Abstract
The aim of the current study was to evaluate the learning curve and accuracy of implant placement by young professionals using a dynamic computer-assisted surgical system for dental implant placement. Ten students tried to place eight implants with a dynamic surgical system in predefined positions on two consecutive weekends, resulting in 160 implant placements in total. Postoperatively, the positions of the implants were scanned with an intraoral scanner and compared for deviations at the entry point, the apex, as well as angular deviations to the master model. The mean values of all measurements improved; statistical significance was found for the changes in the angle as well as for the position of the implants to the apex (p < 0.001). Furthermore, the young professionals indicated subjective improvement in handling the dynamic surgery system. Navigated surgical dental implant placement can be learned quickly and can support young professionals in everyday clinical practice, especially in difficult anatomic situations.
1. Introduction
Prosthetic restoration after dental rehabilitation with implants for optimal aesthetic restoration has a special significance in dentistry and requires high surgical accuracy [1]. Conventional implant placement is performed freehand or using laboratory-made surgical guides. Both are established procedures in dental recovery. Clinically good results and patient satisfaction can be achieved in most patient cases with these procedures [2]. However, these surgical procedures have limitations and operative risks as well, especially in difficult anatomical situations such as the atrophic mandible [3]. Application errors, which are more common for younger surgeons, seem to be the main reason for malfunction [4]. Implant malposition leads to peri-implantitis and craniomandibular dysfunctions, as well as implant loss [5].
Over the last two decades, navigation systems for implantation have constantly evolved to solve these problems and are increasingly used in clinics. Initial weaknesses such as the size of the devices, complicated handling, and errors in the hardware and software significantly improved [6]. Nowadays, navigation systems enable a good alternative in dental surgery. The anatomical situation of patients’ implant region is matched with the digitized prosthetic planning system using three-dimensional imaging such as computed tomography [7]. Computed-navigation systems enable the planning of positions of implants before surgery and the adjustment of the positions in real time by visualizing the anatomic situation on a screen [8]. This technique can reduce the risk ofinjury to important anatomical structures, such as nerves, vessels, or soft tissue [9]. Compared to fully guided static navigation, surgeons can take intraoperative, situational changes into account [10]. Nevertheless, the new technique would need to be learned by experienced surgeons, which may be a reason to reject the application in daily clinical practice. However, for young professionals, dental implant surgery could become easier with the help of navigation systems [11]. Further development and adaptation of navigated implantation using virtual and augmented reality technologies should gain more impact in dental surgery [12]. Usually, 3D computed-tomography data and surgical templates taken before the implants are inserted greatly facilitate the implantation in the correct position. However, there are anatomical situations in which these established surgical procedures reach their limits, and sufficient surgical experience is required to assure optimal implant placement. Therefore, the navigation technique is a great method to promote inexperienced surgeons in their practical preparation. For this reason, younger dentists should learn to use navigation systems in their surgical training or during their studies to be able to offer the entire repertoire of dental implant surgery.
The current study aimed to assess the learning curve and accuracy of implant placement by young professionals using a real-time navigation system. In this way, new technology can be demonstrated in the education of young professionals. Besides this, the technology can also be used to expose practicing surgeons to the digital workflow of implant placement to provide clinical care to patients with difficult anatomical conditions. The hypothesis of this study is that dynamic navigation allows for a more appropriate positioning of dental implants and shortens the learning curve even by unexperienced dental professionals.
2. Materials and Methods
2.1. Study Design
First, a toothless mandible was selected from the anatomical institute of the Christian-Albrechts-University in Kiel. The mandible was transferred into acrylic and duplicated several times. This allowed the same anatomical conditions for each participant to ensure reproducibility and optimal objectivity. Eight implants were placed in a master typodont (Figure 1). A cone beam computed tomography (CBCT) recorded the exact radiological topography of the inserted implants (KaVo 3D eXam, resolution: 0.2 voxels). This topography was transferred into the computer program coDiagnostiX (Dental wings GmbH, Chemnitz, Germany) and read into the Denacam navigation system of the company mininavident AG (Liestal, Schweiz, Switzerland).

Figure 1.
Imaged is the master typodont with the eight implants, which the young professionals had to implant in the same way with the dynamic computer-assisted surgical system. The prefabricated marker has to be placed in the acrylic structure in the middle of both rami of the mandible.
Denacam is a dynamic computer-assisted surgical system and uses the principles of stereo triangulation of optical cameras. As a real-time navigation system, Denacam uses a small, prefabricated intraoral marker to coordinate the planned implant position and the real-time position of the drill during surgery. The prefabricated marker was placed between both rami of the mandible in acrylic. The surgeon detects deviations in the entry point, apex, and angle on a screen during surgery. Thus, the current drill position and the planned implant placement can be coordinated [11].
Ethical approval was obtained from the Ethic Commission of the Faculty of Medicine at the Christian-Albrechts-University, Kiel (D510/22).
2.2. Surgical Protocol
The acrylic jaw was attached to the operating table. All students received individual instructions on implant placement and the function of the Denacam navigation system. The students followed the standard Straumann drill protocol during the surgical procedure; a 1.4 mm round burr was set to define the entry point first. A 2.2 mm pilot drill followed by a 2.8 mm pilot drill, a tap drill and 3.5 mm twist drill were used. Eight Straumann® Standard Plus Tissue Level implants with a length of 10 mm and a diameter of 4.1 mm were placed in each acrylic jaw (Straumann Holding AG, Base, Switzerland) (Figure 2).
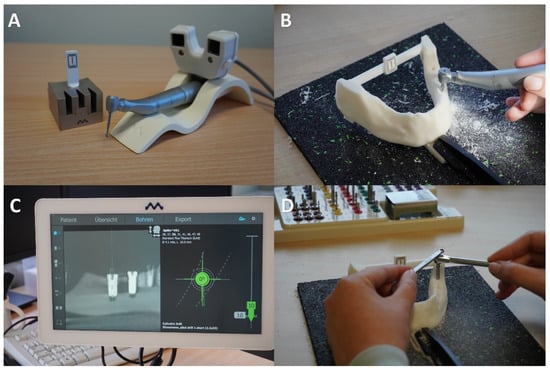
Figure 2.
Illustrated is the dynamic workflow. In (A), a young professional registered the right drill, then the drilling could be performed with the Denacam navigation system (B). In (C), the young professional could see the right position of the drill in all relevant dimensions (angle, basis, apex). In (D), the young professional placed the implant in the drilled position.
None of the students had experience in implant placement and performed their first implant operation on the acrylic jaw. After the first surgery, the students had the opportunity to practice with the Denacam navigation system. One week later, the students were able to practice again prior the second operation. Once the students felt ready, the second surgery was performed.
2.3. Evaluation of the Implant Accuracy
Each operated acrylic jaw was compared with the master typodont. A SmartPeg Type 04 from the company Osstell (Gothenburg, Sweden) was placed on each implant and scanned with the intraoral scanner TRIOS® from the company 3Shape (Copenhagen, Denmark). The data were evaluated and calculated with the coDiagnostix software afterward (Figure 3):
- Total error at the basis/entry point (vestibular, lingual, mesial, distal deviation);
- Total error at the apex (cranial, caudal deviation);
- Angular error.

Figure 3.
On the left side is a scanned and matched acrylic mandible of a student with inserted implants and screwed SmartPegs. On the right side are the computed and protocolled values.
Figure 3.
On the left side is a scanned and matched acrylic mandible of a student with inserted implants and screwed SmartPegs. On the right side are the computed and protocolled values.

The values of the individual implants from the first and last acrylic jaw each student worked on were compared. The evaluation was used to describe the learning curve of the students.
Furthermore, a short questionnaire was evaluated regarding the subjective reliability of implant placement. The questionnaire was completed by all students after the first and second day of surgery. The students described in the questionnaire what problems they encountered during implant placement in both sessions, so the individual and subjective success of each student in the second session could be identified. In this regard, the learning curve could independently checked in accordance with the results and reasons for a change could be given.
2.4. Statistical Analysis
Statistical analyses were performed using SPSS (IBM®, Ehningen, Germany). Normally distributed and non-normally distributed continuous variables were expressed as mean (±SD), and categorical data were presented as total counts. The ratio of deviations in the entry point, apex, and angle was calculated. The relation between variables was evaluated by sample t-test. Associations were considered significant when the p-value was <0.05.
3. Results
A total of 80 implants were inserted on each of the weekends (10 students, implants n = 8). The mean values and standard deviations of each parameter are shown in Table 1 as well as in Figure 4, Figure 5 and Figure 6. Statistical significance was found for the changes in the angle as well as for the position of the implants to the apex (p < 0.001). Although no significance was found for the position of the implants to the basis (p = 0.161), there was a clinical improvement.

Table 1.
Imaged are the mean values and deviations of all students from the master typodont. The deviations of the angles of the implant positions and the exact positions in vestibular/oral and mesial/distal direction (basis) as well as in cranial/caudal direction (apex) were calculated.
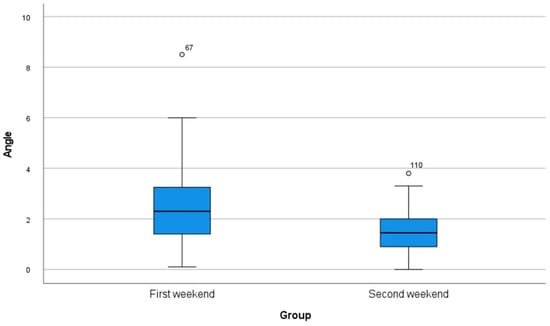
Figure 4.
Box plot of all measurements of deviations in the angle regarding the master typodont.
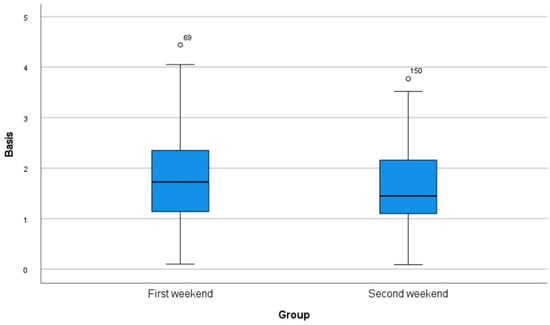
Figure 5.
Box plot of all measurements of deviations in the exact positions in vestibular/oral and mesial/distal direction (basis) regarding the master typodont.
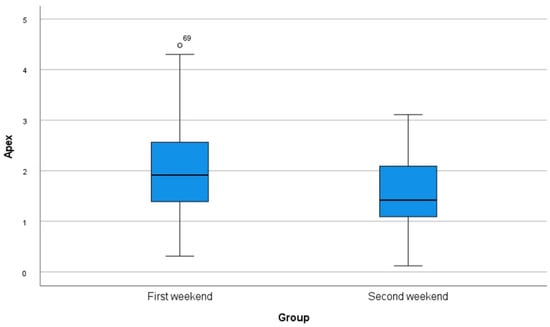
Figure 6.
Box plot of all measurements of deviations in the exact positions in cranial/caudal direction (apex) regarding the master typodont.
Table 2 and Table 3 show the responses from the questionnaire of the ten students and their subjective perception of the improvement in handling the mininavident system on the second weekend. Furthermore, the students declared their difficulties in a free response section of the questionnaire. There were problems with the coordination of the handpiece and the monitor and the detection of the marker with the camera. Other problems were the weight of the handpiece and the field of view in the right distal mandible. On the second weekend, the students declared fewer problems with the operation procedure. Figure 7 and Figure 8 show some of the postoperative acrylic mandibles and present the problems, as well as the successes and the steep learning curve of the students, respectively.
Table 2.
Responses of the ten students regarding subjective reliability in using a dynamic computer-assisted surgical system in dental implant placement (first session).
Table 3.
Responses of the ten students regarding subjective reliability in using a dynamic computer-assisted surgical system in dental implant placement (second session).
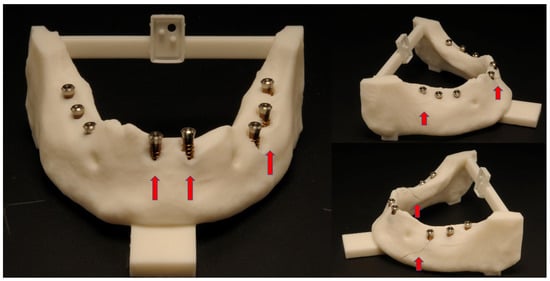
Figure 7.
The main problems during the first session were that the acrylic jaw fractured due to excessive pressure or mishandling of the implant placement. Furthermore, the correct depth was not always achieved with the drills. Some of these mistakes were shown with the red arrows.
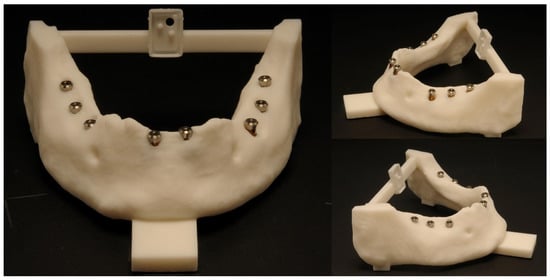
Figure 8.
Illustrated are acrylic mandibles of three different young professionals on the second session. Considerably less problems were seen on the second session; most implants could be inserted in a satisfying position.
4. Discussion
This study demonstrated substantial improvement in dental implant placement with the dynamic computer-assisted surgical system, operated by young professionals. For the students, this was the first implant placement, and the toothless acrylic jaw presented a difficult anatomical situation because no teeth or prosthetic restorations were available for orientation. Significant values were shown for the position at the apex and the angular position as well as there was an increasement for the position at the basis. Golop Deep et al. described similar results; young professionals improved significantly in speed and angulation deviation by using a dynamic navigation system [13]. Sun et al. described a steep learning curve for longitudinal and angular deviations for an experienced dentist [14]. Marques-Guasch et al. saw a decreased learning curve for a young inexperienced surgeon and concluded that the navigation technique requires a lot of practice to learn the right hand–eye coordination [15]. However, dynamic navigation could be a good alternative to the standard procedures and could enable young dentists to perform targeted and reliable therapy that is gentle on the patient [16].
Initially, the dynamic systems were used only with remaining teeth, but Feng et al. used temporary mini-implants to affix the required marker needed to place dental implants in the interforaminal region. After repeated operations with the dynamic system by an experienced surgeon, the accuracy of the implant positions improved significantly [17]. To the best knowledge of the authors, this study was the first to evaluate the accuracy and learning curve of dental implant placement by young professionals with a dynamic computer-assisted surgical system in a toothless acrylic jaw, copied from an elderly patient.
The dynamic navigation system enabled the students to place dental implants in good positions with little practice. Usually, the accuracy of virtually planned and conventionally placed implants depends on the experience of the surgeon [18]. Certainly, this study is only performed on acrylic mandibles and the handling of the system was performed outside the mouth, but experienced surgeons also demonstrated a learning curve for dynamic dental placement to achieve satisfactory results in vivo [19]. Nevertheless, students seem to be able to achieve steeper learning successes, especially with dynamic navigation [20]. While this operation procedure seems easy to master, it must be kept in mind that deviations are greater in vivo due to disruptive factors such as limited mobility, restricted mouth opening, or patient movement [21].
In the current study, the young professionals felt much more confident with the implant placement as well as the handling of the navigation system after the first weekend and another practice time on the second weekend. Only the field of view during operation appears to remain a challenge. The positioning of anterior implants seems to be easier to learn. As a right-handed person, the view of the left side is restricted (especially right posterior mandible), which makes exact drilling more difficult [13].
Furthermore, the young professionals described the coordination of the handpiece with the monitor as a problem. This could be due to the weight of the handpiece, which is occupied by the camera and complicates the operation. In addition, the detection of the marker with the camera was not easy to perform. The marker as an additional intraoral medium can also negatively influence the view. Observing the patient and the monitor correctly during the entire operation can lead to complications and inaccuracies [22,23].
On the first weekend, the students had problems with the acrylic mandible chipping and fracturing. The surface as well as the bone quality are of high importance for the accuracy of implant placement. Surgeons must learn the different patient conditions during education because every patient’s anatomy is different. Wittwer et al. described that an irregular bone condition may lead to uncontrolled shifting of the drills during surgery [24]. In addition, the type of insertion can determine the temperature formed in the bone. Gurdán et al. described that higher temperature values during implantation reduced the survival of dental implants and led to thermal osteonecrosis [25]. Finally, further surgical circumstances and conditions determine the success of dental implantation, such as the contact pressure, the wear and type of the drill or the drill speed [26].
Ultimately, a higher level of surgical experience with dynamic navigation improves the accuracy of implant placement and may also provide a good alternative in daily surgical treatment; the dynamic computer-assisted surgical system enables dentists to plan and operate on the patient quickly [27]. However, most surgeons still use conventional surgical templates, considering the cost and complexity of computer-aided guidance [28]. In many cases, this technique is adequate, but in some cases, it can have limitations [29]. Conventional surgical templates do not offer a solution for difficult anatomical conditions and insufficient field of view, so the surgeon must resort to the freehand technique [30]. Some studies have shown that the accuracy of dental implant placement with surgical navigation systems is superior to that of freehand insertion [28,31]. Zhan et al. concluded that the learning curve was steeper with the dynamic navigation technique than with the freehand technique [32]. Anatomical structures that deviate from the norm can be reasons for major inaccuracies during freehand implant placement [33] and the rate of complications could be reduced by highly accurate implant placement with dynamic surgery systems [34]. This is the reason why especially young professionals could benefit from this new technique and should learn the dynamic dental surgery in their residency. Finally, Hassfeld and Mühling recognized already in 2001 that computer technology could provide precise and reliable support to oral surgeons, as it enables much better orientation and handling, especially in difficult anatomical situations [35]. Dynamic navigation requires a higher radiation dose, more preoperative planning and higher costs; however, dynamic navigation already shows good in vivo results and offers an alternative for implant placement in complex patient cases, as well as for prosthetic restoration after extensive tumor surgery [27,36,37]. Thus, it is the responsibility of universities to show students the newest technologies and provide training for them.
The current study had also some major limitations. First, because the study was based on a small group of ten young professionals, a larger cohort study is needed to improve statistical power. Besides that, not all anatomical structures such as the inferior alveolar nerve or prosthetic sense were considered in the implant position. Furthermore, the lab conditions cannot be accurately compared to real life. The learning curve in real life happens on different patients with different anatomy and bone quality. Thus, also several types of jaw typodonts with wider problems should be compared. In the future, a large database or a prospective in vivo study for dynamic dental implant placement should be established.
5. Conclusions
The current study showed that a dynamic computer-assisted surgical system can be a good alternative in dental implant placement, especially in difficult anatomic situations. Navigated surgery in dental implant placement has a steep learning curve. Young professionals could be acclimated to this novel technology from the very beginning of their training and could use it for difficult operations in the interest of patient well-being. Finally, further studies are needed to ensure a significant conclusion about the advantages of the method for young professionals. However, training in navigated dental implantation should be encouraged and could be a helpful part in residency.
Author Contributions
Conceptualization, J.S., E.H., P.K., J.W. (Jörg Wiltfang) and A.G.; Methodology, H.W.; Software, C.F. and P.K.; Validation, H.N., J.W. (Juliane Wagner) and J.S.; Formal Analysis, H.N., J.-T.W., J.W. (Juliane Wagner) and J.W. (Jörg Wiltfang); Investigation, E.H. and J.-T.W.; Resources, C.F. and A.G.; Data Curation, E.H.; Writing—Original Draft Preparation, J.S. and E.H.; Writing—Review and Editing, P.K., J.-T.W., J.W. (Juliane Wagner), H.W., H.N., C.F., J.W. (Jörg Wiltfang) and A.G.; Visualization, H.W.; Supervision, A.G.; Project Administration, J.W. (Jörg Wiltfang); Funding Acquisition, J.S. All authors have read and agreed to the published version of the manuscript.
Funding
We acknowledge financial support by DFG within the funding programme Open Access-Publikationskosten.
Institutional Review Board Statement
The study was conducted according to the guidelines of the Declaration of Helsinki. Ethical approval was obtained from the Ethic Commission of the Faculty of Medicine at the Christian-Albrechts-University, Kiel (D510/22).
Informed Consent Statement
Written informed consent has been obtained from the participants to publish this paper.
Data Availability Statement
The data presented in this study are available on request from the corresponding author.
Conflicts of Interest
All authors declare no conflict of interest.
References
- Van Assche, N.; Vercruyssen, M.; Coucke, W.; Teughels, W.; Jacobs, R.; Quirynen, M. Accuracy of computer-aided implant placement. Clin. Oral Implant. Res. 2012, 23 (Suppl. S6), 112–123. [Google Scholar] [CrossRef] [PubMed]
- Tahmaseb, A.; Wu, V.; Wismeijer, D.; Coucke, W.; Evans, C. The accuracy of static computer-aided implant surgery: A systematic review and meta-analysis. Clin. Oral Implant. Res. 2018, 29 (Suppl. S16), 416–435. [Google Scholar] [CrossRef] [PubMed]
- Chen, L.W.; Zhao, X.E.; Yan, Q.; Xia, H.B.; Sun, Q. Dynamic navigation system-guided trans-inferior alveolar nerve implant placement in the atrophic posterior mandible: A case report. World J. Clin. Cases 2022, 10, 3907–3915. [Google Scholar] [CrossRef] [PubMed]
- Schnutenhaus, S.; Edelmann, C.; Rudolph, H.; Luthardt, R.G. Retrospective study to determine the accuracy of template-guided implant placement using a novel nonradiologic evaluation method. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. 2016, 121, e72–e79. [Google Scholar] [CrossRef] [PubMed]
- Canullo, L.; Tallarico, M.; Radovanovic, S.; Delibasic, B.; Covani, U.; Rakic, M. Distinguishing predictive profiles for patient-based risk assessment and diagnostics of plaque induced, surgically and prosthetically triggered peri-implantitis. Clin. Oral Implant. Res. 2016, 27, 1243–1250. [Google Scholar] [CrossRef]
- Wei, S.M.; Zhu, Y.; Wei, J.X.; Zhang, C.N.; Shi, J.Y.; Lai, H.C. Accuracy of dynamic navigation in implant surgery: A systematic review and meta-analysis. Clin. Oral Implant. Res. 2021, 32, 383–393. [Google Scholar] [CrossRef]
- D’Haese, J.; Ackhurst, J.; Wismeijer, D.; De Bruyn, H.; Tahmaseb, A. Current state of the art of computer-guided implant surgery. Periodontology 2000 2017, 73, 121–133. [Google Scholar] [CrossRef]
- Kim, S.G.; Lee, W.J.; Lee, S.S.; Heo, M.S.; Huh, K.H.; Choi, S.C.; Kim, T.I.; Yi, W.J. An advanced navigational surgery system for dental implants completed in a single visit: An in vitro study. J. Cranio Maxillofac. Surg. 2015, 43, 117–125. [Google Scholar] [CrossRef]
- Greenstein, G.; Tarnow, D. The mental foramen and nerve: Clinical and anatomical factors related to dental implant placement: A literature review. J. Periodontol. 2006, 77, 1933–1943. [Google Scholar] [CrossRef]
- Gargallo-Albiol, J.; Barootchi, S.; Salomo-Coll, O.; Wang, H.L. Advantages and disadvantages of implant navigation surgery. A systematic review. Ann. Anat. Anat. Anz. 2019, 225, 1–10. [Google Scholar] [CrossRef]
- Spille, J.; Jin, F.; Behrens, E.; Acil, Y.; Lichtenstein, J.; Naujokat, H.; Gulses, A.; Florke, C.; Wiltfang, J. Comparison of implant placement accuracy in two different preoperative digital workflows: Navigated vs. pilot-drill-guided surgery. Int. J. Implant. Dent. 2021, 7, 45. [Google Scholar] [CrossRef] [PubMed]
- Ayoub, A.; Pulijala, Y. The application of virtual reality and augmented reality in Oral & Maxillofacial Surgery. BMC Oral Health 2019, 19, 238. [Google Scholar] [CrossRef]
- Golob Deeb, J.; Bencharit, S.; Carrico, C.K.; Lukic, M.; Hawkins, D.; Rener-Sitar, K.; Deeb, G.R. Exploring training dental implant placement using computer-guided implant navigation system for predoctoral students: A pilot study. Eur. J. Dent. Educ. 2019, 23, 415–423. [Google Scholar] [CrossRef] [PubMed]
- Sun, T.M.; Lan, T.H.; Pan, C.Y.; Lee, H.E. Dental implant navigation system guide the surgery future. Kaohsiung J. Med. Sci. 2018, 34, 56–64. [Google Scholar] [CrossRef] [PubMed]
- Marques-Guasch, J.; Rodriguez-Bauza, R.; Satorres-Nieto, M.; Wang, H.L.; Hernandez-Alfaro, F.; Gargallo-Albiol, J. Accuracy of dynamic implant navigation surgery performed by a novice operator. A preliminary study in a cadaveric model. Int. J. Comput. Dent. 2022, 0, b2588207. [Google Scholar] [CrossRef]
- Casap, N.; Nadel, S.; Tarazi, E.; Weiss, E.I. Evaluation of a navigation system for dental implantation as a tool to train novice dental practitioners. J. Oral Maxillofac. Surg. 2011, 69, 2548–2556. [Google Scholar] [CrossRef] [PubMed]
- Feng, Y.; Yao, Y.; Yang, X. Effect of a dynamic navigation device on the accuracy of implant placement in the completely edentulous mandible: An in vitro study. J. Prosthet. Dent. 2022; in press. [Google Scholar] [CrossRef]
- Gillot, L.; Cannas, B.; Friberg, B.; Vrielinck, L.; Rohner, D.; Pettersson, A. Accuracy of virtually planned and conventionally placed implants in edentulous cadaver maxillae and mandibles: A preliminary report. J. Prosthet. Dent. 2014, 112, 798–804. [Google Scholar] [CrossRef] [PubMed]
- Block, M.S.; Emery, R.W.; Lank, K.; Ryan, J. Implant Placement Accuracy Using Dynamic Navigation. Int. J. Oral Maxillofac. Implant. 2017, 32, 92–99. [Google Scholar] [CrossRef]
- Wang, W.; Zhuang, M.; Li, S.; Shen, Y.; Lan, R.; Wu, Y.; Wang, F. Exploring training dental implant placement using static or dynamic devices among dental students. Eur. J. Dent. Educ. 2022; Online ahead of print. [Google Scholar] [CrossRef]
- Jung, R.E.; Schneider, D.; Ganeles, J.; Wismeijer, D.; Zwahlen, M.; Hammerle, C.H.; Tahmaseb, A. Computer technology applications in surgical implant dentistry: A systematic review. Int. J. Oral Maxillofac. Implant. 2009, 24, 92–109. [Google Scholar]
- Chen, C.K.; Yuh, D.Y.; Huang, R.Y.; Fu, E.; Tsai, C.F.; Chiang, C.Y. Accuracy of Implant Placement with a Navigation System, a Laboratory Guide, and Freehand Drilling. Int. J. Oral Maxillofac. Implant. 2018, 33, 1213–1218. [Google Scholar] [CrossRef]
- Lopes, A.; de Araujo Nobre, M.; Santos, D. The Workflow of a New Dynamic Navigation System for the Insertion of Dental Implants in the Rehabilitation of Edentulous Jaws: Report of Two Cases. J. Clin. Med. 2020, 9, 421. [Google Scholar] [CrossRef] [PubMed]
- Wittwer, G.; Adeyemo, W.L.; Schicho, K.; Birkfellner, W.; Enislidis, G. Prospective randomized clinical comparison of 2 dental implant navigation systems. Int. J. Oral Maxillofac. Implant. 2007, 22, 785–790. [Google Scholar]
- Gurdan, Z.; Szalma, J. Evaluation of the success and complication rates of self-drilling orthodontic mini-implants. Niger. J. Clin. Pract. 2018, 21, 546–552. [Google Scholar] [CrossRef] [PubMed]
- Gurdan, Z.; Vajta, L.; Toth, A.; Lempel, E.; Joob-Fancsaly, A.; Szalma, J. Effect of pre-drilling on intraosseous temperature during self-drilling mini-implant placement in a porcine mandible model. J. Oral Sci. 2017, 59, 47–53. [Google Scholar] [CrossRef]
- Stefanelli, L.V.; DeGroot, B.S.; Lipton, D.I.; Mandelaris, G.A. Accuracy of a Dynamic Dental Implant Navigation System in a Private Practice. Int. J. Oral Maxillofac. Implant. 2019, 34, 205–213. [Google Scholar] [CrossRef]
- Emery, R.W.; Merritt, S.A.; Lank, K.; Gibbs, J.D. Accuracy of Dynamic Navigation for Dental Implant Placement-Model-Based Evaluation. J. Oral Implantol. 2016, 42, 399–405. [Google Scholar] [CrossRef]
- Ochandiano, S.; Garcia-Mato, D.; Gonzalez-Alvarez, A.; Moreta-Martinez, R.; Tousidonis, M.; Navarro-Cuellar, C.; Navarro-Cuellar, I.; Salmeron, J.I.; Pascau, J. Computer-Assisted Dental Implant Placement Following Free Flap Reconstruction: Virtual Planning, CAD/CAM Templates, Dynamic Navigation and Augmented Reality. Front. Oncol. 2021, 11, 754943. [Google Scholar] [CrossRef]
- Cassetta, M.; Bellardini, M. How much does experience in guided implant surgery play a role in accuracy? A randomized controlled pilot study. Int. J. Oral Maxillofac. Surg. 2017, 46, 922–930. [Google Scholar] [CrossRef]
- Brief, J.; Edinger, D.; Hassfeld, S.; Eggers, G. Accuracy of image-guided implantology. Clin. Oral Implant. Res. 2005, 16, 495–501. [Google Scholar] [CrossRef]
- Zhan, Y.; Wang, M.; Cheng, X.; Li, Y.; Shi, X.; Liu, F. Evaluation of a dynamic navigation system for training students in dental implant placement. J. Dent. Educ. 2021, 85, 120–127. [Google Scholar] [CrossRef]
- Tang, T.; Huang, Z.; Liao, L.; Gu, X.; Zhang, J.; Zhang, X. Factors that Influence Direction Deviation in Freehand Implant Placement. J. Prosthodont. 2019, 28, 511–518. [Google Scholar] [CrossRef] [PubMed]
- Jorba-Garcia, A.; Gonzalez-Barnadas, A.; Camps-Font, O.; Figueiredo, R.; Valmaseda-Castellon, E. Accuracy assessment of dynamic computer-aided implant placement: A systematic review and meta-analysis. Clin. Oral Investig. 2021, 25, 2479–2494. [Google Scholar] [CrossRef] [PubMed]
- Hassfeld, S.; Muhling, J. Computer assisted oral and maxillofacial surgery--a review and an assessment of technology. Int. J. Oral Maxillofac. Surg. 2001, 30, 2–13. [Google Scholar] [CrossRef] [PubMed]
- Heiland, M.; Pohlenz, P.; Blessmann, M.; Werle, H.; Fraederich, M.; Schmelzle, R.; Blake, F.A. Navigated implantation after microsurgical bone transfer using intraoperatively acquired cone-beam computed tomography data sets. Int. J. Oral Maxillofac. Surg. 2008, 37, 70–75. [Google Scholar] [CrossRef] [PubMed]
- Kunzendorf, B.; Naujokat, H.; Wiltfang, J. Indications for 3-D diagnostics and navigation in dental implantology with the focus on radiation exposure: A systematic review. Int. J. Implant. Dent. 2021, 7, 52. [Google Scholar] [CrossRef]







Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).