


Use of Digital Diagnostic Aids for Initial Caries Detection: A Review





Abstract
:1. Introduction
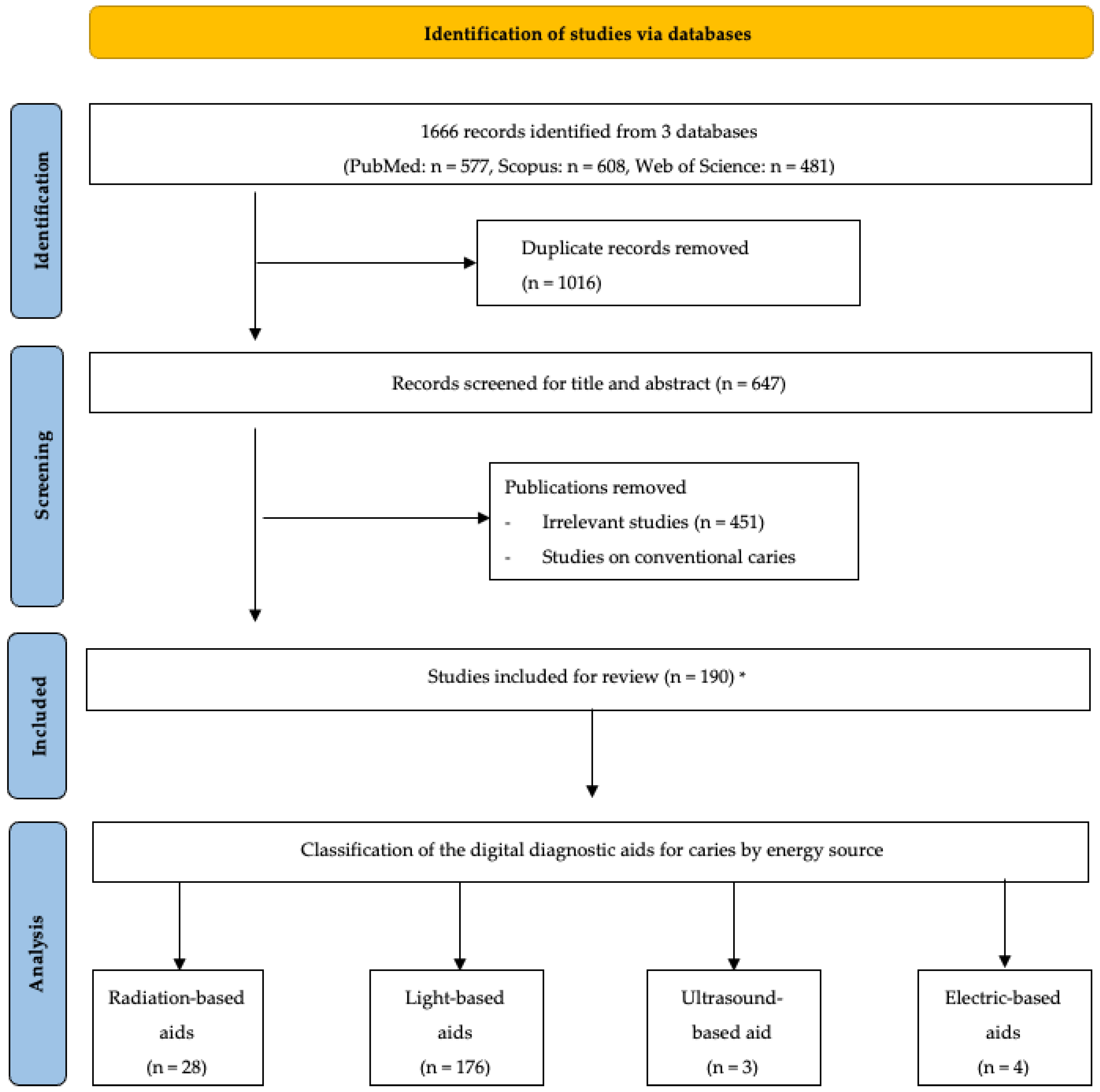
2. Literature Search
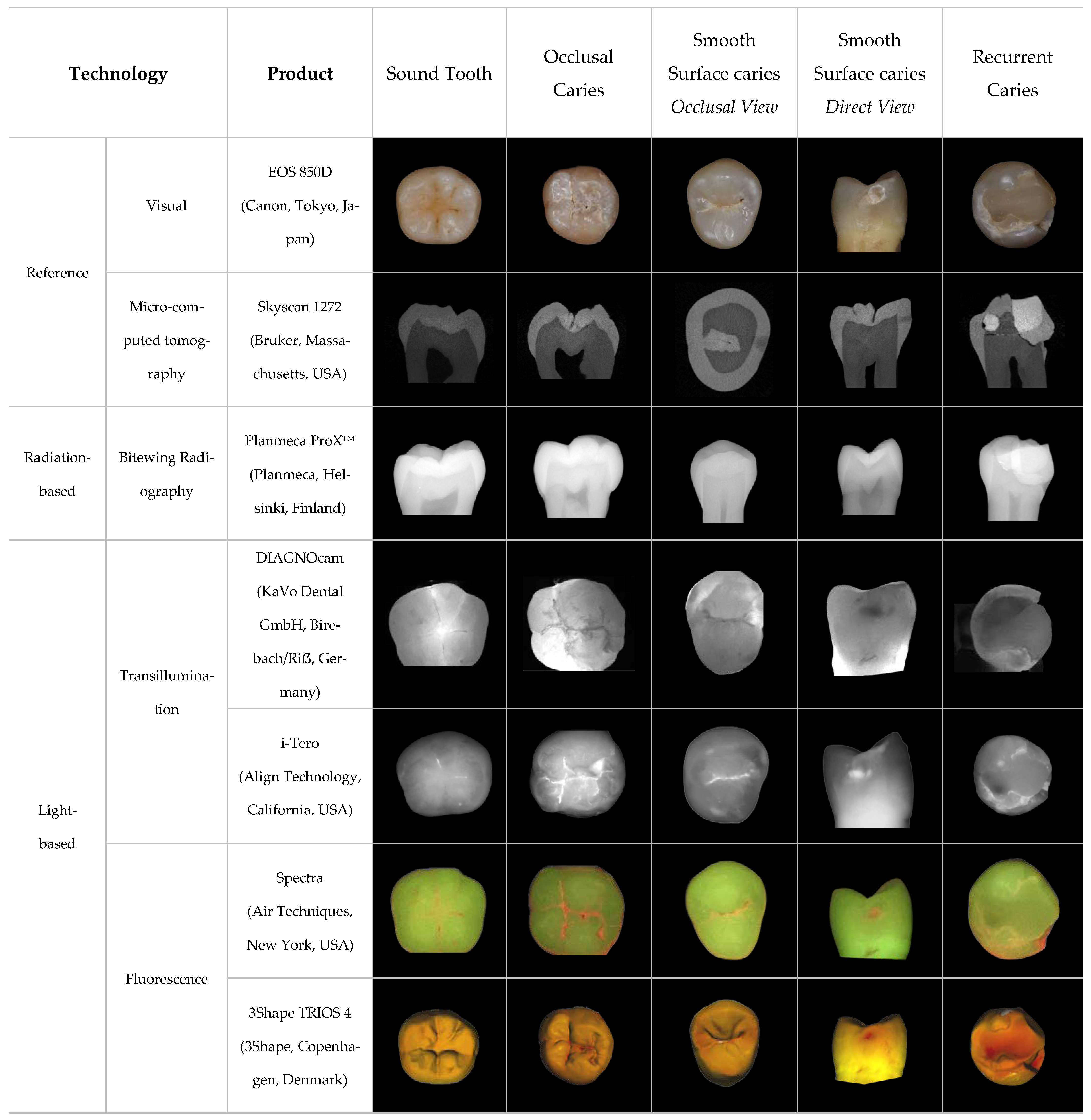
3. Digital Diagnostic Aids for Clinical Use
3.1. Radiation-Based Diagnostic Aids
3.1.1. Digital Bitewing Radiographs
3.1.2. Cone Beam-Computed Tomography
3.2. Light-Based Diagnostic Aids
3.2.1. Digital Transillumination
3.2.2. Light-Induced Fluorescence
3.2.3. Laser-Induced Fluorescence
3.3. Electric-Based Diagnostic Aids
3.3.1. Electrical Conductance Measurement
3.3.2. Alternating Current Impedance Spectroscopy
3.4. Ultrasound-Based Diagnostic Aids

{kind=link}
{kind=link}
| Category | Technology | Examples of Commercial Products | Energy Source |
|---|---|---|---|
| Radiation-based | Bitewing radiography | Planmeca ProXTM (Planmeca, Helsinki, Finland) | X-ray radiation [18] |
| Cone beam computed tomography | Planmeca ProMax 3D (Planmeca, Helsinki, Finland) | X-ray radiation [18] | |
| Light-based | Digital transillumination | DIAGNOcam (KaVo Dental GmbH, Birebach/Riẞ, Germany) | 780 nm near-infrared light [64] |
| i-Tero (Align Technology, San Jose, CA, USA) | 850 nm near-infrared light [65] | ||
| VistaCam iX intraoral camera (Durr Dental, Bietigheim-Bissingen, Germany) | 850 nm infrared light [66] | ||
| Light-induced fluorescence | Spectra (Air Techniques, New York, NY, USA) | 405 nm blue light [67] | |
| SoproLife (SOPRO, ACTEON Group, La Ciotat, France) | 450 nm blue light [37] | ||
| VistaProof (Durr Dental, Bietigheim-Bissingen, Germany) | 405 nm blue light [68] | ||
| 3Shape TRIOS 4 (3Shape, Copenhagen, Denmark) | 415 nm blue light [69] | ||
| Caries Detector (Optica Laser, Sofia, Bulgaria) | 390–420 nm near-ultraviolet light [45] | ||
| Laser-induced fluorescence | DIAGNOdent device (KaVo Dental GmbH, Birebach/Riẞ, Germany) | 655 nm red-light laser [43] | |
| DIAGNOdent Pen (KaVo Dental GmbH, Birebach/Riẞ, Germany) | 655 nm red-light laser [43] | ||
| Ultrasound-based | Ultrasonic caries detector | Ultrasonic Caries Detector (Novadent Ltd., Lod, Israel) | Ultrasonic waves [60] |
| Electric-based | Electrical conductance measurement | Ortek ECDTM electronic device (Ortek Therapeutics, New York, NY, USA) | Electric current [60] |
| Alternating current impedance spectroscopy | CarieScan PROTM (CarieScan Ltd., Dundee, Scotland) | Electric current [59] |
4. Digital Diagnostic Aids under Development
4.1. Optical Coherence Tomography
4.2. Laser-Related Caries Detection
4.2.1. Laser-Induced Thermal Imaging
4.2.2. Frequency-Domain Laser Infrared Photothermal Radiometry and Modulated Luminescence Technology
4.2.3. Laser-Induced Breakdown Spectroscopy
4.2.4. Laser-Induced Acoustic Spectroscopy
4.3. Diagnostic Interpretation Aids
5. Limitations of This Review
6. Summary
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Selwitz, R.H.; Ismail, A.I.; Pitts, N.B. Dental caries. Lancet 2007, 369, 51–59. [Google Scholar] [CrossRef] [PubMed]
- Featherstone, J.D. Dental caries: A dynamic disease process. Aust. Dent. J. 2008, 53, 286–291. [Google Scholar] [CrossRef] [PubMed]
- Conrads, G.; About, I. 1-10 Pathophysiology of Dental Caries. In Caries Excavation: Evolution of Treating Cavitated Carious Lesions; Monographs in Oral Science; Karger: Basel, Switzerland, 2018; Volume 27. [Google Scholar] [CrossRef]
- GBD 2017 Disease and Injury Incidence and Prevalence Collaborators. Global, regional, and national incidence, prevalence, and years lived with disability for 354 diseases and injuries for 195 countries and territories, 1990-2017: A systematic analysis for the Global Burden of Disease Study 2017. Lancet 2018, 392, 1789–1858. [Google Scholar] [CrossRef] [PubMed]
- Foros, P.; Oikonomou, E.; Koletsi, D.; Rahiotis, C. Detection Methods for Early Caries Diagnosis: A Systematic Review and Meta-Analysis. Caries Res. 2021, 55, 247–259. [Google Scholar] [CrossRef]
- Yu, O.Y.; Lam, W.Y.; Wong, A.W.; Duangthip, D.; Chu, C.H. Nonrestorative Management of Dental Caries. Dent. J. 2021, 9, 121. [Google Scholar] [CrossRef]
- Khandelwal, A.; Jose, J.; Ajitha, P. Early detection of dental caries—A review. Drug Invent. Today 2020, 13, 139–143. [Google Scholar]
- Gomez, J. Detection and diagnosis of the early caries lesion. BMC Oral. Health 2015, 15 (Suppl. 1), S3. [Google Scholar] [CrossRef] [PubMed]
- Lee, Y. Diagnosis and Prevention Strategies for Dental Caries. J. Lifestyle Med. 2013, 3, 107–109. [Google Scholar]
- Chong, M.J.; Seow, W.K.; Purdie, D.M.; Cheng, E.; Wan, V. Visual-tactile examination compared with conventional radiography, digital radiography, and Diagnodent in the diagnosis of occlusal occult caries in extracted premolars. Pediatr. Dent. 2003, 25, 341–349. [Google Scholar]
- Ntovas, P.; Loubrinis, N.; Maniatakos, P.; Rahiotis, C. Evaluation of dental explorer and visual inspection for the detection of residual caries among Greek dentists. J. Conserv. Dent. 2018, 21, 311–318. [Google Scholar] [CrossRef]
- Whaites, E. Essentials of Dental Radiography and Radiology; Churchill Livingstone: Edinburgh, UK; New York, NY, USA, 2002. [Google Scholar]
- Jayachandran, S. Digital Imaging in Dentistry: A Review. Contemp. Clin. Dent. 2017, 8, 193–194. [Google Scholar] [CrossRef]
- Dayo, A.F.; Wolff, M.S.; Syed, A.Z.; Mupparapu, M. Radiology of Dental Caries. Dent. Clin. N. Am. 2021, 65, 427–445. [Google Scholar] [CrossRef] [PubMed]
- Hyvönen, M.; Jaakkola, A.; Tanner, T.; Päkkilä, J.; Kämppi, A.; Patinen, P.; Tjäderhane, L.; Sipola, A.; Huumonen, S.; Anttonen, V. Quality and Findings of Bitewing Radiographs among Twenty-Year-Old Conscripts in Finland. Int. J. Dent. 2021, 2021, 8894917. [Google Scholar] [CrossRef]
- Ghodasra, R.; Patel, R.; Brizuela, M. Dental Caries Diagnostic Testing. In StatPearls; StatPearls Publishing: Treasure Island, FL, USA, 2022. [Google Scholar]
- Wenzel, A. Radiographic display of carious lesions and cavitation in approximal surfaces: Advantages and drawbacks of conventional and advanced modalities. Acta Odontol. Scand. 2014, 72, 251–264. [Google Scholar] [CrossRef]
- Walsh, T.; Macey, R.; Riley, P.; Glenny, A.M.; Schwendicke, F.; Worthington, H.V.; Clarkson, J.E.; Ricketts, D.; Su, T.L.; Sengupta, A. Imaging modalities to inform the detection and diagnosis of early caries. Cochrane Database Syst. Rev. 2021, 3, Cd014545. [Google Scholar] [CrossRef] [PubMed]
- Sun, J.; Gil, M.; Khorashadi, S.; Chen, G.; Lee, C.; Ishida, Y.; Nagai, M.; Wada, S.; Ishikawa-Nagai, S.; Da Silva, J.D. Efficacy of bisphosphonates in detection of early enamel caries using NIR fluorescence imaging and inhibition of caries progression. Int. J. Med. Sci. 2021, 18, 2971–2980. [Google Scholar] [CrossRef] [PubMed]
- Bahrololoomi, Z.; Ezoddini, F.; Halvani, N. Comparison of Radiography, Laser Fluorescence and Visual Examination for Diagnosing Incipient Occlusal Caries of Permanent First Molars. J. Dent. 2015, 12, 324–332. [Google Scholar]
- Oh, S.H.; Lee, S.R.; Choi, J.Y.; Choi, Y.S.; Kim, S.H.; Yoon, H.C.; Nelson, G. Detection of Dental Caries and Cracks with Quantitative Light-Induced Fluorescence in Comparison to Radiographic and Visual Examination: A Retrospective Case Study. Sensors 2021, 21, 1741. [Google Scholar] [CrossRef]
- Hintze, H.; Wenzel, A.; Danielsen, B.; Nyvad, B. Reliability of visual examination, fibre-optic transillumination, and bite-wing radiography, and reproducibility of direct visual examination following tooth separation for the identification of cavitated carious lesions in contacting approximal surfaces. Caries Res. 1998, 32, 204–209. [Google Scholar] [CrossRef]
- Kiljunen, T.; Kaasalainen, T.; Suomalainen, A.; Kortesniemi, M. Dental cone beam CT: A review. Phys. Med. 2015, 31, 844–860. [Google Scholar] [CrossRef]
- Kaasalainen, T.; Ekholm, M.; Siiskonen, T.; Kortesniemi, M. Dental cone beam CT: An updated review. Phys. Med. 2021, 88, 193–217. [Google Scholar] [CrossRef]
- Kalathingal, S.M.; Mol, A.; Tyndall, D.A.; Caplan, D.J. In vitro assessment of cone beam local computed tomography for proximal caries detection. Oral. Surg. Oral. Med. Oral. Pathol. Oral. Radiol. Endod. 2007, 104, 699–704. [Google Scholar] [CrossRef] [PubMed]
- Tsuchida, R.; Araki, K.; Okano, T. Evaluation of a limited cone-beam volumetric imaging system: Comparison with film radiography in detecting incipient proximal caries. Oral. Surg. Oral. Med. Oral. Pathol. Oral. Radiol. Endod. 2007, 104, 412–416. [Google Scholar] [CrossRef] [PubMed]
- Haiter-Neto, F.; Wenzel, A.; Gotfredsen, E. Diagnostic accuracy of cone beam computed tomography scans compared with intraoral image modalities for detection of caries lesions. Dentomaxillofac. Radiol. 2008, 37, 18–22. [Google Scholar] [CrossRef]
- Sansare, K.; Singh, D.; Sontakke, S.; Karjodkar, F.; Saxena, V.; Frydenberg, M.; Wenzel, A. Should cavitation in proximal surfaces be reported in cone beam computed tomography examination? Caries Res. 2014, 48, 208–213. [Google Scholar] [CrossRef]
- Donn, S.M. Chapter 21—Transillumination. In Manual of Neonatal Respiratory Care, 2nd ed.; Donn, S.M., Sinha, S.K., Eds.; Mosby: Philadelphia, PA, USA, 2006; pp. 163–164. [Google Scholar]
- Marmaneu-Menero, A.; Iranzo-Cortes, J.E.; Almerich-Torres, T.; Ortola-Siscar, J.C.; Montiel-Company, J.M.; Almerich-Silla, J.M. Diagnostic Validity of Digital Imaging Fiber-Optic Transillumination (DIFOTI) and Near-Infrared Light Transillumination (NILT) for Caries in Dentine. J. Clin. Med. 2020, 9, 420. [Google Scholar] [CrossRef] [PubMed]
- Dündar, A.; Çiftçi, M.E.; İşman, Ö.; Aktan, A.M. In vivo performance of near-infrared light transillumination for dentine proximal caries detection in permanent teeth. Saudi Dent. J. 2020, 32, 187–193. [Google Scholar] [CrossRef]
- Ortiz, M.I.G.; de Melo Alencar, C.; De Paula, B.L.F.; Magno, M.B.; Maia, L.C.; Silva, C.M. Accuracy of near-infrared light transillumination (NILT) compared to bitewing radiograph for detection of interproximal caries in the permanent dentition: A systematic review and meta-analysis. J. Dent. 2020, 98, 103351. [Google Scholar] [CrossRef]
- Laitala, M.L.; Piipari, L.; Sämpi, N.; Korhonen, M.; Pesonen, P.; Joensuu, T.; Anttonen, V. Validity of Digital Imaging of Fiber-Optic Transillumination in Caries Detection on Proximal Tooth Surfaces. Int. J. Dent. 2017, 2017, 8289636. [Google Scholar] [CrossRef]
- Korhonen, M.H.; Piipari, L.; Sämpi, N.; Pesonen, P.; Joensuu, T.; Laitala, M.L.; Anttonen, V. Challenges in Digital Imaging Fiber-Optic Transillumination Method. Dent. Adv. Res. 2019, 4, 163. [Google Scholar]
- Mohanraj, M.; Prabhu, V.; Senthil, R. Diagnostic methods for early detection of dental caries—A review. Int. J. Pedod. Rehabil. 2016, 1, 29–36. [Google Scholar]
- Abogazalah, N.; Ando, M. Alternative methods to visual and radiographic examinations for approximal caries detection. J. Oral. Sci. 2017, 59, 315–322. [Google Scholar] [CrossRef] [PubMed]
- Ahrari, F.; Akbari, M.; Mohammadi, M.; Fallahrastegar, A.; Najafi, M.N. The validity of laser fluorescence (LF) and near-infrared reflection (NIRR) in detecting early proximal cavities. Clin. Oral. Investig. 2021, 25, 4817–4824. [Google Scholar] [CrossRef]
- Macey, R.; Walsh, T.; Riley, P.; Glenny, A.M.; Worthington, H.V.; Fee, P.A.; Clarkson, J.E.; Ricketts, D. Fluorescence devices for the detection of dental caries. Cochrane Database Syst. Rev. 2020, 12, Cd013811. [Google Scholar] [CrossRef]
- Diniz, M.B.; Boldieri, T.; Rodrigues, J.A.; Santos-Pinto, L.; Lussi, A.; Cordeiro, R.C. The performance of conventional and fluorescence-based methods for occlusal caries detection: An in vivo study with histologic validation. J. Am. Dent. Assoc. 2012, 143, 339–350. [Google Scholar] [CrossRef]
- Priya, N.K.; Sowmya, N.K.; Ramakrishna, A. Lasers in dentistry—Thinking ahead…. CODS J. Dent. 2014, 6, 102–107. [Google Scholar] [CrossRef]
- Spaveras, A.; Tsakanikou, A.; Karkazi, F.; Antoniadou, M. Caries detection with laser fluorescence devices. limitations of their use. Stomatol. Edu. J. 2017, 4, 44–52. [Google Scholar] [CrossRef]
- Steier, L.; Figueiredo, J.A.P.; Blatz, M.B. Fluorescence-Enhanced Theragnosis: A Novel Approach to Visualize, Detect, and Remove Caries. Compend. Contin. Educ. Dent. 2021, 42, 460–465. [Google Scholar]
- Amaechi, B.T.; Higham, S.M. Quantitative light-induced fluorescence: A potential tool for general dental assessment. J. Biomed. Opt. 2002, 7, 7–13. [Google Scholar] [CrossRef]
- Gimenez, T.; Braga, M.M.; Raggio, D.P.; Deery, C.; Ricketts, D.N.; Mendes, F.M. Fluorescence-based methods for detecting caries lesions: Systematic review, meta-analysis and sources of heterogeneity. PLoS ONE 2013, 8, e60421. [Google Scholar] [CrossRef]
- Uzunov, T.; Uzunov, T.; Grozdanova, R.; Kosturkov, D. Diagnosis of Dentin Caries—Ultraviolet Fluorescence. Acta Medica Bulg. 2015, 41, 55–60. [Google Scholar] [CrossRef]
- Theocharopoulou, A.; Lagerweij, M.D.; van Strijp, A.J. Use of the ICDAS system and two fluorescence-based intraoral devices for examination of occlusal surfaces. Eur. J. Paediatr. Dent. 2015, 16, 51–55. [Google Scholar]
- Yadav, R. Definitions in laser technology. J. Cutan. Aesthetic Surg. 2009, 2, 45–46. [Google Scholar] [CrossRef]
- Mishra, M.B.; Mishra, S. Lasers and its Clinical Applications in Dentistry. Int. J. Dent. Clin. 2011, 3, 35–39. [Google Scholar]
- Markowitz, K.; Stenvall, R.M.; Graye, M. The effect of distance and tooth structure on laser fluorescence caries detection. Oper. Dent. 2012, 37, 150–160. [Google Scholar] [CrossRef]
- Lussi, A.; Hibst, R.; Paulus, R. DIAGNOdent: An optical method for caries detection. J. Dent. Res. 2004, 83, C80–C83. [Google Scholar] [CrossRef] [PubMed]
- Pretty, I.A.; Ellwood, R.P. The caries continuum: Opportunities to detect, treat and monitor the re-mineralization of early caries lesions. J. Dent. 2013, 41 (Suppl. 2), S12–S21. [Google Scholar] [CrossRef] [PubMed]
- Alammar, R.; Sadaf, D. Accurate Detection of Non-Cavitated Proximal Caries in Posterior Permanent Teeth: An in vivo Study. Risk Manag. Healthc. Policy 2020, 13, 1431–1436. [Google Scholar] [CrossRef]
- Bizhang, M.; Wollenweber, N.; Singh-Hüsgen, P.; Danesh, G.; Zimmer, S. Pen-type laser fluorescence device versus bitewing radiographs for caries detection on approximal surfaces. Head. Face Med. 2016, 12, 30. [Google Scholar] [CrossRef]
- Rochlen, G.K.; Wolff, M.S. Technological advances in caries diagnosis. Dent. Clin. N. Am. 2011, 55, 441–452. [Google Scholar] [CrossRef]
- Chałas, R.; Piątek, D.; Wójcik-Chęcińska, I.; Zubrzycka, J.; Bachanek, T. AC-impedance spectroscopy and caries detection. Curr. Issues Pharm. Med. Sci. 2013, 26, 344–346. [Google Scholar] [CrossRef]
- Pitts, N.B. How Electrical Caries Detection and Monitoring With CarieScan Can Help Deliver Modern Caries Management. Oral Health 2010, 100, 34. [Google Scholar]
- Chatterjee, R.; Acevedo, A.; Kleinberg, I. Comparison of the Detection of Early Occlusal Caries in Extracted Human Permanent Molar Teeth by Electrical Conductance and Biopsy Means. J. Clin. Dent. 2019, 30, 1–5. [Google Scholar] [PubMed]
- Macey, R.; Walsh, T.; Riley, P.; Glenny, A.M.; Worthington, H.V.; Clarkson, J.E.; Ricketts, D. Electrical conductance for the detection of dental caries. Cochrane Database Syst. Rev. 2021. [Google Scholar] [CrossRef]
- Mortensen, D.; Dannemand, K.; Twetman, S.; Keller, M.K. Detection of non-cavitated occlusal caries with impedance spectroscopy and laser fluorescence: An in vitro study. Open Dent. J. 2014, 8, 28–32. [Google Scholar] [CrossRef]
- Matalon, S.; Feuerstein, O.; Calderon, S.; Mittleman, A.; Kaffe, I. Detection of cavitated carious lesions in approximal tooth surfaces by ultrasonic caries detector. Oral. Surg. Oral. Med. Oral. Pathol. Oral. Radiol. Endod. 2007, 103, 109–113. [Google Scholar] [CrossRef]
- Rayleigh, L. On Waves Propagated along the Plane Surface of an Elastic Solid. Proc. Lond. Math. Soc. 1885, s1–s17, 4–11. [Google Scholar] [CrossRef]
- Ling, Y.; Song, M.; Zhonghua, S.; Xiaowu, N.; Jian, L. Theoretical imaging study of early caries by a laser induced Rayleigh wave. Appl. Opt. 2017, 56, 7182–7187. [Google Scholar] [CrossRef]
- Rodriguez Betancourt, A.; Samal, A.; Chan, H.-L.; Kripfgans, O.D. Overview of Ultrasound in Dentistry for Advancing Research Methodology and Patient Care Quality with Emphasis on Periodontal/Peri-implant Applications. Z. Für Med. Phys. 2023, 33, 336–386. [Google Scholar] [CrossRef]
- Elhennawy, K.; Askar, H.; Jost-Brinkmann, P.-G.; Reda, S.; Al-Abdi, A.; Paris, S.; Schwendicke, F. In vitro performance of the DIAGNOcam for detecting proximal carious lesions adjacent to composite restorations. J. Dent. 2018, 72, 39–43. [Google Scholar] [CrossRef]
- Schlenz, M.A.; Schupp, B.; Schmidt, A.; Wöstmann, B.; Baresel, I.; Krämer, N.; Schulz-Weidner, N. New Caries Diagnostic Tools in Intraoral Scanners: A Comparative In Vitro Study to Established Methods in Permanent and Primary Teeth. Sensors 2022, 22, 2156. [Google Scholar] [CrossRef]
- Jablonski-Momeni, A.; Jablonski, B.; Lippe, N. Clinical performance of the near-infrared imaging system VistaCam iX Proxi for detection of approximal enamel lesions. BDJ Open 2017, 3, 17012. [Google Scholar] [CrossRef] [PubMed]
- Freedman, G. (Ed.) Chapter 1—Cariology and Caries Management. In Contemporary Esthetic Dentistry; Mosby: Saint Louis, MO, USA, 2012; pp. 1–32. [Google Scholar]
- Iranzo-Cortés, J.E.; Montiel-Company, J.M.; Almerich-Torres, T.; Bellot-Arcís, C.; Almerich-Silla, J.M. Use of DIAGNOdent and VistaProof in diagnostic of Pre-Cavitated Caries Lesions-A Systematic Review and Meta-Analysis. J. Clin. Med. 2019, 9, 20. [Google Scholar] [CrossRef] [PubMed]
- Ntovas, P.; Michou, S.; Benetti, A.R.; Bakhshandeh, A.; Ekstrand, K.; Rahiotis, C.; Kakaboura, A. Occlusal caries detection on 3D models obtained with an intraoral scanner. A validation study. J. Dent. 2023, 131, 104457. [Google Scholar] [CrossRef]
- Katkar, R.A.; Tadinada, S.A.; Amaechi, B.T.; Fried, D. Optical Coherence Tomography. Dent. Clin. North. Am. 2018, 62, 421–434. [Google Scholar] [CrossRef]
- Shimada, Y.; Nakagawa, H.; Sadr, A.; Wada, I.; Nakajima, M.; Nikaido, T.; Otsuki, M.; Tagami, J.; Sumi, Y. Noninvasive cross-sectional imaging of proximal caries using swept-source optical coherence tomography (SS-OCT) in vivo. J. Biophotonics 2014, 7, 506–513. [Google Scholar] [CrossRef] [PubMed]
- Shimada, Y.; Yoshiyama, M.; Tagami, J.; Sumi, Y. Evaluation of dental caries, tooth crack, and age-related changes in tooth structure using optical coherence tomography. Jpn. Dent. Sci. Rev. 2020, 56, 109–118. [Google Scholar] [CrossRef] [PubMed]
- Macey, R.; Walsh, T.; Riley, P.; Hogan, R.; Glenny, A.M.; Worthington, H.V.; Clarkson, J.E.; Ricketts, D. Transillumination and optical coherence tomography for the detection and diagnosis of enamel caries. Cochrane Database Syst. Rev. 2021, 1, Cd013855. [Google Scholar] [CrossRef] [PubMed]
- Zakian, C.M.; Taylor, A.M.; Ellwood, R.P.; Pretty, I.A. Occlusal caries detection by using thermal imaging. J. Dent. 2010, 38, 788–795. [Google Scholar] [CrossRef]
- Nicolaides, L.; Feng, C.; Mandelis, A.; Abrams, S.H. Quantitative dental measurements by use of simultaneous frequency-domain laser infrared photothermal radiometry and luminescence. Appl. Opt. 2002, 41, 768–777. [Google Scholar] [CrossRef]
- Jeon, R.J.; Matvienko, A.; Mandelis, A.; Abrams, S.H.; Amaechi, B.T.; Kulkarni, G. Detection of interproximal demineralized lesions on human teeth in vitro using frequency-domain infrared photothermal radiometry and modulated luminescence. J. Biomed. Opt. 2007, 12, 034028. [Google Scholar] [CrossRef] [PubMed]
- Singh, V.K.; Rai, A.K. Potential of laser-induced breakdown spectroscopy for the rapid identification of carious teeth. Lasers Med. Sci. 2011, 26, 307–315. [Google Scholar] [CrossRef]
- da Silva, E.J.; de Miranda, E.M.; Mota, C.; Das, A.; Gomes, A.S.L. Photoacoustic imaging of occlusal incipient caries in the visible and near-infrared range. Imaging Sci. Dent. 2021, 51, 107–115. [Google Scholar] [CrossRef]
- Das, A.; Raposo, G.C.C.; Lopes, D.S.; da Silva, E.J.; Carneiro, V.S.M.; Mota, C.; Amaral, M.M.; Zezell, D.M.; Barbosa-Silva, R.; Gomes, A.S.L. Exploiting Nanomaterials for Optical Coherence Tomography and Photoacoustic Imaging in Nanodentistry. Nanomaterials 2022, 12, 506. [Google Scholar] [CrossRef] [PubMed]
- GalvÃo, N.S.; Nascimento, E.H.L.; GaÊta-Araujo, H.; Freitas, D.Q.; Haiter-Neto, F.; Oliveira, M.L. Automatic exposure compensation and subjective image enhancement in the radiographic diagnosis of caries. Braz. Oral Res. 2020, 34, e082. [Google Scholar] [CrossRef]
- Yoshiura, K.; Nakayama, E.; Shimizu, M.; Goto, T.K.; Chikui, T.; Kawazu, T.; Okamura, K. Effects of the automatic exposure compensation on the proximal caries diagnosis. Dentomaxillofac. Radiol. 2005, 34, 140–144. [Google Scholar] [CrossRef]
- Schwendicke, F.; Cejudo Grano de Oro, J.; Garcia Cantu, A.; Meyer-Lueckel, H.; Chaurasia, A.; Krois, J. Artificial Intelligence for Caries Detection: Value of Data and Information. J. Dent. Res. 2022, 101, 1350–1356. [Google Scholar] [CrossRef] [PubMed]


Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chan, E.K.; Wah, Y.Y.; Lam, W.Y.-H.; Chu, C.-H.; Yu, O.Y. Use of Digital Diagnostic Aids for Initial Caries Detection: A Review. Dent. J. 2023, 11, 232. https://doi.org/10.3390/dj11100232
Chan EK, Wah YY, Lam WY-H, Chu C-H, Yu OY. Use of Digital Diagnostic Aids for Initial Caries Detection: A Review. Dentistry Journal. 2023; 11(10):232. https://doi.org/10.3390/dj11100232
Chicago/Turabian StyleChan, Emma Kay, Yuet Ying Wah, Walter Yu-Hang Lam, Chun-Hung Chu, and Ollie Yiru Yu. 2023. "Use of Digital Diagnostic Aids for Initial Caries Detection: A Review" Dentistry Journal 11, no. 10: 232. https://doi.org/10.3390/dj11100232
APA StyleChan, E. K., Wah, Y. Y., Lam, W. Y.-H., Chu, C.-H., & Yu, O. Y. (2023). Use of Digital Diagnostic Aids for Initial Caries Detection: A Review. Dentistry Journal, 11(10), 232. https://doi.org/10.3390/dj11100232