Validation of a White Light and Fluorescence Augmented Panoramic Endoscopic Imaging System on a Bimodal Bladder Wall Experimental Model

 , , ,
, , ,  and
and 
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
1. Introduction
2. Materials and Methods
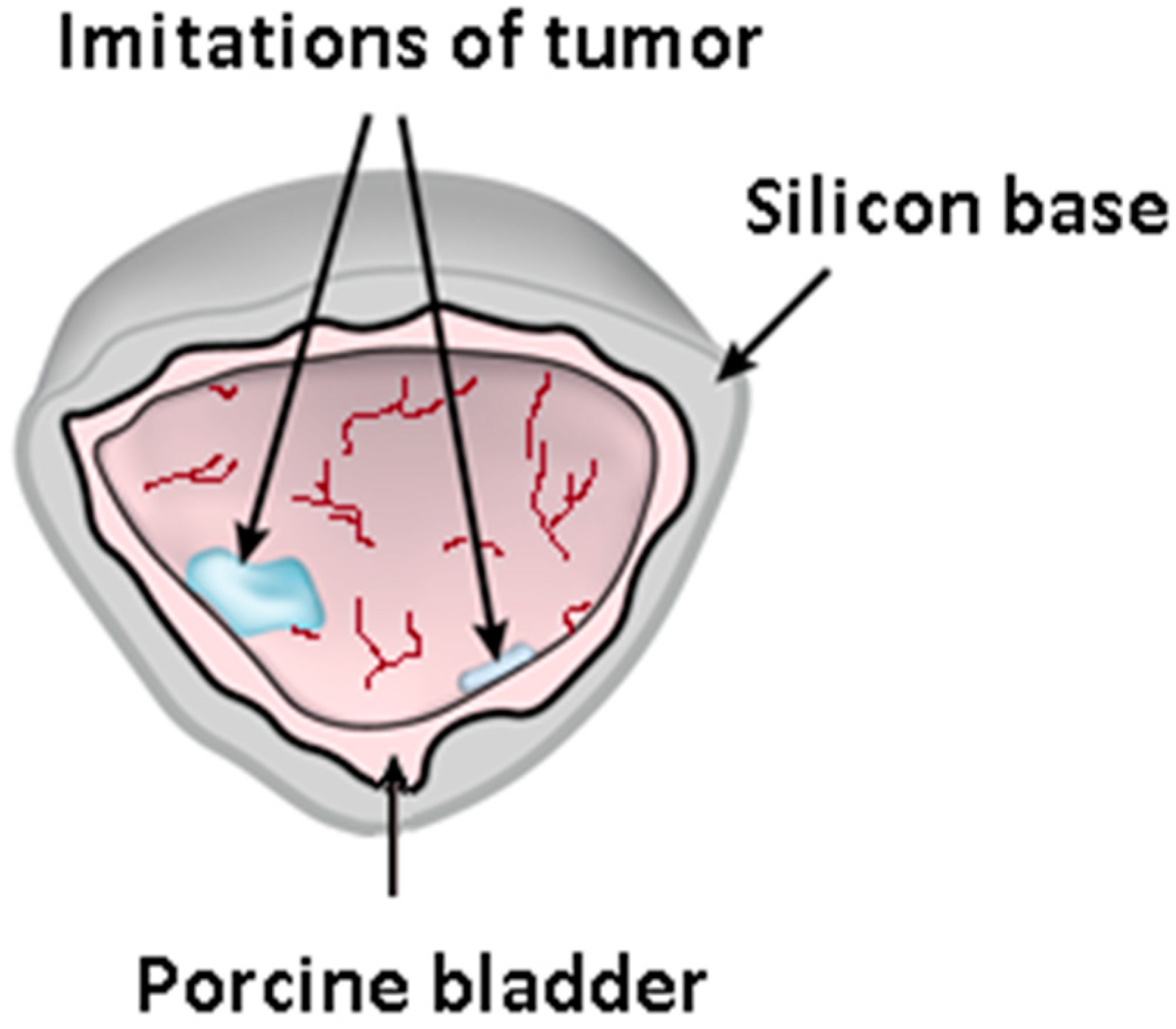
2.1. Three-Dimensional Phantom of the Bladder Wall
2.2. Bimodal Endoscopic System and Image Acquisition Protocol
2.3. Image Mosaicking in the White Light Modality
- The image pre-processing [42] step includes image resampling (down to 0.6 mega-pixels), area masking, noise reduction, dead pixel removal, radial distortion compensation (using the OpenCV library and a chess board pattern), and shading correction.
- Finding the key points (relating to vessel textures/structures in the images; see Figure 2 and Figure 4) using the Scale-Invariant Feature Transform (SIFT) [43] algorithm (3 octave layers, 0.03 contrast threshold, 12-edge threshold, and a sigma value of 1.6) and the determination of homologous SIFT key points between the image pairs by the nearest neighbors search method with subsequent filtering by the threshold ratio test. These homologous key points are later used to determine the parameters of the homography that superimposes the common scene parts seen in two images. A homography is an appropriate geometrical transformation, since quasi-planar bladder parts are seen in the small field of view of the endoscopes.
- The stitching process exploits a graph in which the vertices correspond to images and where the edge weights are given by the number of correct matches of homologous key points between the two images linked by the edge. The images used to determine the mosaic are those with the largest weights.
- Simultaneous evaluation and optimization of the parameters of the homographies linking all image pairs with enough SIFT matches (i.e., with large weight values in the previous step) by minimizing a functional depending on the color differences of the superimposed pixels using the least squares method.
- Construction of a panorama from aligned images either by the seam search method [44], which gives the smallest path in the relative brightness graph of images (placement of seams in areas where the colors of the image are the most similar), or the Laplace pyramid blending method.
2.4. Augmented Visualization
3. Results
3.1. Image Acquisition
3.2. Image Mosaicking and Augmented Visualization
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Soorojebally, Y.; Neuzillet, Y.; Lebret, T.; Allory, Y.; Descotes, F.; Ferlicot, S.; Kassab-Chahmi, D.; Lamy, P.J.; Oudard, S.; Rébillard, X.; et al. Photodynamic cystoscopy for bladder cancer diagnosis and for NMIBC follow-up: An overview of systematic reviews and meta-analyses. Prog. Urol. 2023, 33, 307–318. [Google Scholar] [CrossRef]
- Lerner, S.P.; Goh, A. Novel endoscopic diagnosis for bladder cancer. Cancer 2015, 121, 169–178. [Google Scholar] [CrossRef] [PubMed]
- Mulawkar, P.M.; Sharma, G.; Tamhankar, A.; Shah, U.; Raheem, R. Role of Macroscopic Image Enhancement in Diagnosis of Non-Muscle-Invasive Bladder Cancer: An Analytical Review. Front. Surg. 2022, 9, 762027. [Google Scholar] [CrossRef] [PubMed]
- Li, K.; Lin, T.; Xue, W.; Mu, X.; Xu, E.; Yang, X.; Chen, F.; Li, G.; Ma, L.; Wang, G.; et al. Current status of diagnosis and treatment of bladder cancer in china e analyses of Chinese bladder cancer consortium database. Asian J. Urol. 2015, 2, 63–69. [Google Scholar] [CrossRef] [PubMed]
- Schubert, T.; Rausch, S.; Fahmy, O.; Gakis, G.; Stenzl, A. Optical improvements in the diagnosis of bladder cancer: Implications for clinical practice. Ther. Adv. Urol. 2017, 9, 251–260. [Google Scholar] [CrossRef] [PubMed]
- Kang, W.; Cui, Z.; Chen, Q.; Zhang, D.; Zhang, H.; Jin, X. Narrow band imaging-assisted transurethral resection reduces the recurrence risk of non-muscle invasive bladder cancer: A systematic review and meta-analysis. Oncotarget 2016, 8, 23880–23890. [Google Scholar] [CrossRef]
- Barth, C.W.; Gibbs, S.L. Fluorescence Image-Guided Surgery—A Perspective on Contrast Agent Development. Proc. SPIE—Int. Soc. Opt. Eng. 2020, 11222, 112220J. [Google Scholar] [CrossRef]
- Gurung, P.; Lim, J.; Shrestha, R.; Kim, Y.W. Chlorin e6-associated photodynamic therapy enhances abscopal antitumor effects via inhibition of PD-1/PD-L1 immune checkpoint. Sci. Rep. 2023, 13, 4647. [Google Scholar] [CrossRef] [PubMed]
- Kozlikina, E.I.; Trifonov, I.S.; Sinkin, M.V.; Krylov, V.V.; Loschenov, V.B. The Combined Use of 5-ALA and Chlorin e6 Photosensitizers for Fluorescence-Guided Resection and Photodynamic Therapy under Neurophysiological Control for Recurrent Glioblastoma in the Functional Motor Area after Ineffective Use of 5-ALA: Preliminary Results. Bioengineering 2022, 9, 104. [Google Scholar] [CrossRef]
- Efendiev, K.; Alekseeva, P.; Linkov, K.; Shiryaev, A.; Pisareva, T.; Gilyadova, A.; Reshetov, I.; Voitova, A.; Loschenov, V. Tumor fluorescence and oxygenation monitoring during photodynamic therapy with chlorin e6 photosensitizer. Photodiagnosis Photodyn. Ther. 2024, 45, 103969. [Google Scholar] [CrossRef]
- Jain, R.; Pradhan, R.; Hejmady, S.; Singhvi, G.; Dubey, S.K. Fluorescence-based method for sensitive and rapid estimation of chlorin e6 in stealth liposomes for photodynamic therapy against cancer. Spectrochim. Acta A Mol. Biomol. Spectrosc. 2021, 244, 118823. [Google Scholar] [CrossRef] [PubMed]
- Shrestha, R.; Lee, H.J.; Lim, J.; Gurung, P.; Thapa Magar, T.B.; Kim, Y.T.; Lee, K.; Bae, S.; Kim, Y.W. Effect of Photodynamic Therapy with Chlorin e6 on Canine Tumors. Life 2022, 12, 2102. [Google Scholar] [CrossRef] [PubMed]
- Roberts, D.W.; Olson, J.D.; Evans, L.T.; Kolste, K.K.; Kanick, S.C.; Fan, X.; Bravo, J.J.; Wilson, B.C.; Leblond, F.; Marois, M.; et al. Red-light excitation of protoporphyrin IX fluorescence for subsurface tumor detection. J. Neurosurg. 2018, 128, 1690–1697. [Google Scholar] [CrossRef] [PubMed]
- Markwardt, N.A.; Haj-Hosseini, N.; Hollnburger, B.; Stepp, H.; Zelenkov, P.; Rühm, A. 405 nm versus 633 nm for protoporphyrin IX excitation in fluorescence-guided stereotactic biopsy of brain tumors. J. Biophotonics 2016, 9, 901–912. [Google Scholar] [CrossRef]
- Ruiz, A.J.; LaRochelle, E.P.M.; Gunn, J.R.; Hull, S.M.; Hasan, T.; Chapman, M.S.; Pogue, B.W. Smartphone fluorescence imager for quantitative dosimetry of protoporphyrin-IX-based photodynamic therapy in skin. J. Biomed. Opt. 2019, 25, 063802. [Google Scholar] [CrossRef] [PubMed]
- Yoneda, T.; Nonoguchi, N.; Ikeda, N.; Yagi, R.; Kawabata, S.; Furuse, M.; Hirose, Y.; Kuwabara, H.; Tamura, Y.; Kajimoto, Y.; et al. Spectral Radiance of Protoporphyrin IX Fluorescence and Its Histopathological Implications in 5-Aminolevulinic Acid-Guided Surgery for Glioblastoma. Photomed. Laser Surg. 2018, 36, 266–272. [Google Scholar] [CrossRef] [PubMed]
- Zada, L.; Anwar, S.; Imtiaz, S.; Saleem, M.; Shah, A.A. In vitro study: Methylene blue-based antibacterial photodynamic inactivation of Pseudomonas aeruginosa. Appl. Microbiol. Biotechnol. 2024, 108, 169. [Google Scholar] [CrossRef] [PubMed]
- Malik, S.; Andleeb, F.; Ullah, H. Multimodal imaging of skin lesions by using methylene blue as cancer biomarker. Microsc. Res. Tech. 2020, 83, 1594–1603. [Google Scholar] [CrossRef]
- Matsui, A.; Tanaka, E.; Choi, H.S.; Kianzad, V.; Gioux, S.; Lomnes, S.J.; Frangioni, J.V. Real-time, near-infrared, fluorescence-guided identification of the ureters using methylene blue. Surgery 2010, 148, 78–86. [Google Scholar] [CrossRef]
- Khan, S.; Alam, F.; Azam, A.; Khan, A.U. Gold nanoparticles enhance methylene blue-induced photodynamic therapy: A novel therapeutic approach to inhibit Candida albicans biofilm. Int. J. Nanomed. 2012, 7, 3245–3257. [Google Scholar] [CrossRef]
- Grande, M.P.D.; Miyake, A.M.; Nagamine, M.K.; Leite, J.V.P.; da Fonseca, I.I.M.; Massoco, C.O.; Dagli, M.L.Z. Methylene blue and photodynamic therapy for melanomas: Inducing different rates of cell death (necrosis and apoptosis) in B16-F10 melanoma cells according to methylene blue concentration and energy dose. Photodiagnosis Photodyn. Ther. 2022, 37, 102635. [Google Scholar] [CrossRef] [PubMed]
- Shell, T.A.; Lawrence, D.S. Vitamin B12: A tunable, long wavelength, light-responsive platform for launching therapeutic agents. Acc. Chem. Res. 2015, 48, 2866–2874. [Google Scholar] [CrossRef] [PubMed]
- Correia, J.H.; Rodrigues, J.A.; Pimenta, S.; Dong, T.; Yang, Z. Photodynamic Therapy Review: Principles, Photosensitizers, Applications, and Future Directions. Pharmaceutics 2021, 13, 1332. [Google Scholar] [CrossRef] [PubMed]
- Zhao, H.; Peng, P.; Luo, Z.; Liu, H.; Sun, J.; Wang, X.; Jia, Q.; Yang, Z. Comparison of hexaminolevulinate (HAL) guided versus white light transurethral resection for NMIBC: A systematic review and meta-analysis of randomized controlled trials. Photodiagnosis Photodyn. Ther. 2023, 41, 103220. [Google Scholar] [CrossRef] [PubMed]
- Nagaya, T.; Nakamura, Y.A.; Choyke, P.L.; Kobayashi, H. Fluorescence-Guided Surgery. Front. Oncol. 2017, 7, 314. [Google Scholar] [CrossRef] [PubMed]
- Weibel, T.; Daul, C.; Wolf, D.; Rösch, R.; Guillemin, F. Graph based construction of textured large field of view mosaics for bladder cancer diagnosis. Pattern Recognit. 2012, 45, 4138–4150. [Google Scholar] [CrossRef]
- Phan, T.-B.; Trinh, D.-H.; Lamarque, D.; Wolf, D.; Daul, C. Dense Optical Flow for the Reconstruction of Weakly Textured and Structured Surfaces. In Proceedings of the 2019 IEEE International Conference on Image Processing (ICIP), Taipei, Taiwan, 22–25 September 2019; pp. 310–314. [Google Scholar] [CrossRef]
- Zenteno, O.; Trinh, D.H.; Treuillet, S.; Lucas, Y.; Bazin, T.; Lamarque, D.; Daul, C. Optical biopsy mapping on endoscopic image mosaics with a marker-free probe. Comput. Biol. Med. 2022, 143, 105234. [Google Scholar] [CrossRef]
- Loshchenov, M.; Levkin, V.; Kalyagina, N.; Linkov, K.; Kharnas, S.; Efendiev, K.; Kharnas, P.; Loschenov, V. Laser-induced fluorescence diagnosis of stomach tumor. Lasers Med. Sci. 2020, 35, 1721–1728. [Google Scholar] [CrossRef] [PubMed]
- Loshchenov, M.V.; Seregin, A.V.; Kalyagina, N.A.; Dadashev, Ė.O.; Borodkin, A.V.; Babaev, A.; Loran, O.B.; Loschenov, V.B. Fluorescence visualization of the borders of bladder tumors after TUR with quantitative determination of diagnostic contrast. Transl. Biophotonics 2020, 2, e201900026. [Google Scholar] [CrossRef]
- Udeneev, A.; Kulichenko, A.; Kalyagina, N.; Shiryaev, A.; Pisareva, T.; Plotnikova, A.; Linkov, K.; Zavodnov, S.; Loshchenov, M. Comparison of chlorin-e6 detection efficiency by video systems with excitation wavelengths of 405 nm and 635 nm. Photodiagnosis Photodyn. Ther. 2023, 43, 103729. [Google Scholar] [CrossRef]
- Udeneev, A.M.; Kalyagina, N.A.; Efendiev, K.T.; Febenchukova, A.A.; Kulichenko, A.M.; Shiryaev, A.A.; Pisareva, T.N.; Linkov, K.G.; Loshchenov, M.V. Cost-effective device for locating and circumscribing superficial tumors with contrast enhancement and fluorescence quantification. Photodiagnosis Photodyn. Ther. 2023, 3, 103827. [Google Scholar] [CrossRef] [PubMed]
- Efendiev, K.T.; Alekseeva, P.M.; Shiryaev, A.A.; Skobeltsin, A.S.; Solonina, I.L.; Fatyanova, A.S.; Reshetov, I.V.; Loschenov, V.B. Preliminary low-dose photodynamic exposure to skin cancer with chlorin e6 photosensitizer. Photodiagnosis Photodyn. Ther. 2022, 38, 102894. [Google Scholar] [CrossRef] [PubMed]
- Li, Z.; Pan, W.; Shi, E.; Bai, L.; Liu, H.; Li, C.; Wang, Y.; Deng, J.; Wang, Y. A Multifunctional Nanosystem Based on Bacterial Cell-Penetrating Photosensitizer for Fighting Periodontitis Via Combining Photodynamic and Antibiotic Therapies. ACS Biomater. Sci. Eng. 2021, 7, 772–786. [Google Scholar] [CrossRef] [PubMed]
- Xiu, W.; Gan, S.; Wen, Q.; Qiu, Q.; Dai, S.; Dong, H.; Li, Q.; Yuwen, L.; Weng, L.; Teng, Z.; et al. Biofilm Microenvironment-Responsive Nanotheranostics for Dual-Mode Imaging and Hypoxia-Relief-Enhanced Photodynamic Therapy of Bacterial Infections. Research 2020, 2020, 9426453. [Google Scholar] [CrossRef] [PubMed]
- Uzdensky, A.B.; Dergacheva, O.Y.; Zhavoronkova, A.A.; Reshetnikov, A.V.; Ponomarev, G.V. Photodynamic effect of novel chlorin e6 derivatives on a single nerve cell. Life Sci. 2004, 74, 2185–2197. [Google Scholar] [CrossRef] [PubMed]
- Hope, C.K.; Packer, S.; Wilson, M.; Nair, S.P. The inability of a bacteriophage to infect Staphylococcus aureus does not prevent it from specifically delivering a photosensitizer to the bacterium enabling its lethal photosensitization. J. Antimicrob. Chemother. 2009, 64, 59–61. [Google Scholar] [CrossRef] [PubMed]
- Available online: https://omlc.org/ (accessed on 26 January 2024).
- Shahinyan, G.A.; Amirbekyan, A.Y.; Markarian, S.A. Photophysical properties of methylene blue in water and in aqueous solutions of dimethylsulfoxide. Spectrochim. Acta Part A Mol. Biomol. Spectrosc. 2019, 217, 170–175. [Google Scholar] [CrossRef] [PubMed]
- Brown, M.; Lowe, D.G. Automatic Panoramic Image Stitching using Invariant Features. Int. J. Comput. Vis. 2007, 74, 59–73. [Google Scholar] [CrossRef]
- Bradski, G. The OpenCV Library. Dr. Dobb’s J. Softw. Tools 2000, 120, 122–125. [Google Scholar]
- Miranda-Luna, R.; Hernandez-Mier, Y.; Daul, C.; Blondel, W.C.; Wolf, D. Mosaicing of medical video-endoscopic images: Data quality improvement and algorithm testing. In Proceedings of the (ICEEE) 1st International Conference on Electrical and Electronics Engineering, Acapulco, Mexico, 8–10 September 2004; pp. 530–535. [Google Scholar] [CrossRef]
- Lowe, D.G. Distinctive Image Features from Scale-Invariant Keypoints. Int. J. Comput. Vis. 2004, 60, 91–110. [Google Scholar] [CrossRef]
- Weibel, T.; Daul, C.; Wolf, D.; Rösch, R. Contrast-enhancing seam detection and blending using graph cuts. In Proceedings of the 21st International Conference on Pattern Recognition (ICPR2012), Tsukuba, Japan, 11–15 November 2012; pp. 2732–2735. [Google Scholar]
- Smith, G.T.; Lurie, K.L.; Zlatev, D.V.; Liao, J.C.; Ellerbee Bowden, A.K. Multimodal 3D cancer-mimicking optical phantom. Biomed. Opt. Express 2016, 7, 648–662. [Google Scholar] [CrossRef] [PubMed]
- Choi, E.; Waldbillig, F.; Jeong, M.; Li, D.; Goyal, R.; Weber, P.; Miernik, A.; Grüne, B.; Hein, S.; Suarez-Ibarrola, R.; et al. Soft Urinary Bladder Phantom for Endoscopic Training. Ann. Biomed. Eng. 2021, 49, 2412–2420. [Google Scholar] [CrossRef] [PubMed]
- Hackner, R.; Suarez-Ibarrola, R.; Qiu, T.; Lemke, N.; Pohlmann, P.F.; Wilhelm, K.; Fischer, P.; Miernik, A.; Wittenberg, T. Panoramic Imaging Assessment of Different Bladder Phantoms—An Evaluation Study. Urology 2021, 156, e103–e110. [Google Scholar] [CrossRef] [PubMed]
- Bergen, T.; Wittenberg, T. Stitching and Surface Reconstruction From Endoscopic Image Sequences: A Review of Applications and Methods. IEEE J. Biomed. Health Inform. 2016, 20, 304–321. [Google Scholar] [CrossRef] [PubMed]
- Soper, T.D.; Porter, M.P.; Seibel, E.J. Surface mosaics of the bladder reconstructed from endoscopic video for automated surveillance. IEEE Trans. Biomed. Eng. 2012, 59, 1670–1680. [Google Scholar] [CrossRef] [PubMed]
- Peng, H.; Cheng, C.-H. A panoramic endoscope design and implementation for Minimally Invasive Surgery. In Proceedings of the 2014 IEEE International Symposium on Circuits and Systems (ISCAS), Melbourne, VIC, Australia, 1–5 June 2014; pp. 453–456. [Google Scholar] [CrossRef]
- Phan, T.-B.; Trinh, D.-H.; Wolf, D.; Daul, C. Optical flow-based structure-from-motion for the reconstruction of epithelial surfaces. Pattern Recognit. 2020, 105, 107391. [Google Scholar] [CrossRef]
- Lurie, K.L.; Angst, R.; Zlatev, D.V.; Liao, J.C.; Ellerbee Bowden, A.K. 3D reconstruction of cystoscopy videos for comprehensive bladder records. Biomed. Opt. Express 2017, 8, 2106–2123. [Google Scholar] [CrossRef] [PubMed]
- Lurie, K.L.; Angst, R.; Seibel, E.J.; Liao, J.C.; Ellerbee Bowden, A.K. Registration of free-hand OCT daughter endoscopy to 3D organ reconstruction. Biomed. Opt. Express 2016, 7, 4995–5009. [Google Scholar] [CrossRef]
- Behrens, A.; Bommes, M.; Stehle, T.; Gross, S.; Leonhardt, S.; Aach, T. Real-time image composition of bladder mosaics in fluorescence endoscopy. Comput. Sci. Res. Dev. 2011, 26, 51–64. [Google Scholar] [CrossRef]
- Chenying, Y.; Soper, T.D.; Seibel, E.J. Detecting fluorescence hot-spots using mosaic maps generated from multimodal endoscope imaging. In Endoscopic Microscopy VIII; International Society for Optics and Photonics: Bellingham, WA, USA, 2013; Volume 8575, p. 857508. [Google Scholar] [CrossRef]
- Amouroux, M.; Salleron, J.; Huin-Schohn, C.; Ali, S.; Berthaud, S.; Rizo, P.; Schneider, S.; Vever-Bizet, C.; Bourg-Heckly, G.; Guillemin, F.; et al. Clinical evaluation of a device providing simultaneous white-light and fluorescence video streams as well as panoramic imaging during fluorescence assisted-transurethral resection of bladder cancer. JOSA A 2019, 36, C62–C68. [Google Scholar] [CrossRef]
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Moskalev, A.; Kalyagina, N.; Kozlikina, E.; Kustov, D.; Loshchenov, M.; Amouroux, M.; Daul, C.; Blondel, W. Validation of a White Light and Fluorescence Augmented Panoramic Endoscopic Imaging System on a Bimodal Bladder Wall Experimental Model. Photonics 2024, 11, 514. https://doi.org/10.3390/photonics11060514
Moskalev A, Kalyagina N, Kozlikina E, Kustov D, Loshchenov M, Amouroux M, Daul C, Blondel W. Validation of a White Light and Fluorescence Augmented Panoramic Endoscopic Imaging System on a Bimodal Bladder Wall Experimental Model. Photonics. 2024; 11(6):514. https://doi.org/10.3390/photonics11060514
Chicago/Turabian StyleMoskalev, Arkadii, Nina Kalyagina, Elizaveta Kozlikina, Daniil Kustov, Maxim Loshchenov, Marine Amouroux, Christian Daul, and Walter Blondel. 2024. "Validation of a White Light and Fluorescence Augmented Panoramic Endoscopic Imaging System on a Bimodal Bladder Wall Experimental Model" Photonics 11, no. 6: 514. https://doi.org/10.3390/photonics11060514
APA StyleMoskalev, A., Kalyagina, N., Kozlikina, E., Kustov, D., Loshchenov, M., Amouroux, M., Daul, C., & Blondel, W. (2024). Validation of a White Light and Fluorescence Augmented Panoramic Endoscopic Imaging System on a Bimodal Bladder Wall Experimental Model. Photonics, 11(6), 514. https://doi.org/10.3390/photonics11060514