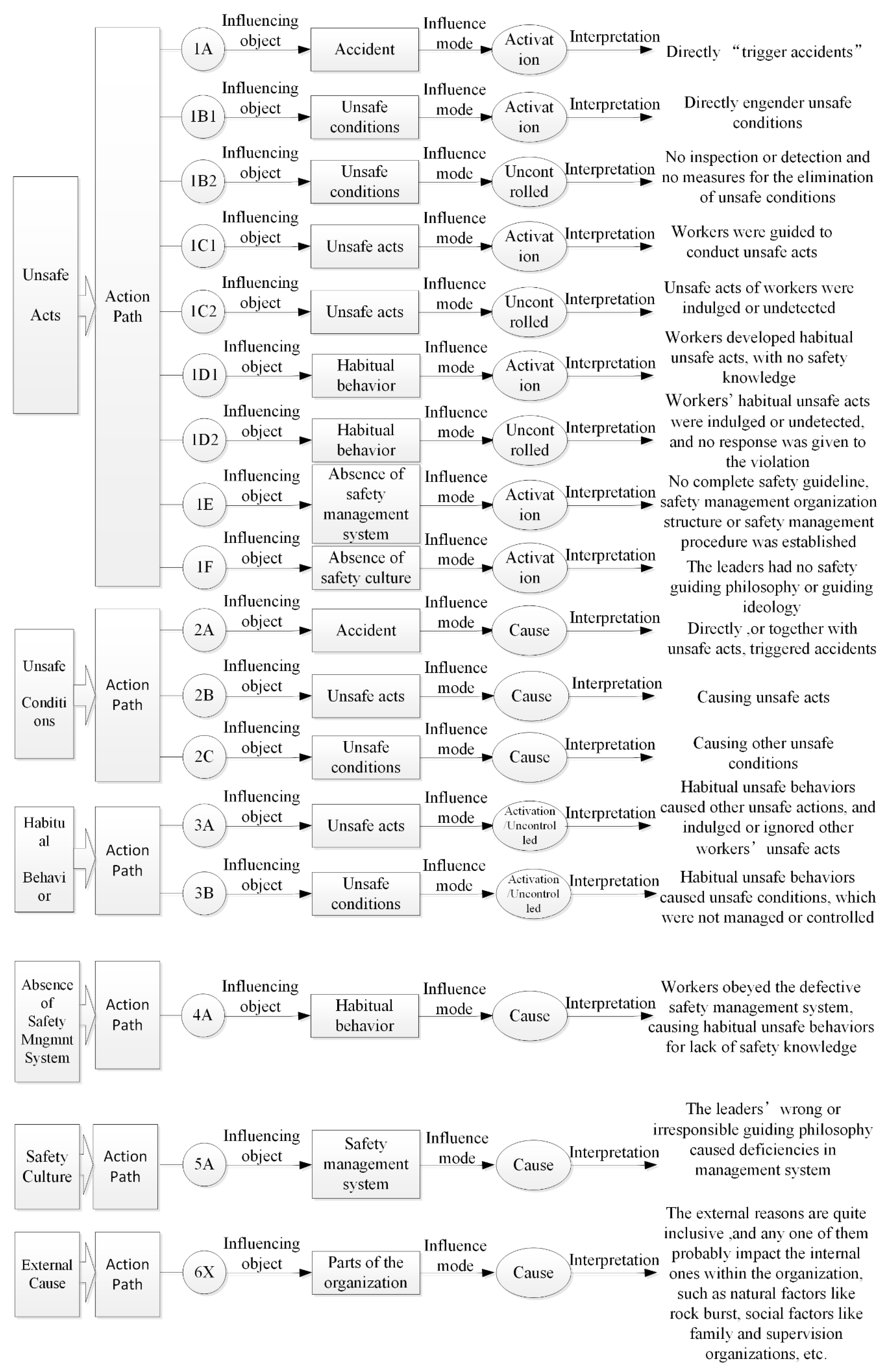
2.3. Specific Definition of 24Model
3. Accident Analysis
3.1. Gas Explosion Accident of Ruizhiyuan Coal Industry Co.
3.2. Accident Analysis Steps
3.2.1. Organizational Carving Up
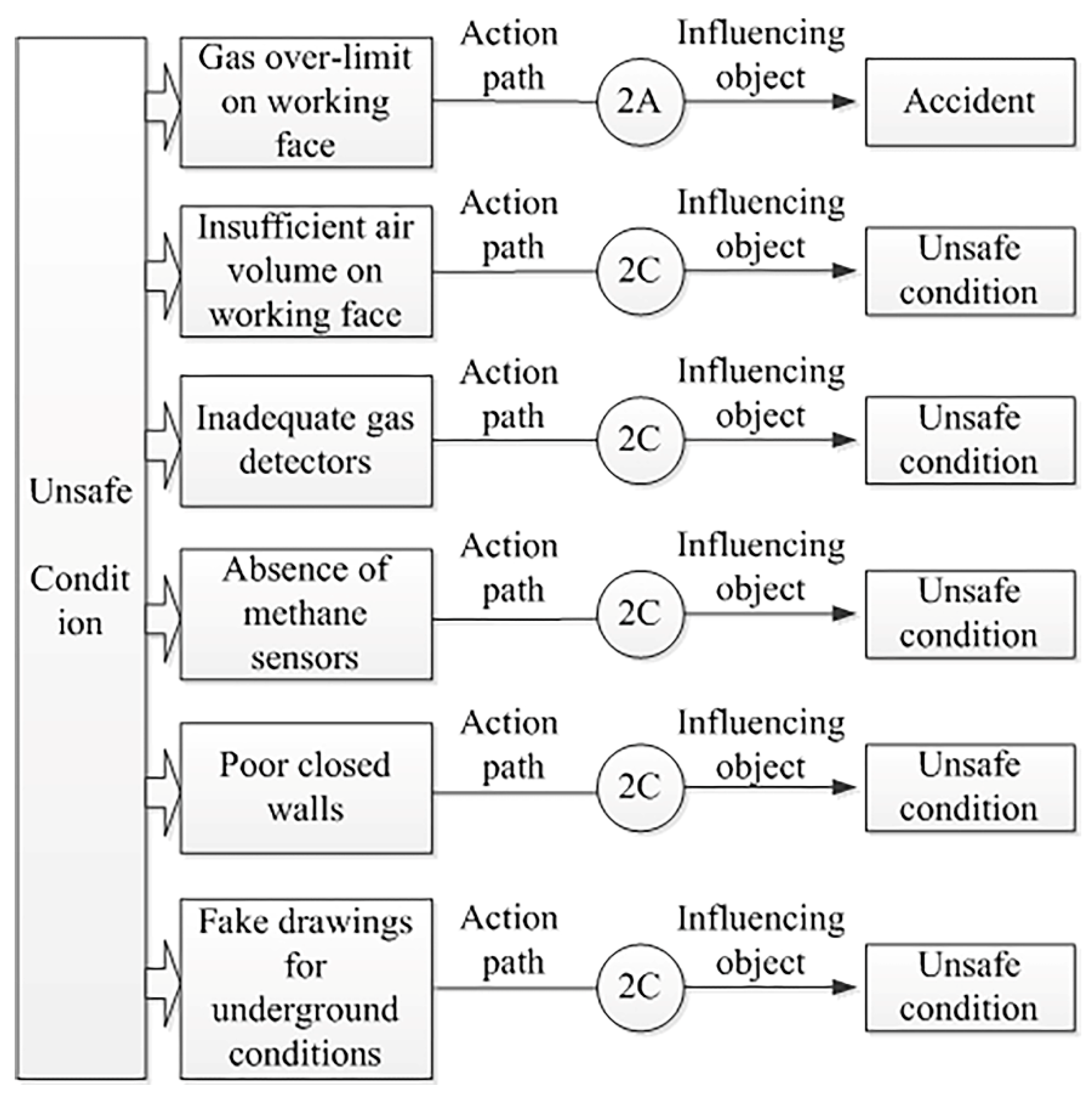
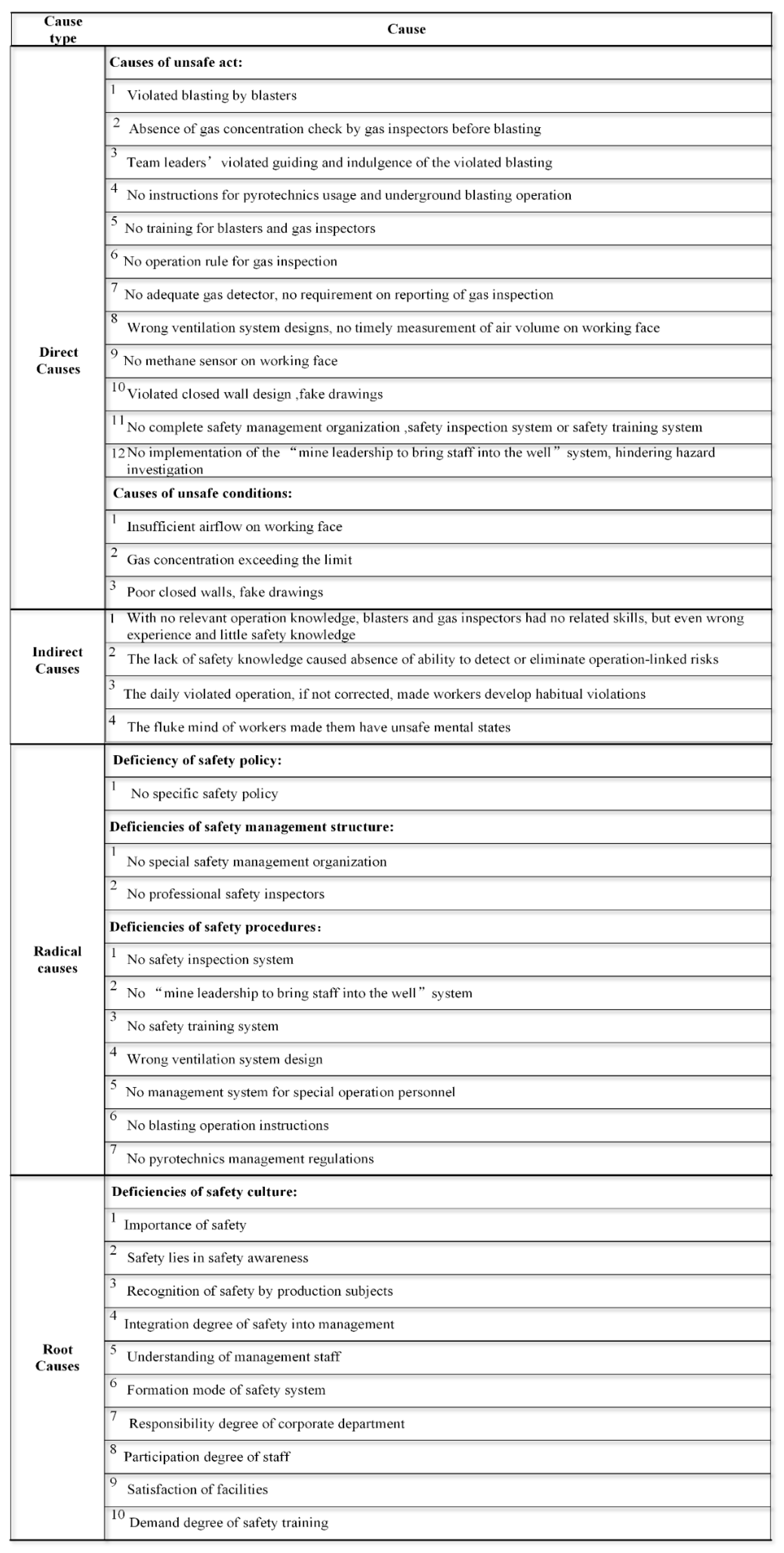
3.2.2. Cause Analysis of Unsafe Conditions
3.2.3. Cause Analysis of Habitual Behaviors
3.2.4. Analysis of Reasons for Safety Management System
- (1)
- Deficiency of a safety policy: There was no clear and specific safety policy.
- (2)
- Deficiency of a safety management organizational structure: There were no special safety management agencies or full-time security personnel.
- (3)
- Deficiency of safety management procedures: There was no implementation of a safety inspection system, no “mine leadership to bring staff into the well” system, no safety training system, an incorrect ventilation system design, no special operation personnel management system, no implementation of blasting procedures, and no pyrotechnics management regulations.
3.2.5. Absence of a Safety Culture
- (1)
- The importance of safety and actual safety are mainly determined by safety awareness and understanding of personnel with safe production. The mine authorities did not establish a safety policy, indicating that management leaders did not believe that safe production and awareness were important or necessary in order to provide a safe environment.
- (2)
- The degree of integration of safety into management, the understanding of responsibility by management staff, and the formation mode of safety systems ensured that there was no basic understanding of safety management or awareness of safety system formation. This resulted in the absence of a basic safety management system.
- (3)
- The degree of emphasis on safety of the enterprise department, the degree of employee participation in safety, the lack of adequate facilities, and the degree of safety training all contributed to the accident. The departments at the management level did not assign specific personnel to be responsible for safe production, and they did not ascertain the use of the wrong design, resulting in operation by workers with no safe production awareness. The workers used equipment purchased by management personnel that had no regular maintenance management, causing a large number of safety hazards. The mine leadership possibly considered it unnecessary to provide safety training and so the safety training system was ignored.
4. Results
5. Conclusions and Suggestions
Analysis and Advice on Preventing General Accidents
Author Contributions
Funding
Conflicts of Interest
References
- BP. BP Statistical Review of World Energy 2017; BP: London, UK, 2017. [Google Scholar]
- State Administration of Coal Mine Safety. Compilation of National Coal Mine Accidents Analysis Report in 2007; State Administration of Coal Mine Safety: Beijing, China, 2008.
- State Administration of Coal Mine Safety. Compilation of National Coal Mine Accidents Analysis Report in 2008; State Administration of Coal Mine Safety: Beijing, China, 2009.
- State Administration of Coal Mine Safety. Compilation of National Coal Mine Accidents Analysis Report in 2009; State Administration of Coal Mine Safety: Beijing, China, 2010.
- State Administration of Coal Mine Safety. Compilation of National Coal Mine Accidents Analysis Report in 2010; State Administration of Coal Mine Safety: Beijing, China, 2011.
- State Administration of Coal Mine Safety. Compilation of National Coal Mine Accidents Analysis Report in 2011; State Administration of Coal Mine Safety: Beijing, China, 2012.
- State Administration of Coal Mine Safety. Compilation of National Coal Mine Accidents Analysis Report in 2012; State Administration of Coal Mine Safety: Beijing, China, 2013.
- State Administration of Coal Mine Safety. Compilation of National Coal Mine Accidents Analysis Report in 2013; State Administration of Coal Mine Safety: Beijing, China, 2014.
- State Administration of Coal Mine Safety. Compilation of National Coal Mine Accidents Analysis Report in 2014; State Administration of Coal Mine Safety: Beijing, China, 2015.
- State Administration of Coal Mine Safety. Compilation of National Coal Mine Accidents Analysis Report in 2015; State Administration of Coal Mine Safety: Beijing, China, 2016.
- State Administration of Coal Mine Safety. Compilation of National Coal Mine Accidents Analysis Report in 2016; State Administration of Coal Mine Safety: Beijing, China, 2017.
- Xie, X.; Guo, D. Human factors risk assessment and management: Process safety in engineering. Process. Saf. Environ. Prot. 2018, 113, 467–482. [Google Scholar] [CrossRef]
- Xie, X.; Fu, G.; Xue, Y.; Zhao, Z.; Chen, P.; Lu, B.; Jiang, S. Risk prediction and factors risk analysis based on IFOA-GRNN and apriority algorithms: Application of artificial intelligence in accident prevention. Process. Saf. Environ. Prot. 2019, 122, 169–184. [Google Scholar] [CrossRef]
- Li, W.-B.; Xiao, D.-S. Overview on Accident-Causing Theories. J. Univ. South China (Soc. Sci. Ed.) 2007, 8, 57–61. [Google Scholar]
- Huang, L.; Wu, C. Study on system of accident-causing model and its general modeling methods and development trend. J. Saf. Sci. Technol. 2017, 13, 10–16. [Google Scholar]
- Greenwood, M.; Woods, H.M. The Incidence of Industrial Accidents upon Individuals with Specific Reference to Multiple Accidents; Report No. 4; Industrial Fatigue Research Board: London, UK, 1919. [Google Scholar]
- Heinrich, H.W.; Petersen, D.; Roos, N.R. Industrial Accident Prevention: A Safety Management Approach, 5th ed.; McGraw-Hill Companies: New York, NY, USA, 1980. [Google Scholar]
- Reason, J. Human Error; Cambridge University Press: New York, NY, USA, 1990. [Google Scholar]
- Levenson, N. System Safety and Computers; Addison Wesley: Boston, MA, USA, 1995. [Google Scholar]
- Rasmussen, J. Risk management in a dynamic society: A modelling problem. Saf. Sci. 1997, 27, 183–213. [Google Scholar] [CrossRef]
- Leveson, N. Engineering a Safer World: Applying Systems Thinking to Safety; MIT Press: Cambridge, MA, USA, 2012. [Google Scholar]
- Leveson, N. A systems approach to risk management through leading safety indicators. Reliab. Eng. Syst. Saf. 2015, 136, 17–34. [Google Scholar] [CrossRef] [Green Version]
- Niu, F.; Wang, Y.; Zhou, C. Analysis of Safety Accidents Caused by Subway Construction Based on STAMP Model. J. Civ. Eng. Manag. 2016, 1, 73–78. [Google Scholar]
- Xiao, S. Causation Analysis Method and Application Research of Gas Explosion Accidents in Coal Mines; China University of Mining & Technology: Beijing, China, 2018. [Google Scholar]
- Salmon, P.M.; Cornelissen, M.; Trotter, M.J. Systems-based accident analysis methods: A comparison of Accimap, HFACS, and STAMP. Saf. Sci. 2012, 50, 1158–1170. [Google Scholar] [CrossRef]
- Suo, X.; Fu, G.; Wang, C.; Jia, Q. An Application of 24Model to Analysis Capsizing of the Eastern Star Ferry. Pol. Marit. Res. 2017, 24, 116–122. [Google Scholar] [CrossRef]
- Xue, Y.; Fu, G. A Modified Accident Analysis and Investigation Model for the General Aviation Industry: Emphasizing on Human and Organizational Factors. J. Saf. Res. 2018, 9, 1–15. [Google Scholar] [CrossRef] [PubMed]
- Hu, Z. The Study on Cause for Food Enterprise Ammonia Leakage Accidents in China; China University of Mining & Technology: Beijing, China, 2018. [Google Scholar]
- Chen, P.; Li, Y. Research on the Formation and the Version Evolution of 24Model. Ind. Saf. Environ. Prot. 2017, 43, 51–54. [Google Scholar]
- Fu, G.; Lu, B.; Chen, X. Behavior Based Model for Organizational Safety Management. China Saf. Sci. J. 2005, 15, 21–27. [Google Scholar]
- Stewart, J.M. The turn-around in safety at the Kenora pulp paper mill. Prof. Saf. 2011, 46, 34–44. [Google Scholar]
- Fu, G.; Yin, W.; Dong, J.; Di, F. Behavior-based accident causation: The 24Model and its safety implication in coal mines. J. China Coal Soc. 2013, 38, 1123–1129. [Google Scholar]
- Fu, G. Studies on the Structure of Safety Science; Safety Science Publishing: Beijing, China, 2015; pp. 13–14. [Google Scholar]
- Fu, G.; Fan, Y.; Tong, R.; Gong, Y. A Universal Methodology for the Causation Analysis of Accidents (4th Edition). J. Accid. Prev. 2016, 2, 7–12. [Google Scholar]
- Fu, G.; Li, R. Fifth Edition 24Model. 2017. Available online: http://blog.sciencenet.cn/blog-603730-1083115.html (accessed on 31 October 2017).
- Yin, W.; Fu, G.; Gong, J. Research on coal miners’ operating against safety regulation: “cognition-behavior” failure mechanism and control measures. China Saf. Sci. J. 2015, 25, 153–159. [Google Scholar]
- Yin, W.; Fu, G.; Zhu, K.; Gong, J. Design and Implementation of Coal Mine Accident Prevention Behavior Safety Method. Saf. Coal Mines 2016, 47, 228–230. [Google Scholar]
- Wu, C.; Fu, G. Interaction Study between Unsafe Acts and Unsafe Conditions. Ind. Saf. Environ. Prot. 2018, 44, 16–18, 23. [Google Scholar]
- Fu, G. Safety Management—A Behavior-based Approach to Accident Prevention; Science Press: Beijing, China, 2013; pp. 79–84. [Google Scholar]
- Rasmussen, J.; Suedung, I. Proactive Risk Management in a Dynamic Society; Swedish Rescue Services Agency: Geneva, Switzerland, 2000.
- Wang, D. Mine Ventilation and Safety; China University of Mining and Technology Press: Xuzhou, China, 2005. [Google Scholar]
- Baidu Baike. 2007. Available online: https://baike.baidu.com/item/12·6临汾煤矿爆炸事故/22080965?fr=aladdin (accessed on 17 August 2018).






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Unsafe Act | Action Maker | Staff Level | Action Path | Influencing Object | Influence Mode | Interpretation |
|---|---|---|---|---|---|---|
| Violated blasting | Blasters on duty | Shift employees | 1A | Accident | Activation | Ignition source in this accident was blasting flames from violated blasting, igniting transfinite gas accumulated on windless working face, resulting in gas explosion |
| Blaster | Shift employees | 3A | Unsafe actions of blasters on duty | Activation | In normal operation, blasters habitually violated rules and regulations, so they did as usual on accident day | |
| Unchecked gas concentration | Gas checkers on duty | Shift employees | 1B2 | Unsafe conditions | Uncontrolled | Gas checkers did not check gas concentration before blasting, so gas concentration limit could not be detected in time |
| Gas checkers | Shift employees | 3A | Unsafe actions of gas checkers on duty | Activation | Gas checkers habitually did not check gas concentration before blasting as usual on accident day | |
| Gas checkers | Shift employees | 3A | Unsafe conditions | Uncontrolled | Gas checkers habitually skived off work | |
| Regulations on management of firework products and blasting operation rules | Mining team | Direct management staff | 1E | Absence of safety management system | Activation | Company did not formulate instructions for blasting operation or relevant knowledge training for blasters, so they had no knowledge or skills in blasting, and were even given wrong information; thus, they were not equipped to detect and eliminate potential risks in blasting; over time, blasters develop habitual violation |
| Production safety deputy head | Mine-level management staff | 1E | Absence of safety management system | Activation | ||
| Absence of safety training on blasters | Mining team | Direct management staff | 1D1 | Habitual unsafe action of blasters | Activation | |
| Directed or condoned violations of workers’ behavior | Mining team, team leader, safety inspection department | Direct management staff | 1D1/1D2 | Bad habits of unsafe actions of blasters | Activation/Uncontrolled | In normal operation, blasters developed habitual violation of regulations in long-term usual practice |
| Team leader | Direct management staff | 1C2 | Unsafe actions of blasters on duty | Uncontrolled | At occurrence of accident, wrong guidance and indulgence of blasters’ violated operation emerged | |
| Absence of gas inspection system | Ventilation team | Direct management staff | 1E | Absence of safety management system | Activation/Uncontrolled | Mine leaders illegally conducted work in closed areas and little emphasized gas prevention and treatment in working environment |
| Production safety deputy head | Mine-level management staff | 1E | Unsafe actions of blasters on duty | Uncontrolled | Absence of gas inspection system provided little knowledge and skills related to gas inspection, and even incorrect information; thus, gas inspectors gradually developed an operation mode of habitual violation | |
| Absence of training on gas inspectors | Ventilation team | Direct management staff | 1D1 | Habitual unsafe actions of gas inspectors | Activation | Absence of gas training for gas inspectors provided little knowledge and skills related to gas inspection, and even incorrect experience, and further made them unable to detect and eliminate gas concentration over limits; thus, they gradually developed an operation mode of habitual violation |
| Usual absence of gas detector | Team leader, ventilation team, safety inspection department | Direct management staff | 1D1/1D2 | Habitual unsafe actions of gas inspectors | Activation/Uncontrolled | Ventilation team had inadequate gas detector and did not implement check system before descending the well, so workers did not bring gas detectors or have gas inspectors give real-time monitoring and reporting of gas concentration |
| Team leader | Direct management staff | 1C2 | Unsafe actions of gas inspector on duty | Uncontrolled | No gas inspectors were designated for inspection | |
| Wrong ventilation system design | Ventilation team | Direct management staff | 1E | Absence of safety management system | Activation | Workers were organized to illegally work in closed area with no consideration of inappropriate ventilation system, resulting in no effective air volume on working face and frequent work under over-limit gas conditions |
| Production safety deputy head | Mine-level management staff | 1E | Absence of safety management system | Activation | ||
| Implementation of inappropriate ventilation system | Ventilation team | Direct management staff | 1B1 | Unsafe conditions | Activation | |
| Absence of methane sensor | Ventilation team | Direct management staff | 1B2 | Unsafe conditions | Uncontrolled | No methane sensor was set for the blind alley on coal seam #9, so gas concentration on the working face could not be monitored |
| No measurement of air volume | Ventilation team | Direct management staff | 1B2 | Unsafe conditions | Uncontrolled | No special air measurer was designated to measure air speed, air volume, etc., in the well |
| Violation of establishing false closed walls and fake drawings | Production technology Section coal mining technician | Direct management staff | 1E | Absence of safety management system | Activation | Mine leaders required workers to illegally operate in the well and formulated fake drawings to evade supervision, resulting in occurrence of the accident |
| Production safety deputy head | Mine-level management staff | 1E | Absence of safety management system | Activation | ||
| Ignorance of closed walls and fake drawings | Production technology Section coal mining technician | Direct management staff | 1B1 | Unsafe conditions | Activation | |
| Failure to implement system of mine leadership shift in well | Mine leaders on duty | Mine-level management staff | 1C2 | Unsafe act | Uncontrolled | Mine leaders failed to find or ignored underground hazards, such as violated blasting, absence of gas check, inadequate air volume, lack of methane sensor, and so on; this can be interpreted to mean that implementation failure of “mine leadership to bring staff into the well” system would increase accident risk |
| 1B2 | Unsafe conditions | Uncontrolled | ||||
| 1D2 | Bad habit of unsafe actions | Uncontrolled |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Fu, G.; Zhao, Z.; Hao, C.; Wu, Q. The Accident Path of Coal Mine Gas Explosion Based on 24Model: A Case Study of the Ruizhiyuan Gas Explosion Accident. Processes 2019, 7, 73. https://doi.org/10.3390/pr7020073
Fu G, Zhao Z, Hao C, Wu Q. The Accident Path of Coal Mine Gas Explosion Based on 24Model: A Case Study of the Ruizhiyuan Gas Explosion Accident. Processes. 2019; 7(2):73. https://doi.org/10.3390/pr7020073
Chicago/Turabian StyleFu, Gui, Ziqi Zhao, Chuanbo Hao, and Qiang Wu. 2019. "The Accident Path of Coal Mine Gas Explosion Based on 24Model: A Case Study of the Ruizhiyuan Gas Explosion Accident" Processes 7, no. 2: 73. https://doi.org/10.3390/pr7020073