Abstract
Objective visual quality evaluation using optical human eye models with actual eye aberration characteristics provides an important reference for clinical vision diagnosis and treatment. To ensure accurate evaluation, it is typically necessary to precisely introduce eye aberrations into the eye model by adjusting the model’s surface shape. However, the detailed relationship between eye aberrations and surface shapes is unclear, causing challenges in aberration introduction. In this paper, a method that enables the accurate introduction of target aberrations into an eye model for objective visual quality evaluation is proposed. The eye aberrations generated by the model’s surface are analyzed based on optical nodal aberration theory. The aberration calculation formulas are proposed and proved by a design example. Using the proposed method, the objective visual quality evaluation is conducted for the patients who underwent refractive surgery. The clinically measured postoperative eye aberrations are accurately introduced into the eye model with an error of less than 1.0 × 10−4 μm. The objective visual evaluation results are consistent with the statistical results of clinical contrast sensitivity tests. With the proposed method, it is expected to aid in clinical visual quality testing and assess the effect of refractive correction.
1. Introduction
The objective human visual quality reflects the imaging performance of the human eye as an optical system, excluding the influence of subjective perception. The objective visual quality evaluation provides an objective reference for clinical subjective vision tests and serves as a basis for judging the effectiveness of refractive correction. In clinical vision therapy, especially, ensuring the accuracy of objective visual evaluation is a fundamental prerequisite.
Optical human eye models are simplified versions of the human eye, based on mathematical and physical principles. They are designed to present the basic optical properties and simulate the actual behavior of a human eye and are widely used in ophthalmology and engineering [1,2]. For example, the optical human eye model could be utilized to predict human vision for objective visual evaluation through the retinal image quality of the eye model [1,2]. It has been well known that human eye aberration has a strong impact on visual quality. Therefore the overall level of the eye aberrations, such as root mean square of wavefront error (RMS WFE), can be directly used to assess human vision in some cases [3]. In addition, the aberration characteristics of human eyes are complicated, and the interaction between different eye aberrations can cause eyes with similar RMS WFEs to exhibit different visual qualities [4,5,6,7]. Considering the influence of aberrations on human vision, to accurately evaluate the visual quality with eye models, the aberrations of the models should be consistent with those measured through the actual human eye as much as possible. Navarro [8] proposed a schematic eye with four aspheric surfaces, introducing experimental measurements of the cornea and lens into the classic anatomy-based Gullstrand-Le Grand eye model [9]. Using this model, the experimentally observed average spherical aberration was predicted without any shape fitting. Subsequently, by adjusting the retinal surface shape, a wide-angle model was obtained [10], and its Seidel aberration had a good agreement with the experimental data. Liou and Brennan [11] achieved the prediction of spherical and chromatic aberrations by introducing a gradient-index lens. The obtained schematic eye model can be used to incorporate irregular surfaces to assess image quality functions in individual eyes. Polans [12] combined the newly acquired aberration data with the model using a reverse building technique and constructed a schematic model that shows excellent agreement with the measured data across the entire field of view. In addition to the schematic eye model that reflects the average aberrations of the human eye, there are critical scenarios where it is necessary to completely and accurately incorporate the target aberrations into the model, such as evaluating the impact of aberrations on human vision or building an individualized model. In this case, the surface shape of the model is typically changed to a more complex form, such as a freeform surface, thereby increasing the model’s flexibility in adjusting aberrations. Tabernero [13] set the posterior surface of the crystalline lens as an “irregular” surface to modify the astigmatic coefficient. Liu [14] set the anterior and posterior surfaces of the lens as Zernike freeform surfaces, so as to accurately introduce the clinically measured aberrations into the individualized eye models for further analysis.
Although freeform surfaces can enhance the eye model’s ability to modify aberrations, they also lead to complex relations between eye aberrations and the eye model’s surface shapes. Typically, when the surface shape changes (such as changing the polynomial term of the freeform surface), the eye model will generate multiple aberrations at the same time. This makes accurate visual quality evaluation much harder by way of introducing the aberration into eye models precisely. In such cases, researchers may choose the local optimization function based on the damping least squares (DLS) algorithm integrated into optical design software to introduce target aberrations into the eye model. However, due to the inherent limitation of the DLS method (getting easily trapped in local minima within a multidimensional variable space [15]), this optimization task will heavily rely on design experience [16,17], such as the setting of reasonable design starting points, optimization variables, and constraints. This can lead to insufficient accuracy in the aberration’s introduction and the distortion of the surface shapes, seriously affecting the efficiency of eye model construction. Therefore, it is crucial to clarify the relationship between eye aberrations and the model’s surface shape, so as to introduce the target aberration into the eye model with high precision and efficiency. Unfortunately, there are currently no reports on the detailed relationship between eye aberrations and the surface shape of the eye model.
This paper proposes a method enabling the accurate introduction of target aberrations into an eye model for objective evaluation of visual quality. We represent the surfaces of the eye model as Zernike freeform surfaces and quantitatively analyze the eye aberrations caused by the Zernike terms within the framework of optical nodal aberration theory (NAT). The calculation formulas of eye aberrations are derived, and their correctness is demonstrated through design examples. According to the derived formulas, a high-precision iterative method to introduce eye aberrations into the eye model is proposed. Using the proposed method, we evaluate the objective visual quality of patients undergoing refractive surgery. The clinically measured postoperative eye aberrations are accurately introduced into the eye model, and the introduced error is less than 1.0 × 10−4 μm. The objective visual quality of postoperative eyes is evaluated based on the image quality of constructed eye models. Through visual evaluation, the effect of visual improvement between two clinical refractive surgeries, the Small Incision lenticule Extraction (SMILE) and wavefront-guided Laser-Assisted in Situ Keratomileusis (WFG LASIK), is compared in some postoperative patients. The objective visual evaluation results are consistent with the clinical contrast sensitivity tests, proving the effectiveness of the proposed method.
2. Theory and Methods
2.1. Eye Aberrations Generated by Surface of Eye Model
In this section, the complex surface shapes of the eye model are expressed as freeform surfaces, represented by non-rotationally symmetric orthogonal Zernike polynomials. Nodal aberration theory (NAT) is used to analyze the relationship between the freeform surface and the aberrations in the eye model. NAT is an aberration theoretical framework applicable to rotationally asymmetric optical systems, and it supports the calculation of the aberration contribution of Zernike terms on freeform surfaces [17,18,19,20]. To accurately modulate the aberrations in the eye model, the main refractive elements, such as the cornea or lens surface, are typically modified into freeform surfaces. In the eye model system, these surfaces are positioned away from the aperture stop. According to NAT, when light beams of different field points illuminate the freeform surface away from the stop, the shape of the light beam on the surface is shown in Figure 1.
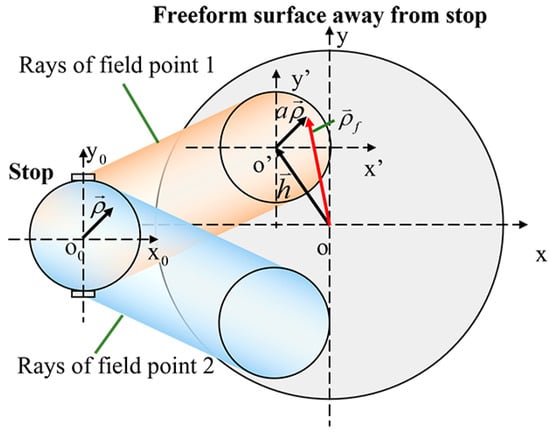
Figure 1.
The light beam of different field points irradiates the freeform surface away from the stop.
In this case, the wave aberration generated by the Zernike terms on this non-stop freeform surface is calculated by [20],
where n and n′ are the refractive index before and after the surface, respectively. λ is the wavelength of the reference light and is the coefficient of the ith Zernike term . is the vector-form normalized aperture coordinate of the freeform surface. As the aberrations are generally fitted to the exit pupil plane, should be transformed into the normalized pupil vector, . For the scaling factor, , denotes the marginal ray height on the freeform surface and is the normalized radius of the freeform surface. is the pupil shift vector, starting from the surface vertex and ending at the intersection of the chief ray with the surface, normalized by . reflects the center of the shift beam footprint. and can be obtained through ray tracing in optical software.
According to Equation (1), when a Zernike term with coefficient is added to the model’s freeform surface, the generated aberration is,
where and k is the order of Zernike term. Equation (2) can be expanded in Cartesian coordinates with a horizontal component and a vertical component, that is,
Typically, clinical eye aberrations are represented by Zernike polynomials recommended by the Optical Society of America (OSA) [21]. To clarify the eye aberrations generated by each Zernike term on the model’s freeform surface, Equation (3) can first be expanded into XY polynomials and then recombined into the clinical OSA Zernike polynomials, as shown in Equation (4),
where is the ith XY term, with the coefficient , they can be written as the multiplication of two vectors including a vector G containing the XY terms and a vector containing the corresponding coefficients. Similarly, is the jth clinical OSA Zernike term, with the coefficient . is the vector containing the clinical OSA Zernike terms. is the corresponding coefficient vector that is required to be calculated. The polynomials up to the 4th order are,
According to Equations (4)–(6), the coefficients of the clinical Zernike aberrations can be obtained by,
Based on Equation (7), the eye aberrations generated by Zernike terms without the first 3 terms that do not affect the image quality are presented in Figure 2, where . The Zernike terms used to represent the model’s freeform surface are listed in Equation (8), which follows the standard order inherent in the optical software CODE V [22].
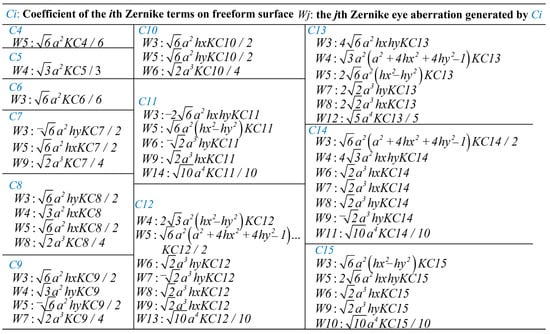
Figure 2.
Eye aberrations generated by Zernike terms on the eye model’s freeform surface.
Figure 2 shows that a single Zernike freeform surface term can generate multiple eye aberrations, rather than just generate a single eye aberration with the expression consistent with this term. To verify the proposed formulas in Figure 2, the Liou–Brennan schematic eye model is built. As an example, the anterior corneal surface is defined as a Zernike freeform surface, and an aberration introduction test is performed. The model is shown in Figure 3, with a wavelength of 555 nm, and the test field of view is (0, −5°), which is typically the angle between the visual axis and optical axis of the human eye. The 4th–15th Zernike terms with a coefficient of 0.1λ are added to the anterior corneal surface simultaneously. The generated eye aberrations calculated using the proposed formulas are considered the theoretical values, and the aberrations read from the software are the actual values. The comparison between the theoretical values and the actual values is shown in Figure 4. The result shows good agreement between the two values, with a maximum relative error of 9.4%. The reason for this error lies in the approximation characteristics of NAT. NAT defaults to rays propagating along the local Z-axis without deviation after passing through the freeform surface, thereby realizing the expression of aberrations as theoretical formulas [17,19]. Therefore, this theory inevitably produces calculation errors while achieving aberration prediction. But overall, the theoretical values are basically consistent with the actual values. In addition, for tasks such as introducing aberrations into the model, this error can be significantly reduced through iterative calculations, which we will explain in the following sections.
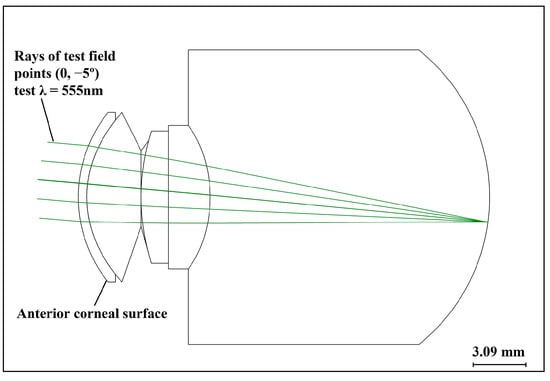
Figure 3.
Schematic diagram of Liou–Brennan eye model, with a test wavelength of 555 nm and a test field point of (0, −5°).
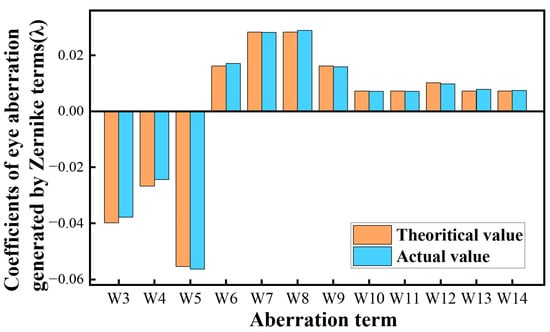
Figure 4.
Comparison between the theoretical eye aberrations calculated using the proposed formulas and the actual values.
2.2. Iterative Method to Accurately Introduce Eye Aberrations into the Eye Model
Based on the formulas in Figure 2, through rearranging and deriving, the sets of Zernike terms that generate each specific eye aberration without introducing others can be obtained, as shown in Figure 5. Using the formulas in Figure 5, designers can control the surface shape of the eye model to independently generate any desired eye aberration in an analytic way, without solely relying on optimization algorithms and design experience.
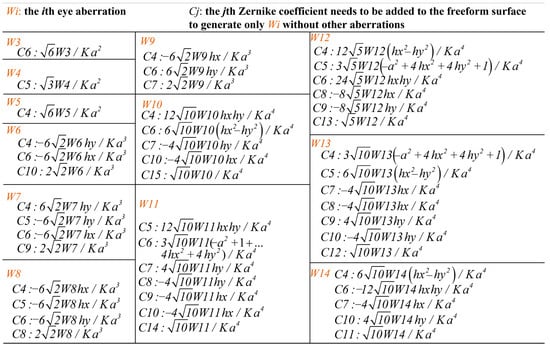
Figure 5.
Sets of Zernike terms that generate each specific eye aberration without others.
On this basis, a high-precision method to introduce the eye aberration into the eye model is proposed, the flowchart is shown in Figure 6. This method takes the target eye aberration that needs to be introduced as the input, denoted by W_tar. W_tar can be predefined or measured clinically from the actual patient’s eyes. Then according to W_tar, the coefficients of Zernike terms Z_coe can be calculated using the proposed formulas in Figure 5. The calculated Z_coe is added to the corresponding surface of the eye model, then the actual aberrations of the model, denoted by W_act, can be read through software. We define the aberration introduction error as
when does not meet the target error , we take the unintroduced residual eye aberration, that is, the difference between W_tar and W_act, as the new W_tar, and perform the next iteration. This process continues until is lower than , and the final human eye model is output. And the further objective visual evaluation can be conducted based on the final eye model. Through the application programming interface between Code V and MATLAB, this iterative process can be performed automatically.
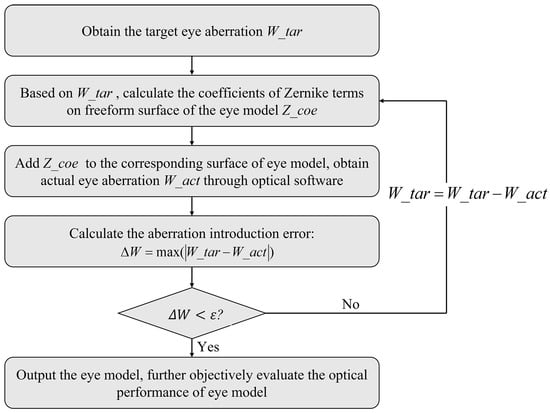
Figure 6.
Flowchart of the aberration introduction method.
3. Objective Visual Quality Evaluation of Patients Undergoing Refractive Surgery Using the Proposed Method
Refractive surgery removes defocus and astigmatism to improve human vision; however, the postoperative residual high-order aberrations affect visual quality [23,24,25,26]. In this section, we use the proposed method to accurately introduce the statistical residual high-order aberrations into eye models to evaluate the objective visual quality of postoperative patients. We first obtained the statistical eye aberration data from patients who underwent two different types of surgical procedures: the Small Incision lenticule Extraction (SMILE) and wavefront-guided Laser-Assisted in Situ Keratomileusis (WFG LASIK). The patients received refractive surgery at Tianjin Eye Hospital. All patients had no intraoperative and postoperative ocular complications. This clinical research protocol complied with the Declaration of Helsinki and was approved by the Ethics Committee of Tianjin Eye Hospital.
The patients were divided into two groups according to the type of surgery they underwent: 12 people (24 eyes) in the group SMILE, and 18 people (36 eyes) in the group WFG LASIK. Their wavefront aberrations are measured using a Hartmann–Shack aberrometer (iDESIGN; Johnson & Johnson Vision, Irvine, CA, USA), the two groups have a similar RMS of high-order aberration (HOAs). The clinical average vertical coma , horizontal coma , primary spherical aberration , and statistical HOAs are shown in Table 1.

Table 1.
Clinically measured postoperative eye aberrations of the two surgeries.
Using the proposed method, we apply the basic structure parameters of the Liou–Brennan eye model in Figure 3 to construct the postoperative SMILE eye and postoperative WFG LASIK eye, each containing the aberrations in Table 1. The anterior corneal surface is set as a Zernike freeform surface to introduce W_tar. The target error is 1.0 × 10−4 μm. The aberration introduction errors of the two models are calculated by . In comparison, another method, denoted by the compared method, is presented. The compared method ignores the effect of multiple eye aberrations generated by a single Zernike term (as shown in Figure 2) and assumes that a term generates only one aberration whose expression matches this term. For model SMILE and model WFG LASIK, the comparison between the aberration introduction errors of the two methods after each iteration are shown in Figure 7a,c, where Er_proposed and Er_compared are the errors of the proposed method and the compared method, respectively. After the fourth iteration, the error of the proposed method meets the target, while the error of the comparison method remains at least two orders of magnitude above the target.
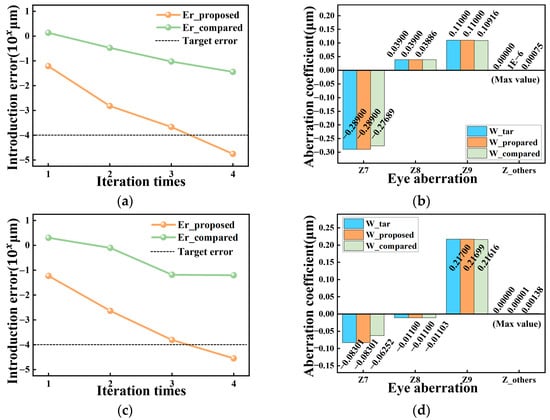
Figure 7.
(a) Aberration-introduced calculation error of the proposed method and the compared method for model SMILE; (b) eye aberrations of the model SMILE in terms of the target value, the actual value introduced by the proposed method, and by the compared method; (c) aberration-introduced calculation error of the proposed method and the compared method for model WFG LASIK; (d) eye aberrations of the model WFG LASIK in terms of the target value, the actual value introduced by the proposed method, and by the compared method.
The aberrations contained In the two models output by the proposed and compared methods after the fourth iteration are shown in Figure 7b,d, where W_tar is the target eye aberrations to be introduced and W_proposed and W_compared denote the actual eye aberrations contained in the models constructed by the two methods, respectively. The models output by the proposed method accurately introduce the target eye aberrations while avoiding interference from other aberrations. However, the aberrations of the models constructed by the comparison method deviate from the target, especially Z7. These results demonstrate the high accuracy and effectiveness of the proposed method.
On this basis, the image quality of the postoperative eye models can be used to objectively evaluate the visual quality of the postoperative eyes. Figure 8a shows the spot diagrams of the two eye models and the MTFs of the models within the spatial frequency of 0–60 cycles/mm and their respective Strehl Ratio (SR). The spot size of the WFG LASIK model is slightly larger than that of the SMILE model, but its SR and MTF across most of the spatial frequency range (0–50.5 c/mm) are significantly better. Therefore, it can be concluded that for these postoperative samples, WFG LASIK has a greater improvement in visual quality than SMILE. As further proof, a clinical contrast sensitivity test was conducted for these patients (with CSV-1000E, Vector vision, Inc. the illumination mesopic environment is 3 candelas/m2). Statistical data can avoid the subjective intervention of individual patients. Additionally, the statistical test result generated by CSV-1000E is presented in Figure 8b, showing that the contrast sensitivity of the WFG LASIK group is better than that of group SMILE. This suggests, from a clinical perspective, that for these patients, the postoperative residual aberrations from SMILE have a more negative impact on visual improvement than WFG LASIK. This result is consistent with the objective evaluation using eye models, further proving the effectiveness of the proposed aberration-introduction method.
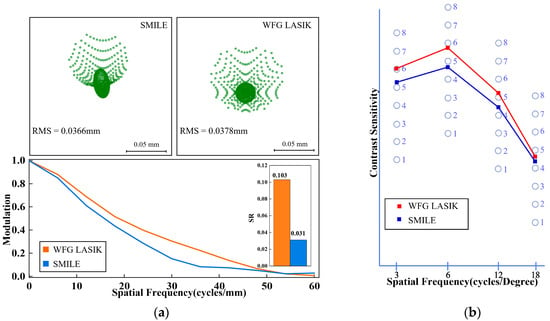
Figure 8.
(a) Spot diagrams, MTFs, and Strehl Ratio of model SMILE and model WFG LASIK; (b) contrast sensitivity of postoperative patients generated by CSV-1000E.
4. Conclusions and Discussion
This paper proposes a method for precisely introducing target aberrations into an eye model to objectively evaluate visual quality. The eye aberrations generated by the model’s freeform surface terms are quantitatively analyzed within the framework of NAT. The aberration calculation formulas are proposed and proved through design examples. A high-precision iterative method to introduce eye aberrations into the eye model is designed. Using the proposed method, the objective visual qualities of patients undergoing refractive surgery are evaluated. The postoperative eye aberrations of these patients are measured and introduced into the eye model with significantly high precision and the introduced error is less than 1.0 × 10−4 μm. The objective visual quality is evaluated based on the image quality of the constructed eye models. On this basis, we compare the effects on visual improvement between two clinical refractive surgeries, SMILE and WFG LASIK, for these selected patients. The objective visual quality evaluation results are consistent with the clinical statistical contrast sensitivity tests, proving the effectiveness of the proposed method.
This paper describes the detailed relationship between the surface shape of the human eye model and eye aberrations. In the experiment, we precisely introduced the postoperative residual aberration into the eye model by manipulating the shape of the anterior corneal surface. In fact, the proposed method enables control of eye aberrations by adjusting any surface of the eye model, not just the cornea, such as defining the lens surface as a freeform surface to construct a personalized model. In addition, here we focus on the control of the single-field aberration to evaluate the human visual quality, because typically only the single-field (gazing point) eye aberration is measured clinically. However, there may be situations where multi-field aberrations are measured and multi-field aberrations need to be introduced into the eye model. This can be regarded as an optimization task, which requires a reasonable starting point to produce the optimal results. In this case, similar to our previous research [17], the NAT-based formulas in this paper can guide the construction of an eye model surface to generate a reasonable starting point, making the optimization easier to converge. Furthermore, this paper compares the visual improvement effects of refractive surgeries in some patients. This work will serve as a basis for further research with a larger sample to explore the generalizability of the differences in surgical outcomes. We hope that this study can provide insights into the construction of different types of eye models, thus aiding in clinical visual quality testing and assessing the effects of refractive correction.
Author Contributions
Conceptualization, S.Z.; methodology, S.Z.; software, X.Z. (Xing Zhao); validation, S.Z. and X.Z. (Xinheng Zhao); formal analysis, D.L.; investigation, S.Z. and X.Z. (Xinheng Zhao); resources, X.Z. (Xing Zhao), L.Z. and Y.W.; data curation, X.Z. (Xinheng Zhao); writing—original draft preparation, S.Z.; writing—review and editing, X.Z. (Xing Zhao) and L.Z.; visualization, D.L.; supervision, X.Z. (Xing Zhao) and Y.W.; project administration, X.Z. (Xing Zhao), L.Z. and Y.W.; funding acquisition, X.Z. (Xing Zhao), L.Z. and Y.W. All authors have read and agreed to the published version of the manuscript.
Funding
This research was funded by the National Natural Science Foundation of China (NSFC) (62075106, 62475122, 82301255), the Nankai University Eye Institute (NKYKD202204, NKYKK202205, NKYKK202209), the Fundamental Research Funds for the Central Universities, Nankai University (63241331), and the Tianjin Key Medical Discipline (Specialty) Construction Project (No. TJYXZDXK-016A).
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki, and approved by the Ethics Committee of Tianjin Eye Hospital.
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
Data are contained within the article.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Atchison, D.A.; Thibos, L.N. Optical models of the human eye. Clin. Exp. Optom. 2016, 99, 99–106. [Google Scholar] [CrossRef] [PubMed]
- Esteve-Taboada, J.J.; Montes-Mico, R.; Ferrer-Blasco, T. Schematic eye models to mimic the behavior of the accommodating human eye. J. Cataract Refract. Surg. 2018, 44, 627–641. [Google Scholar] [CrossRef] [PubMed]
- Marsack, J.D.; Thibos, L.N.; Applegate, R.A. Metrics of optical quality derived from wave aberrations predict visual performance. J. Vis. 2004, 4, 322–328. [Google Scholar] [CrossRef] [PubMed]
- Villegas, E.A.; Alcon, E.; Artal, P. Impact of positive coupling of the eye’s trefoil and coma in retinal image quality and visual acuity. J. Opt. Soc. Am. A 2012, 29, 1667–1672. [Google Scholar] [CrossRef] [PubMed]
- Niu, S.; Shen, J.; Liao, W.; Liang, C.; Zhang, Y. Study on linear conjugated combination of Zernike modes. Chin. Opt. Lett. 2013, 11, 022201–022203. [Google Scholar] [CrossRef][Green Version]
- Hu, C.; Ravikumar, A.; Hastings, G.D.; Marsack, J.D. Visual interaction of 2nd to 5th order Zernike aberration terms with vertical coma. Ophthalmic Physiol. Opt. 2020, 40, 669–679. [Google Scholar] [CrossRef]
- de Gracia, P.; Dorronsoro, C.; Gambra, E.; Marin, G.; Hernandez, M.; Marcos, S. Combining coma with astigmatism can improve retinal image over astigmatism alone. Vision Res. 2010, 50, 2008–2014. [Google Scholar] [CrossRef]
- Navarro, R.; Santamaría, J.; Bescós, J. Accommodation-dependent model of the human eye with aspherics. J. Opt. Soc. Am. A 1985, 2, 1273–1280. [Google Scholar] [CrossRef]
- El Hage, S.G.; Le Grand, Y. Physiological Optics; Springer: Berlin/Heidelberg, Germany, 1980; pp. 64–66. [Google Scholar]
- Escudero-Sanz, I.; Navarro, R. Off-axis aberrations of a wide-angle schematic eye model. J. Opt. Soc. Am. A 1999, 16, 1881–1891. [Google Scholar] [CrossRef]
- Liou, H.L.; Brennan, N.A. Anatomically accurate, finite model eye for optical modeling. J. Opt. Soc. Am. A 1997, 14, 1684–1695. [Google Scholar] [CrossRef]
- Polans, J.; Jaeken, B.; McNabb, R.P.; Artal, P.; Izatt, J.A. Wide-field optical model of the human eye with asymmetrically tilted and decentered lens that reproduces measured ocular aberrations. Optica 2015, 2, 124–134. [Google Scholar] [CrossRef]
- Tabernero, J.; Kallamata, E.; Velonias, G.; Vera-Diaz, F.A. Individualized modeling for the peripheral optics of the human myopic eye. Biomed. Opt. Express 2023, 14, 2726–2735. [Google Scholar] [CrossRef] [PubMed]
- Liu, Y.; Li, X.; Zhang, L.; Yi, X.; Xing, Y.; Li, K.; Wang, Y. Comparison of wavefront aberrations in the object and image spaces using wide-field individual eye models. Biomed. Opt. Express 2022, 13, 4939–4953. [Google Scholar] [CrossRef] [PubMed]
- Zhao, S.; Wu, H.; Ye, H.; Hu, J.; Hu, M.; Zhang, X. A Multi-Objective Local Optimization Method for Imaging Optical Systems. Photonics 2023, 10, 1218. [Google Scholar] [CrossRef]
- Bauer, A.; Schiesser, E.M.; Rolland, J.P. Starting geometry creation and design method for freeform optics. Nat. Commun. 2018, 9, 1756. [Google Scholar] [CrossRef]
- Zhang, S.; Zhao, X.; Li, D.; Feng, H.; Zhao, S.; Wang, L.; Zhang, X. High-precision analysis of aberration contribution of Zernike freeform surface terms for non-zero field of view. Opt. Express 2024, 32, 3167–3183. [Google Scholar] [CrossRef]
- Fuerschbach, K.; Rolland, J.P.; Thompson, K.P. Theory of aberration fields for general optical systems with freeform surfaces. Opt. Express 2014, 22, 26585–26606. [Google Scholar] [CrossRef]
- Yang, T.; Zhu, J.; Jin, G. Nodal aberration properties of coaxial imaging systems using Zernike polynomial surfaces. J. Opt. Soc. Am. A 2015, 32, 822–836. [Google Scholar] [CrossRef]
- Yang, T.; Cheng, D.; Wang, Y. Aberration analysis for freeform surface terms overlay on general decentered and tilted optical surfaces. Opt. Express 2018, 26, 7751–7770. [Google Scholar] [CrossRef]
- Thibos, L.N.; Applegate, R.A.; Schwiegerling, J.T.; Webb, R. Standards for reporting the optical aberrations of eyes. J. Refract. Surg. 2002, 18, S652–S660. [Google Scholar] [CrossRef]
- Synopsys Inc. Code V Reference Manual; Synopsys Inc.: Sunnyvale, CA, USA, 2012. [Google Scholar]
- Kim, T.I.; Alio Del Barrio, J.L.; Wilkins, M.; Cochener, B.; Ang, M. Refractive surgery. Lancet 2019, 393, 2085–2098. [Google Scholar] [CrossRef] [PubMed]
- Gulmez, M.; Tekce, A.; Kamis, U. Comparison of refractive outcomes and high-order aberrations after small incision lenticule extraction and wavefront-guided femtosecond-assisted laser in situ keratomileusis for correcting high myopia and myopic astigmatism. Int. Ophthalmol. 2020, 40, 3481–3489. [Google Scholar] [CrossRef] [PubMed]
- Zhao, X.; Zhang, L.; Ma, J.; Li, M.; Zhang, J.; Zhao, X.; Wang, Y. Comparison of Wavefront-Guided Femtosecond LASIK and Optimized SMILE for Correction of Moderate-to-High Astigmatism. J. Refract. Surg. 2021, 37, 166–173. [Google Scholar] [CrossRef] [PubMed]
- He, X.Y.; He, Q.; Yuan, M.J.; Fang, Z.; Zhang, K.; Zhu, T.P.; Han, W. Evaluation of morphological features: Femtosecond-LASIK flap vs. SMILE cap, and the effects on corneal higher-order aberrations. Graefes Arch. Clin. Exp. Ophthalmol. 2022, 260, 3993–4003. [Google Scholar] [CrossRef]








Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).