

Retrospective Clinical Evaluation of RMGIC/GIC Class V Restorations

Abstract
:1. Introduction
2. Materials and Methods
Data Collection
3. Results
4. Discussion
5. Conclusions
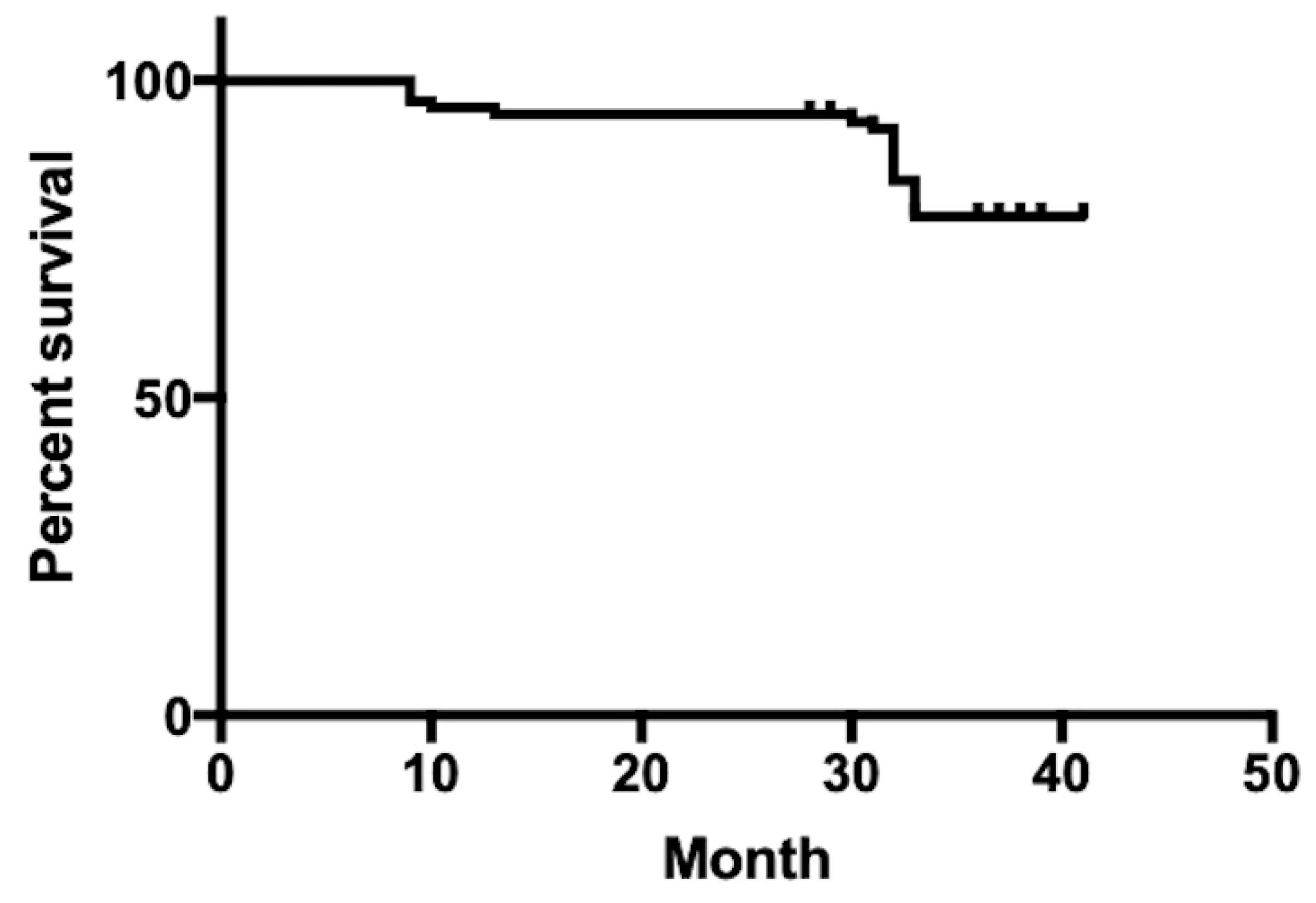
- The overall success rate of Class V restorations in this study was 72.9% for restorations ranging from 2.5 to 3.5 years old.
- RMGIC (Fuji II LC) restorations exhibited higher retention rates and better color match compared to GIC (Fuji IX) restorations.
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Peumans, M.; Kanumilli, P.; De Munck, J.; Van Landuyt, K.; Lambrechts, P.; Van Meerbeek, B. Clinical effectiveness of contemporary adhesives: A systematic review of current clinical trials. Dent. Mater. 2005, 21, 864–881. [Google Scholar] [CrossRef]
- Santos, M.J.; Ari, N.; Steele, S.; Costella, J.; Banting, D. Retention of tooth-colored restorations in non-carious cervical lesions—A systematic review. Clin. Oral Investig. 2014, 18, 1369–1381. [Google Scholar] [CrossRef] [PubMed]
- Wilson, A.D.; Kent, B.E. A new translucent cement for dentistry. The glass ionomer cement. Br. Dent. J. 1972, 132, 133–135. [Google Scholar] [CrossRef] [PubMed]
- Xie, D.; Brantley, W.A.; Culbertson, B.M.; Wang, G. Mechanical properties and microstructures of glass-ionomer cements. Dent. Mater. 2000, 16, 129–138. [Google Scholar] [CrossRef] [PubMed]
- Wilson, A.D. Developments in glass-ionomer cements. Int. J. Prosthodont. 1989, 2, 438–446. [Google Scholar]
- Ching, H.S.; Luddin, N.; Kannan, T.P.; Ab Rahman, I.; Abdul Ghani, N.R.N. Modification of glass ionomer cements on their physical-mechanical and antimicrobial properties. J. Esthet. Restor. Dent. 2018, 30, 557–571. [Google Scholar] [CrossRef]
- Ruengrungsom, C.; Burrow, M.F.; Parashos, P.; Palamara, J.E.A. Comprehensive characterisation of flexural mechanical properties and a new classification for porosity of 11 contemporary ion-leaching dental restorative materials. J. Mech. Behav. Biomed. Mater. 2021, 121, 104615. [Google Scholar] [CrossRef]
- Mustafa, H.A.; Soares, A.P.; Paris, S.; Elhennawy, K.; Zaslansky, P. The forgotten merits of GIC restorations: A systematic review. Clin. Oral Investig. 2020, 24, 2189–2201. [Google Scholar] [CrossRef]
- Fricker, J.P. Therapeutic properties of glass-ionomer cements: Their application to orthodontic treatment. Aust. Dent. J. 2022, 67, 12–20. [Google Scholar] [CrossRef]
- Dezanetti, J.M.P.; Nascimento, B.L.; Orsi, J.S.R.; Souza, E.M. Effectiveness of glass ionomer cements in the restorative treatment of radiation-related caries—A systematic review. Support. Care Cancer 2022, 30, 8667–8678. [Google Scholar] [CrossRef]
- Burke, F.M.; Ray, N.J.; McConnell, R.J. Fluoride-containing restorative materials. Int. Dent. J. 2006, 56, 33–43. [Google Scholar] [CrossRef]
- Cury, J.A.; de Oliveira, B.H.; dos Santos, A.P.; Tenuta, L.M. Are fluoride releasing dental materials clinically effective on caries control? Dent. Mater. 2016, 32, 323–333. [Google Scholar] [CrossRef]
- Yoshihara, K.; Nagaoka, N.; Maruo, Y.; Sano, H.; Yoshida, Y.; Van Meerbeek, B. Bacterial adhesion not inhibited by ion-releasing bioactive glass filler. Dent. Mater. 2017, 33, 723–734. [Google Scholar] [CrossRef]
- Hara, A.T.; Turssi, C.P.; Ando, M.; González-Cabezas, C.; Zero, D.T.; Rodrigues, A.L., Jr.; Serra, M.C.; Cury, J.Á. Influence of fluoride-releasing restorative material on root dentine secondary caries in situ. Caries Res. 2006, 40, 435–439. [Google Scholar] [CrossRef] [PubMed]
- Albelasy, E.H.; Hamama, H.H.; Chew, H.P.; Montaser, M.; Mahmoud, S.H. Secondary caries and marginal adaptation of ion-releasing versus resin composite restorations: A systematic review and meta-analysis of randomized clinical trials. Sci. Rep. 2022, 12, 19244. [Google Scholar] [CrossRef] [PubMed]
- Tanumiharja, M.; Burrow, M.F.; Tyas, M.J. Microtensile bond strengths of glass ionomer (polyalkenoate) cements to dentine using four conditioners. J. Dent. 2000, 28, 361–366. [Google Scholar] [CrossRef]
- Inoue, S.; Van Meerbeek, B.; Abe, Y.; Yoshida, Y.; Lambrechts, P.; Vanherle, G.; Sano, H. Effect of remaining dentin thickness and the use of conditioner on micro-tensile bond strength of a glass-ionomer adhesive. Dent. Mater. 2001, 17, 445–455. [Google Scholar] [CrossRef]
- Cvar, J.F.; Ryge, G. Reprint of criteria for the clinical evaluation of dental restorative materials 1971. Clin. Oral Investig 2005, 9, 215–232. [Google Scholar] [PubMed]
- van Dijken, J.W. A 6-year clinical evaluation of class I poly-acid modified resin composite/resin composite laminate restorations cured with a two-step curing technique. Dent. Mater. 2003, 19, 423–428. [Google Scholar] [CrossRef] [PubMed]
- Folwaczny, M.; Loher, C.; Mehl, A.; Kunzelmann, K.H.; Hinkel, R. Tooth-colored filling materials for the restoration of cervical lesions: A 24-month follow-up study. Oper. Dent. 2000, 25, 251–258. [Google Scholar]
- Stewardson, D.; Creanor, S.; Thornley, P.; Bigg, T.; Bromage, C.; Browne, A.; Cottam, D.; Dalby, D.; Gilmour, J.; Horton, J.; et al. The survival of Class V restorations in general dental practice: Part 3, five-year survival. Br. Dent. J. 2012, 212, E14. [Google Scholar] [CrossRef] [PubMed]
- Hayes, M.; Brady, P.; Burke, F.M.; Finbarr, P. Failures rates of Class V restorations in the management of root caries in adults—A systematic review. Gerodontology 2016, 33, 299–307. [Google Scholar] [CrossRef] [PubMed]
- Rai, N.; Naik, R.; Gupta, R.; Shetty, S.; Singh, A. Evaluating the Effect of Different Conditioning Agents on the Shear Bond Strength of Resin-Modified Glass Ionomers. Contemp. Clin. Dent. 2017, 8, 604–612. [Google Scholar] [CrossRef] [PubMed]
- Pereira, L.C.; Nunes, M.C.; Dibb, R.G.; Powers, J.M.; Roulet, J.F.; Navarro, M.F. Mechanical properties and bond strength of glass-ionomer cements. J. Adhes. Dent. Spring 2002, 4, 73–80. [Google Scholar]
- Moberg, M.; Brewster, J.; Nicholson, J.W.; Roberts, H. Physical property investigation of contemporary glass ionomer and resin-modified glass ionomer restorative materials. Clin. Oral Investig. 2019, 23, 1295–1308. [Google Scholar] [CrossRef]
- Rêgo, H.M.C.; Butler, S.; Santos, M.J.C. Evaluation of the Mechanical Properties of Three Resin-Modified Glass-Ionomer Materials. BioMed Res. Int. 2022, 2022, 4690656. [Google Scholar] [CrossRef]
- van Dijken, J.W.; Pallesen, U. Long-term dentin retention of etch-and-rinse and self-etch adhesives and a resin-modified glass ionomer cement in non-carious cervical lesions. Dent. Mater. 2008, 24, 915–922. [Google Scholar] [CrossRef]
- Stewardson, D.A.; Thornley, P.; Bigg, T.; Bromage, C.; Browne, A.; Cottam, D.; Dalby, D.; Gilmour, J.; Horton, J.; Roberts, E.; et al. The survival of Class V restorations in general dental practice. Part 2, early failure. Br. Dent. J. 2011, 210, E19. [Google Scholar] [CrossRef]
- BarHajizadeh, H.; Ghavamnasiri, M.; Namazikhah, M.S.; Majidinia, S.; Bagheri, M. Effect of different conditioning protocols on the adhesion of a glass ionomer cement to dentin. J. Contemp. Dent. Pract. 2009, 10, 9–16. [Google Scholar]
- Sidhu, S.K. Glass-ionomer cement restorative materials: A sticky subject? Aust. Dent. J. 2011, 56 (Suppl. S1), 23–30. [Google Scholar] [CrossRef]
- Imbery, T.A.; Namboodiri, A.; Duncan, A.; Amos, R.; Best, A.M.; Moon, P.C. Evaluating dentin surface treatments for resin-modified glass ionomer restorative materials. Oper. Dent. 2013, 38, 429–438. [Google Scholar] [CrossRef] [PubMed]
- van Dijken, J.W. Four-year evaluation of the effect of 10% polyacrylic acid or water rinsing pretreatment on retention of glass polyalkenoate cement. Eur. J. Oral Sci. 1996, 104, 64–66. [Google Scholar] [CrossRef] [PubMed]
- Tyas, M.J. The effect of dentine conditioning with polyacrylic acid on the clinical performance of glass ionomer cement—3-year results. Aust. Dent. J. 1994, 39, 220–221. [Google Scholar] [CrossRef]
- Boing, T.F.; de Geus, J.L.; Wambier, L.M.; Loguercio, A.D.; Reis, A.; Gomes, O.M.M. Are Glass-Ionomer Cement Restorations in Cervical Lesions More Long-Lasting than Resin-based Composite Resins? A Systematic Review and Meta-Analysis. J. Adhes. Dent. 2018, 20, 435–452. [Google Scholar]
- Gladys, S.; Van Meerbeek, B.; Lambrechts, P.; Vanherle, G. Marginal adaptation and retention of a glass-ionomer, resin-modified glass-ionomers and a polyacid-modified resin composite in cervical Class-V lesions. Dent. Mater. 1998, 14, 294–306. [Google Scholar] [CrossRef] [PubMed]
- Folwaczny, M.; Loher, C.; Mehl, A.; Kunzelmann, K.H.; Hickel, R. Class V lesions restored with four different tooth-colored materials—3-year results. Clin. Oral Investig. 2001, 5, 31–39. [Google Scholar] [CrossRef]
- Rodrigues, D.S.; Buciumeanu, M.; Martinelli, A.E.; Nascimento, R.M.; Henriques, B.; Silva, F.S.; Souza, J.C.M. Mechanical Strength and Wear of Dental Glass-Ionomer and Resin Composites Affected by Porosity and Chemical Composition. J. Bio Tribocorros 2015, 1, 24. [Google Scholar] [CrossRef]
- Krämer, N.; Schmidt, M.; Lücker, S.; Domann, E.; Frankenberger, R. Glass ionomer cement inhibits secondary caries in an in vitro biofilm model. Clin. Oral Investig. 2018, 22, 1019–1031. [Google Scholar] [CrossRef]
- Heintze, S.D.; Loguercio, A.D.; Hanzen, T.A.; Reis, A.; Rousson, V. Clinical efficacy of resin-based direct posterior restorations and glass-ionomer restorations—An updated meta-analysis of clinical outcome parameters. Dent. Mater. 2022, 38, e109–e135. [Google Scholar] [CrossRef]
- Forss, H.; Widstrom, E. Reasons for restorative therapy and longevity of restorations in adults. Acta Odontol. Scand. 2004, 62, 82–86. [Google Scholar] [CrossRef]
- Manhart, J.; Garcia-Godoy, F.; Hickel, R. Direct posterior restorations: Clinical results and new developments. Dent. Clin. N. Am. 2002, 46, 303–339. [Google Scholar] [CrossRef] [PubMed]
- Abdalla, A.I.; Alhadainy, H.A.; García-Godoy, F. Clinical evaluation of glass ionomers and compomers in Class V carious lesions. Am. J. Dent. 1997, 10, 18–20. [Google Scholar] [PubMed]
- Garshasb, M.; Santos, G.C., Jr.; Rizkalla, A.S.; Bohay, R.; Santos, M.J. Effect of Finishing Procedures on the Surface Roughness of Resin-modified Glass-Ionomer Materials. Compend. Contin. Educ. Dent. 2017, 38, e1–e4. [Google Scholar]
- Mahn, E.; Rousson, V.; Heintze, S. Meta-Analysis of the Influence of Bonding Parameters on the Clinical Outcome of Tooth-colored Cervical Restorations. J. Adhes. Dent. 2015, 17, 391–403. [Google Scholar]
- Sulaiman, T.A.; Abdulmajeed, A.A.; Altitinchi, A.; Ahmed, S.N.; Donovan, T.E. Effect of resin-modified glass ionomer cement dispensing/mixing methods on mechanical properties. Oper. Dent. 2018, 43, E158–E165. [Google Scholar] [CrossRef]
- Oliveira, G.L.; Carvalho, C.N.; Carvalho, E.M.; Bauer, J.; Leal, A.M.A. The Influence of Mixing Methods on the Compressive Strength and Fluoride Release of Conventional and Resin-Modified Glass Ionomer Cements. Int. J. Dent. 2019, 2019, 6834931. [Google Scholar] [CrossRef] [PubMed]
- Al-Taee, L.; Deb, S.; Banerjee, A. An in vitro assessment of the physical properties of manually- mixed and encapsulated glass-ionomer cements. BDJ Open 2020, 6, 12. [Google Scholar] [CrossRef] [PubMed]
- Dowling, A.H.; Fleming, G.J. Is encapsulation of posterior glass-ionomer restoratives the solution to clinically induced variability introduced on mixing? Dent. Mater. 2008, 24, 957–966. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Material | Brand | Composition | Manufacturer |
|---|---|---|---|
| GIC | Fuji IX Capsule | Fluoroaluminium silicate glass, polyacrylic acid, polybasic carboxylic acid | GC America Inc., Alsip, IL, USA |
| RMGIC | Fuji II LC Capsule | 2-Hydroxyethyl methacrylate, polyacrylic acid, water; 58 wt% fluoroaluminumsilicate | GC America Inc., Alsip, IL, USA |
| Conditioner | GC Conditioner | 20% polyacrylic acid and 3% aluminum chloride | GC America Inc., Alsip, IL, USA |
| Characteristic | Rating | Criteria |
|---|---|---|
| Postoperative sensitivity | Alpha | No postoperative sensitivity |
| Bravo | Postoperative sensitivity | |
| Secondary caries | Alpha | No evidence of caries contiguous with margin of restoration |
| Bravo | Caries evident contiguous with margin of restoration | |
| Anatomic form | Alpha | Restoration continuous with existing anatomic form |
| Bravo | Restorations continuous with existing anatomic form, but not exposing cement material or dentin | |
| Charlie | Sufficient material lost to expose cement material or dentin | |
| Color match | Alpha | No mismatch in color, shade, and translucency between restoration and adjacent tooth structure |
| Bravo | Mismatch between restoration and tooth structure within normal range of color, shade, and translucency | |
| Charlie | Mismatch between restoration and tooth structure outside normal range of color, shade, and translucency | |
| Surface roughness | Alpha | Smooth surface |
| Bravo | Slightly rough or pitted, can be refinished | |
| Charlie | Rough, cannot be refinished | |
| Marginal discoloration | Alpha | No discoloration on margin between restoration and tooth structure |
| Bravo | Discoloration on margin between restoration and tooth structure | |
| Charlie | Discoloration has penetrated along margin of restorative material in pulpal direction | |
| Marginal integrity | Alpha | No visible evidence of ditching along margin |
| Bravo | Visible evidence of ditching along margin not extending to DE junction | |
| Charlie | Dentin or base is exposed along margin | |
| Delta | Restoration is mobile, fractured, or missing |
| Aspects ← Evaluated | GIC ↓ Restorations (Age) | Alfa (%) | Bravo (%) | Charlie (%) | Delta (%) | ||||
|---|---|---|---|---|---|---|---|---|---|
| 6 Months to 1.5 Years | 2.5 Years to 3.5 Years | 6 Months to 1.5 Years | 2.5 Years to 3.5 Years | 6 Months to 1.5 Years | 2.5 Years to 3.5 Years | 6 Months to 1.5 Years | 2.5 Years to 3.5 Years | ||
| Postoperative sensitivity | 100 | 100 | - | - | - | - | - | - | |
| Secondary caries | 96.3 | 93.5 | 3.7 | 6.5 | - | - | - | - | |
| Anatomic form | 82.9 | 76.9 | 14.3 | 19.2 | 2.6 | 3.8 | - | - | |
| Color match | 51.4 | 38.5 | 45.7 | 61.5 | 2.9 | - | - | - | |
| Surface roughness | 1.5 | 1.3 | 98.5 | 98.7 | - | - | - | - | |
| Marginal discoloration | 77.1 | 55.8 | 22.9 | 44.2 | - | - | - | - | |
| Marginal integrity | 65.7 | 29.2 | 25.7 | 47.8 | 5.7 | 19.2 | 2.9 | 3.8 | |
| Aspects ← Evaluated | RMGIC ↓ Restorations (Age) | Alfa (%) | Bravo (%) | Charlie (%) | Delta (%) | ||||
|---|---|---|---|---|---|---|---|---|---|
| 6 Months to 1.5 Years | 2.5 Years to 3.5 Years | 6 Months to 1.5 Years | 2.5 Years to 3.5 Years | 6 Months to 1.5 Years | 2.5 Years to 3.5 Years | 6 Months to 1.5 Years | 2.5 Years to 3.5 Years | ||
| Postoperative sensitivity | 98.2 | 100 | 1.8 | - | - | - | - | - | |
| Secondary caries | 98.3 | 92.3 | 1.7 | 7.7 | |||||
| Anatomic form | 94.7 | 82.7 | 5.3 | 17.3 | - | - | - | - | |
| Color match | 73.7 | 73.1 | 22.8 | 23.0 | 3.5 | 3.9 | - | - | |
| Surface roughness | 1.8 | 1.6 | 98.2 | 96.5 | - | 1.9 | - | - | |
| Marginal discoloration | 77.2 | 57.7 | 22.8 | 42.3 | - | - | - | - | |
| Marginal integrity | 54.4 | 28.9 | 43.8 | 62.0 | 1.8 | 9.1 | - | - | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Santos, M.J.M.C.; Leon, L.; Siddique, I.; Butler, S. Retrospective Clinical Evaluation of RMGIC/GIC Class V Restorations. Dent. J. 2023, 11, 225. https://doi.org/10.3390/dj11090225
Santos MJMC, Leon L, Siddique I, Butler S. Retrospective Clinical Evaluation of RMGIC/GIC Class V Restorations. Dentistry Journal. 2023; 11(9):225. https://doi.org/10.3390/dj11090225
Chicago/Turabian StyleSantos, Maria Jacinta M. C., Lucy Leon, Imad Siddique, and Sheila Butler. 2023. "Retrospective Clinical Evaluation of RMGIC/GIC Class V Restorations" Dentistry Journal 11, no. 9: 225. https://doi.org/10.3390/dj11090225
APA StyleSantos, M. J. M. C., Leon, L., Siddique, I., & Butler, S. (2023). Retrospective Clinical Evaluation of RMGIC/GIC Class V Restorations. Dentistry Journal, 11(9), 225. https://doi.org/10.3390/dj11090225