




A Moderated Mediation Model of the Influence of Cynical Distrust, Medical Mistrust, and Anger on Vaccination Hesitancy in Nursing Staff

 ,
,  ,
,  and
and 
Abstract
:1. Introduction
2. Subjects and Methods
2.1. Research Design and Procedure
2.2. Ethical Considerations
2.3. Measurement Tools
2.3.1. Dimensions of Anger Reactions-5 (DAR-5)
2.3.2. Eight-Item “Cynical Distrust” Scale (CDS)
2.3.3. Vaccine Hesitancy
2.3.4. Medical Mistrust Multiformat Scale (MMMS)
2.4. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Chung, H.-Y.; Jian, M.-J.; Chang, C.-K.; Lin, J.-C.; Yeh, K.-M.; Chen, C.-W.; Hsieh, S.-S.; Hung, K.-S.; Tang, S.-H.; Perng, C.-L.; et al. Emergency SARS-CoV-2 Variants of Concern: Novel Multiplex Real-Time RT-PCR Assay for Rapid Detection and Surveillance. Microbiol. Spectr. 2022, 10, e0251321. [Google Scholar] [CrossRef] [PubMed]
- Mukhtar, S. Psychological health during the coronavirus disease 2019 pandemic outbreak. Int. J. Soc. Psychiatry 2020, 66, 512–516. [Google Scholar] [CrossRef] [PubMed]
- Tselebis, A.; Pachi, A. Primary Mental Health Care in a New Era. Healthcare 2022, 10, 2025. [Google Scholar] [CrossRef]
- Sikaras, C.; Ilias, I.; Tselebis, A.; Pachi, A.; Zyga, S.; Tsironi, M.; Gil, A.P.R.; Panagiotou, A. Nursing staff fatigue and burnout during the COVID-19 pandemic in Greece. AIMS Public Health 2022, 9, 94–105. [Google Scholar] [CrossRef]
- Pachi, A.; Sikaras, C.; Ilias, I.; Panagiotou, A.; Zyga, S.; Tsironi, M.; Baras, S.; Tsitrouli, L.A.; Tselebis, A. Burnout, Depression and Sense of Coherence in Nurses during the Pandemic Crisis. Healthcare 2022, 10, 134. [Google Scholar] [CrossRef] [PubMed]
- Pachi, A.; Anagnostopoulou, M.; Antoniou, A.; Papageorgiou, S.M.; Tsomaka, E.; Sikaras, C.; Ilias, I.; Tselebis, A. Family support, anger and aggression in health workers during the first wave of the pandemic. AIMS Public Health 2023, 10, 524–537. [Google Scholar] [CrossRef] [PubMed]
- Sikaras, C.; Zyga, S.; Tsironi, M.; Tselebis, A.; Pachi, A.; Ilias, I.; Panagiotou, A. The Mediating Role of Depression and of State Anxiety οn the Relationship between Trait Anxiety and Fatigue in Nurses during the Pandemic Crisis. Healthcare 2023, 11, 367. [Google Scholar] [CrossRef] [PubMed]
- Tselebis, A.; Lekka, D.; Sikaras, C.; Tsomaka, E.; Tassopoulos, A.; Ilias, I.; Bratis, D.; Pachi, A. Insomnia, Perceived Stress, and Family Support among Nursing Staff during the Pandemic Crisis. Healthcare 2020, 8, 434. [Google Scholar] [CrossRef] [PubMed]
- Khubchandani, J.; Bustos, E.; Chowdhury, S.; Biswas, N.; Keller, T. COVID-19 Vaccine Refusal among Nurses Worldwide: Review of Trends and Predictors. Vaccines 2022, 10, 230. [Google Scholar] [CrossRef] [PubMed]
- Ferland, L.; Carvalho, C.; Dias, J.G.; Lamb, F.; Adlhoch, C.; Suetens, C.; Beauté, J.; Kinross, P.; Plachouras, D.; Hannila-Handelberg, T.; et al. Risk of hospitalization and death for healthcare workers with COVID-19 in nine European countries, January 2020–January 2021. J. Hosp. Infect. 2022, 119, 170–174. [Google Scholar] [CrossRef]
- Gholami, M.; Fawad, I.; Shadan, S.; Rowaiee, R.; Ghanem, H.; Khamis, A.H.; Ho, S.B. COVID-19 and healthcare workers: A systematic review and meta-analysis. Int. J. Infect. Dis. 2021, 104, 335–346. [Google Scholar] [CrossRef] [PubMed]
- Gómez-Ochoa, S.A.; Franco, O.H.; Rojas, L.Z.; Raguindin, P.F.; Roa-Díaz, Z.M.; Wyssmann, B.M.; Guevara, S.L.R.; Echeverría, L.E.; Glisic, M.; Muka, T. COVID-19 in Healthcare Workers: A Living Systematic Review and Meta-analysis of Prevalence, Risk Factors, Clinical Characteristics, and Outcomes. Am. J. Epidemiol. 2021, 190, 161–175. [Google Scholar] [CrossRef] [PubMed]
- Biswas, N.; Mustapha, T.; Khubchandani, J.; Price, J.H. The Nature and Extent of COVID-19 Vaccination Hesitancy in Healthcare Workers. J. Community Health 2021, 46, 1244–1251. [Google Scholar] [CrossRef] [PubMed]
- MacDonald, N.E.; SAGE Working Group on Vaccine Hesitancy. Vaccine Hesitancy: Definition, Scope and Determinants. Vaccine 2015, 33, 4161–4164. [Google Scholar] [CrossRef]
- Paterson, P.; Meurice, F.; Stanberry, L.R.; Glismann, S.; Rosenthal, S.L.; Larson, H.J. Vaccine hesitancy and healthcare providers. Vaccine 2016, 34, 6700–6706. [Google Scholar] [CrossRef]
- Schmid, P.; Rauber, D.; Betsch, C.; Lidolt, G.; Denker, M.-L. Barriers of Influenza Vaccination Intention and Behavior—A Systematic Review of Influenza Vaccine Hesitancy, 2005–2016. PLoS ONE 2017, 12, e0170550. [Google Scholar] [CrossRef]
- Larson, H.J. Defining and measuring vaccine hesitancy. Nat. Hum. Behav. 2022, 6, 1609–1610. [Google Scholar] [CrossRef]
- Perrone, C.; Fiabane, E.; Maffoni, M.; Pierobon, A.; Setti, I.; Sommovigo, V.; Gabanelli, P. Vaccination hesitancy: To be vaccinated, or not to be vaccinated, that is the question in the era of COVID-19. Public Health Nurs. 2023, 40, 90–96. [Google Scholar] [CrossRef]
- Betsch, C.; Schmid, P.; Heinemeier, D.; Korn, L.; Holtmann, C.; Böhm, R. Beyond confidence: Development of a measure assessing the 5C psychological antecedents of vaccination. PLoS ONE 2018, 13, e0208601. [Google Scholar] [CrossRef]
- Lohiniva, A.-L.; Hussein, I.; Lehtinen, J.-M.; Sivelä, J.; Hyökki, S.; Nohynek, H.; Nuorti, P.; Lyytikäinen, O. Qualitative Insights into Vaccine Uptake of Nursing Staff in Long-Term Care Facilities in Finland. Vaccines 2023, 11, 530. [Google Scholar] [CrossRef]
- Greenglass, E.R.; Julkunen, J. Cook-Medley Hostility, Anger, and the Type a Behavior Pattern in Finland. Psychol. Rep. 1991, 68, 1059–1066. [Google Scholar] [CrossRef]
- Peterson, C.J.; Lee, B.; Nugent, K. COVID-19 Vaccination Hesitancy among Healthcare Workers—A Review. Vaccines 2022, 10, 948. [Google Scholar] [CrossRef] [PubMed]
- Jennings, W.; Stoker, G.; Valgarðsson, V.; Devine, D.; Gaskell, J. How trust, mistrust and distrust shape the governance of the COVID-19 crisis. J. Eur. Public Policy 2021, 28, 1174–1196. [Google Scholar] [CrossRef]
- Sanford, K.; Clifton, M. The Medical Mistrust Multiformat Scale: Links with vaccine hesitancy, treatment adherence, and patient–physician relationships. Psychol. Assess. 2022, 34, 10–20. [Google Scholar] [CrossRef] [PubMed]
- Khuller, D. Why Are So Many Health-Care Workers Resisting the COVID Vaccine? The New Yorker. Available online: https://www.newyorker.com/science/medical-dispatch/why-are-so-many-health-care-workers-resisting-the-covid-vaccine (accessed on 2 February 2021).
- Featherstone, J.D.; Zhang, J. Feeling angry: The effects of vaccine misinformation and refutational messages on negative emotions and vaccination attitude. J. Health Commun. 2020, 25, 692–702. [Google Scholar] [CrossRef] [PubMed]
- Deffenbacher, J.L.; Oetting, E.R.; Lynch, R.S.; Morris, C.D. The expression of anger and its consequences. Behav. Res. Ther. 1996, 34, 575–590. [Google Scholar] [CrossRef] [PubMed]
- Lerner, J.S.; Keltner, D. Fear, anger, and risk. J. Pers. Soc. Psychol. 2001, 81, 146–159. [Google Scholar] [CrossRef] [PubMed]
- Bushman, B.J.; Baumeister, R.F.; Phillips, C.M. Phillips. Do people aggress to improve their mood? Catharsis beliefs, affect regulation opportunity, and aggressive responding. J. Pers. Soc. Psychol. 2001, 81, 17–32. [Google Scholar] [CrossRef] [PubMed]
- Leigh, J.P.; Moss, S.J.; White, T.M.; Picchio, C.A.; Rabin, K.H.; Ratzan, S.C.; Wyka, K.; El-Mohandes, A.; Lazarus, J.V. Factors affecting COVID-19 vaccine hesitancy among healthcare providers in 23 countries. Vaccine 2022, 40, 4081–4089. [Google Scholar] [CrossRef] [PubMed]
- Kim, H.J.; Lee, D.H.; Kim, J.H.; Kang, S.-E. Validation of the Dimensions of Anger Reactions Scale (the DAR-5) in non-clinical South Korean adults. BMC Psychol. 2023, 11, 74. [Google Scholar] [CrossRef]
- Forbes, D.; Alkemade, N.; Hopcraft, D.; Hawthorne, G.; O’halloran, P.; Elhai, J.D.; McHugh, T.; Bates, G.; Novaco, R.W.; Bryant, R.; et al. Evaluation of the Dimensions of Anger Reactions-5 (DAR-5) Scale in combat veterans with posttraumatic stress disorder. J. Anxiety Disord. 2014, 28, 830–835. [Google Scholar] [CrossRef]
- Pachi, A.; Kavourgia, E.; Bratis, D.; Fytsilis, K.; Papageorgiou, S.M.; Lekka, D.; Sikaras, C.; Tselebis, A. Anger and Aggression in Relation to Psychological Resilience and Alcohol Abuse among Health Professionals during the First Pandemic Wave. Healthcare 2023, 11, 2031. [Google Scholar] [CrossRef] [PubMed]
- Everson, S.A.; Kauhanen, J.; Kaplan, G.A.; Goldberg, D.E.; Julkunen, J.; Tuomilehto, J.; Salonen, J.T. Hostility and Increased Risk of Mortality and Acute Myocardial Infarction: The Mediating Role of Behavioral Risk Factors. Am. J. Epidemiol. 1997, 146, 142–152. [Google Scholar] [CrossRef]
- Christensen, U.; Lund, R.; Damsgaard, M.T.; Holstein, B.E.; Ditlevsen, S.; Diderichsen, F.; Due, P.; Iversen, L.; Lynch, J. Cynical Hostility, Socioeconomic Position, Health Behaviors, and Symptom Load: A Cross-Sectional Analysis in a Danish Population-Based Study. Psychosom. Med. 2004, 66, 572–577. [Google Scholar] [CrossRef]
- Anagnostopoulou, T.; Kioseoglou, G. Cynical distrust scale [in modern greek]. In Psychometric Tools in Greece [In Modern Greek]; Stalikas, A., Triliva, S., Roussi, P., Eds.; Ellinika Grammata: Athens, Greece, 2000; pp. 295–296. [Google Scholar]
- Hayes, A.F. PROCESS: A Versatile Computational Tool for Observed Variable Mediation, Moderation, and Conditional Process Modeling [White Paper]. 2012. Available online: http://www.afhayes.com/public/process2012.pdf (accessed on 25 August 2023).
- Hayes, A.F. An Index and Test of Linear Moderated Mediation. Multivar. Behav. Res. 2015, 50, 1–22. [Google Scholar] [CrossRef]
- Hayes, A.F. Introduction to Mediation, Moderation, and Conditional Process Analysis: A Regression-Based Approach, 3rd ed.; The Guilford Press: New York, NY, USA, 2022. [Google Scholar]
- Nazlı, B.; Yığman, F.; Sevindik, M.; Özturan, D.D. Psychological factors affecting COVID-19 vaccine hesitancy. Ir. J. Med. Sci. 2021, 191, 71–80. [Google Scholar] [CrossRef]
- Kim, H.J.; Kim, E.; Han, D.H. Effect of psychological factors on COVID-19 vaccine hesitancy. J. Public Health 2023, 45, e522–e531. [Google Scholar] [CrossRef] [PubMed]
- Shacham, M.; Hamama-Raz, Y.; Ben-Ezra, M.; Levin, Y. Association between COVID-19 and Seasonal Influenza Vaccines to Vaccine Hesitancy, Intolerance of Uncertainty and Mental Health. Vaccines 2023, 11, 403. [Google Scholar] [CrossRef] [PubMed]
- McNeil, A.; Purdon, C. Anxiety disorders, COVID-19 fear, and vaccine hesitancy. J. Anxiety Disord. 2022, 90, 102598. [Google Scholar] [CrossRef]
- Dubé, E.; Vivion, M.; E MacDonald, N. Vaccine hesitancy, vaccine refusal and the anti-vaccine movement: Influence, impact and implications. Expert Rev. Vaccines 2015, 14, 99–117. [Google Scholar] [CrossRef] [PubMed]
- Peretti-Watel, P.; Raude, J.; Sagaon-Teyssier, L.; Constant, A.; Verger, P.; Beck, F. Attitudes toward vaccination and the H1N1 vaccine: Poor people’s unfounded fears or legitimate concerns of the elite? Soc. Sci. Med. 2014, 109, 10–18. [Google Scholar] [CrossRef] [PubMed]
- Chou, W.-Y.S.; Budenz, A. Considering Emotion in COVID-19 Vaccine Communication: Addressing Vaccine Hesitancy and Fostering Vaccine Confidence. Health Commun. 2020, 35, 1718–1722. [Google Scholar] [CrossRef]
- Dasch, S.; Wachinger, J.; Bärnighausen, T.; Chen, S.; McMahon, S.A. Deliberation, context, emotion and trust – understanding the dynamics of adults’ COVID-19 vaccination decisions in Germany. BMC Public Health 2023, 23, 136. [Google Scholar] [CrossRef]
- Liu, S.; Chu, H. Examining the direct and indirect effects of trust in motivating COVID-19 vaccine uptake. Patient Educ. Couns. 2022, 105, 2096–2102. [Google Scholar] [CrossRef]
- Simione, L.; Vagni, M.; Gnagnarella, C.; Bersani, G.; Pajardi, D. Mistrust and Beliefs in Conspiracy Theories Differently Mediate the Effects of Psychological Factors on Propensity for COVID-19 Vaccine. Front. Psychol. 2021, 12, 683684. [Google Scholar] [CrossRef] [PubMed]
- Lazarus, R.S. Cognition and motivation in emotion. Am. Psychol. 1991, 46, 352. [Google Scholar] [CrossRef] [PubMed]
- Smith, C.A.; Ellsworth, P.C. Patterns of cognitive appraisal in emotion. J. Pers. Soc. Psychol. 1985, 48, 813. [Google Scholar] [CrossRef]
- Galanis, P.; Moisoglou, I.; Vraka, I.; Siskou, O.; Konstantakopoulou, O.; Katsiroumpa, A.; Kaitelidou, D. Predictors of COVID-19 Vaccine Uptake in Healthcare Workers: A cross-sectional study in Greece. J. Occup. Environ. Med. 2022, 64, e191–e196. [Google Scholar] [CrossRef]
- Bell, S.; Clarke, R.M.; Ismail, S.A.; Ojo-Aromokudu, O.; Naqvi, H.; Coghill, Y.; Donovan, H.; Letley, L.; Paterson, P.; Mounier-Jack, S. COVID-19 vaccination beliefs, attitudes, and behaviours among health and social care workers in the UK: A mixed-methods study. PLoS ONE 2022, 17, e0260949. [Google Scholar] [CrossRef]
- Galanis, P.; Katsiroumpa, A.; Vraka, I.; Siskou, O.; Konstantakopoulou, O.; Katsoulas, T.; Kaitelidou, D. Seasonal Influenza Vaccine Intention among Nurses Who Have Been Fully Vaccinated against COVID-19: Evidence from Greece. Vaccines 2023, 11, 159. [Google Scholar] [CrossRef]
- Tram, K.H.; Saeed, S.; Bradley, C.; Fox, B.; Eshun-Wilson, I.; Mody, A.; Geng, E. Deliberation, Dissent, and Distrust: Understanding Distinct Drivers of Coronavirus Disease 2019 Vaccine Hesitancy in the United States. Clin. Infect. Dis. 2022, 74, 1429–1441. [Google Scholar] [CrossRef] [PubMed]
- Holford, D.L.; Fasce, A.; Costello, T.H.; Lewandowsky, S. Psychological profiles of anti-vaccination argument endorsement. Sci. Rep. 2023, 13, 11219. [Google Scholar] [CrossRef]
- Miyazaki, K.; Uchiba, T.; Tanaka, K.; Sasahara, K. Aggressive behaviour of anti-vaxxers and their toxic replies in English and Japanese. Humanit. Soc. Sci. Commun. 2022, 9, 229. [Google Scholar] [CrossRef]
- Chapleau, R.R. Toward Understanding Genetic Risk of Burnout through Genome-wide Associations of Cynicism and Cynical Distrust. medRxiv 2023. [Google Scholar] [CrossRef]
- van der Wath, A.; van Wyk, N. A hermeneutic literature review to conceptualise altruism as a value in nursing. Scand. J. Caring Sci. 2020, 34, 575–584. [Google Scholar] [CrossRef]
- Dozois, D.J.A.; Beck, A.T. Cognitive schemas, beliefs and assumptions. In Risk Factors in Depression; Dobson, K.S., Dozois, D.J.A., Eds.; Elsevier/Academic Press: Oxford, UK, 2008; pp. 121–143. [Google Scholar]
- Nabi, R.L. A Cognitive-Functional Model for the Effects of Discrete Negative Emotions on Information Processing, Attitude Change, and Recall. Commun. Theory 1999, 9, 292–320. [Google Scholar] [CrossRef]
- Walter, N.; Tukachinsky, R.; Pelled, A.; Nabi, R. Meta-Analysis of Anger and Persuasion: An Empirical Integration of Four Models. J. Commun. 2019, 69, 73–93. [Google Scholar] [CrossRef]
- Freeman, D.; Loe, B.S.; Chadwick, A.; Vaccari, C.; Waite, F.; Rosebrock, L.; Jenner, L.; Petit, A.; Lewandowsky, S.; Vanderslott, S.; et al. COVID-19 vaccine hesitancy in the UK: The Oxford coronavirus explanations, attitudes, and narratives survey (Oceans) II. Psychol. Med. 2022, 52, 3127–3141. [Google Scholar] [CrossRef]
- Loewenstein, G.; Lerner, J.S. The role of affect in decision making. In Handbook of Affective Science; Davidson, R., Scherer, K., Goldsmith, H., Eds.; Oxford University Press: New York, NY, USA, 2003; pp. 619–642. [Google Scholar]
- Vuong, L.; Bidwell, J.T.; Apesoa-Varano, E.C.; Cothran, F.A.; Catz, S.L. COVID-19 vaccine hesitancy and intent in California registered nurses. Vaccine X 2022, 11, 100162. [Google Scholar] [CrossRef] [PubMed]
- Zintel, S.; Flock, C.; Arbogast, A.L.; Forster, A.; von Wagner, C.; Sieverding, M. Gender differences in the intention to get vaccinated against COVID-19: A systematic review and meta-analysis. J. Public Health 2022, 31, 1303–1327. [Google Scholar] [CrossRef] [PubMed]
- Dror, A.A.; Eisenbach, N.; Taiber, S.; Morozov, N.G.; Mizrachi, M.; Zigron, A.; Srouji, S.; Sela, E. Vaccine hesitancy: The next challenge in the fight against COVID-19. Eur. J. Epidemiol. 2020, 35, 775–779. [Google Scholar] [CrossRef] [PubMed]
- Gołębiowska, J.; Zimny-Zając, A.; Dróżdż, M.; Makuch, S.; Dudek, K.; Mazur, G.; Agrawal, S. Evaluation of the Approach towards Vaccination against COVID-19 among the Polish Population—In Relation to Sociodemographic Factors and Physical and Mental Health. Vaccines 2023, 11, 700. [Google Scholar] [CrossRef]
- Muscatello, M.R.A.; Bruno, A.; Carroccio, C.; Cedro, C.; La Torre, D.; Di Rosa, A.E.; Zoccali, R.; Aragona, M.; La Torre, F.; Mattei, A.; et al. Association between Burnout and Anger in Oncology versus Ophthalmology Health Care Professionals. Psychol. Rep. 2006, 99, 641–650. [Google Scholar] [CrossRef]
- Ersoy-Kart, M. Relations Among Social Support, Burnout, and Experiences of Anger: An Investigation Among Emergency Nurses. Nurs. Forum 2009, 44, 165–174. [Google Scholar] [CrossRef]
- Galanis, P.; Katsiroumpa, A.; Sourtzi, P.; Siskou, O.; Konstantakopoulou, O.; Katsoulas, T.; Kaitelidou, D. COVID-19-Related Burnout and Intention of Fully Vaccinated Individuals to Get a Booster Dose: The Mediating Role of Resilience. Vaccines 2023, 11, 62. [Google Scholar] [CrossRef]
- Siegler, A.J.; Luisi, N.; Hall, E.W.; Bradley, H.; Sanchez, T.; Lopman, B.A.; Sullivan, P.S. Trajectory of COVID-19 Vaccine Hesitancy Over Time and Association of Initial Vaccine Hesitancy with Subsequent Vaccination. JAMA Netw. Open 2021, 4, e2126882. [Google Scholar] [CrossRef] [PubMed]
- Sato, R. Vaccine hesitancy against COVID-19 vaccine over time in Nigeria. Vaccine 2023, 41, 2749–2753. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
{kind=link}
| Participants | Age | Work Experience (in Years) | COVID-19 Vaccine Hesitancy | H1N1 Vaccine Hesitancy | Medical Mistrust Multiformat Scale | Cynical Distrust Scale | Dimensions of Anger Reactions | Total Vaccine Hesitancy | |
|---|---|---|---|---|---|---|---|---|---|
| Men N = 66 | Mean | 45.53 | 19.26 | 3.36 | 2.48 | 19.97 | 22.58 ** | 10.35 * | 5.85 |
| S. D | 10.96 | 11.89 | 1.58 | 1.56 | 5.65 | 6.53 | 3.18 | 2.84 | |
| Women N = 321 | Mean | 43.04 | 17.78 | 3.62 | 2.72 | 20.73 | 24.96 ** | 11.48 * | 6.33 |
| S. D | 10.99 | 12.09 | 1.27 | 1.47 | 5.43 | 6.10 | 3.96 | 2.42 | |
| Total N = 387 | Mean | 43.46 | 18.03 | 3.58 ** | 2.68 ** | 20.60 | 24.55 | 11.29 | 6.25 |
| S. D | 11.011 | 12.05 | 1.33 | 1.49 | 5.47 | 6.23 | 3.86 | 2.50 | |
| In the Next Flu Shot (H1N1) Recommendation, Would You Get Vaccinated? | If a New Shot Dose Were Recommended as an Adjunct to the Current Vaccination Schedule for COVID-19, Would You Get Vaccinated? | |||
|---|---|---|---|---|
| Frequency | Percent | Frequency | Percent | |
| I would definitely get vaccinated | 125 | 32.3% | 38 | 9.8% |
| I would probably get vaccinated | 68 | 17.6% | 51 | 13.2% |
| I’m not sure | 68 | 17.6% | 77 | 19.9% |
| I probably wouldn’t get vaccinated | 59 | 15.2% | 92 | 23.8% |
| I definitely wouldn’t get vaccinated | 67 | 17.3% | 129 | 33.3% |
| Total | 387 | 100% | 387 | 100% |
| Pearson Correlation N = 387 | Age | Work Experience (in Years) | COVID-19 Vaccine Hesitancy | H1N1 Vaccine Hesitancy | MMMS | CDS | DAR | |
|---|---|---|---|---|---|---|---|---|
| Work experience (in years) | r | 0.878 ** | ||||||
| COVID-19 vaccine hesitancy | r | −0.035 | −0.020 | |||||
| H1N1 vaccine hesitancy | r | −0.030 | −0.023 | 0.571 ** | ||||
| Medical Mistrust Multiformat Scale (MMMS) | r | −0.179 ** | −0.125 * | 0.249 ** | 0.180 ** | |||
| Cynical Distrust Scale (CDS) | r | −0.140 ** | −0.110 * | 0.203 ** | 0.207 ** | 0.408 ** | ||
| Dimensions of Anger Reactions (DAR) | r | −0.063 | −0.051 | 0.197 ** | 0.208 ** | 0.384 ** | 0.453 ** | |
| Total Vaccine Hesitancy | r | −0.036 | −0.024 | 0.872 ** | 0.899 ** | 0.240 ** | 0.231 ** | 0.229 ** |
| Dependent Variable: Total Vaccine Hesitancy | R Square | R Square Change | Beta | t | p | VIF | Durbin–Watson |
|---|---|---|---|---|---|---|---|
| Medical Mistrust Multiformat Scale | 0.058 | 0.058 | 0.146 | 2.651 | 0.01 * | 1.27 | 1.957 |
| Dimensions of Anger Reactions | 0.079 | 0.022 | 0.119 | 2.114 | 0.05 ** | 1.34 | |
| Cynical Distrust Scale | 0.090 | 0.010 | 0.118 | 2.065 | 0.05 ** | 1.37 |
| Variable | b | SE | t | p | 95% Confidence Interval | |
|---|---|---|---|---|---|---|
| LLCI | ULCI | |||||
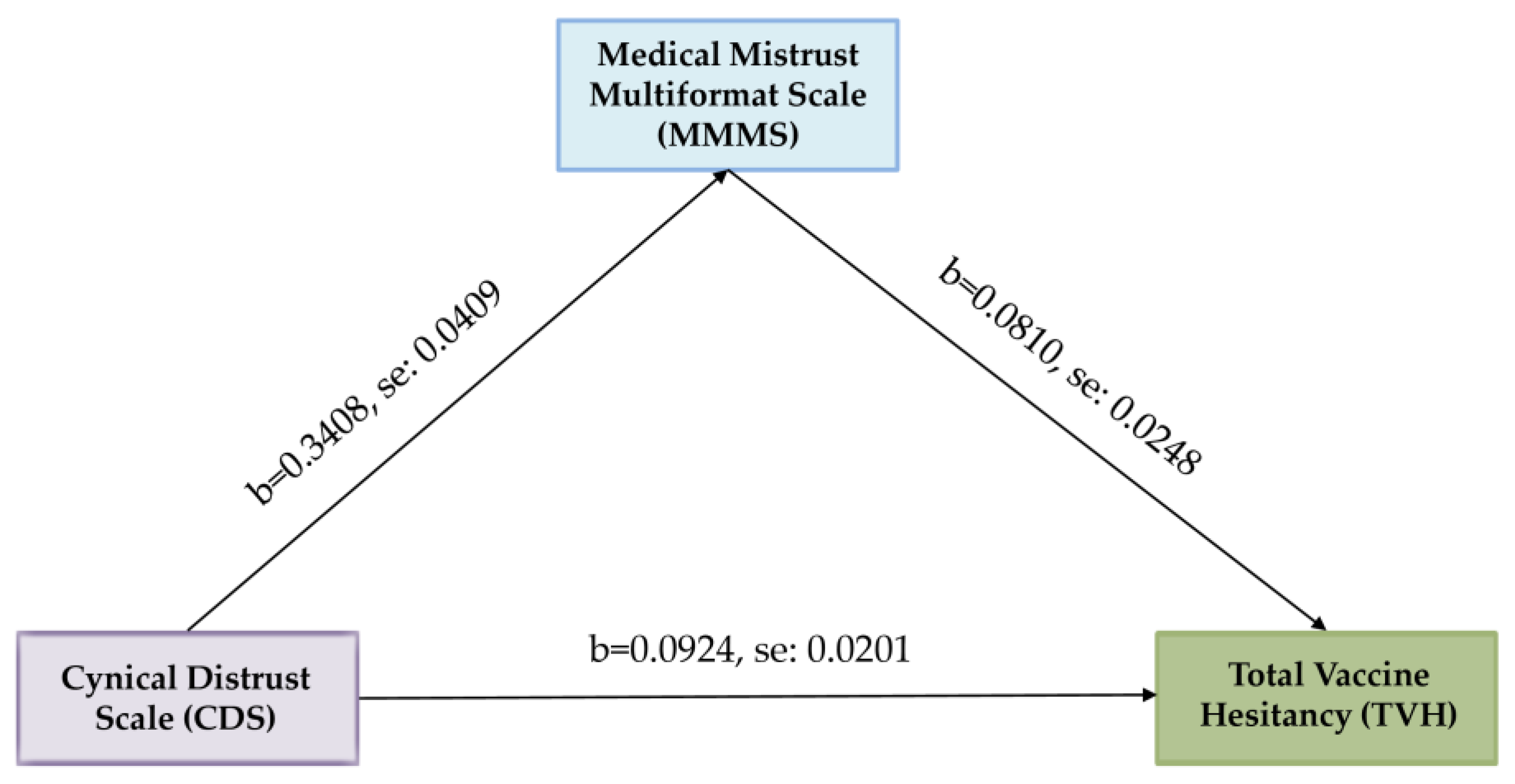
| CDS → MMMS | 0.3408 | 0.0409 | 8.3313 | 0.0000 | 0.2603 | 0.4212 |
| CDS → TVH | 0.0924 | 0.0201 | 4.5889 | 0.0000 | 0.0528 | 0.1320 |
| CDS → MMMS → TVH | 0.0810 | 0.0248 | 3.2594 | 0.0012 | 0.0321 | 0.1298 |
| Effects | ||||||
| Direct | 0.0648 | 0.0216 | 2.9983 | 0.0029 | 0.0223 | 0.1073 |
| Indirect * | 0.0276 | 0.0093 | 2.9677 | 0.0097 | 0.0470 | |
| Total | 0.0924 | 0.0201 | 4.5889 | 0.0000 | 0.0528 | 0.1320 |
| Direct Relationships | ||||||
|---|---|---|---|---|---|---|
| Variable | b | SE | t | p | 95% Confidence Interval | |
| LLCI | ULCI | |||||
| CDS → MMMS | 0.5875 | 0.1126 | 5.2155 | 0.0000 | 0.3660 | 0.8090 |
| CDS → TVH | 0.0642 | 0.0215 | 2.9867 | 0.0030 | 0.0219 | 0.1065 |
| MMMS → TVH | 0.0798 | 0.0245 | 3.2544 | 0.0012 | 0.0316 | 0.1280 |
| CDS*DAR → MMMS | −0.0318 | 0.0100 | −3.1800 | 0.0016 | −0.0515 | -0.0121 |
| Indirect Relationships | ||||||
| Effects | ||||||
| Direct | 0.0642 | 0.0215 | 2.9867 | 0.0030 | 0.0219 | 0.1065 |
| Indirect | 0.0182 | 0.0067 | 2.7164 | 0.0064 | 0.0322 | |
| Probing Moderated Indirect Relationships | ||||||
| Low Level of DAR | 0.0280 | 0.0097 | 2.8866 | 0.0101 | 0.0479 | |
| High Level of DAR | 0.0084 | 0.0058 | 1.4482 | −0.0017 | 0.0210 | |
| Index of Moderated Mediation | −0.0025 | 0.0011 | 2.2727 | -0.0051 | −0.0006 | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tselebis, A.; Sikaras, C.; Milionis, C.; Sideri, E.P.; Fytsilis, K.; Papageorgiou, S.M.; Ilias, I.; Pachi, A. A Moderated Mediation Model of the Influence of Cynical Distrust, Medical Mistrust, and Anger on Vaccination Hesitancy in Nursing Staff. Eur. J. Investig. Health Psychol. Educ. 2023, 13, 2373-2387. https://doi.org/10.3390/ejihpe13110167
Tselebis A, Sikaras C, Milionis C, Sideri EP, Fytsilis K, Papageorgiou SM, Ilias I, Pachi A. A Moderated Mediation Model of the Influence of Cynical Distrust, Medical Mistrust, and Anger on Vaccination Hesitancy in Nursing Staff. European Journal of Investigation in Health, Psychology and Education. 2023; 13(11):2373-2387. https://doi.org/10.3390/ejihpe13110167
Chicago/Turabian StyleTselebis, Athanasios, Christos Sikaras, Charalampos Milionis, Eleni Paraskevi Sideri, Konstantinos Fytsilis, Styliani Maria Papageorgiou, Ioannis Ilias, and Argyro Pachi. 2023. "A Moderated Mediation Model of the Influence of Cynical Distrust, Medical Mistrust, and Anger on Vaccination Hesitancy in Nursing Staff" European Journal of Investigation in Health, Psychology and Education 13, no. 11: 2373-2387. https://doi.org/10.3390/ejihpe13110167
APA StyleTselebis, A., Sikaras, C., Milionis, C., Sideri, E. P., Fytsilis, K., Papageorgiou, S. M., Ilias, I., & Pachi, A. (2023). A Moderated Mediation Model of the Influence of Cynical Distrust, Medical Mistrust, and Anger on Vaccination Hesitancy in Nursing Staff. European Journal of Investigation in Health, Psychology and Education, 13(11), 2373-2387. https://doi.org/10.3390/ejihpe13110167