
Transepithelial Gingival Depigmentation Using a New Protocol with Q-Switched Nd:YAG: An In Vivo Observational Study


 ,
,  ,
, 

Abstract
:
1. Introduction
2. Materials and Methods
2.1. Study Design and Participants
- Score 0: no clinical pigmentation (pink-colored gingiva);
- Score 1: mild clinical pigmentation (mild light brown color);
- Score 2: moderate clinical pigmentation (medium brown or mixed pink and brown);
- Score 3: heavy clinical pigmentation (deep brown or bluish-black color).
- Score 0: no pigmentation;
- Score 1: solitary unit(s) of pigmentation in the papillary gingiva without extension between neighboring solitary units;
- Score 2: formation of continuous ribbon extending from neighboring solitary units.
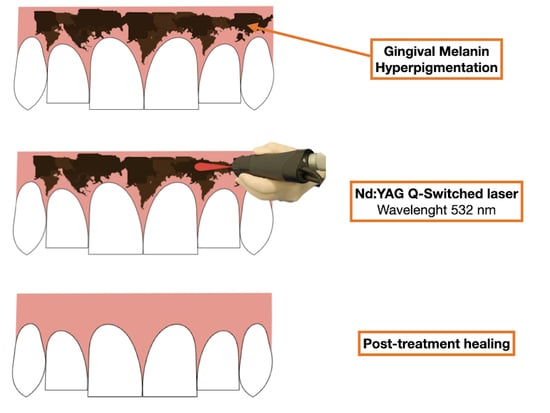
2.2. Laser Treatment
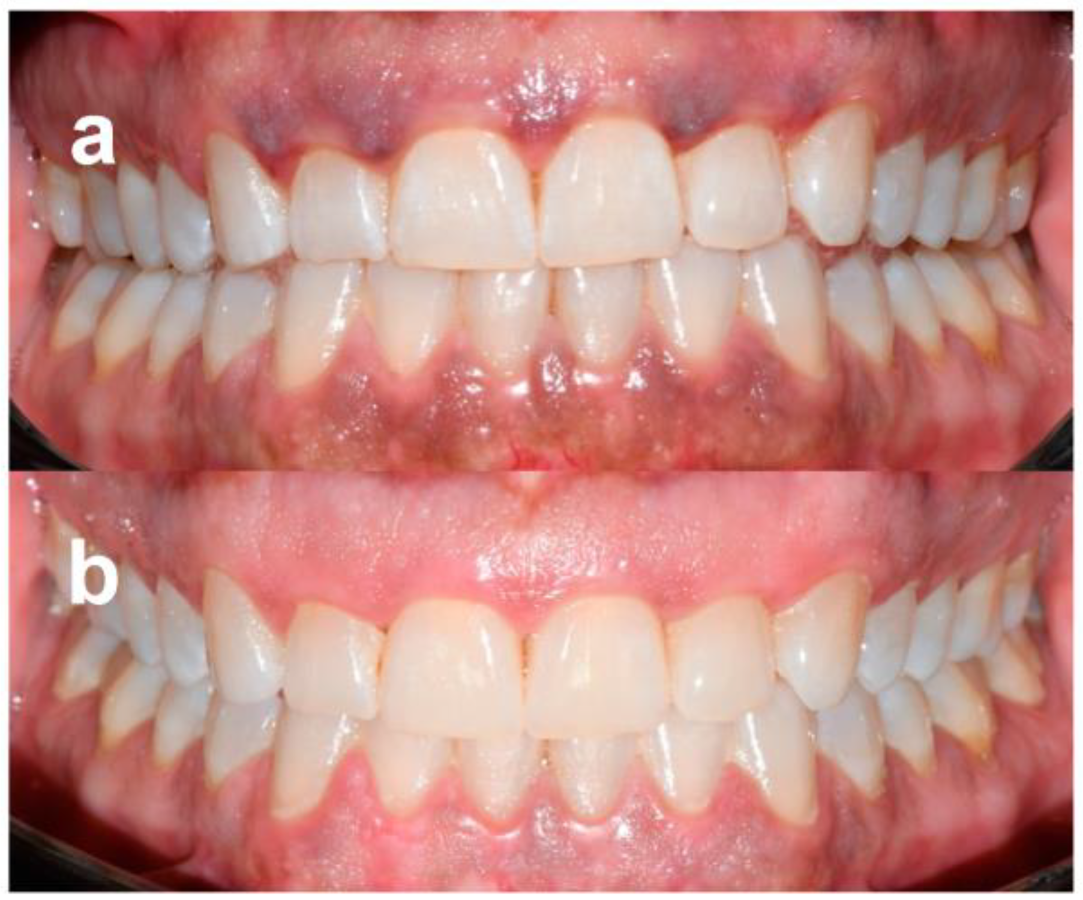
2.3. Outcomes Assessment
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Feller, L.; Masilana, A.; Khammissa, R.A.G.; Altini, M.; Jadwat, Y.; Lemmer, J. Melanin: The biophysiology of oral melanocytes and physiological oral pigmentation. Head Face Med. 2014, 10, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Squier, C.A.; Kremer, M.J. Biology of oral mucosa and esophagus. J. Natl. Cancer Inst. Monogr. 2001, 2001, 7–15. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Batra, P.; Daing, A.; Azam, I.; Miglani, R.; Bhardwaj, A. Impact of altered gingival characteristics on smile esthetics: Laypersons’ perspectives by Q sort methodology. Am. J. Orthod. Dentofac. Orthop. 2018, 154, 82–90.e2. [Google Scholar] [CrossRef] [PubMed]
- Kathariya, R.; Pradeep, A.R. Split mouth de-epithelization techniques for gingival depigmentation: A case series and review of literature. J. Indian Soc. Periodontol. 2011, 15, 161–168. [Google Scholar] [CrossRef] [PubMed]
- Murthy, M.B.; Kaur, J.; Das, R. Treatment of gingival hyperpigmentation with rotary abrasive, scalpel, and laser techniques: A case series. J. Indian Soc. Periodontol. 2012, 16, 614–619. [Google Scholar] [CrossRef]
- Gufran, K. A comparative evaluation of two different techniques for esthetic management of gingival melanin hyperpigmentation: A clinical study. J. Dent. Res. Rev. 2016, 3, 13. [Google Scholar] [CrossRef]
- Narayankar, S.D.; Deshpande, N.C.; Dave, D.H.; Thakkar, D.J. Comparative evaluation of gingival depigmentation by tetrafluroethane cryosurgery and surgical scalpel technique. A randomized clinical study. Contemp. Clin. Dent. 2017, 8, 90–95. [Google Scholar] [CrossRef]
- Sowmya, N.K.; Neeharika Sree, G.; Patil, P.; Mehta, D.S. Depigmenting effect of banana stem and flower on melanocytes. J. Oral. Biol. Craniofac. Res. 2022, 12, 454–457. [Google Scholar]
- Lin, Y.H.; Tu, Y.K.; Lu, C.T.; Chung, W.C.; Huang, C.F.; Huang, M.S.; Lu, H.K. Systematic review of treatment modalities for gingival depigmentation: A random-effects poisson regression analysis. J. Esthet. Restor. Dent. 2014, 26, 162–178. [Google Scholar] [CrossRef]
- Suragimath, G.; Lohana, M.H.; Varma, S. A split mouth randomized clinical comparative study to evaluate the efficacy of gingival depigmentation procedure using conventional scalpel tech- nique or diode laser. J. Lasers Med. Sci. 2016, 7, 227–232. [Google Scholar] [CrossRef] [Green Version]
- Ribeiro, F.V.; Cavaller, C.P.; Casarin, R.C.V.; Casati, M.Z.; Cirano, F.R.; Dutra-Corrêa, M.; Pimentel, S.P. Esthetic treatment of gingival hyperpigmentation with Nd:YAG laser or scalpel technique: A 6- month RCT of patient and professional assessment. Lasers Med. Sci. 2014, 29, 537–544. [Google Scholar] [CrossRef]
- Kishore, A.; Kathariya, R.; Deshmukh, V.; Vaze, S.; Khalia, N.; Dandgaval, R. Effectiveness of Er:YAG and CO2 lasers in the management of gingival melanin hyperpigmentation. Oral. Health Dent. Manag. 2014, 13, 486–491. [Google Scholar]
- Gholami, L.; Moghaddam, S.A.; Rigi Ladiz, M.A.; Molai Manesh, Z.; Hashemzehi, H.; Fallah, A.; Gutknecht, N. Comparison of gingival depigmentation with Er,Cr:YSGG laser and surgical stripping, a 12-month follow-up. Lasers Med. Sci. 2018, 33, 1647–1656. [Google Scholar] [CrossRef]
- Santonocito, S.; Polizzi, A.; Cavalcanti, R.; Ronsivalle, V.; Chaurasia, A.; Spagnuolo, G.; Isola, G. Impact of laser therapy on periodontal and peri-implant diseases. Photobiomodul. Photomed. Laser Surg. 2022, 40, 454–462. [Google Scholar]
- Muruppel, A.M.; Jagadish Pai, B.S.; Bhat, S.; Parker, S.; Lynch, E. Laser-assisted depigmentation-an introspection of the science, techniques, and perceptions. Dent. J. 2020, 8, 88. [Google Scholar] [CrossRef]
- Graber, E.; Iyengar, V.; Rohrer, T.; Arndt, K. Laser treatment of tattoos and pigmented lesions. In Surgery of the Skin, 2nd ed.; Elsevier: Amsterdam, The Netherlands, 2010; p. 868. [Google Scholar]
- Cannarozzo, G.; Negosanti, F.; Sannino, M.; Santoli, M.; Bennardo, L.; Banzola, N.; Negosanti, L.; Nisticò, S.P. Q-switched Nd:YAG laser for cosmetic tattoo removal. Dermatol. Ther. 2019, 32, e13042. [Google Scholar] [CrossRef]
- Herd, R.M.; Alora, M.B.; Smoller, B.; Arndt, K.A.; Dover, J.S. A clinical and histologic prospective controlled comparative study of the the picosecond titanium: Sapphire (795 nm) laser versus the Q switched alexandrite (752 nm) laser for removing tattoo pigment. J. Am. Acad. Dermatol. 1999, 40, 603–606. [Google Scholar] [CrossRef]
- Ge, Y.; Jia, G.; Lin, T. Q-switched Nd:YAG laser treatment for labial lentigines associated with Peutz-Jeghers syndrome. J. Dtsch. Dermatol. Ges. 2015, 13, 551–555. [Google Scholar] [CrossRef]
- Meleti, M.; Vescovi, P.; Mooi, W.J.; van der Waal, I. Pigmented lesions of the oral mucosa and perioral tissues: A flow-chart for the diagnosis and some recommendations for the management. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endodontol. 2008, 105, 606–616. [Google Scholar] [CrossRef]
- Dummett, C.O.; Gupta, O.P. Estimating the epidemiology of oral pigmentation. J. Natl. Med. Assoc. 1964, 56, 419–420. [Google Scholar]
- Hanioka, T.; Tanaka, K.; Ojima, M.; Yuuki, K. Association of melanin pigmentation in the gingiva of children with parents who smoke. Pediatrics 2005, 116, e186–e190. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fitzpatrick, T.B. Soleil et peau [Sun and skin]. J. Méd. Esthétique 1975, 2, 33–34. [Google Scholar]
- Frost, N.A.; Mealey, B.L.; Jones, A.A.; Huynh-Ba, G. Periodontal Biotype: Gingival Thickness as It Relates to Probe Visibility and Buccal Plate Thickness. J. Periodontol. 2015, 86, 1141–1149. [Google Scholar] [CrossRef] [PubMed]
- Shah, S.D.; Aurangabadkar, S.J. Newer trends in laser tattoo removal. J. Cutan. Aesthet Surg. 2015, 8, 25–29. [Google Scholar] [CrossRef] [PubMed]
- Hjermstad, M.J.; Fayers, P.M.; Haugen, D.F.; Caraceni, A.; Hanks, G.W.; Loge, J.H.; Fainsinger, R.; Aass, N.; Kaasa, S. Studies comparing Numerical Rating Scales, Verbal Rating Scales, and Visual Analogue Scales for assessment of pain intensity in adults: A systematic literature review. J. Pain Symptom Manag. 2011, 41, 1073–1093. [Google Scholar] [CrossRef]
- Nammour, S.; El Mobadder, M.; Namour, M.; Namour, A.; Rompen, E.; Maalouf, E.; Brugnera Junior, A.; Brugnera, A.P.; Vescovi, P.; Zeinoun, T. A Randomized Comparative Clinical Study to Evaluate the Longevity of Esthetic Results of Gingival Melanin Depigmentation Treatment Using Different Laser Wavelengths (Diode, CO2, and Er:YAG). Photobiomodul. Photomed. Laser Surg. 2020, 38, 167–173. [Google Scholar] [CrossRef]
- Moneim, R.A.A.; El Deeb, M.; Rabea, A.A. Gingival pigmentation (cause, treatment and histological preview). Future Dent. J. 2017, 3, 1–7. [Google Scholar] [CrossRef]
- Moeintaghavi, A.; Ahrari, F.; Fallahrastegar, A.; Salehnia, A. Comparison of the Effectiveness of CO2 and Diode Lasers for Gingival Melanin Depigmentation: A Randomized Clinical Trial. J. Lasers Med. Sci. 2022, 13, e8. [Google Scholar] [CrossRef]
- Altayeb, W.; Hamadah, O.; Alhaffar, B.A.; Abdullah, A.; Romanos, G. Gingival depigmentation with diode and Er,Cr:YSGG laser: Evaluating re-pigmentation rate and patient perceptions. Clin. Oral Investig. 2021, 25, 5351–5361. [Google Scholar] [CrossRef]
- Jnaid Harb, Z.K.; El-Sayed, W.; Alkhabuli, J. Gingival Depigmentation Using Diode 980 nm and Erbium-YAG 2940 nm Lasers: A Split-Mouth Clinical Comparative Study. Int. J. Dent. 2021, 2021, 9424793. [Google Scholar] [CrossRef]
- Rosa, D.S.; Aranha, A.C.; Eduardo Cde, P.; Aoki, A. Esthetic treatment of gingival melanin hyperpigmentation with Er:YAG laser: Short-term clinical observations and patient follow-up. J. Periodontol. 2007, 78, 2018–2025. [Google Scholar] [CrossRef]
- Neelakantan, P.; Liu, P.; Dummer, P.M.H.; McGrath, C. Oral health-related quality of life (OHRQoL) before and after endodontic treatment: A systematic review. Clin. Oral Investig. 2020, 24, 25–36. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Fitzpatrick Classification | |
|---|---|
| I | Pale white skin |
| II | Fair skin |
| III | Darker white to light brown skin |
| IV | Olive, light to moderate brown skin |
| V | Brown skin |
| VI | Dark brown or black skin |
| Patients | Sex | Age | Skin Type | Gingival Phenotype | OPI 1 at Baseline | MPI 2 at Baseline |
|---|---|---|---|---|---|---|
| 1. | M | 72 | III | Thick | 2 | 1 |
| 2. | F | 28 | III | Thick | 1 | 1 |
| 3. | M | 32 | IV | Thick | 2 | 2 |
| 4. | F | 21 | IV | Thin | 2 | 2 |
| 5. | F | 53 | VI | Thick | 3 | 2 |
| 6. | F | 40 | III | Thick | 2 | 2 |
| 7. | F | 49 | III | Thick | 1 | 2 |
| 8. | M | 57 | III | Thick | 2 | 1 |
| 9. | F | 36 | IV | Thick | 2 | 2 |
| 10. | F | 27 | V | Thick | 2 | 2 |
| Patient 1 | Patient 2 | Patient 3 | Patient 4 | Patient 5 | Patient 6 | Patient 7 | Patient 8 | Patient 9 | Patient 10 | |
|---|---|---|---|---|---|---|---|---|---|---|
| Laser session | 1 | 1 | 3 | 1 | 4 | 2 | 1 | 1 | 2 | 3 |
| Gingival pigmentation | ||||||||||
| Baseline | OPI = 2 MPI = 1 | OPI = 1 MPI = 1 | OPI = 2 MPI = 2 | OPI = 2 MPI = 2 | OPI = 3 MPI = 2 | OPI = 2 MPI = 2 | OPI = 1 MPI = 2 | OPI = 2 MPI = 1 | OPI = 2 MPI = 2 | OPI = 2 MPI = 2 |
| 1 session | OPI = 0 MPI = 0 | OPI = 0 MPI = 0 | OPI = 2 MPI = 1 | OPI = 0 MPI = 0 | OPI = 2 MPI = 2 | OPI = 1 MPI = 1 | OPI = 0 MPI = 0 | OPI = 0 MPI = 0 | OPI = 1 MPI = 1 | OPI = 2 MPI =1 |
| 2 session | / | / | OPI = 1 MPI = 1 | / | OPI = 2 MPI = 1 | OPI = 0 MPI = 0 | / | / | OPI = 0 MPI = 0 | OPI = 1 MPI =1 |
| 3 session | / | / | OPI = 0 MPI = 0 | / | OPI = 1 MPI = 1 | / | / | / | / | OPI = 0 MPI = 0 |
| 4 session | / | / | / | / | OPI = 0 MPI = 0 | / | / | / | / | / |
| Recurrence at 1 year of follow up | NO | NO | NO | NO | NO | NO | NO | NO | NO | NO |
| Time | Patient 1 | Patient 2 | Patient 3 | Patient 4 | Patient 5 | Patient 6 | Patient 7 | Patient 8 | Patient 9 | Patient 10 |
|---|---|---|---|---|---|---|---|---|---|---|
| Pain (NRS 1) | ||||||||||
| baseline | 0 | 1 | 2 | 3 | 3 | 2 | 0 | 1 | 2 | 2 |
| 1 day | 0 | 0 | 2 | 3 | 4 | 0 | 0 | 0 | 2 | 3 |
| 3 day | 0 | 0 | 0 | 1 | 3 | 0 | 0 | 0 | 2 | 2 |
| 5 day | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 |
| Discomfort at 12 months | ||||||||||
| Would you repeat treatment if necessary? | YES | YES | YES | YES | YES | YES | YES | YES | YES | YES |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Armogida, N.G.; Rengo, C.; Cernera, M.; Iaculli, F.; Spagnuolo, G. Transepithelial Gingival Depigmentation Using a New Protocol with Q-Switched Nd:YAG: An In Vivo Observational Study. Dent. J. 2023, 11, 2. https://doi.org/10.3390/dj11010002
Armogida NG, Rengo C, Cernera M, Iaculli F, Spagnuolo G. Transepithelial Gingival Depigmentation Using a New Protocol with Q-Switched Nd:YAG: An In Vivo Observational Study. Dentistry Journal. 2023; 11(1):2. https://doi.org/10.3390/dj11010002
Chicago/Turabian StyleArmogida, Niccolò Giuseppe, Carlo Rengo, Mariangela Cernera, Flavia Iaculli, and Gianrico Spagnuolo. 2023. "Transepithelial Gingival Depigmentation Using a New Protocol with Q-Switched Nd:YAG: An In Vivo Observational Study" Dentistry Journal 11, no. 1: 2. https://doi.org/10.3390/dj11010002
APA StyleArmogida, N. G., Rengo, C., Cernera, M., Iaculli, F., & Spagnuolo, G. (2023). Transepithelial Gingival Depigmentation Using a New Protocol with Q-Switched Nd:YAG: An In Vivo Observational Study. Dentistry Journal, 11(1), 2. https://doi.org/10.3390/dj11010002