


Surgical Treatment in Patients with Toxic Phosphorus Osteonecrosis of Facial Skull Middle Zone

 , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
- aged from 18 years (due to the age of admitted patients);
- history data—an intake of phosphoric narcotics such as desomorphine and pervitin for more than a year;
- medical history—written approval from narcologist at the place of residence—drug use remission for at least 3 months prior to the planned hospital admission;
- the presence of bone tissue disruption according to the patient’s complaints for more than 2 months.
- lack of compliance;
- constant narcotics abuse and inability/unwillingness to stop using them;
- comorbidity in the decompensation stage or its exacerbation;
- drug addiction relapse;
- voluntary refusal from treatment;
- history of bisphosphonates/denosumab.
- Type 1: patients with local pathological process in maxilla (1 or 2 teeth/dental sockets are included)—15 patients (30%) (Figure 1a,b);
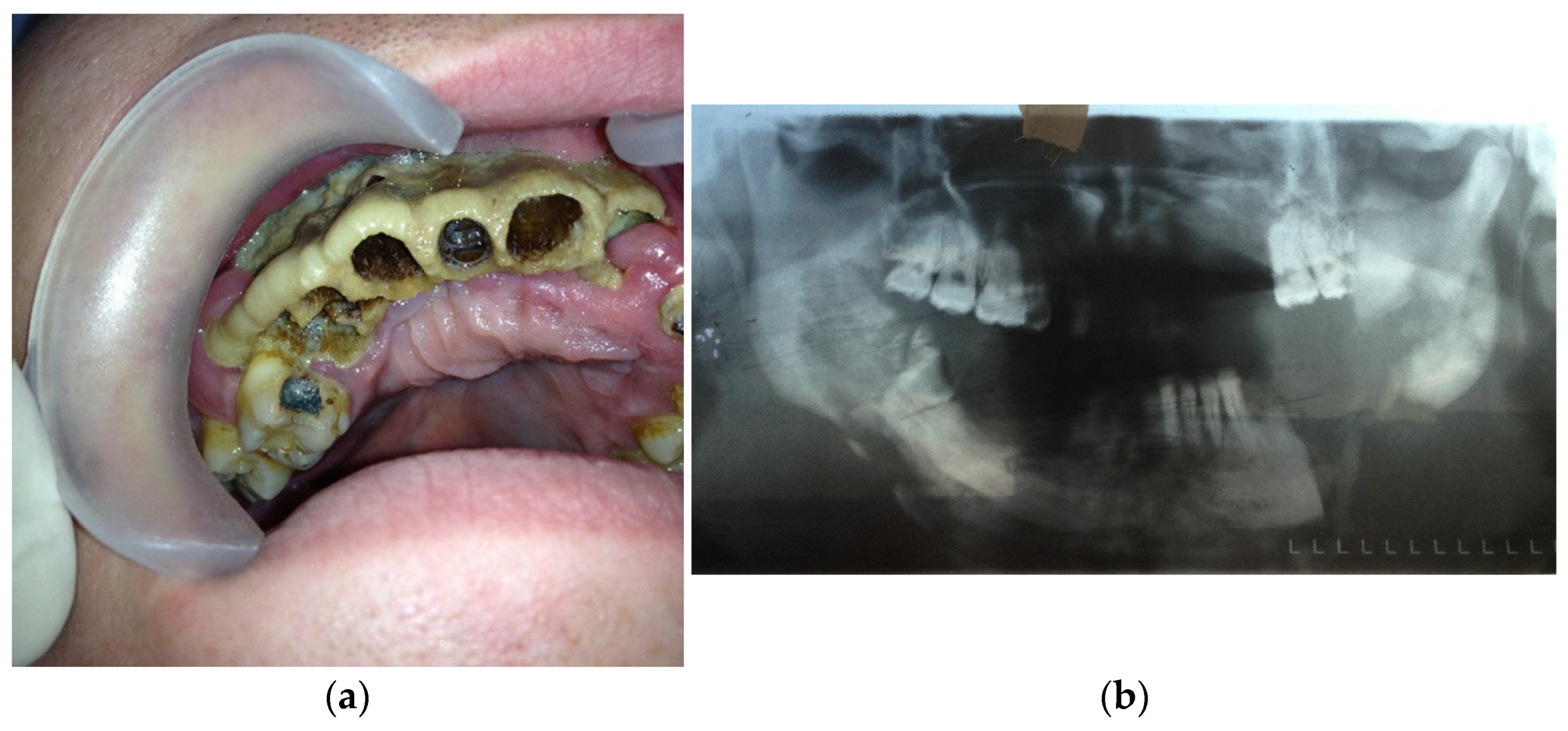
- Type 2: patients with maxilla involved (at least three teeth are included)—14 patients (28%) (Figure 2a,b);Figure 2. (a) Patient with type 2 toxic phosphorus osteonecrosis. Intraoral view; (b) patient OPG.
![Dentistry 11 00108 g002]()

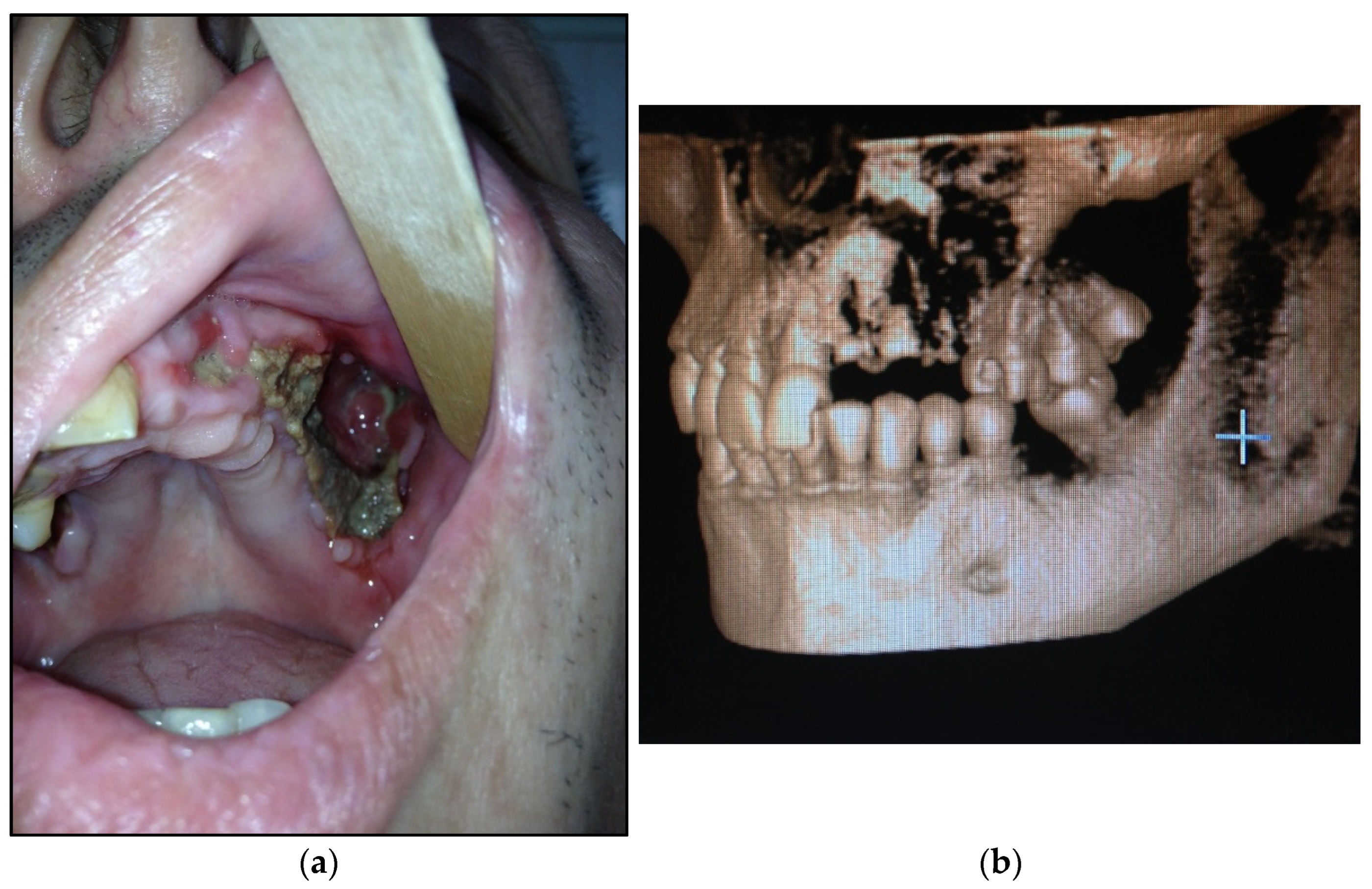
- Type 3: patients with maxilla and partially zygomatic bone (its body) involved—11 patients (22%) (Figure 3a–c);Figure 3. (a) Patient with type 3 toxic phosphorus osteonecrosis. Intraoral view; (b) extraoral view, (c) multi CT-scan of patient’s skull before operation.Figure 3. (a) Patient with type 3 toxic phosphorus osteonecrosis. Intraoral view; (b) extraoral view, (c) multi CT-scan of patient’s skull before operation.
![Dentistry 11 00108 g003]()

- Type 4: patients with maxilla, zygomatic bone, floor of the orbit involved—10 patients (20%) (Figure 4a,b)Figure 4. (a) Patient with type 4 toxic phosphorus osteonecrosis. Intraoral view; (b) multi CT-scan of patient’s skull before operation.Figure 4. (a) Patient with type 4 toxic phosphorus osteonecrosis. Intraoral view; (b) multi CT-scan of patient’s skull before operation.
![Dentistry 11 00108 g004]()

3. Results
3.1. The Results of the Radiological Investigation
3.2. Surgical Approaches in Patients with Maxillofacial Osteonecrosis
3.3. Early Postoperative Period (before 14 Days after Surgery)
3.4. Late Postoperative Period (1 Month–2 Years after Surgery)
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
References
- Alves, E.A. DARK Classics in Chemical Neuroscience: Krokodil. ACS Chem. Neurosci. 2020, 11, 3968–3978. [Google Scholar] [CrossRef] [PubMed]
- Mella-Raipán, J.; Romero-Parra, J.; Recabarren-Gajardo, G. DARK Classics in Chemical Neuroscience: Heroin and Desomorphine. ACS Chem. Neurosci. 2020, 11, 3905–3927. [Google Scholar] [CrossRef]
- Poghosyan, Y.M.; Hakobyan, K.A.; Poghosyan, A.Y.; Avetisyan, E.K. Surgical treatment of jaw osteonecrosis in “Krokodil” drug addicted patients. J. Cranio Maxillofac. Surg. 2014, 42, 1639–1643. [Google Scholar] [CrossRef] [PubMed]
- Grund, J.-P.C.; Latypov, A.; Harris, M. Breaking worse: The emergence of krokodil and excessive injuries among people who inject drugs in Eurasia. Int. J. Drug Policy 2013, 24, 265–274. [Google Scholar] [CrossRef]
- Poghosyan, Y.; Hakobyan, K. Krokodil drug-related osteonecrosis of skull base: A case report. Neurochirurgie 2022, 68, 466–468. [Google Scholar] [CrossRef] [PubMed]
- Nicolatou-Galitis, O.; Schiødt, M.; Mendes, R.A.; Ripamonti, C.; Hope, S.; Drudge-Coates, L.; Niepel, D.; Van den Wyngaert, T. Medication-related osteonecrosis of the jaw: Definition and best practice for prevention, diagnosis, and treatment. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. 2019, 127, 117–135. [Google Scholar] [CrossRef]
- Hughes, D.E.; Wright, K.R.; Uy, H.L.; Sasaki, A.; Yoneda, T.; Roodman, D.G.; Mundy, G.R.; Boyce, B.F. Bisphosphonates promote apoptosis in murine osteoclasts in vitro and in vivo. J. Bone Miner. Res. 2009, 10, 1478–1487. [Google Scholar] [CrossRef]
- Ruggiero, S.L.; Mehrotra, B.; Rosenberg, T.J.; Engroff, S.L. Osteonecrosis of the jaws associated with the use of bisphosphonates: A review of 63 cases. J. Oral Maxillofac. Surg. 2004, 62, 527–534. [Google Scholar] [CrossRef]
- Wan, J.T.; Sheeley, D.M.; Somerman, M.J.; Lee, J.S. Mitigating osteonecrosis of the jaw (ONJ) through preventive dental care and understanding of risk factors. Bone Res. 2020, 8, 14. [Google Scholar] [CrossRef]
- Khan, A.A.; Morrison, A.; Hanley, D.A.; Felsenberg, D.; McCauley, L.K.; O’Ryan, F.; Reid, I.R.; Ruggiero, S.L.; Taguchi, A.; Tetradis, S.; et al. Diagnosis and Management of Osteonecrosis of the Jaw: A Systematic Review and International Consensus. J. Bone Miner. Res. 2015, 30, 3–23. [Google Scholar] [CrossRef]
- Adornato, M.C.; Morcos, I.; Rozanski, J. The treatment of bisphosphonate-associated osteonecrosis of the jaws with bone resection and autologous platelet-derived growth factors. J. Am. Dent. Assoc. 2007, 138, 971–977. [Google Scholar] [CrossRef] [PubMed]
- Basin, E.M.; Medvedev, Y.A. Toxic phosphorus osteonecrosis of facial bones among drug addicts to desomorphine and pervitin. Part I. Stomatologiya 2015, 94, 53–57. [Google Scholar] [CrossRef]
- Bowen, K.P.; Barusch, N.M.; Lara, D.L.; Trinidad, B.J.; Caplan, J.P.; McKnight, C.A. Don׳t Feed the “Krokodil”: Desomorphine Fear Outpaces Reality. Psychosomatics 2015, 56, 312–313. [Google Scholar] [CrossRef]
- Alves, E.A.; Grund, J.-P.C.; Afonso, C.M.; Netto, A.D.P.; Carvalho, F.; Dinis-Oliveira, R.J. The harmful chemistry behind krokodil (desomorphine) synthesis and mechanisms of toxicity. Forensic Sci. Int. 2015, 249, 207–213. [Google Scholar] [CrossRef]
- Nelson, M.E.; Bryant, S.M.; Aks, S.E. Emerging drugs of abuse. Dis. Mon. 2014, 60, 110–132. [Google Scholar] [CrossRef] [PubMed]
- Booth, R.E. ‘Krokodil’ and other home-produced drugs for injection: A perspective from Ukraine. Int. J. Drug Policy 2013, 24, 277–278. [Google Scholar] [CrossRef] [PubMed]
- Gahr, M.; Freudenmann, R.; Hiemke, C.; Gunst, I.M.; Connemann, B.; Schönfeldt-Lecuona, C. Desomorphine Goes “Crocodile”. J. Addict. Dis. 2012, 31, 407–412. [Google Scholar] [CrossRef]
- Idashkina, N.; Horoshko, A.; Rasinska, T. Oral rehabilitation in patients with maxillary osteonecrosis: A case report. Rom. J. Oral Rehabil. 2020, 2020, 12. [Google Scholar]
- Rustemeyer, J.; Melenberg, A.; Junker, K.; Sari-Rieger, A. Osteonecrosis of the maxilla related to long-standing methamphetamine abuse: A possible new aspect in the etiology of osteonecrosis of the jaw. Oral Maxillofac. Surg. 2014, 18, 237–241. [Google Scholar] [CrossRef]
- Pabst, A.; Castillo-Duque, J.C.; Mayer, A.; Klinghuber, M.; Werkmeister, R. Meth Mouth—A Growing Epidemic in Dentistry? Dent. J. 2017, 5, 29. [Google Scholar] [CrossRef]
- Oliver, T.; Gheevarghese, S.J.; Gandhi, U.; Bhat, Z.Y.; Pillai, U. “Krokodil”—A Menace Slowly Spreading Across the Atlantic. Am. J. Ther. 2015, 22, 231–233. [Google Scholar] [CrossRef]
- Thekkemuriyi, D.V.; John, S.G.; Pillai, U. ‘Krokodil’—A Designer Drug from Across the Atlantic, with Serious Consequences. Am. J. Med. 2014, 127, e1–e2. [Google Scholar] [CrossRef] [PubMed]
- Hakobyan, K.A.; Poghosyan, Y.M.; Poghosyan, A.Y. C-terminal telopeptide level in “Krokodil” drug-related jaw osteonecrosis patients. New Armen Med. J. 2017, 11, 57–61. [Google Scholar]
- Williamson, A.; Hoggart, B. Pain: A review of three commonly used pain rating scales. J. Clin. Nurs. 2005, 14, 798–804. [Google Scholar] [CrossRef] [PubMed]
- Marx, R.E.; Sawatari, Y.; Fortin, M.; Broumand, V. Bisphosphonate-Induced Exposed Bone (Osteonecrosis/Osteopetrosis) of the Jaws: Risk Factors, Recognition, Prevention, and Treatment. J. Oral Maxillofac. Surg. 2005, 63, 1567–1575. [Google Scholar] [CrossRef]
- E Coleman, R. Risks and benefits of bisphosphonates. Br. J. Cancer 2008, 98, 1736–1740. [Google Scholar] [CrossRef] [PubMed]
- Florez, D.H.; Moreira, A.M.D.S.; da Silva, P.R.; Brandão, R.; Borges, M.M.C.; de Santana, F.J.M.; Borges, K.B. Desomorphine (Krokodil): An overview of its chemistry, pharmacology, metabolism, toxicology and analysis. Drug Alcohol Depend. 2017, 173, 59–68. [Google Scholar] [CrossRef]
- Hakobyan, K.; Poghosyan, Y. “Krokodil” drug—Related osteonecrosis of midface: A case series. J. Cranio Maxillofac. Surg. 2019, 47, 1918–1921. [Google Scholar] [CrossRef]
- Sergent, J.-F.; Bader, G.; Hamon, J.; Peigne, L.; Lejeune, S. Krokodil (Desomorphine)-induced osteonecrosis of the maxilla: A case report and literature review. J. Oral Med. Oral Surg. 2019, 25, 26. [Google Scholar] [CrossRef]
- Eisele, D.W.; Smith, R.V. Complications in Head and Neck Surgery, 2nd ed.; Mosby: Philadelphia, PA, USA, 2009; p. 792. [Google Scholar]
- Hakobyan, K.; Poghosyan, Y.; Kasyan, A. The use of buccal fat pad in surgical treatment of ‘Krokodil’ drug-related osteonecrosis of maxilla. J. Cranio Maxillofac. Surg. 2018, 46, 831–836. [Google Scholar] [CrossRef]
- Hakobyan, K.A.; Poghosyan, Y.M. Spontaneous closure of bilateral oro-antral communication formed after maxillary partial resection in “Krokodil” drug related jaw osteonecrosis patient: Case report. New Armen Med. J. 2017, 11, 78–80. [Google Scholar]
- Hakobyan, K.; Poghosyan, Y. Spontaneous bone formation after mandible segmental resection in “krokodil” drug-related jaw osteonecrosis patient: Case report. Oral Maxillofac. Surg. 2017, 21, 267–270. [Google Scholar] [CrossRef] [PubMed]
- Medvedev, Y.A.; Basin, E.M.; Serova, N.S.; Korshunova, A.V.; Babkova, A.A.; Kureshova, D.N. Total jaw osteonecrosis among drug addicts. Russ. J. Dent. 2016, 20, 183–189. [Google Scholar] [CrossRef]
- Malanchuk, V.A.; Brodeckij, I.S. Kompleksnoe lechenie bol’nyh osteomielitom cheljustej na fone narkoticheskoj zavisimosti. Vestn. VGMU 2014, 13, 115–123. [Google Scholar]



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| NRS Score | Type 1 (n = 15) | Type 2 (n = 14) | Type 3 (n = 11) | Type 4 (n = 10) | p |
|---|---|---|---|---|---|
| No pain | 5 (33.3%) | 4 (28.6%) | 2 (18.2%) | 0 | <0.05 |
| Mild pain | 2 (13.3%) | 2 (14.3%) | 1 (9.1%) | 0 | <0.05 |
| Moderate pain | 2 (13.3%) | 3 (21.4%) | 2 (18.2%) | 0 | <0.05 |
| Intense pain | 3 (20%) | 2 (14.3%) | 2 (18.2%) | 1 (10%) | >0.05 |
| Very intense pain | 2 (13.3%) | 2 (14.3%) | 2 (18.2%) | 1 (10%) | >0.05 |
| Unsufferable pain | 1 (6.8%) | 1 (7.1%) | 2 (18.2%) | 8 (80%) | >0.05 |
| Symptom | Groups | p | |||
|---|---|---|---|---|---|
| 1 | 2 | 3 | 4 | ||
| Demarcation line in maxilla | 15 (100%) | 14 (100%) | 11 (100%) | 10 (100%) | * |
| Demarcation line in the zygomatic bone | 0 (0%) | 4 (28.6%) | 11 (100%) | 10 (100%) | * |
| Demarcation line in the floor of the orbit | 0 (0%) | 0 (0%) | 0 (0%) | 10 (100%) | * |
| Presence of sequestrum | 6 (40%) | 4 (28.6%) | 5 (45.5%) | 8 (80%) | <0.05 |
| Cortical plate sclerosis | 15 (100%) | 14 (100%) | 11 (100%) | 10 (100%) | * |
| Periosteal reaction | 15 (100%) | 14 (100%) | 11 (100%) | 10 (100%) | * |
| NRS Score | Type 1 (n = 15) | Type 2 (n = 14) | Type 3 (n = 11) | Type 4 (n = 10) | p |
|---|---|---|---|---|---|
| No pain | 5 (33.3%) | 4 (28.6%) | 2 (18.2%) | 0 | * |
| Mild pain | 2 (13.3%) | 2 (14.3%) | 1 (9.1%) | 0 | * |
| Moderate pain | 2 (13.3%) | 3 (21.4%) | 2 (18.2%) | 0 | * |
| Intense pain | 3 (20%) | 2 (14.3%) | 2 (18.2%) | 1 (10%) | <0.05 |
| Very intense pain | 2 (13.3%) | 2 (14.3%) | 2 (18.2%) | 1 (10%) | <0.05 |
| Unsufferable pain | 1 (6.8%) | 1 (7.1%) | 2 (18.2%) | 8 (80%) | <0.05 |
| NRS Score | Type 1 (n = 15) | Type 2 (n = 14) | Type 3 (n = 11) | Type 4 (n = 10) | p |
|---|---|---|---|---|---|
| No pain | 10 (66.7%) | 7 (28.6%) | 5 (45.4%) | 1 (10%) | <0.05 |
| Mild pain | 3 (20%) | 3 (21.4%) | 3 (27.3%) | 3 (30%) | <0.05 |
| Moderate pain | 2 (13.3%) | 3 (21.4%) | 1 (9.1%) | 5 (50%) | <0.05 |
| Intense pain | 0 (0%) | 1 (7.1%) | 2 (18.2%) | 1 (10%) | * |
| Very intense pain | 0 (0%) | 0 (0%) | 0 (0%) | 0 (0%) | * |
| Unsufferable pain | 0 (0%) | 0 (0%) | 0 (0%) | 0 (0%) | * |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ispiryan, D.H.; Hakobyan, G.; Li, A.; Diachkova, E.Y.; Vasil’ev, Y.; Kheygetyan, A.; Ivanova, E.; Zhandarov, K.; Kireeva, N.; Safronov, R.; et al. Surgical Treatment in Patients with Toxic Phosphorus Osteonecrosis of Facial Skull Middle Zone. Dent. J. 2023, 11, 108. https://doi.org/10.3390/dj11050108
Ispiryan DH, Hakobyan G, Li A, Diachkova EY, Vasil’ev Y, Kheygetyan A, Ivanova E, Zhandarov K, Kireeva N, Safronov R, et al. Surgical Treatment in Patients with Toxic Phosphorus Osteonecrosis of Facial Skull Middle Zone. Dentistry Journal. 2023; 11(5):108. https://doi.org/10.3390/dj11050108
Chicago/Turabian StyleIspiryan, Davit H., Gagik Hakobyan, Anastasia Li, Ekaterina Yu. Diachkova, Yuriy Vasil’ev, Artur Kheygetyan, Elena Ivanova, Kirill Zhandarov, Natalia Kireeva, Roman Safronov, and et al. 2023. "Surgical Treatment in Patients with Toxic Phosphorus Osteonecrosis of Facial Skull Middle Zone" Dentistry Journal 11, no. 5: 108. https://doi.org/10.3390/dj11050108
APA StyleIspiryan, D. H., Hakobyan, G., Li, A., Diachkova, E. Y., Vasil’ev, Y., Kheygetyan, A., Ivanova, E., Zhandarov, K., Kireeva, N., Safronov, R., Serikov, A., & Medvedev, Y. A. (2023). Surgical Treatment in Patients with Toxic Phosphorus Osteonecrosis of Facial Skull Middle Zone. Dentistry Journal, 11(5), 108. https://doi.org/10.3390/dj11050108