

Smartphone Applications in Dentistry: A Scoping Review

 , ,
, ,  and
and 
Abstract
:1. Introduction
- -
- Analyze the latest literature regarding the prevention, management, and monitoring of oral diseases using MHAs;
- -
- Evaluate the clinical outcomes of MHAs in different fields of dentistry among people of different ages;
- -
- Define future perspectives for the research on MHAs.
2. Materials and Methods
2.1. Focused Questions
2.2. Eligibility Criteria
- (I)
- Study model: interventional studies, observational studies, cohort studies, case series/case reports studies;
- (II)
- Participants: adolescents, adolescents with fixed orthodontic appliances, mothers of small children, oral practitioners, patients with severe apnea–hypopnea sleep obstructive syndrome, elderly patients affected by systemic disease or having relied on oral health care professionals, patients with fixed orthodontic appliances, dental practice patients, children, adult patients, healthy dental students;
- (III)
- Interventions: use of MHAs related to oral healthcare;
- (IV)
- Outcome: clinical results of the use of MHAs related to oral healthcare.
- (I)
- Abstracts of articles written and published in languages different from English;
- (II)
- Duplicate studies;
- (III)
- Non-relevant studies (full-text articles whose purpose was not appropriate to answer the focused questions; analysis of different supplementary treatments; full-text content not corresponding to the abstract);
- (IV)
- No Ethics Committee approval was provided;
- (V)
- Narrative reviews, systematic reviews, or systematic and meta-analysis reviews.
2.3. Search Strategy
2.4. Research
2.5. Quality Assessment of Included Studies
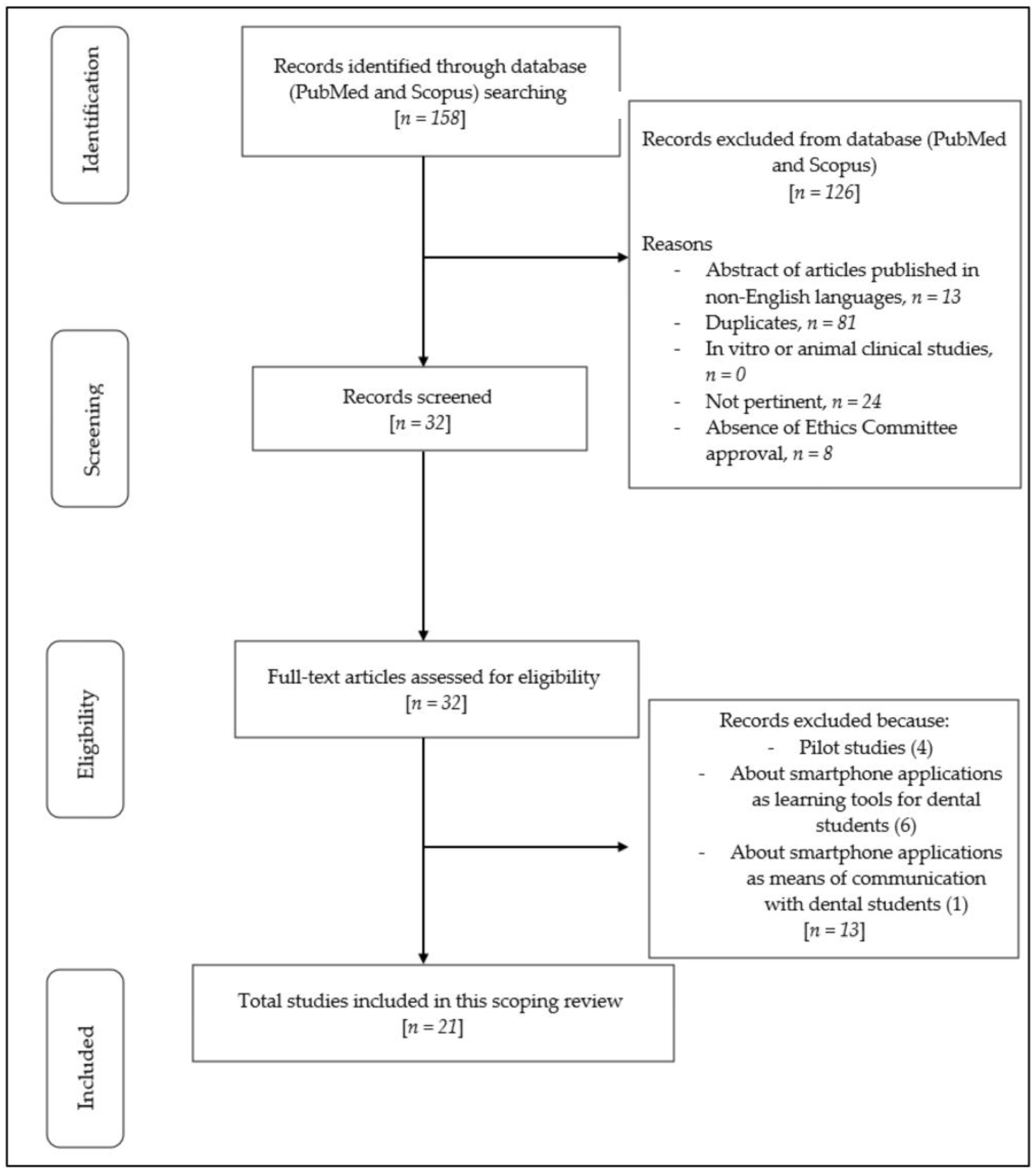
3. Results
Risk of Bias
4. Discussion
4.1. Oral Hygiene
4.2. Children’s Oral Health
4.3. Severe Apnea–Hypopnea Sleep Obstructive Syndrome
4.4. Compliance and Duration of Treatment of Orthodontic Patients
4.5. Oral Care and Swallowing-Related Quality of Living in Elderly Age
4.6. Dental Anxiety
4.7. Traumatic Dental Injuries
4.8. Dental Erosion
4.9. Awake Bruxism
4.10. Limitations and Future Perspectives
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Luxton, D.D.; McCann, R.A.; Bush, N.E.; Mishkind, M.C.; Reger, G.M. mHealth for mental health: Integrating smartphone technology in behavioral healthcare. Prof. Psychol. Res. Pract. 2011, 42, 505–512. [Google Scholar] [CrossRef]
- Underwood, B.; Birdsall, J.; Kay, E. The use of a mobile app to motivate evidence-based oral hygiene behaviour. Br. Dent. J. 2015, 219, E2. [Google Scholar] [CrossRef] [PubMed]
- Kebede, M.M.; Liedtke, T.P.; Möllers, T.; Pischke, C.R. Characterizing active ingredients of ehealth interventions targeting persons with poorly controlled type 2 diabetes mellitus using the behavior change techniques taxonomy: Scoping review. J. Med. Internet Res. 2017, 19, e348. [Google Scholar] [CrossRef] [PubMed]
- Nelligan, R.K.; Hinman, R.S.; Atkins, L.; Bennell, K.L. A short message service intervention to support adherence to home-based strengthening exercise for people with knee osteoarthritis: Intervention design applying the behavior change Wheel. JMIR mHealth uHealth 2019, 7, e14619. [Google Scholar] [CrossRef] [PubMed]
- Badawy, S.M.; Shah, R.; Beg, U.; Heneghan, M.B. Habit strength, medication adherence, and habit-based mobile health interventions across chronic medical conditions: Systematic review. J. Med. Internet Res. 2020, 22, e17883. [Google Scholar] [CrossRef]
- Estai, M.; Bunt, S.M.; Esther, K.; Marc, T. The use of mobile health applications in school dental screening. Aust. Dent. J. 2017, 62, 394–396. [Google Scholar] [CrossRef]
- Gandini, P.; Scribante, A. Clinical Applications for Dentistry and Oral Health. Appl. Sci. 2023, 13, 2428. [Google Scholar] [CrossRef]
- Dawood, A.; Marti, B.M.; Sauret-Jackson, V.; Darwood, A. 3D printing in dentistry. Br. Dent. J. 2015, 219, 521–529. [Google Scholar] [CrossRef]
- Stanley, M.; Paz, A.G.; Miguel, I.; Coachman, C. Fully digital workflow, integrating dental scan, smile design and CAD-CAM: Case report. BMC Oral Health 2018, 18, 134. [Google Scholar] [CrossRef]
- Thurzo, A.; Urbanová, W.; Neuschlová, I.; Paouris, D.; Čverha, M. Use of optical scanning and 3d printing to fabricate customized appliances for patients with craniofacial disorders. Semin. Orthod. 2022, 28, 92–99. [Google Scholar] [CrossRef]
- Nguyen, T.T.; Larrivée, N.; Lee, A.; Bilaniuk, O.; Durand, R. Use of Artificial Intelligence in Dentistry: Current Clinical Trends and Research Advances. Dent. News 2021, 28, 50–57. [Google Scholar] [CrossRef]
- Thurzo, A.; Urbanová, W.; Novák, B.; Czako, L.; Siebert, T.; Stano, P.; Mareková, S.; Fountoulaki, G.; Kosnáčová, H.; Varga, I. Where Is the Artificial Intelligence Applied in Dentistry? Systematic Review and Literature Analysis. Healthcare 2022, 10, 1269. [Google Scholar] [CrossRef] [PubMed]
- Strunga, M.; Urban, R.; Surovková, J.; Thurzo, A. Artificial Intelligence Systems Assisting in the Assessment of the Course and Retention of Orthodontic Treatment. Healthcare 2023, 11, 683. [Google Scholar] [CrossRef] [PubMed]
- Maqsood, A.; Sadiq, M.S.K.; Mirza, D.; Ahmed, N.; Lal, A.; Alam, M.K.; Bin Halim, M.S. The Teledentistry, Impact, Current Trends, and Application in Dentistry: A Global Study. BioMed Res. Int. 2021, 2021, 5437237. [Google Scholar] [CrossRef] [PubMed]
- Wang, L.; Ren, J.; Fiscella, K.A.; Bullock, S.; Sanders, M.R.; Loomis, E.L.; Eliav, E.; Mendoza, M.; Cacciato, R.; Thomas, M.; et al. Interprofessional collaboration and smartphone use as promising strategies to improve prenatal oral health care utilization among US underserved women: Results from a qualitative study. BMC Oral Health 2020, 20, 333. [Google Scholar] [CrossRef]
- Tiffany, B.; Blasi, P.; Catz, S.L.; McClure, J.B. Mobile apps for oral health promotion: Content review and heuristic usability analysis. JMIR mHealth uHealth 2018, 6, e11432. [Google Scholar] [CrossRef]
- Fijačko, N.; Gosak, L.; Cilar, L.; Novšak, A.; Creber, R.M.; Skok, P.; Štiglic, G. The effects of gamification and oral self-care on oral hygiene in children: Systematic search in app stores and evaluation of apps. JMIR mHealth uHealth 2020, 8, e16365. [Google Scholar] [CrossRef]
- Chen, R.; Santo, K.; Wong, G.; Sohn, W.; Spallek, H.; Chow, C.; Irving, M. Mobile Apps for Dental Caries Prevention: Systematic Search and Quality Evaluation. JMIR mHealth uHealth 2021, 9, e19958. [Google Scholar] [CrossRef]
- Patil, S.; Hedad, I.A.; Jafer, A.A.; Abutaleb, G.K.; Arishi, T.M.; Arishi, S.A.; Arishi, H.A.; Jafer, M.; Gujar, A.N.; Khan, S.; et al. Effectiveness of mobile phone applications in improving oral hygiene care and outcomes in orthodontic patients. J. Oral Biol. Craniofacial Res. 2021, 11, 26–32. [Google Scholar] [CrossRef]
- Thurzo, A.; Strunga, M.; Havlínová, R.; Reháková, K.; Urban, R.; Surovková, J.; Kurilová, V. Smartphone-Based Facial Scanning as a Viable Tool for Facially Driven Orthodontics? Sensors 2022, 22, 7752. [Google Scholar] [CrossRef]
- El Hajj, H.K.; Fares, Y.; Abou-Abbas, L. Assessment of dental anxiety and dental phobia among adults in Lebanon. BMC Oral Health 2021, 21, 2–10. [Google Scholar] [CrossRef]
- Zhang, C.; Ran, L.; Chai, Z.; Yu, C.; Song, J. The design, development and usability testing of a smartphone-based mobile system for management of children’s oral health. Health Inform. J. 2022, 28, 14604582221113432. [Google Scholar] [CrossRef] [PubMed]
- Abduljalil, H.S.; Abuaffan, A.H. Knowledge and practice of mothers in relation to dental health of pre- school children. Adv. Genet. Eng. 2016, 5, 1–7. [Google Scholar] [CrossRef]
- Di, R.; Li, G. Use of a Smartphone Medical App Improves Complications and Quality of Life in Patients with Nasopharyngeal Carcinoma Who Underwent Radiotherapy and Chemotherapy. Experiment 2018, 24, 6151–6156. [Google Scholar] [CrossRef]
- Manfredini, D.; Bracci, A.; Djukic, G. BruxApp: The ecological momentary assessment of awake bruxism. Minerva Stomatol. 2016, 65, 252–255. [Google Scholar]
- Vaid, N.R.; Hansa, I.; Bichu, Y. Smartphone applications used in orthodontics: A scoping review of scholarly literature. J. World Fed. Orthod. 2020, 9, S67–S73. [Google Scholar] [CrossRef]
- Ben-Omran, M.O.; Livinski, A.A.; Kopycka-Kedzierawski, D.T.; Boroumand, S.; Williams, D.; Weatherspoon, D.J.; Iafolla, T.J.; Fontelo, P.; Dye, B.A. The use of teledentistry in facilitating oral health for older adults: A scoping review. J. Am. Dent. Assoc. 2021, 152, 998–1011.e17. [Google Scholar] [CrossRef]
- Tufanaru, C.; Aromataris, E.; Campbell, J.; Hopp, L. JBI Manual for Evidence Synthesis. 2020. Available online: https://synthesismanual.jbi.global (accessed on 24 April 2023).
- Tricco, A.C.; Lillie, E.; Zarin, W.; O’Brien, K.K.; Colquhoun, H.; Levac, D.; Moher, D.; Peters, M.D.; Horsley, T.; Weeks, L.; et al. PRISMA extension for scoping reviews (PRISMA-ScR): Checklist and explanation. Ann. Intern. Med. 2018, 169, 467–473. [Google Scholar] [CrossRef]
- Choi, E.; Mun, S.; Han, S.; Kang, J.; Choi, J.; Noh, H. Learning outcomes of a mobile application for dental infection control education. J. Dent. Educ. 2022, 86, 1678–1684. [Google Scholar] [CrossRef]
- Golshah, A.; Dehdar, F.; Imani, M.M.; Nikkerdar, N. Efficacy of smartphone-based Mobile learning versus lecture-based learning for instruction of Cephalometric landmark identification. BMC Med. Educ. 2020, 20, 287. [Google Scholar] [CrossRef]
- Humm, V.; Wiedemeier, D.; Attin, T.; Schmidlin, P.; Gartenmann, S. Treatment Success and User-Friendliness of An Electric Toothbrush App: A Pilot Study. Dent. J. 2020, 8, 97. [Google Scholar] [CrossRef] [PubMed]
- Khatoon, B.; Hill, K.B.; Walmsley, A.D. Instant Messaging in Dental Education. J. Dent. Educ. 2015, 79, 1471–1478. [Google Scholar] [CrossRef] [PubMed]
- Matos Lamenha-Lins, R.; Maria de Carvelho Pugliesi, D.; José Camello de Lima, F.; Regina Oliveira Moreira, A.; Gonçalves Correia de Leite de Marcelos, P.; Dos Santos, V.E., Jr. Mobile application as a learning tool for improving dental students’ knowledge regarding dental trauma. Eur. J. Dent. Educ. 2022, 26, 700–706. [Google Scholar] [CrossRef] [PubMed]
- Mergany, N.N.; Dafalla, A.-E.; Awooda, E. Effect of mobile learning on academic achievement and attitude of Sudanese dental students: A preliminary study. BMC Med. Educ. 2021, 21, 121. [Google Scholar] [CrossRef]
- Moylan, H.B.; Carrico, C.K.; Lindauer, S.J.; Tüfekçi, E. Accuracy of a smartphone-based orthodontic treatment–monitoring application: A pilot study. Angle Orthod. 2019, 89, 727–733. [Google Scholar] [CrossRef]
- Panchal, V.; Gurunathan, D.; Shanmugaavel, A.K. Smartphone application as an aid in determination of caries risk and prevention: A pilot study. Eur. J. Dent. 2017, 11, 469–474. [Google Scholar] [CrossRef]
- Singh, R.P.; Gopalakrishnapillai, A.C.; Bhat, N.; Pawar, A. Perception of Dental and Medical Teaching Faculty Regarding Mobile Dental Application. J. Pharm. Bioallied Sci. 2019, 11, 530–539. [Google Scholar] [CrossRef]
- Stanisic, N.; Do, C.T.; Skarping, S.; Chrcanovic, B.; Bracci, A.; Manfredini, D.; Häggman-Henrikson, B. Smartphone application to report awake bruxism: Development and testing of the Swedish version and a pilot study to evaluate family history in young adults and their parents. J. Oral Rehabil. 2023. [Google Scholar] [CrossRef]
- Suner, A.; Yilmaz, Y.; Pişkin, B. Mobile learning in dentistry: Usage habits, attitudes and perceptions of undergraduate students. PeerJ 2019, 7, e7391. [Google Scholar] [CrossRef]
- Alkadhi, O.H.; Zahid, M.N.; Almanea, R.S.; Althaqeb, H.K.; Alharbi, T.H.; Ajwa, N.M. The effect of using mobile applications for improving oral hygiene in patients with orthodontic fixed appliances: A randomised controlled trial. J. Orthod. 2017, 44, 157–163. [Google Scholar] [CrossRef]
- Alkilzy, M.; Midani, R.; Höfer, M.; Splieth, C. Improving Toothbrushing with a Smartphone App: Results of a Randomized Controlled Trial. Caries Res. 2019, 53, 628–635. [Google Scholar] [CrossRef]
- Desai, R.V.; Badrapur, N.C.; Mittapalli, H.; Srivastava, B.K.; Eshwar, S.; Jain, V. “Brush up”: An innovative technological aid for parents to keep a check of their children’s oral hygiene behaviour. Rev. Paul Pediatr. 2021, 39, e2020085. [Google Scholar] [CrossRef] [PubMed]
- Kay, E.; Shou, L. A randomised controlled trial of a smartphone application for improving oral hygiene. Br. Dent. J. 2019, 226, 508–511. [Google Scholar] [CrossRef] [PubMed]
- Ki, J.Y.; Jo, S.R.; Cho, K.S.; Park, J.E.; Cho, J.W.; Jang, J.H. Effect of Oral Health Education Using a Mobile App (OHEMA) on the Oral Health and Swallowing-Related Quality of Life in Community-Based Integrated Care of the Elderly: A Randomized Clinical Trial. Int. J. Environ. Res. Public Health 2021, 18, 11679. [Google Scholar] [CrossRef]
- Li, X.; Xu, Z.-R.; Tang, N.; Ye, C.; Zhu, X.-L.; Zhou, T.; Zhao, Z.-H. Effect of intervention using a messaging app on compliance and duration of treatment in orthodontic patients. Clin. Oral Investig. 2016, 20, 1849–1859. [Google Scholar] [CrossRef]
- Marchetti, G.; Fraiz, F.C.; Nascimento, W.M.D.; Soares, G.M.S.; Assunção, L.R.D.S. Improving adolescents’ periodontal health: Evaluation of a mobile oral health App associated with conventional educational methods: A cluster randomized trial. Int. J. Paediatr. Dent. 2018, 28, 410–419. [Google Scholar] [CrossRef] [PubMed]
- O’Connor-Reina, C.; Garcia, J.M.I.; Ruiz, E.R.; Dominguez, M.D.C.M.; Barrios, V.I.; Jardin, P.B.; Morente, J.C.C.; Iriarte, M.T.G.; Plaza, G. Myofunctional Therapy App for Severe Apnea–Hypopnea Sleep Obstructive Syndrome: Pilot Randomized Controlled Trial. JMIR mHealth uHealth 2020, 8, e23123. [Google Scholar] [CrossRef] [PubMed]
- Scheerman, J.F.M.; van Meijel, B.; van Empelen, P.; Verrips, G.H.W.; van Loveren, C.; Twisk, J.W.R.; Pakpour, A.H.; Braak, M.C.T.v.D.; Kramer, G.J.C. The effect of using a mobile application (“WhiteTeeth”) on improving oral hygiene: A randomized controlled trial. Int. J. Dent. Hyg. 2020, 18, 73–83. [Google Scholar] [CrossRef] [PubMed]
- Shirmohammadi, M.; Razeghi, S.; Shamshiri, A.R.; Mohebbi, S.Z. Impact of smartphone application usage by mothers in improving oral health and its determinants in early childhood: A randomised controlled trial in a paediatric dental setting. Eur. Arch. Paediatr. Dent. 2022, 23, 629–639. [Google Scholar] [CrossRef]
- Zolfaghari, M.; Shirmohammadi, M.; Shahhosseini, H.; Mokhtaran, M.; Mohebbi, S.Z. Development and evaluation of a gamified smart phone mobile health application for oral health promotion in early childhood: A randomized controlled trial. BMC Oral Health 2021, 21, 18. [Google Scholar] [CrossRef]
- Kanoute, A.; Carrouel, F.; Gare, J.; Dieng, S.N.; Dieng, A.; Diop, M.; Faye, D.; Fraticelli, L.; Bourgeois, D. Evaluation of Oral Hygiene-Related Mobile Apps for Children in Sub-Saharan Africa. Int. J. Environ. Res. Public Heal. 2022, 19, 12565. [Google Scholar] [CrossRef] [PubMed]
- Huang, X.; Zeng, J.; Zhao, N.; Fan, L.; Ruan, D.; Wang, J.; Hong, X.; Yu, C. Experience of using a smartphone WeChat applet for dental anxiety assessment and preoperative evaluation: A nationwide multicenter study. Front. Public Health 2022, 10, 900899. [Google Scholar] [CrossRef] [PubMed]
- Butera, A.; Maiorani, C.; Gallo, S.; Pascadopoli, M.; Buono, S.; Scribante, A. Dental Erosion Evaluation with Intact-Tooth Smartphone Application: Preliminary Clinical Results from September 2019 to March 2022. Sensors 2022, 22, 5133. [Google Scholar] [CrossRef] [PubMed]
- Câmara-Souza, M.B.; Carvalho, A.G.; Figueredo, O.M.C.; Bracci, A.; Manfredini, D.; Garcia, R.C.M.R. Awake bruxism frequency and psychosocial factors in college preparatory students. Cranio® 2023, 41, 178–184. [Google Scholar] [CrossRef]
- Colonna, A.; Lombardo, L.; Siciliani, G.; Bracci, A.; Guarda-Nardini, L.; Djukic, G.; Manfredini, D. Smartphone-based application for EMA assessment of awake bruxism: Compliance evaluation in a sample of healthy young adults. Clin. Oral Investig. 2019, 24, 1395–1400. [Google Scholar] [CrossRef]
- Nykänen, L.; Manfredini, D.; Lobbezoo, F.; Kämppi, A.; Bracci, A.; Ahlberg, J. Assessment of awake bruxism by a novel bruxism screener and ecological momentary assessment among patients with masticatory muscle myalgia and healthy controls. J. Oral Rehabil. 2023. [Google Scholar] [CrossRef]
- Osiewicz, M.A.; Lobbezoo, F.; Bracci, A.; Ahlberg, J.; Pytko-Polończyk, J.; Manfredini, D. Ecological Momentary Assessment and Intervention Principles for the Study of Awake Bruxism Behaviors, Part 2: Development of a Smartphone Application for a Multicenter Investigation and Chronological Translation for the Polish Version. Front. Neurol. 2019, 10, 170. [Google Scholar] [CrossRef]
- Zani, A.; Lobbezoo, F.; Bracci, A.; Ahlberg, J.; Manfredini, D. Ecological Momentary Assessment and Intervention Principles for the Study of Awake Bruxism Behaviors, Part 1: General Principles and Preliminary Data on Healthy Young Italian Adults. Front. Neurol. 2019, 10, 169. [Google Scholar] [CrossRef]
- Zaror, C.; Espinoza-Espinoza, G.; Atala-Acevedo, C.; Muñoz-Millán, P.; Li, Y.; Clarke, K.; Onetto, J.; Díaz, J.; Hallet, K.; Manton, D.; et al. Validation and usability of a mobile phone application for epidemiological surveillance of traumatic dental injuries. Dent. Traumatol. 2019, 35, 33–40. [Google Scholar] [CrossRef]
- Bourgeois, D.; Bravo, M.; Llodra, J.-C.; Inquimbert, C.; Viennot, S.; Dussart, C.; Carrouel, F. Calibrated Interdental Brushing for the Prevention of Periodontal Pathogens Infection in Young Adults—A Randomized Controlled Clinical Trial. Sci. Rep. 2019, 9, 15127. [Google Scholar] [CrossRef]
- Timmers, T.; Janssen, L.; Kool, R.B.; Kremer, J.A. Educating Patients by Providing Timely Information Using Smartphone and Tablet Apps: Systematic Review. J. Med. Internet Res. 2020, 22, e17342. [Google Scholar] [CrossRef] [PubMed]
- Hausmann, E.; Hausmann, B. Motivation—Key to patient success in mechanical plaque control. J. Am. Dent. Assoc. 1976, 92, 403–408. [Google Scholar] [CrossRef]
- National Institute for Clinical and Healthcare Excellence. Oral Health Promotion: General Dental Practice. NICE Guideline [NG30]. 2015. Available online: https://www.nice.org.uk/guidance/ng30 (accessed on 30 August 2023).
- Toniazzo, M.P.; Nodari, D.; Muniz, F.W.M.G.; Weidlich, P. Effect of mHealth in improving oral hygiene: A systematic review with meta-analysis. J. Clin. Periodontol. 2019, 46, 297–309. [Google Scholar] [CrossRef] [PubMed]
- El Tantawi, M.; Bakhurji, E.; Al-Ansari, A.; AlSubaie, A.; Al Subaie, H.A.; AlAli, A. Indicators of adolescents’ preference to receive oral health information using social media. Acta Odontol. Scand. 2019, 77, 213–218. [Google Scholar] [CrossRef]
- Anil, S.; Anand, P.S. Early Childhood caries: Prevalence, risk factors, and prevention. Front. Pediatr. 2017, 5, 157. [Google Scholar] [CrossRef]
- Chang, Y.C.; Lo, J.L.; Huang, C.J.; Hsu, N.Y.; Chu, H.H.; Wang, H.Y.; Chi, P.Y.; Hsieh, Y.L. Playful toothbrush: Ubicomp technology for teaching tooth brushing to kindergarten children. In Proceedings of the CHI ‘08: Proceedings of the SIGCHI Conference on Human Factors in Computing Systems, Florence, Italy, 5–10 April 2008; pp. 363–372. [Google Scholar]
- Morais, E.R.; Vergara, C.M.A.C.; Brito, F.O.; Sampaio, H.A.C. Serious games for children’s oral hygiene education: An integrative review and application search. Cien. Saude Colet. 2020, 25, 3299–3310. [Google Scholar] [CrossRef]
- Hanning, C.D. Laryngeal and Velopharyngeal Sensory Impairment in Obstructive Sleep Apnea. Sleep 2005, 28, 1335. [Google Scholar] [CrossRef]
- Camacho, M.; Certal, V.; Abdullatif, J.; Zaghi, S.; Ruoff, C.M.; Capasso, R.; Kushida, C.A. Myofunctional Therapy to Treat Obstructive Sleep Apnea: A Systematic Review and Meta-analysis. Sleep 2015, 38, 669–675. [Google Scholar] [CrossRef]
- Baptista, P.M.; Martin, F.; Ross, H.; O’Connor Reina, C.; Plaza, G.; Casale, M. A systematic review of smartphone applications and devices for obstructive sleep apnea. Braz. J. Otorhinolaryngol. 2022, 88 (Suppl. S5), S188–S197. [Google Scholar] [CrossRef]
- Sfondrini, M.F.; Scribante, A. New Materials and Techniques for Orthodontics. Materials 2023, 16, 1924. [Google Scholar] [CrossRef]
- Huang, J.; Yao, Y.; Jiang, J.; Li, C. Effects of motivational methods on oral hygiene of orthodontic patients: A systematic review and meta-analysis. Medicine 2018, 97, e13182. [Google Scholar] [CrossRef] [PubMed]
- Sudjalim, T.; Woods, M.; Manton, D. Prevention of white spot lesions in orthodontic practice: A contemporary review. Aust. Dent. J. 2006, 51, 284–289. [Google Scholar] [CrossRef] [PubMed]
- Loke, S.; Tan, S. Factors influencing duration of orthodontic treatment: A 12-year retrospective study. Malays. Dent. J. 2012, 34, 16–30. [Google Scholar]
- Choi, E.; Park, B.; Noh, H. Efficacy of mobile health care in patients undergoing fixed orthodontic treatment: A systematic review. Int. J. Dent. Hyg. 2021, 19, 29–38. [Google Scholar] [CrossRef]
- Baheti, M.J.; Toshniwal, N. Orthodontic apps at fingertips. Prog. Orthod. 2014, 15, 36. [Google Scholar] [CrossRef]
- Al-Moghrabi, D.; Alkadhimi, A.; Tsichlaki, A.; Pandis, N.; Fleming, P.S. The influence of mobile applications and social media-based interventions in producing behavior change among orthodontic patients: A systematic review and meta-analysis. Am. J. Orthod. Dentofac. Orthop. 2022, 161, 338–354. [Google Scholar] [CrossRef]
- Minakuchi, S.; Tsuga, K.; Ikebe, K.; Ueda, T.; Tamura, F.; Nagao, K.; Furuya, J.; Matsuo, K.; Yamamoto, K.; Kanazawa, M.; et al. Oral hypofunction in the older population: Position paper of the Japanese Society of Gerodontology in 2016. Gerodontology 2018, 35, 317–324. [Google Scholar] [CrossRef]
- Park, S.J. Dysphagia risk and associated factors among community-dwelling elders. J. Korean Soc. Food Sci. Nutr. 2015, 4, 49–56. [Google Scholar] [CrossRef]
- Yerrakalva, D.; Yerrakalva, D.; Hajna, S.; Griffin, S. Effects of Mobile Health App Interventions on Sedentary Time, Physical Activity, and Fitness in Older Adults: Systematic Review and Meta-Analysis. J. Med. Internet Res. 2019, 21, e14343. [Google Scholar] [CrossRef]
- Armfield, J.M. What goes around comes around: Revisiting the hypothesized vicious cycle of dental fear and avoidance. Community Dent. Oral Epidemiol. 2012, 41, 279–287. [Google Scholar] [CrossRef]
- Dhar, V.; Randall, C.L.; Marghalani, A.; Jayaraman, J.; Chen, C.-Y.; Wells, M.; Law, C.; Gosnell, E.; Majstorović, M.; Townsend, J.; et al. Nonpharmacological Behavior Guidance for Children During Preventive Dental Visits: A Systematic Review—Part 1. Pediatr. Dent. 2023, 45, 181–196. [Google Scholar] [PubMed]
- Cagetti, M.G.; Marcoli, P.A.; Berengo, M.; Cascone, P.; Cordone, L.; Defabianis, P.; De Giglio, O.; Esposito, N.; Federici, A.; Laino, A.; et al. Italian guidelines for the prevention and management of dental trauma in children. Ital. J. Pediatr. 2019, 45, 157. [Google Scholar] [CrossRef] [PubMed]
- van Mechelen, D.M.; van Mechelen, W.; Verhagen, E.A.L.M. Sports injury prevention in your pocket?! Prevention apps assessed against the available scientific evidence: A review. Br. J. Sports Med. 2014, 48, 878–882. [Google Scholar] [CrossRef] [PubMed]
- Iskander, M.; Lou, J.; Wells, M.; Scarbecz, M. A poster and a mobile healthcare application as information tools for dental trauma management. Dent. Traumatol. 2016, 32, 457–463. [Google Scholar] [CrossRef] [PubMed]
- Vieira Pedrosa, B.R.; de Menezes, V.A. Prevalence of Erosive Tooth Wear and Related Risk Factors in Adolescents: An Integrative Review. J. Dent. Child. 2020, 87, 18–25. [Google Scholar]
- Picos, A.; Badea, M.E.; Dumitrascu, D.L. Dental erosion in gastro-esophageal reflux disease. A systematic review. Med. Pharm. Rep. 2018, 91, 387–390. [Google Scholar] [CrossRef]
- Butera, A.; Pascadopoli, M.; Pellegrini, M.; Trapani, B.; Gallo, S.; Radu, M.; Scribante, A. Biomimetic hydroxyapatite paste for molar–incisor hypomineralization: A randomized clinical trial. Oral Dis. 2022, 29, 2789–2798. [Google Scholar] [CrossRef]
- Lobbezoo, F.; Ahlberg, J.; Raphael, K.G.; Wetselaar, P.; Glaros, A.G.; Kato, T.; Santiago, V.; Winocur, E.; De Laat, A.; De Leeuw, R.; et al. International consensus on the assessment of bruxism: Report of a work in progress. J. Oral Rehabil. 2018, 45, 837–844. [Google Scholar] [CrossRef]


{kind=link}
| Random Sequence Generation | Allocation Concealment | Blinding | Incomplete Outcome Data | Selective Reporting | |
|---|---|---|---|---|---|
| Alkadhi et al., 2017 [41] |  | | | | |
| Alkilzy et al., 2019 [42] | | | | | |
| Butera et al., 2022 [54] |  | | | | |
| Câmara-Souza et al., 2020 [55] | | | | | |
| Colonna et al., 2019 [56] | | | | | |
| Desai et al., 2021 [43] | | | | | |
| Huang et al., 2022 [53] | | | | | |
| Kanoute et al., 2022 [52] | | | | | |
| Kay et al., 2019 [44] | | | | | |
| Ki et al., 2021 [45] | | | | | |
| Li et al., 2016 [46] | | | | | |
| Marchetti et al., 2018 [47] | | | | | |
| Nykänen et al., 2023 [57] | | | | | |
| O’Connor-Reina et al., 2020 [48] | | | | | |
| Osiewicz et al., 2019 [58] | | | | | |
| Scheerman et al., 2020 [49] | | | | | |
| Shirmohammadi et al., 2022 [50] | | | | | |
| Stanisic et al., 2023 [39] | | | | | |
| Zani et al., 2019 [59] | | | | | |
| Zaror et al., 2019 [60] | | | | | |
| Zolfaghari et al., 2021 [51] | | | | | |
| References (Authors, Year of Publication, and Study Design) | No. of Participants Women (W) Men (M) | Age (Years), Mean (SD or Range) | Inclusion and Exclusion Criteria | Clinical Outcome |
|---|---|---|---|---|
| Alkadhi et al., 2017; RCT [41] | Group 1: 22 W: 11 M: 11 Group 2: 22 W: 14 M: 8 | Group 1: 16.6 ± 3.2 Group 2: 17.2 ± 5.2 | Inclusion criteria:
| Oral hygiene improvement in patients with fixed orthodontic appliances. |
| Alkilzy et al., 2019; RCT [42] | Group 1: 26 Group 2: 23 W: 27 M: 22 | 5.1 ± 0.62 | Inclusion criteria:
| Improvement in toothbrushing. |
| Butera et al., 2022; OS [54] | Group 1: 1839 W: N.R. M: N.R. Group 2: 3894 W: 2002 M: 1892 | Group 1: N.R. Group 2: 36.72 ± 14.52 | Inclusion criteria: N.R. Excluded criteria: N.R. | Dental erosion evaluation. |
| Câmara-Souza et al., 2020 [55] | 69 W: 50 M: 19 | 18.6 ± 1.5 | Inclusion criteria:
| Correlation of AB frequency with levels of anxiety, depression, stress, and OHRQoL in college preparatory students. |
| Colonna et al., 2019; OS [56] | 60 W: 35 M: 25 | 24.2 ± 4.1 | Inclusion criteria:
| Awake bruxism evaluation. |
| Desai et al., 2021; RCT [43] | Group 1: 82 Group 2: 83 Group 3: 82 W: 121 M: 126 | 4.98 ± 0.84 | Inclusion criteria:
| Improvement in children’s oral hygiene. |
| Huang et al., 2022; BAS [53] | Group 1: 180 W: 104 M: 76 Group 2: 20 W: 9 M: 11 | Group 1: 3 to 74 Group 2: N.R. | Inclusion criteria:
| Dental anxiety evaluation. |
| Kanoute et al., 2022; CSS [52] | 10 W: N.R. M: N.R. | N.R. | Inclusion criteria:
| Children’s oral hygiene evaluation. |
| Kay et al., 2019; RCT [44] | Group 1: 53 W: 34 M: 19 Group 2: 51 W: 27 M: 24 | Group 1: 36.6 ± N.R. Group 2: 39.1 ± N.R. | Inclusion criteria:
| Improvement in oral hygiene. |
| Ki et al., 2021; RCT [45] | Group 1: 20 W: 10 M: 10 Group 2: 20 W: 13 M: 7 | ≥65 | Inclusion criteria:
| Improvement in oral health and swallowing-related quality of life. |
| Li et al., 2016; RCT [46] | Group 1: 112 W: 79 M: 33 Group 2: 112 W: 77 M: 35 | Group 1: 17.6 ± 0.8 Group 2: 18.7 ± 1.0 | Inclusion criteria:
| Orthodontic patients’ compliance and duration of treatment evaluation. |
| Marchetti et al., 2018; RCT [47] | 291 W: 159 M: 132 | 16.1 ± 1.21 | Inclusion criteria:
| Adolescents’ periodontal health improvement. |
| Nykänen et al., 2023 [57] | Group 1: 68 W: 60 M: 8 Group 2: 47 W: 41M: 6 | Group 1: 45.7 ± 10.6 Group 2: 43.5 ± 9.8 | Inclusion criteria:
| AB’s prevalence evaluation. |
| O’Connor-Reina et al., 2020; RCT [48] | Group 1: 18 W: 4 M: 14 Group 2: 10 W: 2 M: 8 | Group 1: 59.17 (53.7–64.6) Group 2: 63.9 (56.4–71.38) | Inclusion criteria:
| OSAHS severity and symptoms. |
| Osiewicz et al., 2019 [58] | N.R. | N.R. | N.R. | Bruxism evaluation. |
| Scheerman et al., 2020; RCT [49] | Group 1: 67 W: 41 M: 26 Group 2: 65 W: 32 M: 33 | Group 1: 13.2 ± 1.01 Group 2: 13.5 ± 0.97 | Inclusion criteria:
| Oral hygiene improvement in patients with fixed orthodontic appliances. |
| Shirmohammadi et al., 2022; RCT [50] | Group 1: 45 Group 2: 45 W: 90 M: 0 | 35.6 ± 5.0 | Inclusion criteria:
| Children’s oral health improvement. |
| Stanisic et al., 2023 [39] | Group 1: 10 W: 6 M: 4 Group 2: 10 W: 7 M: 3 | Group 1: aged between 23 and 30 Group 2: aged between 42 and 67 | Inclusion criteria: N.R. Exclusion criteria: N.R. | Awake bruxism evaluation. |
| Zani et al., 2019 [59] | 30 W: 21 M: 9 | 24 ± 3.5 | Inclusion criteria:
| Awake bruxism evaluation. |
| Zaror et al., 2019; OS [60] | 182 W: 129 M: 53 | 36.2 ± 9.3 | Inclusion criteria:
| Traumatic dental injury evaluation. |
| Zolfaghari et al., 2021; RCT [51] | Group 1: 29 Group 2: 29 W: 58 M: 0 | Group 1: 36.5 ± 4.9 Group 2: 36.3 ± 4.5 | Inclusion criteria:
| Children’s oral health improvement. |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pascadopoli, M.; Zampetti, P.; Nardi, M.G.; Pellegrini, M.; Scribante, A. Smartphone Applications in Dentistry: A Scoping Review. Dent. J. 2023, 11, 243. https://doi.org/10.3390/dj11100243
Pascadopoli M, Zampetti P, Nardi MG, Pellegrini M, Scribante A. Smartphone Applications in Dentistry: A Scoping Review. Dentistry Journal. 2023; 11(10):243. https://doi.org/10.3390/dj11100243
Chicago/Turabian StylePascadopoli, Maurizio, Paolo Zampetti, Maria Gloria Nardi, Matteo Pellegrini, and Andrea Scribante. 2023. "Smartphone Applications in Dentistry: A Scoping Review" Dentistry Journal 11, no. 10: 243. https://doi.org/10.3390/dj11100243
APA StylePascadopoli, M., Zampetti, P., Nardi, M. G., Pellegrini, M., & Scribante, A. (2023). Smartphone Applications in Dentistry: A Scoping Review. Dentistry Journal, 11(10), 243. https://doi.org/10.3390/dj11100243