

Systematic Review and Meta Analysis of the Relative Effect on Plaque Index among Pediatric Patients Using Powered (Electric) versus Manual Toothbrushes


Abstract
:
1. Introduction
2. Materials and Methods
2.1. Human Subjects Approval
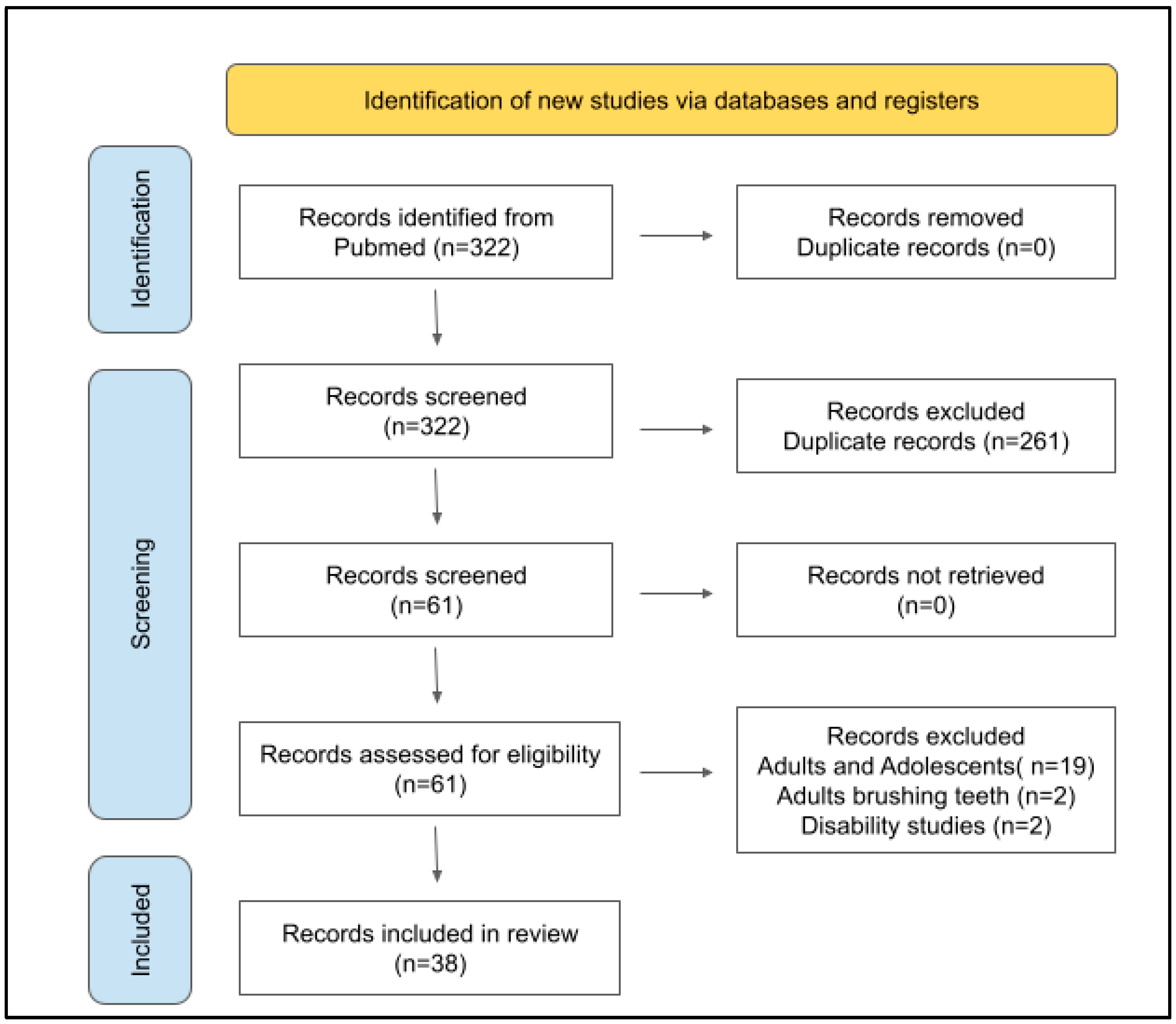
2.2. PRISMA Protocol
2.3. Two-Step Review
2.4. Data Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Grender, J.; Goyal, C.R.; Qaqish, J.; Timm, H.; Adam, R. A 12-Week Randomized Controlled Trial Comparing a Novel Electric Toothbrush with an Extra Gentle Brush Head to a Manual Toothbrush for Plaque and Gingivitis Reduction. Compend. Contin. Educ. Dent. 2022, 43, f20–f29. [Google Scholar] [PubMed]
- Nevins, M.; Chen, C.Y.; Kerr, E.; Mendoza-Azpur, G.; Isola, G.; Soto, C.P.; Stacchi, C.; Lombardi, T.; Kim, D.; Rocchietta, I. Comparison of a Novel Sonic Toothbrush to Manual Brushing on Plaque Control and Gingival Inflammation: A Multicenter, Randomized, Controlled Clinical Trial. Int. J. Periodontics Restor. Dent. 2021, 41, 99–104. [Google Scholar] [CrossRef] [PubMed]
- Adam, R.; Grender, J.; Timm, H.; Qaqish, J.; Goyal, C.R. Anti-gingivitis and Anti-plaque Efficacy of an Oral Hygiene System: Results from a 12-Week Randomized Controlled Trial. Compend. Contin. Educ. Dent. 2021, 42, e1–e4. [Google Scholar] [PubMed]
- Zini, A.; Mazor, S.; Timm, H.; Barker, M.L.; Grender, J.M.; Gerlach, R.W.; Biesbrock, A.R. Effects of an oral hygiene regimen on progression of gingivitis/early periodontitis: A randomized controlled trial. Can. J. Dent. Hyg. 2021, 55, 85–94. [Google Scholar]
- Ramseier, C.A.; Petitat, C.; Trepp, S.; Lang, N.P.; Eick, S.; Adam, R.; Ccahuana-Vasquez, R.A.; Barker, M.L.; Timm, H.; Klukowska, M.; et al. Clinical Parameters and Oral Fluid Biomarkers in Gingivitis Subjects using an Electric Toothbrush with Irrigator vs. a Manual Toothbrush Alone over 8 Weeks: A Randomised Controlled Clinical Trial. Oral Health Prev. Dent. 2021, 19, 137–147. [Google Scholar] [CrossRef]
- Thomassen, T.M.; Van der Weijden, F.G.; Slot, D.E. The efficacy of powered toothbrushes: A systematic review and network meta-analysis. Int. J. Dent. Hyg. 2022, 20, 3–17. [Google Scholar] [CrossRef]
- Ying, Y.; Nicolau, B. Oscillating-rotating electric toothbrushes may have a better effect on gingivitis and plaque control than sonic and manual toothbrushes in adults. J. Evid. Based Dent. Pract. 2021, 21, 101575. [Google Scholar] [CrossRef]
- Grender, J.; Adam, R.; Zou, Y. The effects of oscillating-rotating electric toothbrushes on plaque and gingival health: A meta-analysis. Am. J. Dent. 2020, 33, 3–11. [Google Scholar]
- Nathoo, S.; Mankodi, S.; Mateo, L.R.; Chaknis, P.; Panagakos, F. A clinical study comparing the supragingival plaque and gingivitis efficacy of a specially engineered sonic powered toothbrush with unique sensing and control technologies to a commercially available manual flat-trim toothbrush. J. Clin. Dent. 2012, 23, A11–A16. [Google Scholar]
- Farhadian, N.; Bidgoli, M.; Jafari, F.; Mahmoudzadeh, M.; Yaghobi, M.; Miresmaeili, A. Comparison of Electric Toothbrush, Persica and Chlorhexidine Mouthwashes on Reduction of Gingival Enlargement in Orthodontic Patients: A Randomised Clinical Trial. Oral Health Prev. Dent. 2015, 13, 301–307. [Google Scholar] [CrossRef]
- Clerehugh, V.; Williams, P.; Shaw, W.C.; Worthington, H.V.; Warren, P. A practice-based randomised controlled trial of the efficacy of an electric and a manual toothbrush on gingival health in patients with fixed orthodontic appliances. J. Dent. 1998, 26, 633–639. [Google Scholar] [CrossRef] [PubMed]
- Sivaramakrishnan, G.; Alsobaiei, M.; Sridharan, K. Powered toothbrushes for plaque control in fixed orthodontic patients: A network meta-analysis. Aust. Dent. J. 2021, 66, 20–31. [Google Scholar] [CrossRef] [PubMed]
- Preda, C.; Butera, A.; Pelle, S.; Pautasso, E.; Chiesa, A.; Esposito, F.; Oldoini, G.; Scribante, A.; Genovesi, A.M.; Cosola, S. The Efficacy of Powered Oscillating Heads vs. Powered Sonic Action Heads Toothbrushes to Maintain Periodontal and Peri-Implant Health: A Narrative Review. Int. J. Environ. Res. Public Health 2021, 18, 1468. [Google Scholar] [CrossRef]
- Nathoo, S.; Mateo, L.R.; Chaknism, P.; Kemp, J.H.; Gatzemeyer, J.; Morrison, B.M., Jr.; Panagakos, F. Efficacy of two different toothbrush heads on a sonic power toothbrush compared to a manual toothbrush on established gingivitis and plaque. J. Clin. Dent. 2014, 25, 65–70. [Google Scholar] [PubMed]
- Chicalé-Ferreira, A.B.; Palma-Dibb, R.G.; Faraoni, J.J.; Gatón-Hernández, P.; Silva, L.A.D.; Silva, R.A.D.; de Queiroz, A.M.; Lucisano, M.P.; Nelson-Filho, P. Effect of manual and electrical brushing on the enamel of sound primary teeth and teeth with induced white spot lesions. Am. J. Dent. 2020, 33, 25–28. [Google Scholar] [PubMed]
- Davidovich, E.; Grender, J.; Zini, A. Factors Associated with Dental Plaque, Gingivitis, and Caries in a Pediatric Population: A Records-Based Cross-Sectional Study. Int. J. Environ. Res. Public Health 2020, 17, 8595. [Google Scholar] [CrossRef]
- Nagy, P.; Kövér, K.; Gera, I.; Horváth, A. Elektromos és kézi fogkefék hatékonyságának összehasonlítása az orális prevencióban. Irodalmi áttekintés, systematic review, meta-analízis [Evaluation of the efficacy of powered and manual toothbrushes in preventing oral diseases (Systematic review with meta-analysis)]. Fogorv. Szle. 2016, 109, 3–22. [Google Scholar]
- Davidovich, E.; Shafir, S.; Shay, B.; Zini, A. Plaque Removal by a Powered Toothbrush Versus a Manual Toothbrush in Children: A Systematic Review and Meta-Analysis. Pediatr. Dent. 2020, 42, 280–287. [Google Scholar]
- Cugini, M.; Thompson, M.; Warren, P.R. Correlations between two plaque indices in assessment of toothbrush effectiveness. J. Contemp. Dent. Pract. 2006, 7, 1–9. [Google Scholar] [CrossRef]
- Agnihotry, A.; Fedorowicz, Z.; Worthington, H.V.; Manheimer, E.; Stevenson, R.G. Systematic reviews in oral health: A quality imperative. J. Evid. Based Med. 2016, 9, 47–52. [Google Scholar] [CrossRef]
- Rader, T.; Mann, M.; Stansfield, C.; Cooper, C.; Sampson, M. Methods for documenting systematic review searches: A discussion of common issues. Res. Synth. Methods 2014, 5, 98–115. [Google Scholar] [CrossRef] [PubMed]
- Ritsert, E.F.; Binns, W.H., Jr. Adolescents brush better with an electric toothbrush. J. Dent. Child. 1967, 34, 354–358. [Google Scholar]
- Owen, T.L. A clinical evaluation of electric and manual toothbrushing by children with primary dentitions. ASDC J. Dent. Child. 1972, 39, 15–21. [Google Scholar] [PubMed]
- Crawford, A.N.; McAllan, L.H.; Murray, J.J.; Brook, A.H. Oral hygiene instruction and motivation in children using manual and electric toothbrushes. Community Dent. Oral Epidemiol. 1975, 3, 257–261. [Google Scholar] [CrossRef] [PubMed]
- Yankell, S.L.; Emling, R.C. A thirty-day evaluation of the Rowenta Dentiphant powered toothbrush in children for safety and efficacy. J. Clin. Dent. 1996, 7, 96–100. [Google Scholar] [PubMed]
- Borutta, A. Plaque removal efficacy of a newly developed powered toothbrush in the primary dentition of pre-school children. J. Clin. Dent. 1997, 8, 151–155. [Google Scholar] [PubMed]
- Jongenelis, A.P.; Wiedemann, W. A comparison of plaque removal effectiveness of an electric versus a manual toothbrush in children. ASDC J. Dent. Child. 1997, 64, 176–182. [Google Scholar]
- Grossman, E.; Proskin, H. A comparison of the efficacy and safety of an electric and a manual children’s toothbrush. J. Am. Dent. Assoc. 1997, 128, 469–474. [Google Scholar] [CrossRef]
- Zimmer, S.; Didner, B.; Roulet, J.F. Clinical study on the plaque-removing ability of a new triple-headed toothbrush. J. Clin. Periodontol. 1999, 26, 281–285. [Google Scholar] [CrossRef]
- da Costa, C.C.; da Costa Filho, L.C.; Sória, M.L.; Mainardi, A.P. Plaque removal by manual and electric toothbrushing among children. Pesqui. Odontológica Bras. 2001, 15, 296–301. [Google Scholar] [CrossRef]
- García-Godoy, F.; Marcushamer, M.; Cugini, M.; Warren, P.R. The safety and efficacy of a children’s power toothbrush and a manual toothbrush in 6–11 year-olds. Am. J. Dent. 2001, 14, 195–199. [Google Scholar] [PubMed]
- Nourallah, A.W.; Splieth, C.H. Efficacy of occlusal plaque removal in erupting molars: A comparison of an electric toothbrush and the cross-toothbrushing technique. Caries Res. 2004, 38, 91–94. [Google Scholar] [CrossRef] [PubMed]
- Silverman, J.; Rosivack, R.G.; Matheson, P.B.; Houpt, M.I. Comparison of powered and manual toothbrushes for plaque removal by 4- to 5-year-old children. Pediatr. Dent. 2004, 26, 225–230. [Google Scholar]
- Mascarenhas, A.K.; Soparkar, P.; Al-Mutawaa, S.; Udani, T.M. Plaque removal using a battery-powered toothbrush compared to a manual toothbrush. J. Clin. Dent. 2005, 16, 23–25. [Google Scholar]
- Sun, D.F.; Wang, Y.J.; Hu, W.Q.; Qu, H.X.; Ni, X.K. The efficacy of dental plaque removed by using sonic electric toothbrush in children. Shanghai Kou Qiang Yi Xue 2006, 15, 28–30. (In Chinese) [Google Scholar] [PubMed]
- Kallar, S.; Pandit, I.K.; Srivastava, N.; Gugnani, N. Plaque removal efficacy of powered and manual toothbrushes under supervised and unsupervised conditions: A comparative clinical study. J. Indian Soc. Pedod. Prev. Dent. 2011, 29, 235–238. [Google Scholar] [CrossRef] [PubMed]
- Taschner, M.; Rumi, K.; Master, A.S.; Wei, J.; Strate, J.; Pelka, M. Comparing efficacy of plaque removal using professionally applied manual and power toothbrushes in 4- to 7-year-old children. Pediatr. Dent. 2012, 34, 61–65. [Google Scholar] [PubMed]
- Ghassemi, A.; Vorwerk, L.; Hooper, W.; Patel, V.; Sharma, N.; Qaqish, J. Comparative plaque removal efficacy of a new children’s powered toothbrush and a manual toothbrush. J. Clin. Dent. 2013, 24, 1–4. [Google Scholar]
- Mazzoleni, S.; Bonaldo, G.; Pontarolo, E.; Zuccon, A.; De Francesco, M.; Stellini, E. Experimental assessment of oral hygiene achieved by children wearing rapid palatal expanders, comparing manual and electric toothbrushes. Int. J. Dent. Hyg. 2014, 12, 187–192. [Google Scholar] [CrossRef]
- Davidovich, E.; Ccahuana-Vasquez, R.A.; Timm, H.; Grender, J.; Cunningham, P.; Zini, A. Randomised clinical study of plaque removal efficacy of a power toothbrush in a paediatric population. Int. J. Paediatr. Dent. 2017, 27, 558–567. [Google Scholar] [CrossRef] [Green Version]
- Zhao, S.M.; Chen, H.; Yu, P.B.; Wang, J. A clinical investigation of plaque control efficacy and safety of Sonicare toothbrush in children. Shanghai Kou Qiang Yi Xue 2018, 27, 313–317. (In Chinese) [Google Scholar] [PubMed]
- Erbe, C.; Klees, V.; Ferrari-Peron, P.; Ccahuana-Vasquez, R.A.; Timm, H.; Grender, J.; Cunningham, P.; Adam, R.; Farrell, S.; Wehrbein, H. A comparative assessment of plaque removal and toothbrushing compliance between a manual and an interactive power toothbrush among adolescents: A single-center, single-blind randomized controlled trial. BMC Oral Health 2018, 18, 130. [Google Scholar] [CrossRef] [PubMed]
- Chandra, S.; Jain, N.; Garg, R.; Dhawan, P.; Tuli, A.; Kumar, G. Ionic vs. Manual Toothbrushes: Effect on Plaque and Oral Hygiene Status in Children. Int. J. Clin. Pediatr. Dent. 2019, 12, 375–378. [Google Scholar] [CrossRef] [PubMed]
- Kerr, R.; Claman, D.; Amini, H.; Alexy, E.; Kumar, A.; Casamassimo, P.S. Evaluation of the Ability of Five- to 11-Year-Olds to Brush Their Teeth Effectively with Manual and Electric Toothbrushing. Pediatr. Dent. 2019, 41, 20–24. [Google Scholar] [PubMed]
- Aggarwal, N.; Gupta, S.; Grover, R.; Sadana, G.; Bansal, K. Plaque Removal Efficacy of Different Toothbrushes: A Comparative Study. Int. J. Clin. Pediatr. Dent. 2019, 12, 385–390. [Google Scholar] [CrossRef]
- Davidovich, E.; Ccahuana-Vasquez, R.A.; Timm, H.; Grender, J.; Zini, A. Randomised clinical study of plaque removal efficacy of an electric toothbrush in primary and mixed dentition. Int. J. Paediatr. Dent. 2021, 31, 657–663. [Google Scholar] [CrossRef]
- Purushotham, P.M.; Rao, A.; Natarajan, S.; Shrikrishna, S.B. Comparison of the efficacy of parental brushing using powered versus manual tooth brush: A randomized, four-period, two-treatment, single-blinded crossover study. J. Indian Soc. Pedod. Prev. Dent. 2021, 39, 95–100. [Google Scholar] [CrossRef]
- Francis, M.; Hooper, W.J.; Worob, D.; Huy, G.; Santos, S.; Goyal, C.R.; Qaqish, K.; Qaqish, J.G.; Ghassemi, A. Comparative plaque removal efficacy of a new children’s powered toothbrush and a manual toothbrush: Randomized, single use clinical study. Am. J. Dent. 2021, 34, 338–344. [Google Scholar]
- White, L.W. Efficacy of a sonic toothbrush in reducing plaque and gingivitis in adolescent patients. J. Clin. Orthod. 1996, 30, 85–90. [Google Scholar]
- Ho, H.P.; Niederman, R. Effectiveness of the Sonicare sonic toothbrush on reduction of plaque, gingivitis, probing pocket depth and subgingival bacteria in adolescent orthodontic patients. J. Clin. Dent. 1997, 8, 15–19. [Google Scholar]
- Heasman, P.; Wilson, Z.; Macgregor, I.; Kelly, P. Comparative study of electric and manual toothbrushes in patients with fixed orthodontic appliances. Am. J. Orthod. Dentofac. Orthop. 1998, 114, 45–49. [Google Scholar] [CrossRef] [PubMed]
- Pucher, J.J.; Lamendola-Sitenga, K.; Ferguson, D.; Van Swoll, R. The effectiveness of an ionic toothbrush in the removal of dental plaque and reduction on gingivitis in orthodontic patients. J. West. Soc. Periodontol. Periodontal Abstr. 1999, 47, 101–107. [Google Scholar] [PubMed]
- Borutta, A.; Pala, E.; Fischer, T. Effectiveness of a powered toothbrush compared with a manual toothbrush for orthodontic patients with fixed appliances. J. Clin. Dent. 2002, 13, 131–137. [Google Scholar] [PubMed]
- Hickman, J.; Millett, D.T.; Sander, L.; Brown, E.; Love, J. Powered vs. manual tooth brushing in fixed appliance patients: A short term randomized clinical trial. Angle Orthod. 2002, 72, 135–140. [Google Scholar] [CrossRef]
- Costa, M.R.; Silva, V.C.; Miqui, M.N.; Sakima, T.; Spolidorio, D.M.P.; Cirelli, J.A. Efficacy of ultrasonic, electric and manual toothbrushes in patients with fixed orthodontic appliances. Angle Orthod. 2007, 77, 361–366. [Google Scholar] [CrossRef] [PubMed]
- Biavati, A.S.; Gastaldo, L.; Dessi, M.; Biavati, F.S.; Migliorati, M. Manual orthodontic vs. oscillating-rotating electric toothbrush in orthodontic patients: A randomised clinical trial. Eur. J. Paediatr. Dent. 2010, 11, 200–202. [Google Scholar]
- Marini, I.; Bortolotti, F.; Parenti, S.I.; Gatto, M.R.; Bonetti, G.A. Combined effects of repeated oral hygiene motivation and type of toothbrush on orthodontic patients: A blind randomized clinical trial. Angle Orthod. 2014, 84, 896–901. [Google Scholar] [CrossRef] [PubMed]
- Zingler, S.; Pritsch, M.; Wrede, D.J.; Ludwig, B.; Bister, D.; Kneist, S.; Lux, C.J. A randomized clinical trial comparing the impact of different oral hygiene protocols and sealant applications on plaque, gingival, and caries index scores. Eur. J. Orthod. 2014, 36, 150–163. [Google Scholar] [CrossRef]
- Mylonopoulou, I.M.; Pepelassi, E.; Madianos, P.; Halazonetis, D.J. A randomized, 3-month, parallel-group clinical trial to compare the efficacy of electric 3-dimensional toothbrushes vs. manual toothbrushes in maintaining oral health in patients with fixed orthodontic appliances. Am. J. Orthod. Dentofac. Orthop. 2021, 160, 648–658. [Google Scholar] [CrossRef]
- Li, L.W.; Wong, H.M.; Sun, L.; Wen, Y.F.; McGrath, C.P. Anthropometric measurements and periodontal diseases in children and adolescents: A systematic review and meta-analysis. Adv. Nutr. 2015, 6, 828–841. [Google Scholar] [CrossRef] [PubMed]
- Li, L.W.; Wong, H.M.; Peng, S.M.; McGrath, C.P. Anthropometric measurements and dental caries in children: A systematic review of longitudinal studies. Adv. Nutr. 2015, 6, 52–63. [Google Scholar] [CrossRef] [PubMed]
- Boyd, R.L. Clinical and laboratory evaluation of powered electric toothbrushes: Review of the literature. J. Clin. Dent. 1997, 8, 67–71. [Google Scholar] [PubMed]
- Kaklamanos, E.G.; Kalfas, S. Meta-analysis on the effectiveness of powered toothbrushes for orthodontic patients. Am. J. Orthod. Dentofac. Orthop. 2008, 133, 187.e1–187.e14. [Google Scholar] [CrossRef]
- Bain, C.; Sayed, A.A.; Kaklamanos, E.G.; Kazi, H.A. Toothbrushing-Should We Advise Mechanical or Power Brushes? Results of an International Delphi Conference. J. Contemp. Dent. Pract. 2018, 19, 1169–1173. [Google Scholar] [CrossRef]
- Hollaar, V.R.Y. Effectiviteit van plaqueverwijdering met elektrische of handtandenborstel bij vaste orthodontische apparatuur Effectiveness of electric or manual toothbrush in dental plaque removal in patients with fixed orthodontic appliances. Ned. Tijdschr. Voor Tandheelkd. 2021, 128, 475–478. [Google Scholar] [CrossRef]
- Pabel, S.O.; Freitag, F.; Hrasky, V.; Zapf, A.; Wiegand, A. Randomised controlled trial on differential learning of toothbrushing in 6- to 9-year-old children. Clin. Oral Investig. 2018, 22, 2219–2228. [Google Scholar] [CrossRef]
- Collett, B.R.; Huebner, C.E.; Seminario, A.L.; Wallace, E.; Gray, K.E.; Speltz, M.L. Observed child and parent toothbrushing behaviors and child oral health. Int. J. Paediatr. Dent. 2016, 26, 184–192. [Google Scholar] [CrossRef] [PubMed]
- Joufi, A.I.; Claiborne, D.M.; Shuman, D. Oral Health Education and Promotion Activities by Early Head Start Programs in the United States: A systematic review. J. Dent. Hyg. 2021, 95, 14–21. [Google Scholar] [PubMed]
- Aksoy, M.; Topsakal, K.G. YouTube™ for information on paediatric oral health instructions. Int. J. Dent. Hyg. 2022, 20, 496–503. [Google Scholar] [CrossRef] [PubMed]
- Escribano, M.; Figuero, E.; Martin, C.; Tobias, A.; Serrano, J.; Roldan, S.; Herrera, D. Efficacy of adjunctive anti-plaque chemical agents: A systematic review and network meta-analyses of the Turesky modification of the Quigley and Hein plaque index. J. Clin. Periodontol. 2016, 43, 1059–1073. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
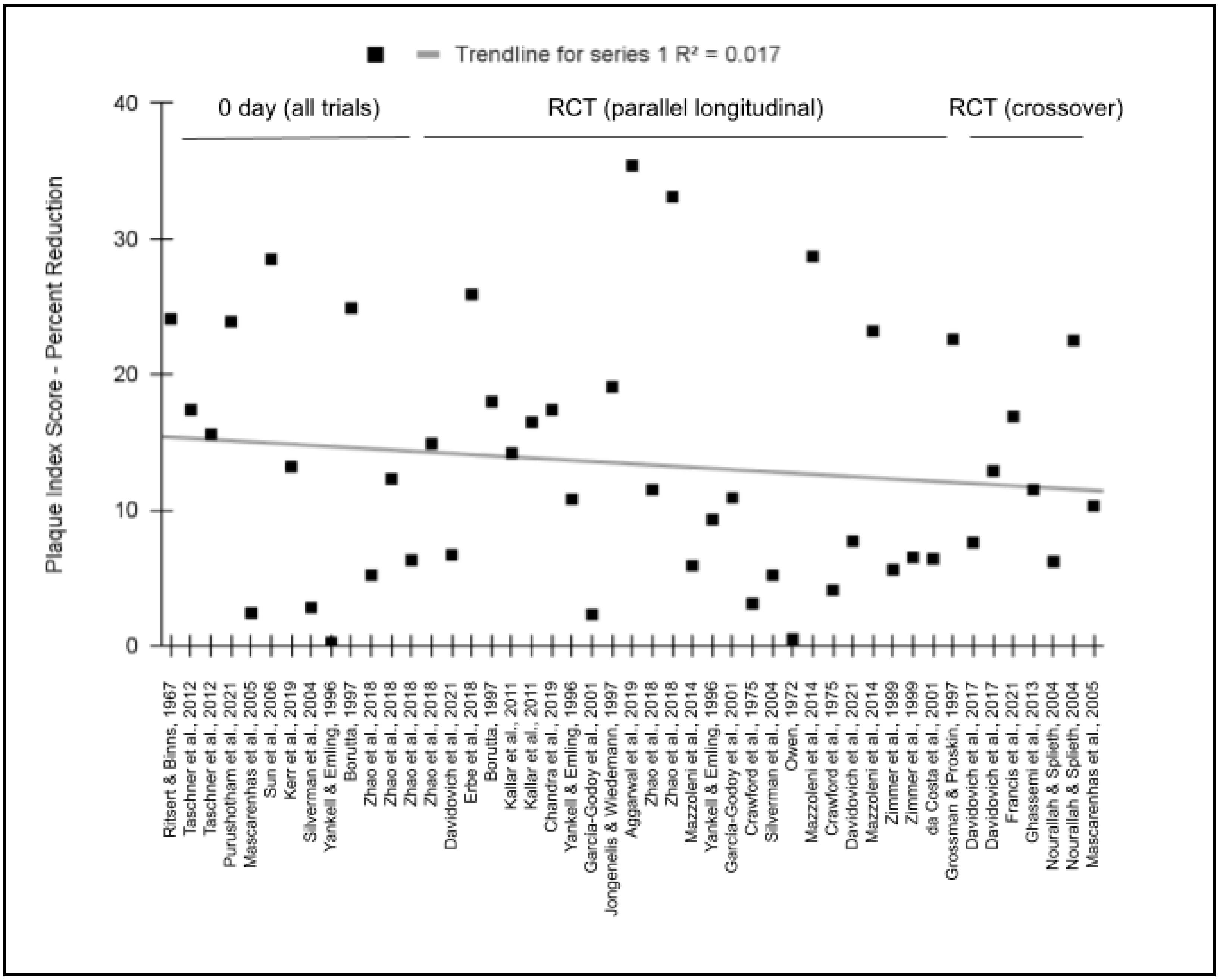
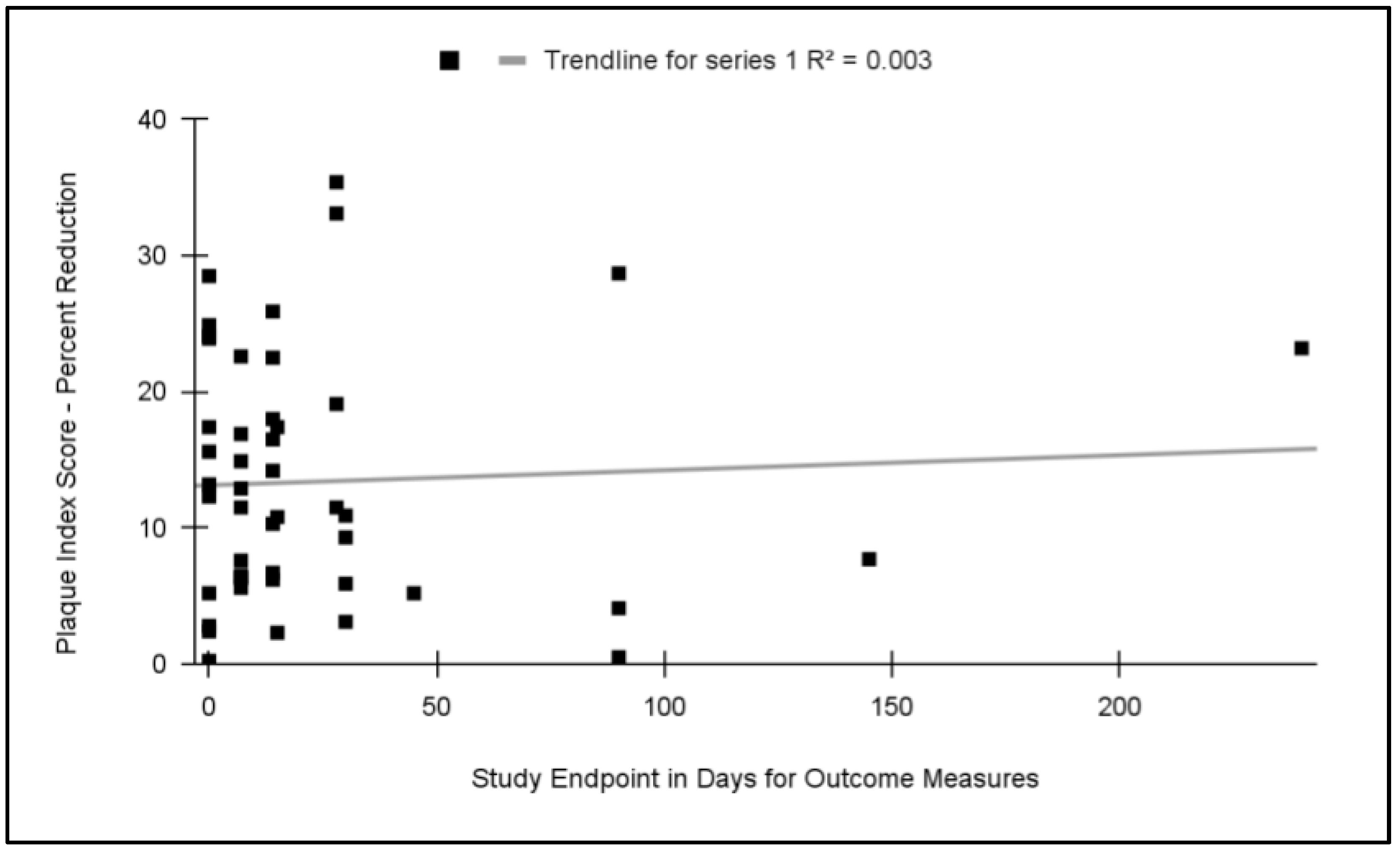
| Study | Study Design | Sample Size | Age Range (Median) | Study Endpoint(s) Follow-Up Period(s) | Plaque Index Score—Percent Reduction |
|---|---|---|---|---|---|
| Ritsert and Binns, 1967 [22] | Split-mouth parallel single day trial | n = 56 | 11–17 years (13.5 years) | 0 days | Silness and Loe (SLPI) (0 days) 24.1% |
| Owen, 1972 [23] | Randomized RCT parallel longitudinal trial | n = 40 | 2–6 years (4.3 years) | 90 days | Modified Ramfjord (MRPI) (90 days) 0.5% |
| Crawford et al., 1975 [24] | Randomized RCT parallel longitudinal trial | n = 123 | 9–15 years (12.1 years) | 30 days 90 days | Silness and Loe (SLPI) (30 days) 3.1% (90 days) 4.1% |
| Yankell and Emling, 1996 [25] | Randomized RCT parallel longitudinal trial | n = 65 | 6–8 years (7.0 years) | 0 days 15 days 30 days | Turesky Modified Quigley Hein Plaque Index (TQHPI) (0 days) 0.23% (15 days) 10.8% (30 days) 9.3% |
| Borutta, 1997 [26] | Randomized RCT parallel longitudinal trial | n = 73 | 4–6 years (5.1 years) | 0 days 14 days | Rustogi Modified Navy Plaque Index (RMNPI) (0 days) 24.9% (14 days) 18.0% |
| Jongenelis and Wiedemann, 1997 [27] | Randomized RCT parallel longitudinal trial | n = 24 | 5–10 years (7.8 years) | 28 days | Turesky Modified Quigley Hein Plaque Index (TQHPI) (28 days) 19.1% |
| Grossman and Proskin, 1997 [28] | Randomized Crossover longitudinal trial | n = 32 | 8–12 years (10.6 years) | 7 days | Global Plaque Index (GPI)(7 days) 22.6% |
| Zimmer et al., 1999 [29] | Randomized Crossover longitudinal trial | n = 12 | 6–12 years (9 years) | 7 days | Turesky Modified Quigley Hein Plaque Index (TQHPI) Primary (7 days) 5.6% Mixed (7 days) 6.5% |
| da Costa et al., 2001 [30] | Randomized Crossover longitudinal trial | n = 15 | 4–5 years (4.5 years) | 7 days | Silness and Loe (SLPI) (7 days) 6.4% |
| García-Godoy et al., 2001 [31] | Randomized RCT parallel longitudinal trial | n = 70 | 6–11 years (8.5 years) | 15 days 30 days | Turesky Modified Quigley Hein Plaque Index (TQHPI) (15 days) 2.3% (30 days) 10.9% |
| Nourallah and Splieth, 2004 [32] | Randomized Crossover longitudinal trial | n = 16 | 5–7 years (6 years) | 14 days | Occlusal Plaque Index (OPI) (14 days) 6.2% Approximal Plaque Index (API) (14 days) 22.5% |
| Silverman et al., 2004 [33] | Randomized RCT parallel longitudinal trial | n = 20 | 4–5 years (4.5 years) | 0 days 45 days | Turesky Modified Quigley Hein Plaque Index (TQHPI) (0 days) 2.75% (45 days) 5.2% |
| Mascarenhas et al., 2005 [34] | Randomized Crossover longitudinal trial | n = 30 | 9–11 years (10 years) | 0 days 14 days | Turesky Modified Quigley Hein Plaque Index (TQHPI) (0 days) 2.4% (14 days) 10.3% |
| Sun et al., 2006 [35] | Randomized RCT parallel single day trial | n = 50 | 6–7 years (6.5 years) | 0 days | Turesky Modified Quigley Hein Plaque Index (TQHPI) (0 days) 28.5% |
| Kallar et al., 2011 [36] | Randomized RCT parallel longitudinal trial | n = 200 | 6–13 years (9.75 years) | 14 days | Turesky Modified Quigley Hein Plaque Index (TQHPI) Supervised (14 days) 16.5% Unsupervised (14 days) 14.2% |
| Taschner et al., 2012 [37] | Split-mouth parallel single day trial | n = 68 | 4–7 years (5.3 years) | 0 days | Turesky Modified Quigley Hein Plaque Index (TQHPI) (0 days; low speed) 15.6% (0 days; high speed) 17.4% |
| Ghassemi et al., 2013 [38] | Randomized Crossover longitudinal trial | n = 105 | 8–17 years (12.5 years) | 7 days | Rustogi Modified Navy Plaque Index (RMNPI) (7 days) 11.5% |
| Mazzoleni et al., 2014 [39] | Randomized RCT parallel longitudinal trial | n = 40 | 7–12 years (9.5 years) | 30 days 90 days 240 days | Silness and Loe (SLPI) (30 days) 5.9% (90 days) 28.7% (240 days) 23.2% |
| Davidovich et al., 2017 [40] | Randomized Crossover longitudinal trial | n = 41 | 8–11 years (9 years) | 7 days | Turesky Modified Quigley Hein Plaque Index (TQHPI) (7 days; Mixed dentition) 12.9% (7 days; Permanent dentition) 7.6% |
| Zhao et al., 2018 [41] | Randomized RCT parallel longitudinal trial | n = 90 n = 90 | 3–6 years (4.5 years) 6–9 years (7.5 years) | 0 days 7 days 28 days | Rustogi Modified Navy Plaque Index (RMNPI) 3–6 years (0 days) 5.2% (7 days) 14.9% (28 days) 33.1% 6–9 years (0 days) 12.3% (7 days) 6.3% (28 days) 11.5% |
| Erbe et al., 2018 [42] | Randomized RCT parallel longitudinal trial | n = 60 | 13–17 years (15.3 years) | 14 days | Turesky Modified Quigley Hein Plaque Index (TQHPI) (14 days) 25.9% |
| Chandra et al., 2019 [43] | Randomized RCT parallel longitudinal trial | n = 30 | 6–12 years (9 years) | 15 days | Turesky Modified Quigley Hein Plaque Index (TQHPI) (15 days) 17.4% |
| Kerr et al., 2019 [44] | Randomized RCT parallel single day trial | n = 120 | 5–11 years (8 years) | 0 days | Simplified Oral Health Index (SOHI) (0 days) 13.2% |
| Aggarwal et al., 2019 [45] | Randomized RCT parallel longitudinal trial | n = 40 | 9–16 years (12.5 years) | 28 days | Turesky Modified Quigley Hein Plaque Index (TQHPI) (28 days) 35.4% |
| Davidovich et al., 2021 [46] | Randomized RCT parallel longitudinal trial | n = 20 n = 21 | 3–6 years (4.5 years) 7–9 years (8 years) | 7–14 days | Turesky Modified Quigley Hein Plaque Index (TQHPI) (14 days; 3–6 years) 6.7% (14 days; 7–9 years) 7.7% |
| Purushotham et al., 2021 [47] | RCT parallel single day trial | n = 20 | 3–5 years (4 years) | 0 days | Turesky Modified Quigley Hein Plaque Index (TQHPI) (0 days) 23.9% |
| Francis et al., 2021 [48] | Randomized Crossover longitudinal trial | n = 55 | 5–8 years (6.8 years) | 7 days | Rustogi Modified Navy Plaque Index (RMNPI) (7 days) 16.9% |
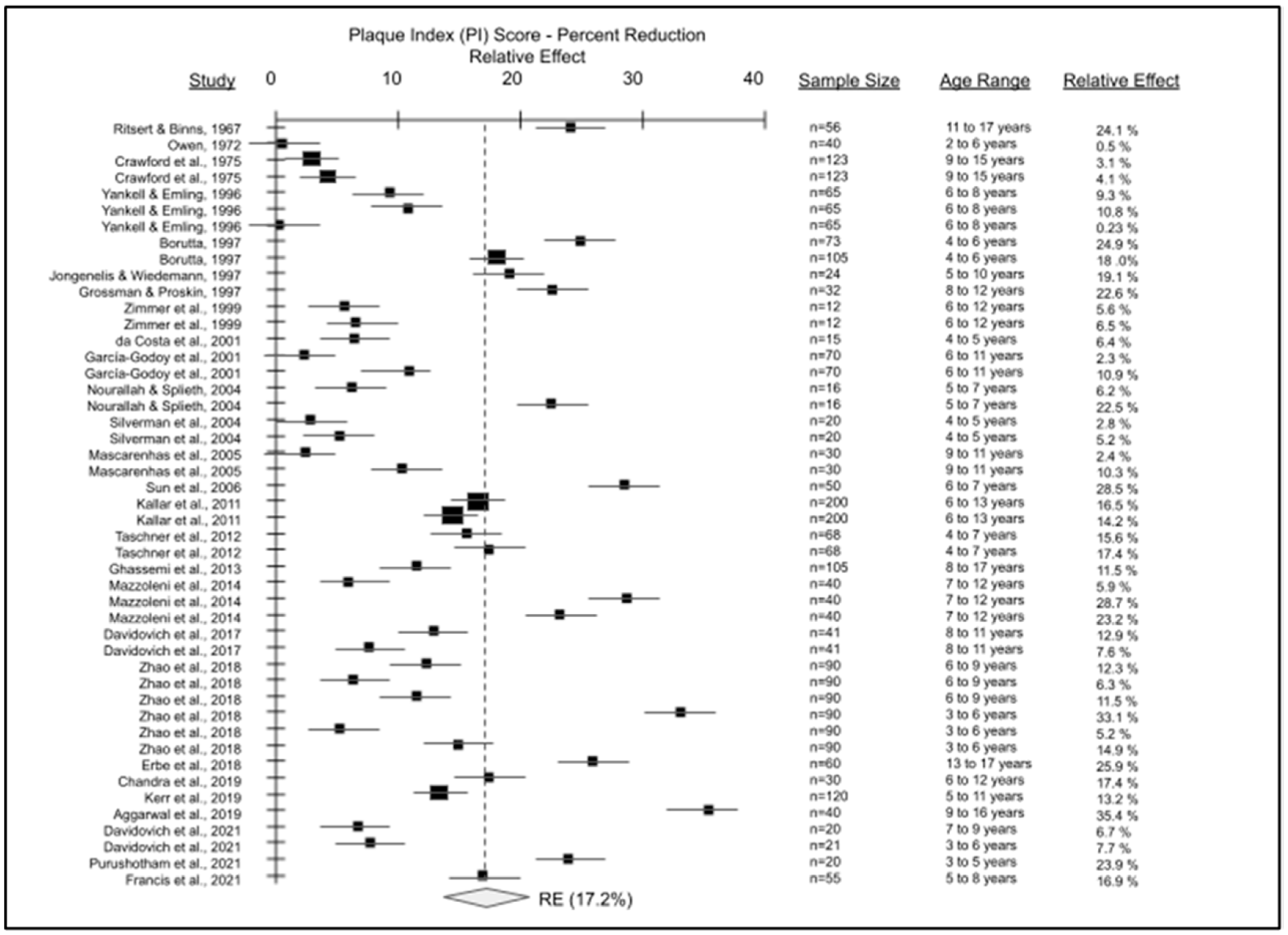
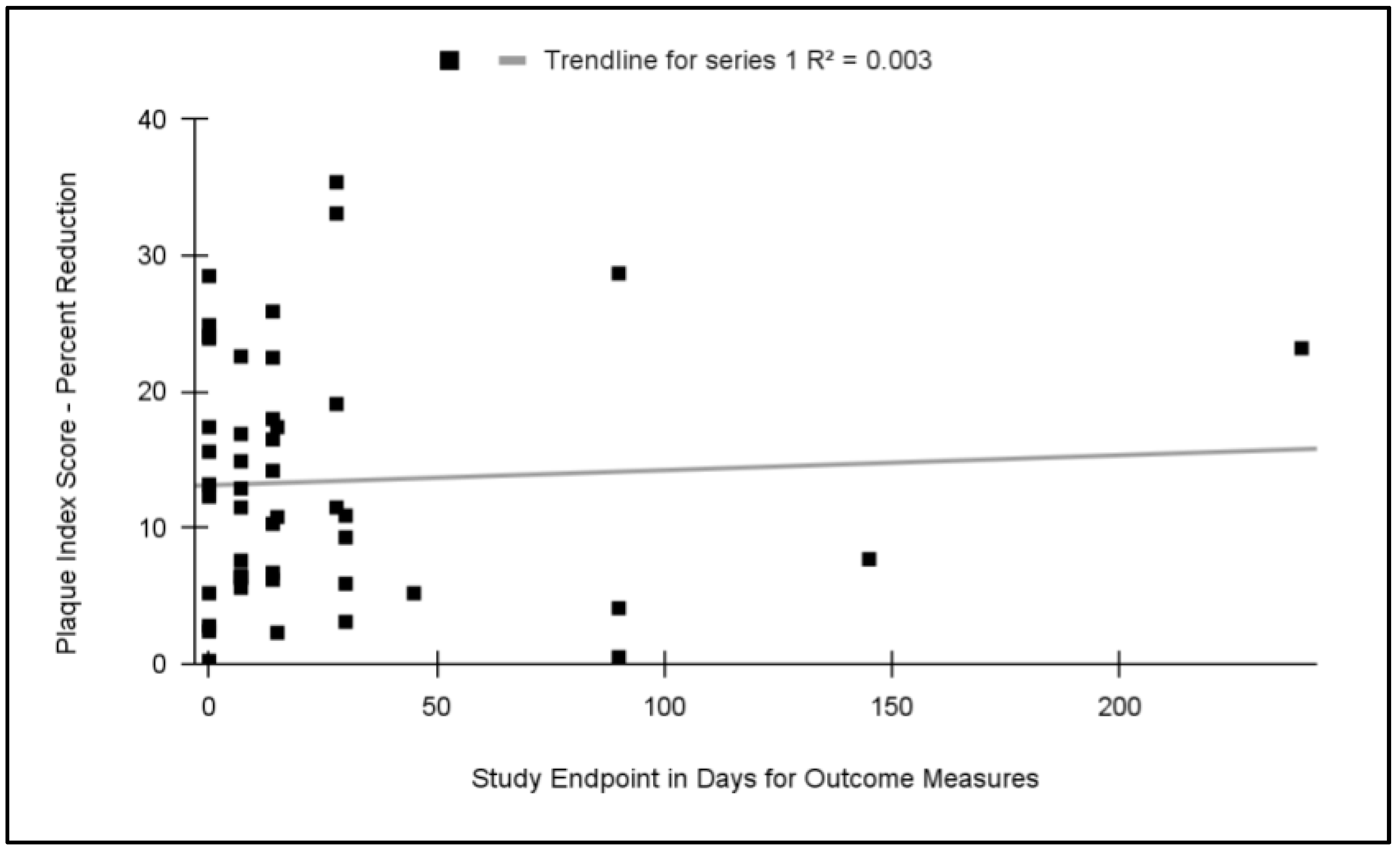
| Total number of pediatric non-orthodontic studies n = 27 (1967–2021) | Total: 1626 Average: 60.2 Range: 12–200 | Average: 7.9 years Range: 2–17 years | Average: 25.2 days Range: 0–240 days | Average PI reduction: 17.2% |
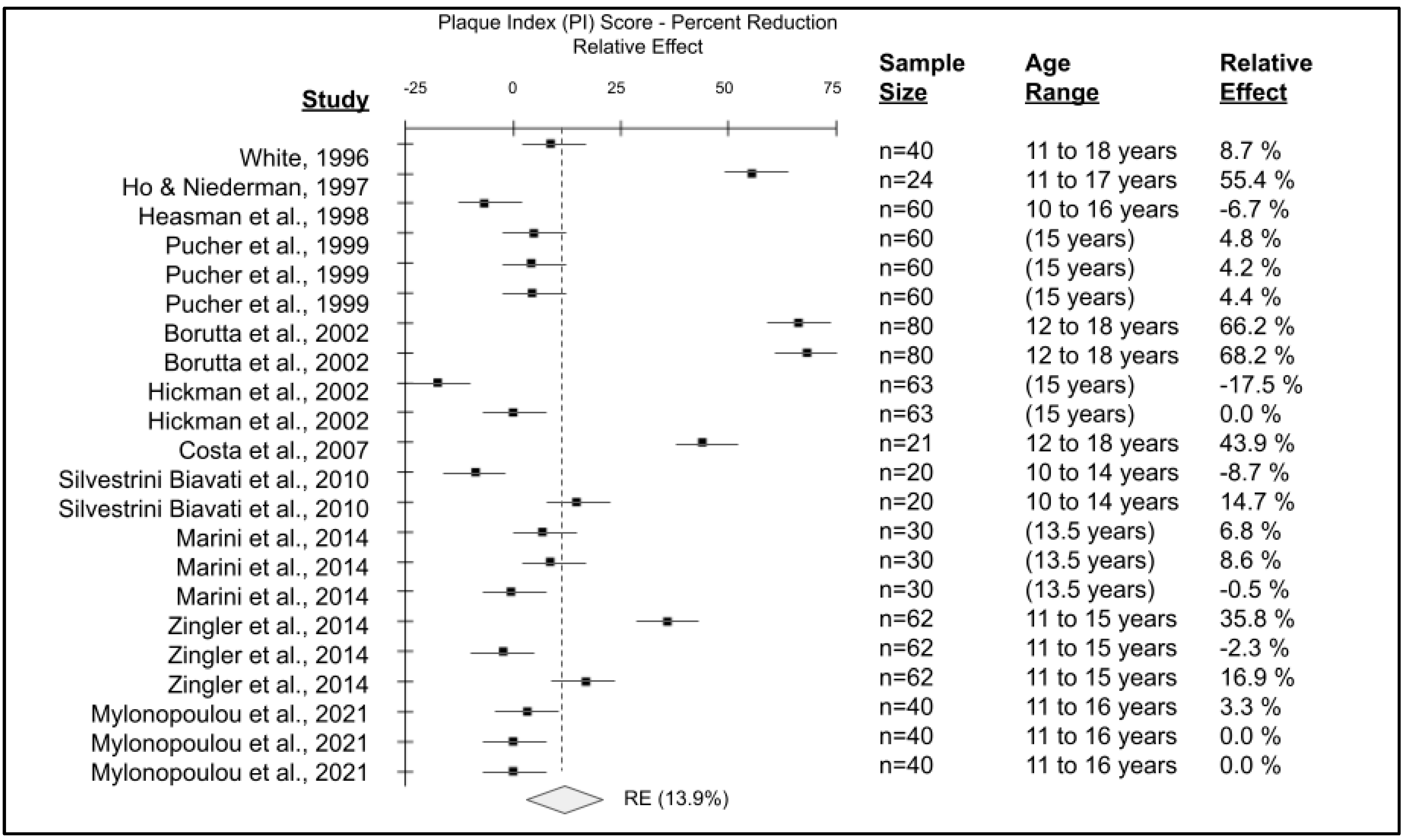
| Study | Study Design | Sample Size | Age Range (Median) | Study Endpoint(s) Follow-up Period(s) | Plaque Index Score—Percent Reduction |
|---|---|---|---|---|---|
| White, 1996 [49] | Randomized RCT parallel longitudinal trial | n = 40 | 11–18 years (14.5) | 84 days | Hygiene Analysis Index (HAI) 8.7% |
| Ho and Niederman, 1997 [50] | Randomized RCT parallel longitudinal trial | n = 24 | 11–17 years (14 years) | 28 days | Silness and Loe (SLPI) 55.4% |
| Heasman et al., 1998 [51] | Randomized Crossover longitudinal trial | n = 60 | 10–16 years (13.6 years) | 28 days | Visual Plaque Index (VPI) −6.7% |
| Pucher et al., 1999 [52] | Randomized RCT parallel longitudinal trial | n = 60 | (15 years) | 0 days 15 days 42 days | Turesky Modified Quigley Hein Plaque Index (TQHPI) (0 days) 4.8% (15 days) 4.2% (42 days) 4.4% |
| Borutta et al., 2002 [53] | Randomized RCT parallel longitudinal trial | n = 80 | 12–18 years (13.5 years) | 14 days 28 days | Turesky Modified Quigley Hein Plaque Index (TQHPI) (14 days) 66.2% (28 days) 68.2% |
| Hickman et al., 2002 [54] | Randomized RCT parallel longitudinal trial | n = 63 | (15 years) | 28 days 56 days | Silness & Loe (SLPI) (28 days) −17.5% (28 days) 0.0% |
| Costa et al., 2007 [55] | Randomized RCT parallel longitudinal trial | n = 21 | 12–18 years (15.2 years) | 30 days | Silness and Loe (SLPI) 43.9% |
| Silvestrini Biavati et al., 2010 [56] | Randomized RCT parallel longitudinal trial | n = 20 | 10–14 years (11.4 years) | 14 days 28 days | O’Leary Plaque Index (OLPI) −8.7% 14.7% |
| Marini et al., 2014 [57] | Randomized RCT parallel longitudinal trial | n = 30 | (13.5 years) | 28 days 56 days 84 days | Turesky Modified Quigley Hein Plaque Index (TQHPI) (28 days) 6.8% (56 days) 8.6% (84 days) −0.5% |
| Zingler et al., 2014 [58] | Randomized RCT parallel longitudinal trial | n = 62 | 11–15 years (13.1 years) | 28 days 56 days 84 days | Turesky Modified Quigley Hein Plaque Index (TQHPI) (28 days) 35.8% (56 days) 2.3% (84 days) 16.9% |
| Mylonopoulou et al., 2021 [59] | Randomized RCT parallel longitudinal trial | n = 40 | 11–16 years (14 years) | 30 days 60 days 90 days | Silness & Loe (SLPI) (30 days) 3.3% (60 days) 0.0% (90 days) 0.0% |
| Total number of orthodontic pediatric studies, n = 11 (1996–2021) | Total: 500 Average: 45.5 Range: 20–80 | Average: 13.9 years Range: 10–17 years | Average: 61 days Range: 0–84 days | Average PI reduction: 13.9% |
| Study Authors | Selection Bias | Attrition Bias | Reporting (Observer) Bias |
|---|---|---|---|
| Ritsert and Binns, 1967 [22] | High (Randomized from Convenience sample) | Very low (Attrition 0%) | Unknown (Not reported) |
| Owen, 1972 [23] | High (Randomized from Convenience sample) | Very low (Attrition 5.0%) | Unknown (Not reported) |
| Crawford et al., 1975 [24] | Low (RCT) | Very low (Attrition 2.2%) | Low (Two independent operators) |
| Yankell and Emling, 1996 [25] | High (Randomized from Convenience sample) | Very low (Attrition 1.6%) | Low (Multiple operators) |
| Borutta, 1997 [26] | Low (RCT) | Low (Attrition 13.3%) | Low (Two independent operators) |
| Jongenelis and Wiedemann, 1997 [27] | High (Randomized from Convenience sample) | Very low (Attrition 1.6%) | Low (Multiple operators) |
| Grossman and Proskin, 1997 [28] | Low (RCT) | Very low (Attrition 0.0%) | Moderate (One blinded operator) |
| Zimmer et al., 1999 [29] | High (Randomized from Convenience sample) | Very low (Attrition 0.0%) | Moderate (One blinded operator) |
| da Costa et al., 2001 [30] | High (Randomized from Convenience sample) | Very low (Attrition 0.0%) | Moderate (One blinded operator) |
| García-Godoy et al., 2001 [31] | Low (RCT) | Very low (Attrition 5.3%) | Low (Multiple operators) |
| Nourallah and Splieth, 2004 [32] | High (Randomized from Convenience sample) | Very low (Attrition 0.0%) | Low (Multiple operators) |
| Silverman et al., 2004 [33] | High (Randomized from Convenience sample) | Very low (Attrition 3.4%) | Low (Multiple operators) |
| Mascarenhas et al., 2005 [34] | High (Randomized from Convenience sample) | Very low (Attrition 0.0%) | Moderate (One blinded operator) |
| Sun et al., 2006 [35] | High (Randomized from Convenience sample) | Very low (Attrition 0.0%) | Low (Multiple operators) |
| Kallar et al., 2011 [36] | Unknown | Very low (Attrition 0.0%) | Unknown (Not reported) |
| Taschner et al., 2012 [37] | Low (RCT) | Very low (Attrition 1.4%) | Moderate (One blinded operator) |
| Ghassemi et al., 2013 [38] | Low (RCT) | Very low (Attrition 1.9%) | Moderate (One blinded operator) |
| Mazzoleni et al., 2014 [39] | High (Randomized from Convenience sample) | Very low (Attrition 0.0%) | Moderate (One blinded operator) |
| Davidovich et al., 2017 [40] | Low (RCT) | Very low (Attrition 0.0%) | Low (Multiple operators) |
| Zhao et al., 2018 [41] | Unknown | Very low (Attrition 4.4%) | Unknown (Not reported) |
| Erbe et al., 2018 [42] | Low (RCT) | Very low (Attrition 1.7%) | Moderate (One blinded operator) |
| Chandra et al., 2019 [43] | Low (RCT) | Very low (Attrition 0.0%) | Unknown (Not reported) |
| Kerr et al., 2019 [44] | High (Randomized from Convenience sample) | Very low (Attrition 0.0%) | Low (Multiple operators) |
| Aggarwal et al., 2019 [45] | Low (RCT) | Very low (Attrition 0.0%) | Moderate (One blinded operator) |
| Davidovich et al., 2021 [46] | Low (RCT) | Low (Attrition 4.8%) | Moderate (One blinded operator) |
| Purushotham et al., 2021 [47] | Low (RCT) | Low (Attrition 5%) | Low (Multiple operators) |
| Francis et al., 2021 [48] | Low (RCT) | Very low (Attrition 0.0%) | Moderate (One blinded operator) |
| White, 1996 [49] | Low (RCT) | High (Attrition 20%) | Moderate (One blinded operator) |
| Ho and Niederman, 1997 [50] | Low (RCT) | Very low (Attrition 0.0%) | Moderate (One blinded operator) |
| Heasman et al., 1998 [51] | Low (RCT) | Very low (Attrition 0.0%) | Low (Multiple operators) |
| Pucher et al., 1999 [52] | Low (RCT) | Moderate (Attrition 13%) | Moderate (One blinded operator) |
| Borutta et al., 2002 [53] | Low (RCT) | Low (Attrition 5%) | Moderate (One blinded operator) |
| Hickman et al., 2002 [54] | Low (RCT) | Low (Attrition 5%) | Moderate (One blinded operator) |
| Costa et al., 2007 [55] | Low (RCT) | Very low (Attrition 0.0%) | Moderate (One blinded operator) |
| Silvestrini Biavati et al., 2010 [56] | Low (RCT) | Very low (Attrition 0.0%) | Low (Multiple operators) |
| Marini et al., 2014 [57] | Low (RCT) | Very low (Attrition 0.0%) | Moderate (One blinded operator) |
| Zingler et al., 2014 [58] | Low (RCT) | Low (Attrition 8%) | Moderate (One blinded operator) |
| Mylonopoulou et al., 2021 [59] | Low (RCT) | Very low (Attrition 0.0%) | Moderate (One blinded operator) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Graves, A.; Grahl, T.; Keiserman, M.; Kingsley, K. Systematic Review and Meta Analysis of the Relative Effect on Plaque Index among Pediatric Patients Using Powered (Electric) versus Manual Toothbrushes. Dent. J. 2023, 11, 46. https://doi.org/10.3390/dj11020046
Graves A, Grahl T, Keiserman M, Kingsley K. Systematic Review and Meta Analysis of the Relative Effect on Plaque Index among Pediatric Patients Using Powered (Electric) versus Manual Toothbrushes. Dentistry Journal. 2023; 11(2):46. https://doi.org/10.3390/dj11020046
Chicago/Turabian StyleGraves, Andrew, Troy Grahl, Mark Keiserman, and Karl Kingsley. 2023. "Systematic Review and Meta Analysis of the Relative Effect on Plaque Index among Pediatric Patients Using Powered (Electric) versus Manual Toothbrushes" Dentistry Journal 11, no. 2: 46. https://doi.org/10.3390/dj11020046