Trajectories of Depressive Individual Symptoms over Time during Transcranial Photobiomodulation

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Intervention
2.3. Statistical Analyses
3. Results
3.1. Patient Disposition and Characteristics
3.2. Persistent Baseline Symptoms
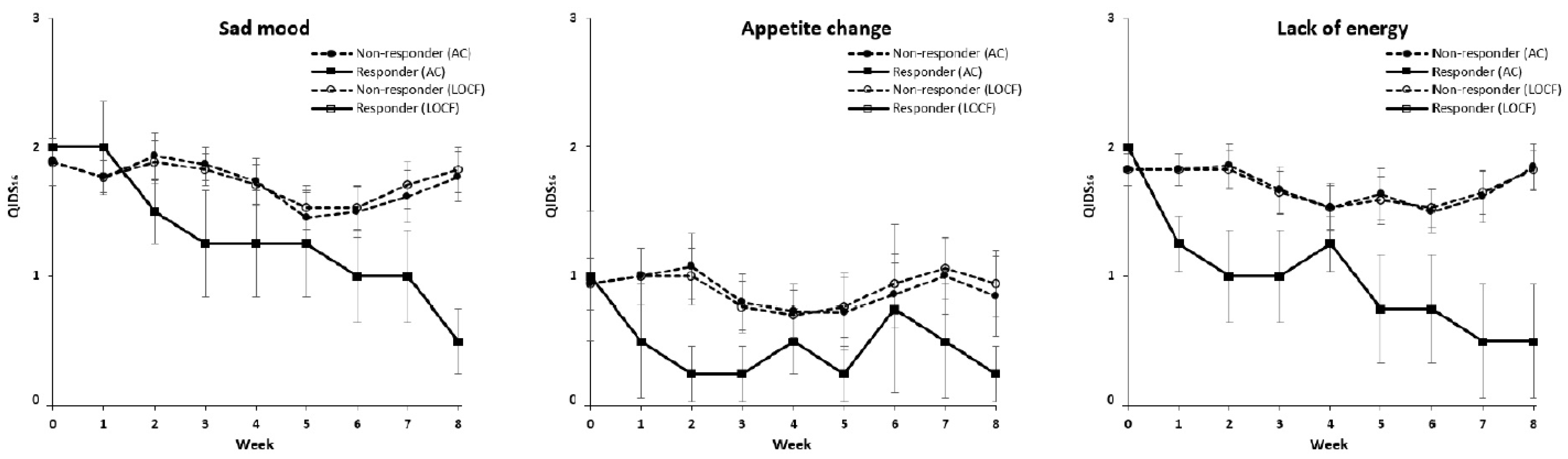
3.3. Trajectories of Individual Symptoms over Time during t-PBM
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Sakurai, H.; Noma, H.; Watanabe, K.; Uchida, H.; Furukawa, T. Cumulative Remission Rate after Sequential Treatments in Depression: Reappraisal of the STAR*D Trial Data. World Psychiatry, 2023; in press. [Google Scholar]
- Sharma, T.; Guski, L.S.; Freund, N.; Meng, D.M.; Gøtzsche, P.C. Drop-out Rates in Placebo-Controlled Trials of Antidepressant Drugs: A Systematic Review and Meta-Analysis Based on Clinical Study Reports. Int. J. Risk Saf. Med. 2019, 30, 217–232. [Google Scholar] [CrossRef]
- Lee, M.-S.; Lee, H.-Y.; Kang, S.-G.; Yang, J.; Ahn, H.; Rhee, M.; Ko, Y.-H.; Joe, S.-H.; Jung, I.-K.; Kim, S.-H. Variables Influencing Antidepressant Medication Adherence for Treating Outpatients with Depressive Disorders. J. Affect. Disord. 2010, 123, 216–221. [Google Scholar] [CrossRef] [PubMed]
- Barrett, B.; Byford, S.; Knapp, M. Evidence of Cost-Effective Treatments for Depression: A Systematic Review. J. Affect. Disord. 2005, 84, 1–13. [Google Scholar] [CrossRef] [PubMed]
- Cuijpers, P.; van Straten, A.; Schuurmans, J.; van Oppen, P.; Hollon, S.D.; Andersson, G. Psychotherapy for Chronic Major Depression and Dysthymia: A Meta-Analysis. Clin. Psychol. Rev. 2010, 30, 51–62. [Google Scholar] [CrossRef] [PubMed]
- Andrade, C.; Arumugham, S.S.; Thirthalli, J. Adverse Effects of Electroconvulsive Therapy. Psychiatr. Clin. N. Am. 2016, 39, 513–530. [Google Scholar] [CrossRef] [PubMed]
- Ma, H.; Du, Y.; Xie, D.; Wei, Z.Z.; Pan, Y.; Zhang, Y. Recent Advances in Light Energy Biotherapeutic Strategies with Photobiomodulation on Central Nervous System Disorders. Brain Res. 2023, 1822, 148615. [Google Scholar] [CrossRef]
- Iosifescu, D.V.; Collins, K.A.; Hurtado-Puerto, A.; Irvin, M.K.; Clancy, J.A.; Sparpana, A.M.; Sullivan, E.F.; Parincu, Z.; Ratai, E.-M.; Funes, C.J.; et al. Grant Report on the Transcranial near Infrared Radiation and Cerebral Blood Flow in Depression (TRIADE) Study. Photonics 2023, 10, 90. [Google Scholar] [CrossRef]
- Maiello, M.; Losiewicz, O.M.; Bui, E.; Spera, V.; Hamblin, M.R.; Marques, L.; Cassano, P. Transcranial Photobiomodulation with Near-Infrared Light for Generalized Anxiety Disorder: A Pilot Study. Photobiomodul. Photomed. Laser Surg. 2019, 37, 644–650. [Google Scholar] [CrossRef]
- Schiffer, F.; Johnston, A.L.; Ravichandran, C.; Polcari, A.; Teicher, M.H.; Webb, R.H.; Hamblin, M.R. Psychological Benefits 2 and 4 Weeks after a Single Treatment with near Infrared Light to the Forehead: A Pilot Study of 10 Patients with Major Depression and Anxiety. Behav. Brain Funct. 2009, 5, 46. [Google Scholar] [CrossRef]
- Cassano, P.; Petrie, S.R.; Mischoulon, D.; Cusin, C.; Katnani, H.; Yeung, A.; De Taboada, L.; Archibald, A.; Bui, E.; Baer, L.; et al. Transcranial Photobiomodulation for the Treatment of Major Depressive Disorder. The ELATED-2 Pilot Trial. Photomed. Laser Surg. 2018, 36, 634–646. [Google Scholar] [CrossRef] [PubMed]
- Uher, R.; Maier, W.; Hauser, J.; Marusic, A.; Schmael, C.; Mors, O.; Henigsberg, N.; Souery, D.; Placentino, A.; Rietschel, M.; et al. Differential Efficacy of Escitalopram and Nortriptyline on Dimensional Measures of Depression. Br. J. Psychiatry 2009, 194, 252–259. [Google Scholar] [CrossRef] [PubMed]
- Sakurai, H.; Uribe, S.; Cirillo, P.; Fuertes-Saiz, A.; Camprodon, J.A.; Barbour, T. Residual Symptoms after Achieving Remission with Repetitive Transcranial Magnetic Stimulation in Depression. J. Affect. Disord. 2022, 301, 154–161. [Google Scholar] [CrossRef] [PubMed]
- Sakurai, H.; Uchida, H.; Abe, T.; Nakajima, S.; Suzuki, T.; Pollock, B.G.; Sato, Y.; Mimura, M. Trajectories of Individual Symptoms in Remitters versus Non-Remitters with Depression. J. Affect. Disord. 2013, 151, 506–513. [Google Scholar] [CrossRef] [PubMed]
- Sakurai, H.; Suzuki, T.; Yoshimura, K.; Mimura, M.; Uchida, H. Predicting Relapse with Individual Residual Symptoms in Major Depressive Disorder: A Reanalysis of the STAR*D Data. Psychopharmacology 2017, 234, 2453–2461. [Google Scholar] [CrossRef] [PubMed]
- Iosifescu, D.V.; Norton, R.J.; Tural, U.; Mischoulon, D.; Collins, K.; McDonald, E.; De Taboada, L.; Foster, S.; Cusin, C.; Yeung, A.; et al. Very Low-Level Transcranial Photobiomodulation for Major Depressive Disorder: The ELATED-3 Multicenter, Randomized, Sham-Controlled Trial. J. Clin. Psychiatry 2022, 83, 21m14226. [Google Scholar] [CrossRef] [PubMed]
- Terman, M.; Terman, J.S. Light Therapy for Seasonal and Nonseasonal Depression: Efficacy, Protocol, Safety, and Side Effects. CNS Spectr. 2005, 10, 647–663. [Google Scholar] [CrossRef]
- Van Maanen, A.; Meijer, A.M.; van der Heijden, K.B.; Oort, F.J. The Effects of Light Therapy on Sleep Problems: A Systematic Review and Meta-Analysis. Sleep Med. Rev. 2016, 29, 52–62. [Google Scholar] [CrossRef]
- Dowling, G.A.; Graf, C.; Hubbard, E.M.; Luxenberg, J.S. Light Treatment for Neuropsychiatric Behaviors in Alzheimer’s Disease. West. J. Nurs. Res. 2007, 29, 961–975. [Google Scholar] [CrossRef]
- Ostrin, L.A. Ocular and Systemic Melatonin and the Influence of Light Exposure. Clin. Exp. Optom. 2019, 102, 99–108. [Google Scholar] [CrossRef]
- De Freitas, L.F.; Hamblin, M.R. Proposed Mechanisms of Photobiomodulation or Low-Level Light Therapy. IEEE J. Sel. Top. Quantum. Electron. 2016, 22, 7000417. [Google Scholar] [CrossRef] [PubMed]
- Hamblin, M.R. Mechanisms and Mitochondrial Redox Signaling in Photobiomodulation. Photochem. Photobiol. 2018, 94, 199–212. [Google Scholar] [CrossRef] [PubMed]
- Askalsky, P.; Iosifescu, D.V. Transcranial Photobiomodulation for The Management of Depression: Current Perspectives. Neuropsychiatr. Dis. Treat. 2019, 15, 3255–3272. [Google Scholar] [CrossRef] [PubMed]
- Xu, Z.; Guo, X.; Yang, Y.; Tucker, D.; Lu, Y.; Xin, N.; Zhang, G.; Yang, L.; Li, J.; Du, X.; et al. Low-Level Laser Irradiation Improves Depression-like Behaviors in Mice. Mol. Neurobiol. 2017, 54, 4551–4559. [Google Scholar] [CrossRef]
- Karu, T.I. Mitochondrial Signaling in Mammalian Cells Activated by Red and Near-IR Radiation. Photochem. Photobiol. 2008, 84, 1091–1099. [Google Scholar] [CrossRef] [PubMed]
- Li, Y.; Jin, H.; Chen, Y.; Huang, T.; Mi, Y.; Zou, Z. Cancer Cachexia: Molecular Mechanism and Pharmacological Management. Biochem. J. 2021, 478, 1663–1688. [Google Scholar] [CrossRef]
- Li, L.; Shen, J.J.; Bournat, J.C.; Huang, L.; Chattopadhyay, A.; Li, Z.; Shaw, C.; Graham, B.H.; Brown, C.W. Activin Signaling: Effects on Body Composition and Mitochondrial Energy Metabolism. Endocrinology 2009, 150, 3521–3529. [Google Scholar] [CrossRef]
- Rezin, G.T.; Cardoso, M.R.; Gonçalves, C.L.; Scaini, G.; Fraga, D.B.; Riegel, R.E.; Comim, C.M.; Quevedo, J.; Streck, E.L. Inhibition of Mitochondrial Respiratory Chain in Brain of Rats Subjected to an Experimental Model of Depression. Neurochem. Int. 2008, 53, 395–400. [Google Scholar] [CrossRef]
- Hartmann, C.; Kempf, A. Mitochondrial Control of Sleep. Curr. Opin. Neurobiol. 2023, 81, 102733. [Google Scholar] [CrossRef]
- Chen, J.-B.; Li, M.-J.; Huo, X.-H.; Gong, T.-J.; Han, X.; Liu, J.-H.; Liu, S.; Sun, Y.-S. Ginsenoside Rg5 Improves Sleep by Regulating Energy Metabolism in Sleep-Deprived Rats. Am. J. Chin. Med. 2023, 51, 1845–1864. [Google Scholar] [CrossRef]
- Lutfy, R.H.; Salam, S.A.; Mohammed, H.S.; Shakweer, M.M.; Essawy, A.E. Photomodulatory Effects in the Hypothalamus of Sleep-Deprived Young and Aged Rats. Behav. Brain Res. 2024, 458, 114731. [Google Scholar] [CrossRef]
- Fried, E.I.; Epskamp, S.; Nesse, R.M.; Tuerlinckx, F.; Borsboom, D. What Are “good” Depression Symptoms? Comparing the Centrality of DSM and Non-DSM Symptoms of Depression in a Network Analysis. J. Affect. Disord. 2016, 189, 314–320. [Google Scholar] [CrossRef]
- Sueki, A.; Suzuki, E.; Takahashi, H.; Ishigooka, J. Does Early Improvement in Depressive Symptoms Predict Subsequent Remission in Patients with Depression Who Are Treated with Duloxetine? Neuropsychiatr. Dis. Treat. 2016, 12, 1269–1273. [Google Scholar] [CrossRef]
- Faries, D.; Herrera, J.; Rayamajhi, J.; DeBrota, D.; Demitrack, M.; Potter, W.Z. The Responsiveness of the Hamilton Depression Rating Scale. J. Psychiatr. Res. 2000, 34, 3–10. [Google Scholar] [CrossRef] [PubMed]
- Nierenberg, A.A.; Husain, M.M.; Trivedi, M.H.; Fava, M.; Warden, D.; Wisniewski, S.R.; Miyahara, S.; Rush, A.J. Residual Symptoms after Remission of Major Depressive Disorder with Citalopram and Risk of Relapse: A STAR*D Report. Psychol. Med. 2010, 40, 41–50. [Google Scholar] [CrossRef] [PubMed]
- Fried, E.I.; Nesse, R.M. Depression Sum-Scores Don’t Add up: Why Analyzing Specific Depression Symptoms Is Essential. BMC Med. 2015, 13, 72. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
| Characteristics | Responders (n = 4) | Non-Responders (n = 17) |
|---|---|---|
| Age in years, mean ± SD | 47.3 ± 16.5 | 38.4 ± 15.5 |
| Gender, female, n (%) | 4 (100.0%) | 13 (76.5%) |
| Race, n (%) | ||
| White | 3 (75.0%) | 14 (82.4%) |
| Asian | 1 (25.0%) | 2 (11.8%) |
| Black | 0 (0.0%) | 1 (5.9%) |
| Ethnicity, n (%) | ||
| Hispanic or Latino | 0 (0.0%) | 1 (5.9%) |
| Not Hispanic or Latino | 3 (75.0%) | 14 (82.4%) |
| Not specified | 1 (25.0%) | 2 (11.8%) |
| HAM-D17, mean ± SD | 21.5 ± 3.3 | 19.9 ± 2.9 |
| QIDS, mean ± SD | 14.0 ± 2.1 | 14.9 ± 2.7 |
| Symptom at Baseline | Symptom at Endpoint among Those Who Had It at Baseline | |
|---|---|---|
| Sleep onset insomnia | 71.4% (15/21) | 73.3% (11/15) |
| Mid-nocturnal insomnia | 71.4% (15/21) | 86.7% (13/15) |
| Early morning insomnia | 42.9% (9/21) | 33.3% (3/9) |
| Hypersomnia | 47.6% (10/21) | 30.0% (3/10) |
| Sad mood | 100.0% (21/21) | 90.5% (19/21) |
| Appetite change | 61.9% (13/21) | 46.2% (6/13) |
| Weight change | 66.7% (14/21) | 57.1% (8/14) |
| Concentration/decision making | 90.5% (19/21) | 73.7% (14/19) |
| Negative self-view | 85.7% (18/21) | 72.2% (13/18) |
| Suicidal ideation | 57.1% (12/21) | 75.0% (9/12) |
| Reduced involvement | 95.2% (20/21) | 85.0% (17/20) |
| Lack of energy | 100.0% (21/21) | 85.7% (18/21) |
| Slowing down | 47.6% (10/21) | 30.0% (3/10) |
| Restlessness | 52.4% (11/21) | 72.7% (8/11) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Urata, M.; Cassano, P.; Norton, R.; Sylvester, K.M.; Watanabe, K.; Iosifescu, D.V.; Sakurai, H. Trajectories of Depressive Individual Symptoms over Time during Transcranial Photobiomodulation. Photonics 2023, 10, 1324. https://doi.org/10.3390/photonics10121324
Urata M, Cassano P, Norton R, Sylvester KM, Watanabe K, Iosifescu DV, Sakurai H. Trajectories of Depressive Individual Symptoms over Time during Transcranial Photobiomodulation. Photonics. 2023; 10(12):1324. https://doi.org/10.3390/photonics10121324
Chicago/Turabian StyleUrata, Minoru, Paolo Cassano, Richard Norton, Katelyn M. Sylvester, Koichiro Watanabe, Dan V. Iosifescu, and Hitoshi Sakurai. 2023. "Trajectories of Depressive Individual Symptoms over Time during Transcranial Photobiomodulation" Photonics 10, no. 12: 1324. https://doi.org/10.3390/photonics10121324
APA StyleUrata, M., Cassano, P., Norton, R., Sylvester, K. M., Watanabe, K., Iosifescu, D. V., & Sakurai, H. (2023). Trajectories of Depressive Individual Symptoms over Time during Transcranial Photobiomodulation. Photonics, 10(12), 1324. https://doi.org/10.3390/photonics10121324