

The Story, Properties and Applications of Bioactive Glass “1d”: From Concept to Early Clinical Trials

 ,
, 
 ,
,  ,
, 
Abstract
1. Introduction
2. The Genesis of the 1d Composition
3. Material Preparation and Basic Properties
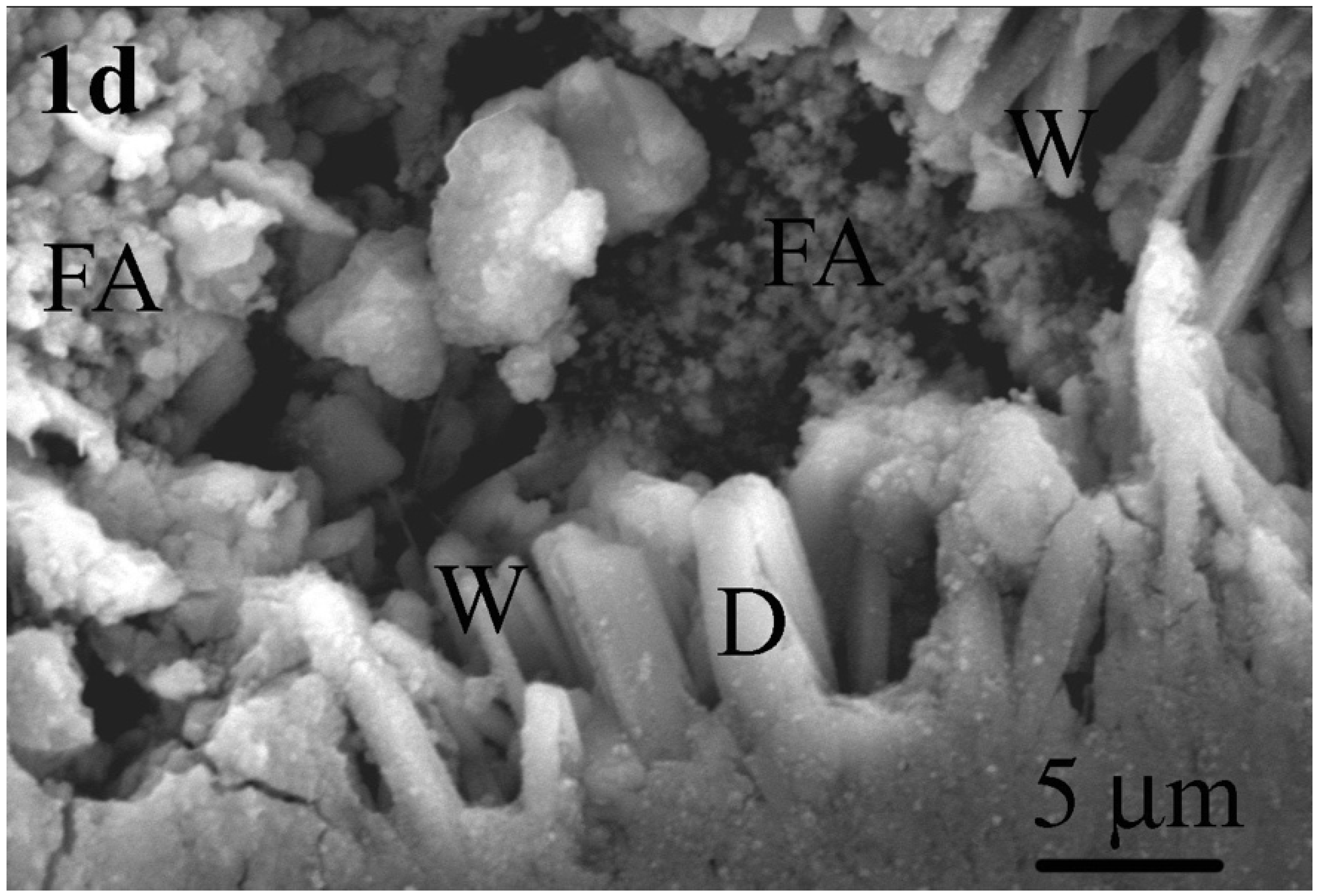
4. Crystalline Phases and Mechanical Properties
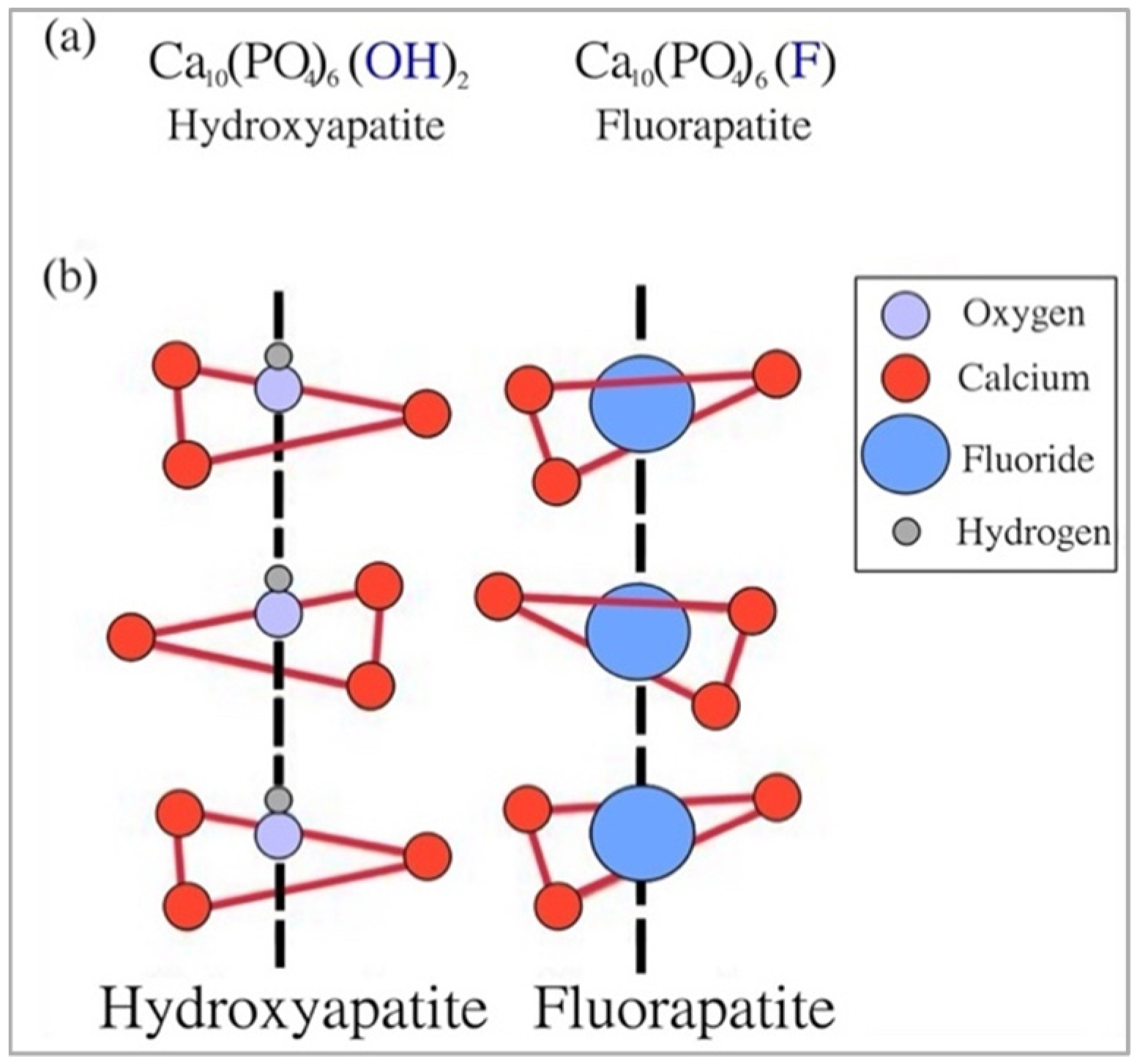
4.1. Fluorapatite
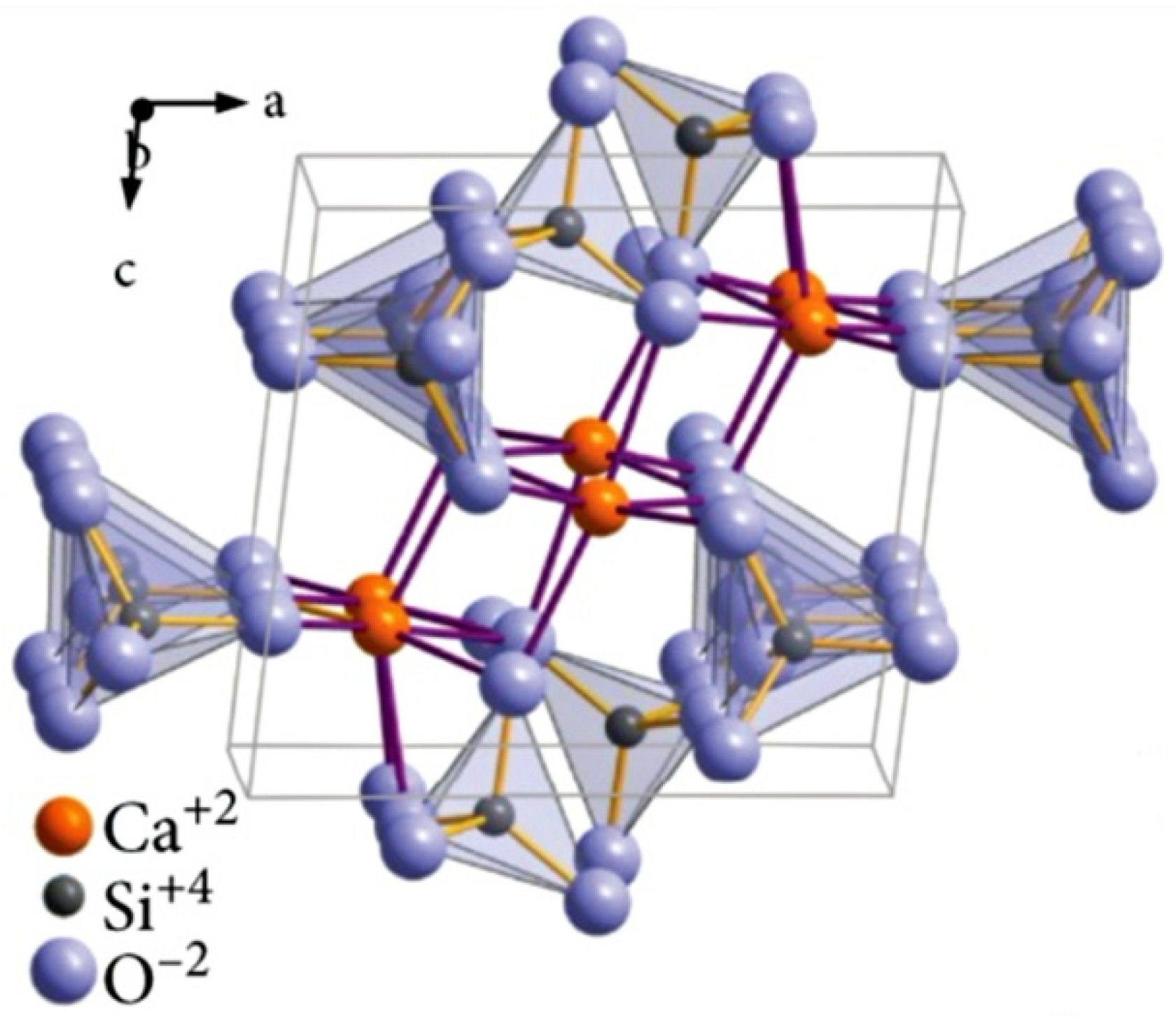
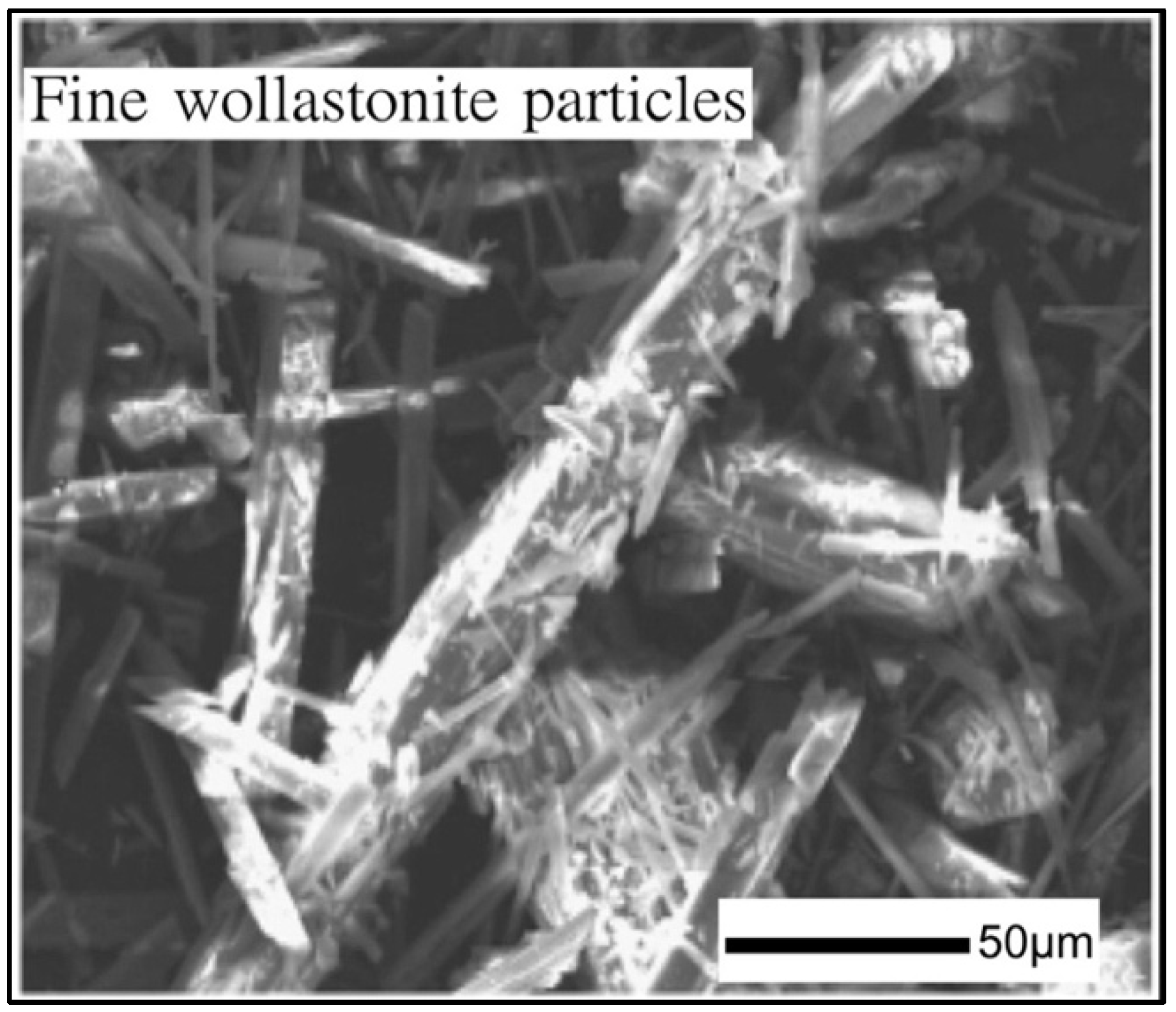
4.2. Wollastonite
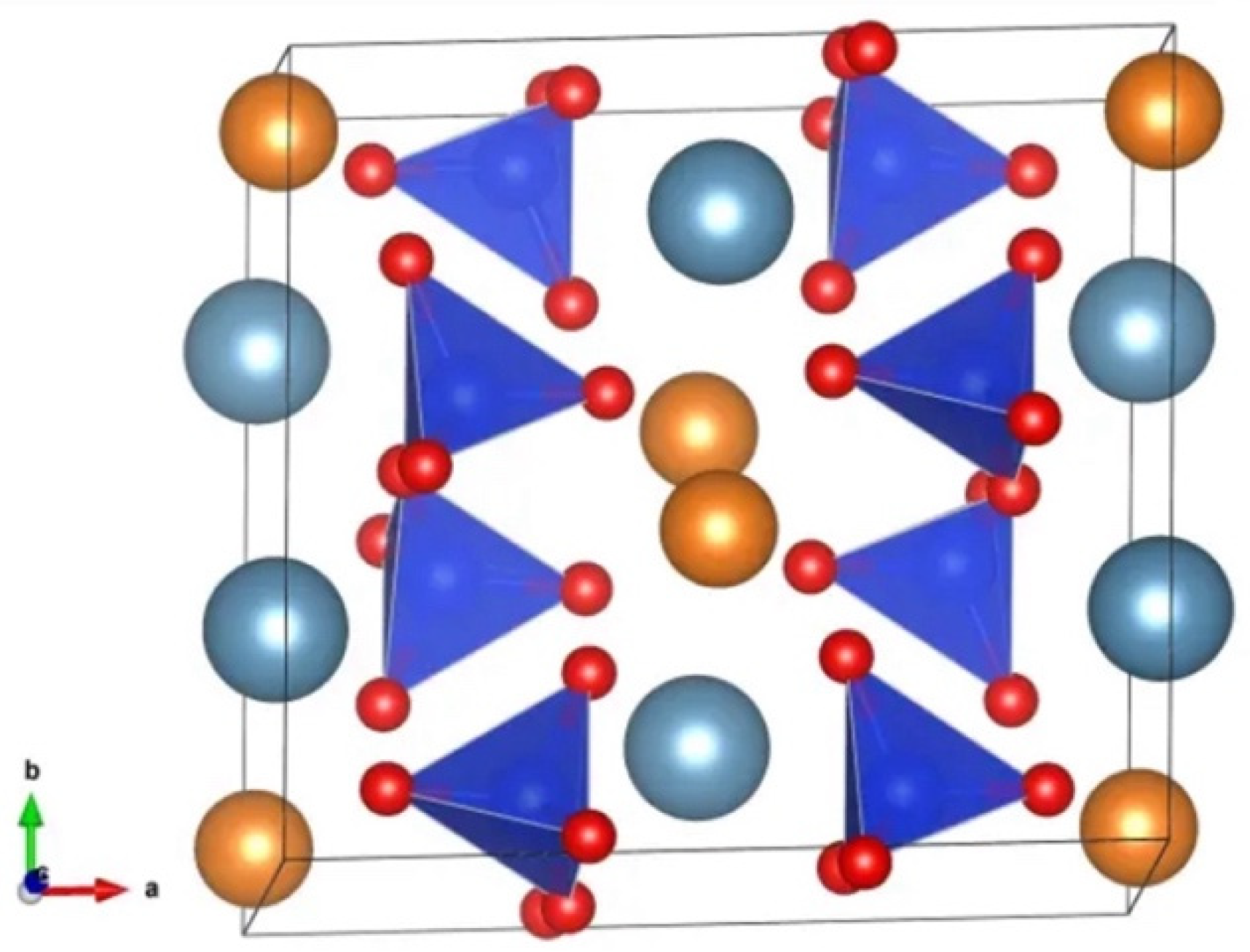
4.3. Diopside
5. Comparison between 1d Formulation and 45S5 Bioglass®
5.1. Chemical Composition
- The content of Na2O in 45S5 is more than five times greater when compared to 1d;
- The 1d glass contains additional MgO and CaF2, which are not present in the case of the 45S5 Bioglass®.
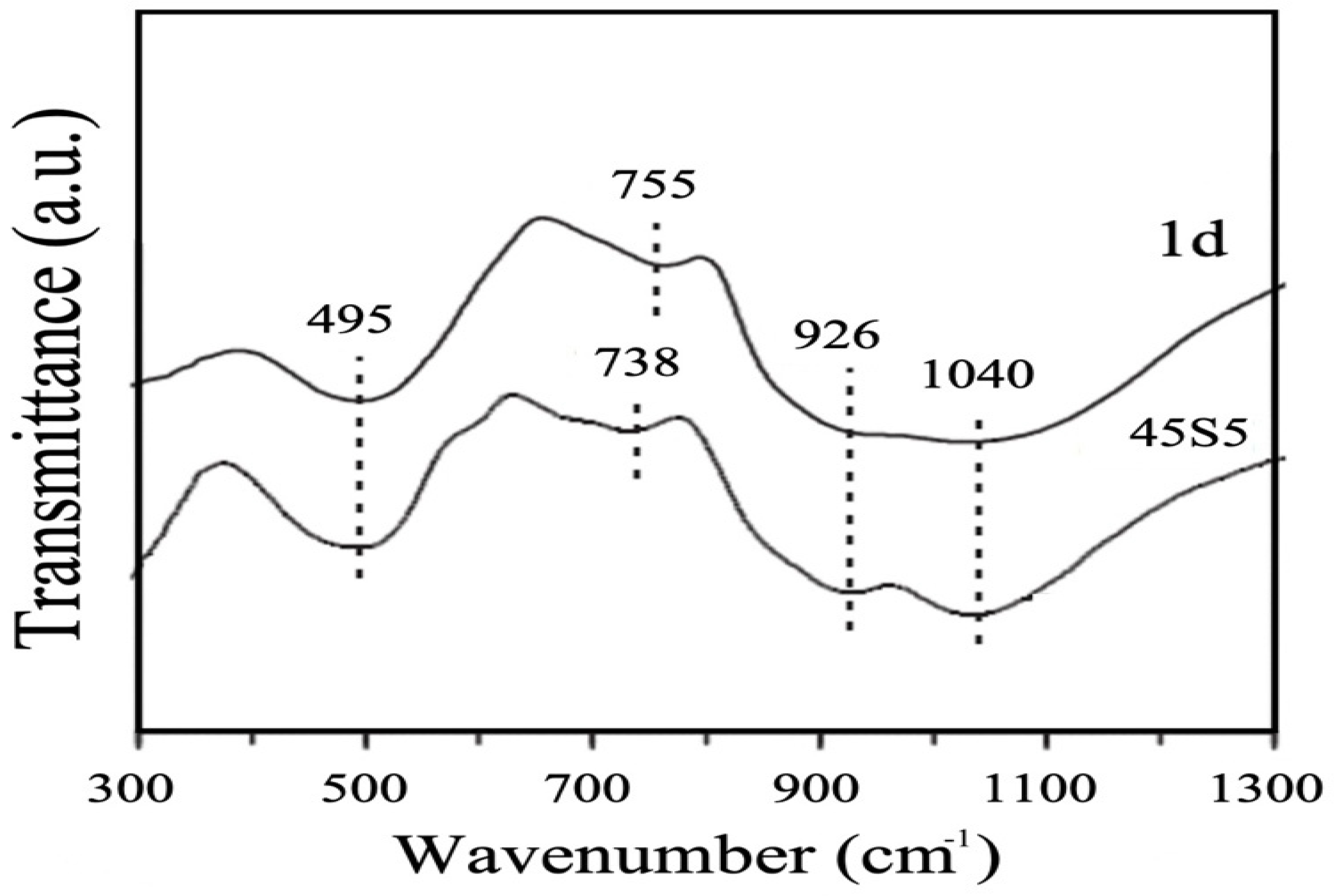
5.2. Advanced Microstructural Analysis (Qn Units)
5.3. pH In Vitro
5.4. Mass Loss
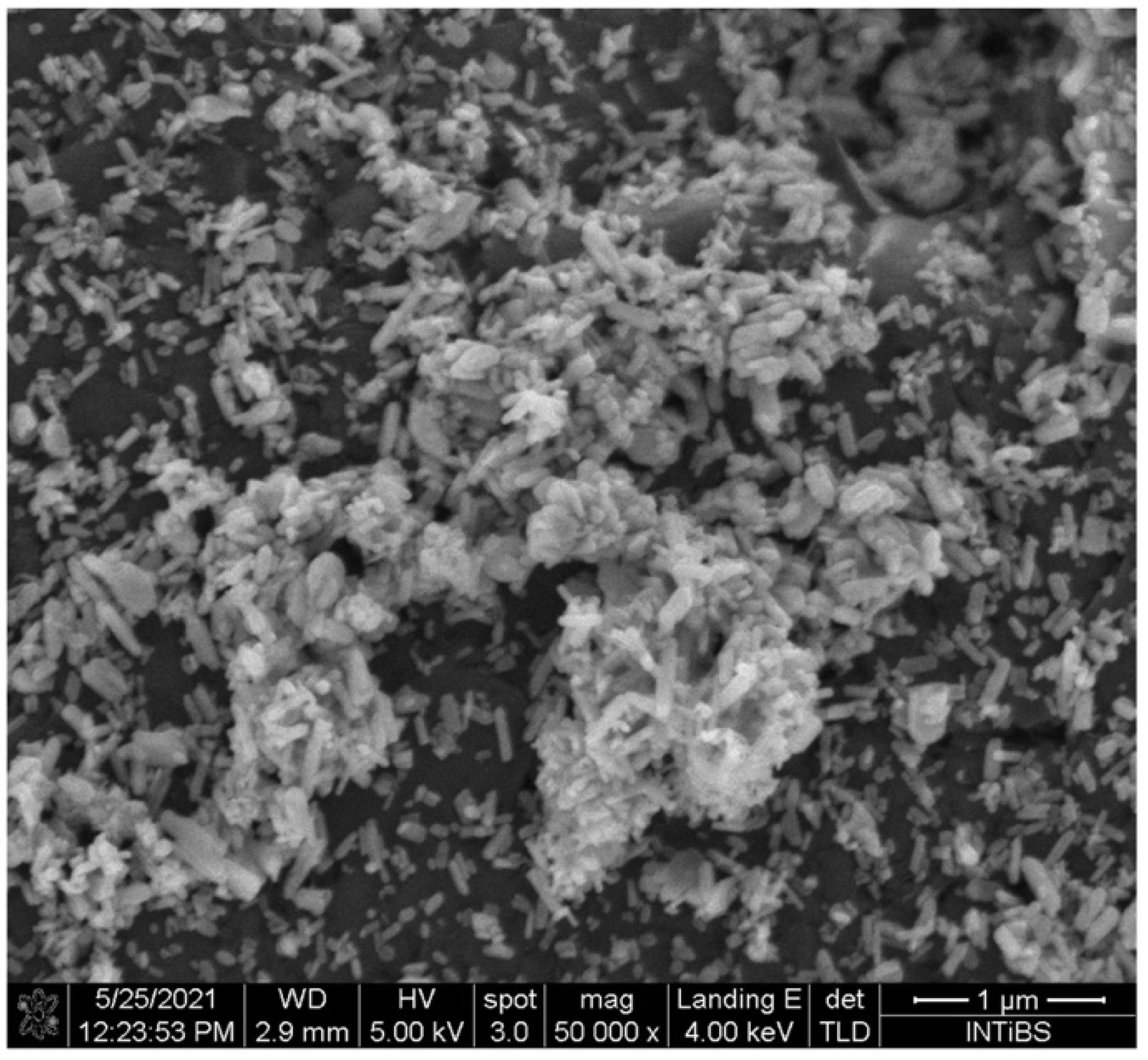
5.5. In Vitro Bioactivity
5.6. Direct and Indirect Cell Culture
- (a)
- Indirect culture: the bioactive glasses were immersed in a solution for 24 h at body temperature and shaken to promote the release of ionic dissolution products. At the end of this first phase, the glasses were removed, and the solution was filtered and used as a culture medium for mesenchymal stem cells (MSCs). This setting is used to verify the effects of the ions released.
- (b)
- Direct culture: the bioactive glasses removed from the solution in the point (a) were placed in direct contact with MSCs.
- -
- Indirect culture setting: 45S5 glass elicited a better osteogenic action compared to 1d glass. This behaviour was because, in the former case, there was a higher concentration of P and Si ions in the cell culture medium having osteostimulatory effects. In fact, phosphorus stimulates osteogenic differentiation and bone mineralization [50], and Si ions also activate gene families in bone cells, ultimately promoting osteogenic differentiation [51].
- -
- Direct culture setting: there was a reversal in the trend compared to the indirect culture setting. In fact, the osteogenic action was no longer so different between the two bioactive glasses, although the expression of the specific protein OCN (marker of osteogenic differentiation) was greater in the 1d cultures. The concentration of magnesium, which was released by the 1d glass, in the first 24 h was one tenth of that detected after a week, and the concentration of Ca increased over time in the medium. This progressive, increasing release of beneficial ions is important as magnesium ions have the ability to increase cell viability [52], and calcium ions improve cell viability and proliferation [53]. These promising in vitro results on 1d glass were corroborated by in vivo tests.
5.7. Antibacterial Properties
6. In Vivo Experiments and Clinical Trials
7. Towards the Future: 1d-Derived GC Dental Implants and Porous Scaffolds
7.1. GC Dental Implants
7.2. Glass-Derived Porous Scaffolds
8. Conclusions
Author Contributions
Funding
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Hench, L.L. The story of Bioglass. J. Mater. Sci. Mater. Med. 2006, 17, 967978. [Google Scholar] [CrossRef]
- Wu, C.; Chang, J. Mesoporous bioactive glasses: Structure characteristics, drug/growth factor delivery and bone regeneration application. Interface Focus 2012, 2, 292–306. [Google Scholar] [CrossRef]
- Moeini, A.; Hassanzadeh Chinijani, T.; Malek Khachatourian, A.; Fook, M.V.L.; Baino, F.; Montazerian, M. A critical review of bioactive glasses and glass-ceramics in cancer therapy. Int. J. Appl. Glass. Sci. 2023, 14, 69–87. [Google Scholar] [CrossRef]
- Miguez-Pacheco, V.; Greenspan, D.; Hench, L.; Boccaccini, A. Bioactive glasses in soft tissue repair. Am. Ceram. Soc. Bull. 2015, 94, 27–31. [Google Scholar]
- Hench, L.L.; Greenspan, D. Interactions between bioactive glass and collagen: A review and new perspectives. J. Aust. Ceram. Soc. 2013, 49, 1–40. [Google Scholar]
- Hench, L.L. Bioactive ceramics. Ann. N. Y. Acad. Sci. 1988, 523, 54–71. [Google Scholar] [CrossRef]
- Roy, M.; Bandyopadhyay, A.; Bose, S. Ceramics in Bone Grafts and Coated Implants. In Materials for Bone Disorders, 1st ed.; Bandyopadhyay, A., Bose, S., Eds.; Elsevier: Philadelphia, PA, USA, 2017; pp. 265–314. [Google Scholar]
- Bi, L.; Rahaman, M.N.; Day, D.E.; Brown, Z.; Samujh, C.; Liu, X.; Mohammadkhah, A.; Dusevich, V.; Eick, J.D.; Bonewald, L.F. Effect of bioactive borate glass microstructure on bone regeneration, angiogenesis, and hydroxyapatite conversion in a rat calvarial defect model. Acta Biomater. 2013, 9, 8015–8026. [Google Scholar] [CrossRef]
- Abou Neel, E.A.; Pickup, D.M.; Valappil, S.P.; Newport, R.J.; Knowles, J.C. Bioactive functional materials: A perspective on phosphate-based glasses. J. Mater. Chem. 2009, 19, 690–701. [Google Scholar] [CrossRef]
- McEntire, B.; Bal, B.S.; Rahaman, M.; Chevalier, J.; Pezzotti, G. Ceramics and ceramic coatings in orthopaedics. J. Eur. Ceram. Soc. 2015, 35, 4327–4369. [Google Scholar] [CrossRef]
- Balasubramanian, S.; Gurumurthy, B.; Balasubramanian, A. Biomedical applications of ceramic nanomaterials: A review. Int. J. Pharma Sci. Res. 2017, 8, 4950–4959. [Google Scholar]
- Shanmugam, K.; Sahadevan, R. Bioceramics—An Introductory Overview. In Fundamental Biomaterials: Ceramics, 1st ed.; Thomas, S., Balakrishnan, P., Sreekala, M.S., Eds.; Elsevier Ltd.: Philadelphia, PA, USA, 2018; pp. 1–46. [Google Scholar]
- Montazerian, M.; Zanotto, E.D. History and trends of bioactive glass-ceramics. J. Biomed. Mater. Res. A 2016, 104, 1231–1249. [Google Scholar] [CrossRef] [PubMed]
- Blayney, A.W.; Bebear, J.P.; Williams, K.R.; Portmann, M. Ceravital in ossiculoplasty: Experimental studies and early clinical results. Am. J. Otol. 1986, 100, 1359–1366. [Google Scholar] [CrossRef] [PubMed]
- Nonami, T.; Tsutsumi, S. Study of diopside ceramics for biomaterials. J. Mater. Sci. Mater. Med. 1999, 10, 475–479. [Google Scholar] [CrossRef] [PubMed]
- Salinas, A.J.; Vallet-Regí, M. Bioactive ceramics: From bone grafts to tissue engineering. RSC Adv. 2013, 3, 11116–11131. [Google Scholar] [CrossRef]
- Peitl, O.; LaTorre, G.P.; Hench, L.L. Effect of crystallization on apatite layer formation of bioactive glass 45S5. J. Biomed. Mater. Res. 1996, 30, 509–514. [Google Scholar]
- Kansal, I.; Tulyaganov, D.U.; Goel, A.; Pascual, M.J.; Ferreira, J.M.F. Structural analysis and thermal behavior of diopside fluorapatite wollastonite based glasses and glass ceramics. Acta Biomater. 2010, 6, 4380–4388. [Google Scholar] [CrossRef] [PubMed]
- Dimitriadis, K.; Vasilopoulos, K.C.; Vaimakis, T.C.; Karakassides, M.A.; Tulyaganov, D.U.; Agathopoulos, S. Synthesis of glass ceramics in the Na2O/K2O-CaO-MgO-SiO2-P2O5-CaF2 system as candidate materials for dental applications. Int. J. Appl. Ceram. Technol. 2020, 17, 2025–2035. [Google Scholar] [CrossRef]
- Dimitriadis, K.; Moschovas, D.; Tulyaganov, D.U.; Agathopoulos, S. Development of novel bioactive glass ceramics in the Na2O/K2O-CaO-MgO-SiO2-P2O5-CaF2 system. J. Non-Cryst. Solids 2020, 533, 119936. [Google Scholar] [CrossRef]
- Tulyaganov, D.U.; Agathopoulos, S.; Ventura, J.M.G.; Karakassides, M.A.; Fabrichnaya, O.; Ferreira, J.M.F. Synthesis of glass–ceramics in the CaO–MgO–SiO2 system with B2O3, P2O5, Na2O andCaF2 additives. J. Eur. Ceram. Soc. 2006, 26, 1463–1471. [Google Scholar] [CrossRef]
- Tulyaganov, D.U.; Agathopoulos, S.; Valerio, P.; Balamurugan, A.; Saranti, A.; Karakassides, M.A.; Ferreira, J.M.F. Synthesis, bioactivity and preliminary biocompatibility studies of glasses in the system CaO-MgO-SiO2-Na2O-P2O5-CaF2. J. Mater. Sci. Mater. Med. 2011, 22, 217–227. [Google Scholar] [CrossRef]
- Schmitz, S.I.; Widholz, B.; Essers, C.; Becker, M.; Tulyaganov, D.U.; Moghaddam, A.; Gonzalo de Juan, I.; Westhauser, F. Superior biocompatibility and comparable osteoinductive properties: Sodium-reduced fluoride-containing bioactive glass belonging to the CaO–MgO–SiO2 system as a promising alternative to 45S5 bioactive glass. Bioact. Mater. 2020, 5, 55–65. [Google Scholar] [CrossRef] [PubMed]
- Tulyaganov, D.U.; Akbarov, A.; Zyyadullaeva, N.; Khabilov, B.; Baino, F. Injectable bioactive glass-based pastes for potential use in bone tissue repair. Biomed. Glas. 2020, 6, 23–33. [Google Scholar] [CrossRef]
- Baino, F.; Tulyaganov, D.U.; Kahharov, Z.; Rahdar, A.; Vernè, E. Foam-Replicated Diopside/Fluorapatite/Wollastonite-Based Glass–Ceramic Scaffolds. Ceramics 2022, 5, 120–130. [Google Scholar] [CrossRef]
- Tulyaganov, D.U.; Makhkamov, M.E.; Urazbaev, A.; Goel, A.; Ferreira, J.M.F. Synthesis, processing and characterization of a bioactive glass composition for bone regeneration. Ceram. Int. 2013, 39, 2519–2526. [Google Scholar] [CrossRef]
- Boccaccini, A.R. Machinability and brittleness of glass-ceramics. J. Mater. Process Technol. 1997, 65, 302–304. [Google Scholar] [CrossRef]
- Dimitriadis, K.; Tulyaganov, D.U.; Agathopoulos, S. Production of Bioactive Glass-Ceramics for Dental Application through Devitrification of Glasses in the Na2O/K2O–CaO–MgO–SiO2–P2O5–CaF2 System. In Bioactive Glasses and Glass-Ceramics: Fundamentals, Applications, and Advances; Baino, F., Kargozar, S., Eds.; John Wiley and Sons Ltd.: Hoboken, NJ, USA, 2022; pp. 431–457. [Google Scholar]
- Kapoor, S.; Goel, A.; Filipa, A.; Pascual, M.J.; Lee, H.; Kim, H.; Ferreira, J.M.F. Influence of ZnO/MgO substitution on sintering, crystallisation, and bio-activity of alkali-free glass-ceramics. Mater. Sci. Eng. C 2015, 53, 252–261. [Google Scholar] [CrossRef]
- Soares, V.O.; Daguano, J.K.M.B.; Lombello, C.B.; Bianchin, O.S.; Gonçalves, L.M.G.; Zanotto, E.D. New sintered wollastonite glass-ceramic for biomedical applications. Ceram. Int. 2018, 44, 20019–20027. [Google Scholar] [CrossRef]
- Saadaldin, S.A.; Rizkalla, A.S. Synthesis and characterization of wollastonite glassceramics for dental implant applications. Dent. Mater. 2014, 30, 364–371. [Google Scholar] [CrossRef]
- Saadaldin, S.A.; Dixon, S.J.; Rizkalla, A.S. Bioactivity and biocompatibility of a novel wollastonite glass-ceramic biomaterial. J. Biomater. Tissue Eng. 2014, 4, 939–946. [Google Scholar] [CrossRef]
- Garcia, E.; Miranzo, P.; Sainz, M.A. Thermally sprayed wollastonite and wollastonite-diopside compositions as new modulated bioactive coatings for metal implants. Ceram. Int. 2018, 44, 12896–12904. [Google Scholar] [CrossRef]
- Dorozhkin, S.V. Calcium orthophosphates as bioceramics: State of the art. J. Funct. Mater. 2010, 1, 22–107. [Google Scholar] [CrossRef]
- Ramadoss, R.; Padmanaban, R.; Subramanian, B. Role of bioglass in enamel remineralization: Existing strategies and future prospects-A narrative review. J. Biomed. Mater. Res. B Appl. Biomater. 2022, 110, 45–66. [Google Scholar] [CrossRef] [PubMed]
- Wiglusz, K.; Dobrzynski, M.; Gutbier, M.; Wiglusz, R.J. Nanofluorapatite Hydrogels in the treatment of Dentin Hypersensitivity: A study of physiochemical Proprieties and Fluoride Realease. Gels 2023, 9, 271–287. [Google Scholar] [CrossRef]
- Zenebe, C.G. A Review on the Role of Wollastonite Biomaterial in Bone Tissue Engineering. BioMed Res. Int. 2022, 2022, 996530. [Google Scholar] [CrossRef]
- Tulyaganov, D.U.; Dimitriadis, K.; Agathopoulos, S.; Baino, F.; Fernandes, H.R. Wollastonite-containing glass-ceramics from the CaO–Al2O3–SiO2 and CaO–MgO–SiO2 ternary systems. Open Ceram. 2024, 17, 100507. [Google Scholar] [CrossRef]
- Kokubo, T.; Shigematsu, M.; Nagashima, Y.; Tashiro, M.; Nakamura, T.; Yamamuro, T.; Higash, S. Apatite-and wollastonite-containing glass-ceramics for prosthetic application. Bull. Inst. Chem. Res. Kyoto Univ. 1982, 60, 260–268. [Google Scholar]
- Hench, L.L.; Splinter, R.J.; Allen, W.C.; Greenlee, T.K. Bonding mechanisms at the interface of ceramic prosthetic materials. J. Biomed. Mater. Res. 1971, 5, 117–141. [Google Scholar] [CrossRef]
- Vichaphund, S.; Kitiwan, M.; Atong, D.; Thavorniti, P. Microwave synthesis of wollastonite powder from eggshells. J. Eur. Ceram. Soc. 2011, 31, 2435–2440. [Google Scholar] [CrossRef]
- He, Z.; Shen, A.; Lyu, Z.; Li, Y.; Wu, H.; Wang, W. Effect of wollastonite microfibers as cement replacement on the properties of cementitious composites: A review. Constr. Build. Mater. 2020, 261, 119920. [Google Scholar] [CrossRef]
- “Chrome Diopside”, Chemistry Views. 22 May 2014. Available online: https://www.chemistryviews.org/details/ezine/6047511/Chrome_Diopside/#:~:text=Diopside%20has%20the%20composition%20CaMgSi,the%20crystals%20are%20often%20twinned (accessed on 1 November 2023).
- “A Surprisingly Important Structure-Diopside”, Chrystallography365. 23 August 2014. Available online: https://crystallography365.wordpress.com/2014/08/23/a-surprisingly-important-structure-diopside/ (accessed on 1 November 2023).
- Wang, G.C.; Lu, Z.F.; Zreiqat, H. Bioceramics for Skeletal Bone Regeneration. In Bone Substitute Biomaterials, 1st ed.; Mallick, K., Ed.; Woodhead Publishing: Cambridge, UK, 2014; pp. 180–186. [Google Scholar]
- Dietrich, E.; Oudadesse, H.; Lucas Girot, A.; Le Gal, Y.; Jeanne, S.; Cathelineau, G. Effects of Mg and Zn on the surface of doped melt derived glass for biomaterials applications. Appl. Surf. Sci. 2008, 255, 391–395. [Google Scholar] [CrossRef]
- Tilocca, A. Structural models of bioactive glasses from molecular dynamics simulations. Proc. R Soc. A 2009, 465, 1003–1027. [Google Scholar] [CrossRef]
- Brauer, D.S.; Karpulthina, N.; O’Donnell, M.D.; Law, R.V.; Hill, R.G. Fluoride-containing bioactive glasses: Effect of glass design and structure on degradation, pH and apatite formation in simulated body fluid. Acta Biomater. 2010, 6, 3275–3282. [Google Scholar] [CrossRef] [PubMed]
- Mozafari, M.; Banijamali, S.; Baino, F.; Kargozar, S.; Hill, R.G. Calcium carbonate: Adored and ignored in bioactivity assessment. Acta Biomater. 2019, 91, 35–47. [Google Scholar] [CrossRef] [PubMed]
- Khoshniat, S.; Bourgine, A.; Julien, M.; Petit, M.; Pilet, P.; Rouillon, T.; Masson, M.; Gatius, M.; Weiss, P.; Guicheux, J.; et al. Phosphate-dependent stimulation of MGP and OPN expression in osteoblasts via the ERK1/2 pathway is modulated by calcium. Bone 2011, 48, 894–902. [Google Scholar] [CrossRef] [PubMed]
- Reffitt, D.M.; Ogston, N.; Jugdaohsingh, R.; Cheung, H.F.; Evans, B.A.; Thompson, R.P.; Powell, J.J.; Hampson, G.N. Orthosilicic acid stimulates collagen type 1 synthesis and osteoblastic differentiation in human osteoblast-like cells in vitro. Bone 2003, 32, 127–135. [Google Scholar] [CrossRef]
- Zheng, J.; Mao, X.; Ling, J.; Chen, C.; Zhang, W. Role of magnesium transporter subtype 1 (MagT1) in the osteogenic differentiation of rat bone marrow stem cells. Biol. Trace Elem. Res. 2016, 171, 131–137. [Google Scholar] [CrossRef] [PubMed]
- Hench, L.L. Genetic design of bioactive glasses. J. Eur. Ceram. Soc. 2009, 29, 1257–1265. [Google Scholar] [CrossRef]
- Gonzalo-Juan, I.; Xie, F.; Becker, M.; Tulyaganov, D.U.; Fischer, A.; Riedel, R. Synthesis of silver modified bioactive glassy materials with antibacterial properties via facile and low-temperature route. Materials 2020, 13, 5115. [Google Scholar] [CrossRef] [PubMed]
- Gonzalo-Juan, I.; Tulyaganov, D.U.; Balan, C.; Linser, R.; Ferreira, J.M.F.; Riedel, R.; Ionescu, E. Tailoring the viscoelastic properties of injectable biocomposites: A spectroscopic assessment of the interactions between organic carriers and bioglass particles. Mater. Des. 2016, 97, 45–50. [Google Scholar] [CrossRef]
- Jones, J.R.; Brauer, D.S.; Hupa, L.; Greenspan, D.C. Bioglass and bioactive glasses and their impact on healthcare. Int. J. Appl. Glass Sci. 2016, 7, 423–434. [Google Scholar] [CrossRef]
- Fernandes, H.R.; Gaddam, A.; Rebelo, A.; Brazete, D.; Stan, G.E.; Ferreira, J.M.F. Bioactive glasses and glass-ceramics for healthcare applications in bone regeneration and tissue engineering. Materials 2018, 11, 2530. [Google Scholar] [CrossRef]
- Albrektsson, T.; Johansson, C. Osteoinduction, osteoconduction and osseointegration. Eur. Spine J. 2001, 10, S96–S101. [Google Scholar]
- Lakatos, É.; Magyar, L.; Bojtár, I. Material properties of the mandibular trabecular bone. J. Med. Eng. 2014, 2014, 470539. [Google Scholar] [CrossRef]
- Dimitriadis, K.; Tulyaganov, D.U.; Agathopoulos, S. Development of novel alumina-containing bioactive glass-ceramics in the CaO-MgO-SiO2 system as possible candidates for dental implant applications. J. Eur. Ceram. Soc. 2021, 41, 929–940. [Google Scholar] [CrossRef]
- Montazerian, M.; Zanotto, E.D. Bioactive and inert dental glass-ceramics. Biomed. Mater. Res. A 2017, 105, 619–639. [Google Scholar] [CrossRef] [PubMed]
- Saadaldin, S.A.; Dixon, S.J.; Costa, D.O.; Rizkalla, A.S. Synthesis of bioactive and machinable miserite glass-ceramics for dental implant applications. Dent. Mater. 2013, 29, 645–655. [Google Scholar] [CrossRef] [PubMed]
- Fillingham, Y.; Jacobs, J. Bone grafts and their substitutes. Bone Jt. J. 2016, 98-B, 6–9. [Google Scholar] [CrossRef]
- Laurencin, C.; Khan, Y.; El-Amin, S.F. Bone graft substitutes. Expert. Rev. Med. Devices 2006, 3, 49–57. [Google Scholar] [CrossRef] [PubMed]
- Kumar, P.; Vinitha, B.; Fathima, G. Bone grafts in dentistry. J. Pharm. Bioallied. Sci. 2013, 5, S125–S127. [Google Scholar] [CrossRef]
- Chen, Q.Z.; Thompson, I.D.; Boccaccini, A.R. 45S5 Bioglass-derived glass-ceramic scaffolds for bone tissue engineering. Biomaterials 2006, 27, 2414–2425. [Google Scholar] [CrossRef] [PubMed]
- Fu, L.; Engqvist, H.; Xia, W. Glass-ceramics in dentistry: A review. Materials. 2020, 13, 1049. [Google Scholar] [CrossRef]
- Rezwan, K.; Chen, Q.Z.; Blaker, J.J.; Boccaccini, A.R. Biodegradable and bioactive porous polymer/inorganic composite scaffolds for bone tissue engineering. Biomaterials 2006, 27, 3413–3431. [Google Scholar] [CrossRef] [PubMed]
- Mohamad Yunos, D.; Bretcanu, O.; Boccaccini, A.R. Polymer-bioceramic composites for tissue engineering scaffolds. J. Mater. Sci. 2008, 43, 4433–4442. [Google Scholar] [CrossRef]
- Rehorek, L.; Chlup, Z.; Meng, D.; Yunos, D.M.; Boccaccini, A.R.; Dlouhy, I. Response of 45S5 bioglass® foams to tensile loading. Ceram. Int. 2013, 39, 8015–8020. [Google Scholar] [CrossRef]
- Baino, F.; Fiume, E.; Barberi, J.; Kargozar, S.; Marchi, J.; Massera, J.; Verné, E. Processing methods for making porous bioactive glass-based scaffolds—A state-of-the-art review. Int. J. Appl. Ceram. Technol. 2019, 16, 1762–1796. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Composition | SiO2 | CaO | MgO | P2O5 | Na2O | K2O | CaF2 |
|---|---|---|---|---|---|---|---|
| Parent glass composition | |||||||
| 1d | 46.1 | 28.7 | 8.8 | 6.2 | 4.5 | 0 | 5.7 |
| 1d-a | 41.8 | 32.85 | 8.85 | 6.24 | 4.54 | 0 | 5.72 |
| 1d-b | 37.51 | 37.07 | 8.88 | 6.26 | 4.55 | 0 | 5.73 |
| 1e | 43.5 | 30.4 | 8.8 | 7.2 | 4.5 | 0 | 5.6 |
| 1e-a | 43.09 | 30.13 | 8.67 | 9.17 | 4.44 | 0 | 4.47 |
| 1e-b | 42.71 | 29.85 | 8.59 | 11.1 | 4.41 | 0 | 3.33 |
| 1e-c | 42.33 | 29.59 | 8.52 | 13.00 | 4.37 | 0 | 2.19 |
| K2O for Na2O substitution | |||||||
| 1d-k | 45.0 | 28.0 | 8.60 | 6.1 | 0 | 6.7 | 5.6 |
| 1e-k | 42.5 | 29.7 | 8.5 | 7.1 | 0 | 6.7 | 5.5 |
| MgO for CaO partial substitution | |||||||
| 1d-m | 46.6 | 24.8 | 11.9 | 6.3 | 4.6 | 0 | 5.8 |
| 1e-m | 44.00 | 26.7 | 11.8 | 7.3 | 4.5 | 0 | 5.7 |
| Article | Powders | Batch and Milling | Heat Treatment | Frits and Glass Powders |
|---|---|---|---|---|
| I. Kansal et al. [18] | SiO2 (purity > 99.5%), CaCO3 (>99.5%), MgCO3 (>99%), Na2CO3(>99%), CaF2 (>99.9%), NH4H2PO4 (>99%) | Homogenous mixture of precursors of about 100 g obtained by ball milling. | Pre-heating at 900 °C for 1 h for calcination. Melting in Pt crucible at 1450–1550 °C for 1 h. | Frits are obtained by quenching of melted glass in water. Frits are dried and then milled in agate mill. Powders are sieved to obtain a mean particle size of about 10 μm. |
| D. U. Tulyaganov et al. [22] | SiO2 (purity>99.5%), CaCO3 (>99.5%), 4MgCO3∙Mg(OH)2∙5H2O (>99%), Na2CO3 (>99%), CaF2 (>99%), NH4H2PO4 (>99%) | Homogenous mixture of precursors of about 100 g obtained by ball milling. | Pre-heating at 1000 °C for 1 h for decarbonization. Melting in Pt crucible at 1400 °C for 1 h. | Frits are obtained by quenching of melted glass in water. Frits are dried and then milled in a porcelain mill. Powders are sieved to obtain a mean particle size of 11–14 μm. |
| S. I. Schmitz et al. [23] | SiO2 (purity > 99.5%), CaCO3 (>99.5%), 4MgCO3·Mg(OH)2·5H2O (>99%), Na2CO3 (>99%), CaF2 (>99%), NH4H2PO4 (>99%) | Homogenous mixture of precursors. | Pre-heating at 1000 °C for 1 h for decarbonization. Melting in Pt-crucible at 1400 °C for 1 h. | Frits are obtained by quenching of melted glass in deionized water. Frits are dried and then milled in a planetary mill. Powders are sieved to obtain a final particle size <32 μm. |
| D. U. Tulyaganov et al. [24] | SiO2 (purity > 99.5%), CaCO3 (>99.5%), MgCO3 (>99%), Na2CO3 (>99%), CaF2 (>99%), NH4H2PO4 (>99%) | Homogenous mixture of precursors. | Pre-heating at 1000 °C for 1 h for decarbonization. Melting in Pt crucible at 1400 °C for 1 h. | Frits are obtained by quenching of melted glass in water. Frites are dried and then milled. Powders are sieved to obtain a mean particle size of 10–15 μm. |
| K. Dimitriadis et al. [20] | SiO2 (purity > 99.5%), CaCO3 (>99.5%), Mg(NO3)2∙6H2O (>99%), Na2CO3 (>99%), CaF2 (>99%), (NH4)2HPO4 (>99%) | Homogenous mixture of precursors of about 100 g. | Pre-heating at 900 °C for 1 h for decarbonization. Melting in Pt crucible at 1400 °C for 1 h. | Frits are obtained by quenching of melted glass in water. Frits are dried and then milled in a planetary mill. Powders are sieved to obtain a final particle size <32 μm. |
| F. Baino et al. [25] | SiO2 (purity > 99.5%), CaCO3 (>99.5%), MgCO3 (>99%), Na2CO3 (>99%), CaF2 (>99.9%), NH4H2PO4 (>99%) | Homogenous mixture of precursors of about 100 g by ball milling. | Pre-heating at 850 °C for 1 h in an Al2O3 at heating rate of 2.5 °C/min. Melting in Pt crucible at 1420 °C for 1 h. | Frits are obtained by quenching of melted glass in water. Frits are dried and then milled in a planetary mill. Powders are sieved to obtain a final particle size <56 μm. |
| K. Dimitriadis et al. [19] | SiO2 (purity > 99.8%), CaCO3 (>99%), Mg(NO3)2∙6H2O (>99%), Na2CO3 (>99.6%), CaF2 (>99%), (NH4)2HPO4 (>99%) | Homogenous mixture of precursors of about 100 g by ball milling. | Pre-heating at 900 °C for 1 h in an Al2O3 crucible at heating rate of 1.5 °C/min. Melting in Pt crucible at 1400 °C for 1 h. | Frits are obtained by rapid pouring of melted glass in water. Frits are dried and then milled in a planetary ball-mill at 400 rpm for 45 min in a YSZ milling jar. Powders are sieved to obtain a final particle size <32 μm. |
| Article | Tg (°C) | Tc (°C) | Tp (°C) |
|---|---|---|---|
| K. Dimitriadis et al. [19] | 649 ± 9 | 783 ± 2 | 815 ± 13 |
| F. Baino et al. [25] | 640 | 785 | 830 |
| K. Dimitriadis et al. [20] | 655 ± 5 | 783 ± 2 | 845 ± 13 |
| D. U. Tulyaganov et al. [24] | 607 ± 7 | - | 815 ± 13 |
| D. U. Tulyaganov et al. [22] | 590 ± 10 | - | - |
| Materials | Heat Treatment (°C) | Flexural Strength (σ, MPa) | Elastic Modulus (E, GPa) | Vickers Microhardness (HV, GPa) | Fracture Tοughness (KIC, MPa · m0.5) |
|---|---|---|---|---|---|
| 1d-derived GCs [28] | 800 | 119 ± 10 | 24 ± 6 | 6.0 ± 0.4 | 1.6 ± 0.1 |
| 850 | 171 ± 11 | 27 ± 5 | 6.1 ± 0.5 | 1.7 ± 0.1 | |
| 900 | 141 ± 6 | 22 ± 4 | 5.2 ± 0.7 | 1.4 ± 0.1 | |
| GCs containing diopside and fluorapatite [29] | 850 | 120–195 | - | - | - |
| GCs containing wollastonite and quartz [30] | 900–1000 | 98 ± 6 | - | 5.9–6.7 | - |
| GCs containing wollastonite, hydroxyapatite and fluorite [31,32] | 700–1000 | - | 89–100 | - | 4.6–5.6 |
| GCs containing wollastonite [33] | 3100 (flame-spraying) | - | 37–56 | 2.6–5.4 | - |
| GCs containing wollastonite and diopside [33] | 3100 (flame-spraying) | - | 62–77 | 2.2–6.5 | - |
| Glasses | SiO2 | CaO | MgO | P2O5 | CaF2 | Na2O |
|---|---|---|---|---|---|---|
| 1d glass (wt.%) | 46.1 | 28.7 | 8.8 | 6.2 | 5.7 | 4.5 |
| 45S5 Bioglass® (wt.%) | 45 | 24.5 | - | 6 | - | 24.5 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tulyaganov, D.U.; Agathopoulos, S.; Dimitriadis, K.; Fernandes, H.R.; Gabrieli, R.; Baino, F. The Story, Properties and Applications of Bioactive Glass “1d”: From Concept to Early Clinical Trials. Inorganics 2024, 12, 224. https://doi.org/10.3390/inorganics12080224
Tulyaganov DU, Agathopoulos S, Dimitriadis K, Fernandes HR, Gabrieli R, Baino F. The Story, Properties and Applications of Bioactive Glass “1d”: From Concept to Early Clinical Trials. Inorganics. 2024; 12(8):224. https://doi.org/10.3390/inorganics12080224
Chicago/Turabian StyleTulyaganov, Dilshat U., Simeon Agathopoulos, Konstantinos Dimitriadis, Hugo R. Fernandes, Roberta Gabrieli, and Francesco Baino. 2024. "The Story, Properties and Applications of Bioactive Glass “1d”: From Concept to Early Clinical Trials" Inorganics 12, no. 8: 224. https://doi.org/10.3390/inorganics12080224
APA StyleTulyaganov, D. U., Agathopoulos, S., Dimitriadis, K., Fernandes, H. R., Gabrieli, R., & Baino, F. (2024). The Story, Properties and Applications of Bioactive Glass “1d”: From Concept to Early Clinical Trials. Inorganics, 12(8), 224. https://doi.org/10.3390/inorganics12080224