
Clinical and Radiographic Parameters for Early Periodontitis Diagnosis: A Comparative Study

 , , and
, , and
Abstract

1. Introduction
2. Material and Method
2.1. Study Participant
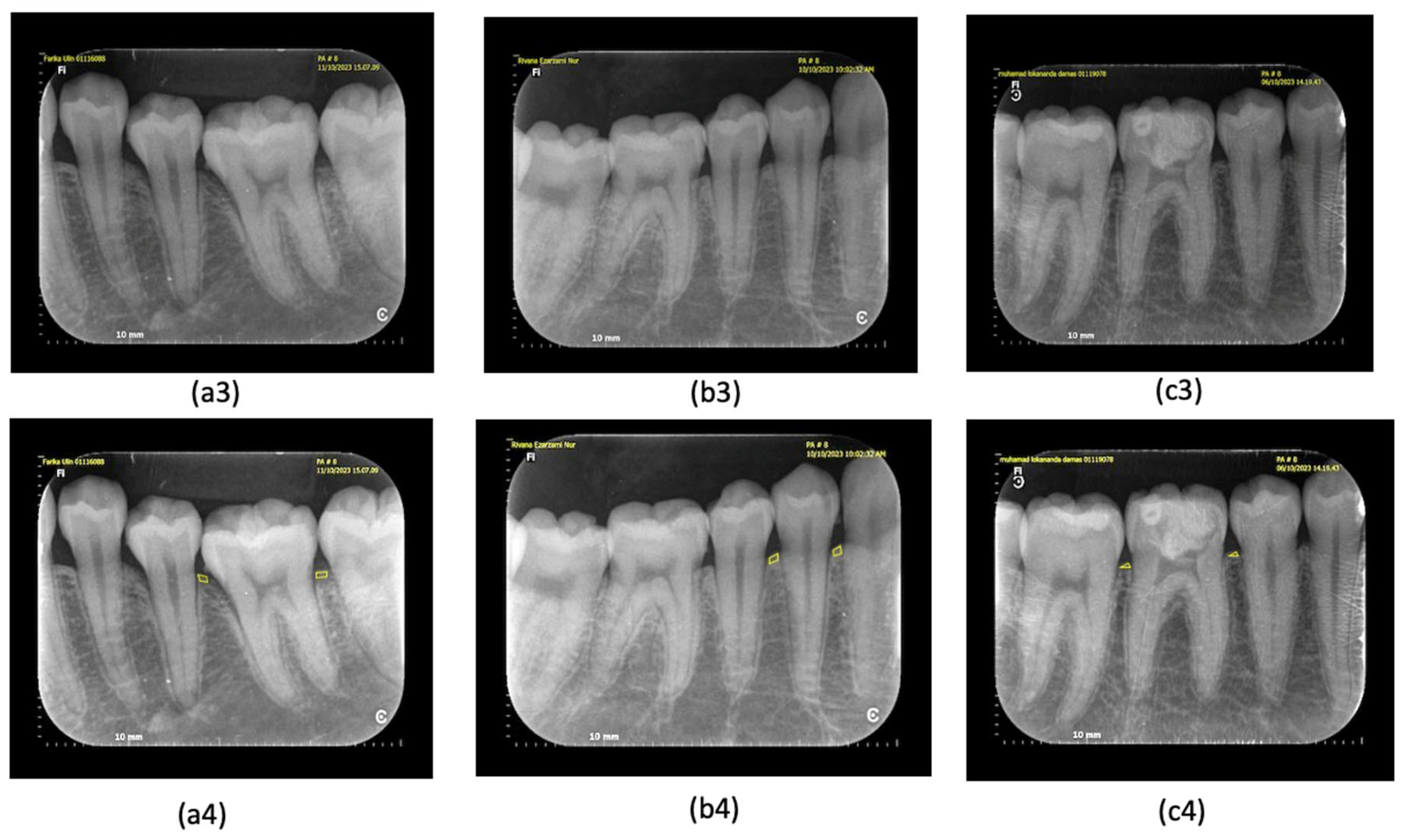
2.2. Set of Clinical Examination and Periapical Radiograph
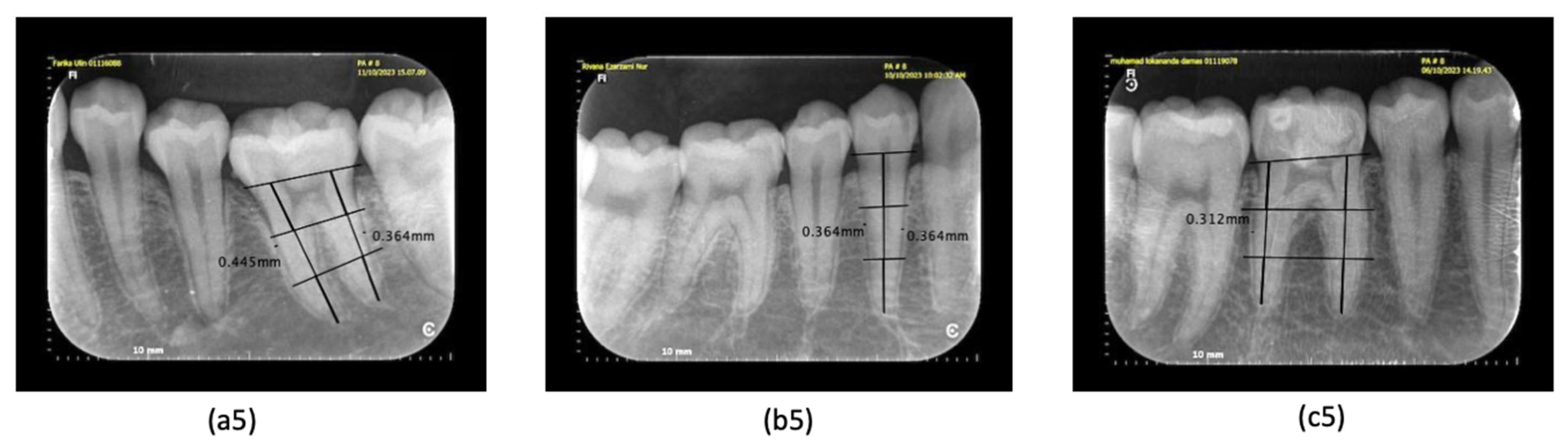
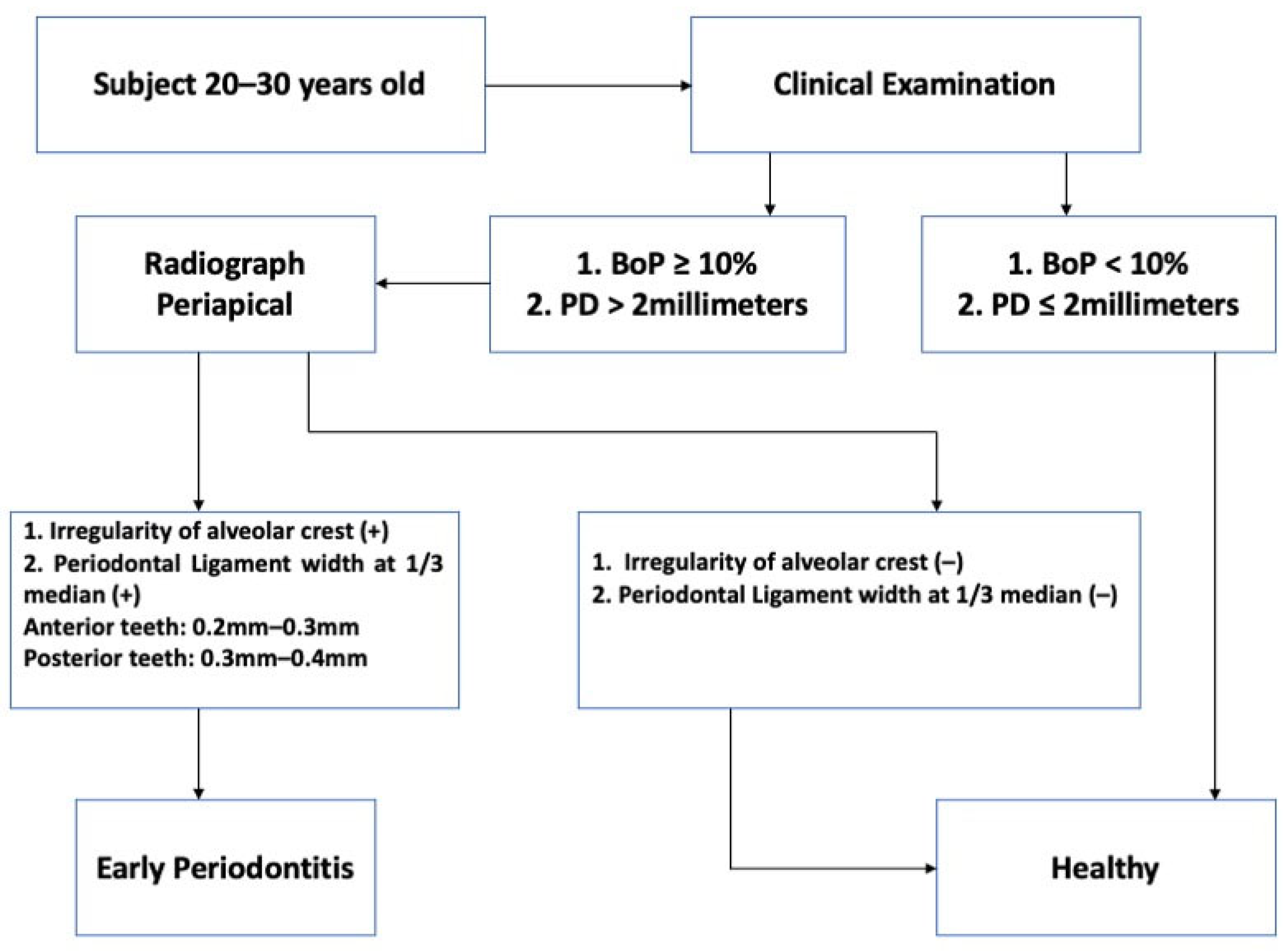
2.3. Diagnostic Standard
2.4. Consensus Decision (Reference Standard)
2.5. Data Management and Statistical Analysis
3. Result
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Do, J.H.; Takei, H.H.; Carranza, F.A. Periodontal Examination and Diagnosis. In Carranza; Elsevier: Amsterdam, The Netherlands, 2019; pp. 378–396. ISBN 0323523005. [Google Scholar]
- Chapple, I.L.C.; Mealey, B.L.; Van Dyke, T.E.; Bartold, P.M.; Dommisch, H.; Eickholz, P.; Geisinger, M.L.; Genco, R.J.; Glogauer, M.; Goldstein, M.; et al. Periodontal health and gingival diseases and conditions on an intact and a reduced periodontium: Consensus report of workgroup 1 of the 2017 World Workshop on the Classification of Periodontal and Peri-Implant Diseases and Conditions. J. Periodontol. 2018, 89, S74–S84. [Google Scholar] [CrossRef] [PubMed]
- Tonetti, M.S.; Greenwell, H.; Kornman, K.S. Staging and grading of periodontitis: Framework and proposal of a new classification and case definition. J. Clin. Periodontol. 2018, 45, S149–S161. [Google Scholar] [CrossRef]
- Papapanou, P.N.; Sanz, M.; Buduneli, N.; Dietrich, T.; Feres, M.; Fine, D.H.; Flemmig, T.F.; Garcia, R.; Giannobile, W.V.; Graziani, F.; et al. Periodontitis: Consensus report of workgroup 2 of the 2017 World Workshop on the Classification of Periodontal and Peri-Implant Diseases and Conditions. J. Clin. Periodontol. 2018, 45, S162–S170. [Google Scholar] [CrossRef]
- Elashiry, M.; Meghil, M.M.; Arce, R.M.; Cutler, C.W. From manual periodontal probing to digital 3-D imaging to endoscopic capillaroscopy: Recent advances in periodontal disease diagnosis. J. Periodontal Res. 2019, 54, 1–9. [Google Scholar] [CrossRef]
- Scarfe, W.C.; Azevedo, B.; Pinheiro, L.R.; Priaminiarti, M.; Sales, M.A.O. The emerging role of maxillofacial radiology in the diagnosis and management of patients with complex periodontitis. Periodontol. 2000 2017, 74, 116–139. [Google Scholar] [CrossRef]
- Ortman, L.F.; McHenry, K.; Hausmann, E. Relationship Between Alveolar Bone Measured by 125 I Absorptiometry With Analysis of Standardized Radiographs: 2. Bjorn Technique. J. Periodontol. 1982, 53, 311–314. [Google Scholar] [CrossRef] [PubMed]
- Hull, P.S.; Hillam, D.G.; Beal, J.F. A radiographic study of the prevalence of chronic periodontitis in 14-year-old English schoolchildren. J. Clin. Periodontol. 1975, 2, 203–210. [Google Scholar] [CrossRef] [PubMed]
- Xie, J.X. Radiographic analysis of normal periodontal tissues. Zhonghua Kou Qiang Yi Xue Za Zhi 1991, 26, 339–341. [Google Scholar]
- White, S.; Pharoah, M. Oral Radiology: Principles and Interpretation, 7th ed.; Elsevier: St. Louis, MO, USA, 2014. [Google Scholar]
- Kronfeld, R. Histologic Study of the Influence of Function on the Human Periodontal Membrane. J. Am. Dent. Assoc. 1931, 18, 1242–1274. [Google Scholar] [CrossRef]
- Coolidge, E.D. The Thickness of the Human Periodontal Membrane. J. Am. Dent. Assoc. Dent. Cosm. 1937, 24, 1260–1270. [Google Scholar] [CrossRef]
- Black, G.V. A study of the Periosteum and Periodontal Membrane; WT Keener: Chicago, IL, USA, 1887; p. 73. [Google Scholar]
- Bodecker, C.F. Fundamentals of Dental Histology and Embryology; The Macmillan Company: New York, NY, USA, 1926. [Google Scholar]
- Eickholz, P.; Hausmann, E. Accuracy of radiographic assessment of interproximal bone loss in intrabony defects using linear measurements. Eur. J. Oral Sci. 2000, 108, 70–73. [Google Scholar] [CrossRef] [PubMed]
- Pepelassi, E.A.; Diamanti-Kipioti, A. Selection of the most accurate method of conventional radiography for the assessment of periodontal osseous destruction. J. Clin. Periodontol. 1997, 24, 557–567. [Google Scholar] [CrossRef]
- Tonetti, M.S.; Prato, G.P.; Williams, R.C.; Cortellini, P. Periodontal Regeneration of Human Infrabony Defects. III. Diagnostic Strategies to Detect Bone Gain. J. Periodontol. 1993, 64, 269–277. [Google Scholar] [CrossRef]
- Chapple, I.L.C.; Wilson, N.H.F. Manifesto for a paradigm shift: Periodontal health for a better life. Br. Dent. J. 2014, 216, 159–162. [Google Scholar] [CrossRef]
- Moutinho, R.P.; Coelho, L.; Silva, A.; Lobo Pereira, J.A.; Pinto, M.; Baptista, I.P. Validation of a dental image-analyzer tool to measure the radiographic defect angle of the intrabony defect in periodontitis patients. J. Periodontal Res. 2012, 47, 695–700. [Google Scholar] [CrossRef] [PubMed]
- Leroy, R.; Eaton, K.A.; Savage, A. Methodological issues in epidemiological studies of periodontitis—How can it be improved? BMC Oral Health 2010, 10, 8. [Google Scholar] [CrossRef]
- Scott, J.; Biancardi, A.M.; Jones, O.; Andrew, D. Artificial Intelligence in Periodontology: A Scoping Review. Dent. J. 2023, 11, 43. [Google Scholar] [CrossRef]
- Garnick, J.J.; Silverstein, L. Periodontal Probing: Probe Tip Diameter. J. Periodontol. 2000, 71, 96–103. [Google Scholar] [CrossRef]
- Trombelli, L.; Farina, R.; Silva, C.O.; Tatakis, D.N. Plaque-induced gingivitis: Case definition and diagnostic considerations. J. Periodontol. 2018, 89, S46–S73. [Google Scholar] [CrossRef]
- Cuschieri, S. The STROBE guidelines. Saudi J. Anaesth. 2019, 13, S31–S34. [Google Scholar] [CrossRef]
- Saxer, U.P.; Mühlemann, H.R. [Motivation and education]. SSO Schweiz. Monatsschr. Zahnheilkd 1975, 85, 905–919. [Google Scholar] [PubMed]
- Dentino, A.R.; Kassab, M.M.; Renner, E.J. Prevention of periodontal diseases. Dent. Clin. N. Am. 2005, 49, 573–594. [Google Scholar] [CrossRef] [PubMed]
- Kakar, A.; Blanchard, S.; Shin, D.; Maupomé, G.; Eckert, G.J.; John, V. Periodontal diagnosis and treatment planning—An assessment of the understanding of the new classification system. J. Dent. Educ. 2022, 86, 1573–1580. [Google Scholar] [CrossRef] [PubMed]
- White, S.C.; Pharoah, M.J. Oral Radiology: Principles and Interpretation; Elsevier Health Sciences: Amsterdam, The Netherlands, 2013. [Google Scholar]
- Peeran, S.W. Karthikeyan Ramalingam. Periodontal Diagnosis. In Essentials of Periodontics & Oral Implantology; Peeran, S.W., Karthikeyan, R., Eds.; Saranraj Jps Publication: Tamil Nadu, India, 2021; pp. 8–35. ISBN 9788195047543. [Google Scholar]
- Langland, O.; Langlais, R. .Principles of Dental Imaging, 2nd ed.; Lippincott Williams and Wilkins: Philadelphia, PA, USA, 1997. [Google Scholar]
- Kinane, D.F.; Stathopoulou, P.G.; Papapanou, P.N. Periodontal diseases. Nat. Rev. Dis. Prim. 2017, 3, 1–14. [Google Scholar] [CrossRef]
- Löe, H. The Gingival Index, the Plaque Index and the Retention Index Systems. J. Periodontol. 1967, 38, 610–616. [Google Scholar] [CrossRef]
- Patel, J.S.; Shin, D.; Willis, L.; Zai, A.; Kumar, K.; Thyvalikakath, T.P. Comparing gingivitis diagnoses by bleeding on probing (BOP) exclusively versus BOP combined with visual signs using large electronic dental records. Sci. Rep. 2023, 13, 17065. [Google Scholar] [CrossRef]
- Tonetti, M.S.; Sanz, M. Implementation of the new classification of periodontal diseases: Decision-making algorithms for clinical practice and education. J. Clin. Periodontol. 2019, 46, 398–405. [Google Scholar] [CrossRef] [PubMed]
- Fiorellini, J.P.; Sourvanos, D.; Sarimento, H.; Karimbux, N.; Luan, K.W. Periodontal and Implant Radiology. Dent. Clin. N. Am. 2021, 65, 447–473. [Google Scholar] [CrossRef]
- Eshraghi, V.T.; Malloy, K.A.; Tahmasbi, M. Role of cone-beam computed tomography in the management of periodontal disease. Dent. J. 2019, 7, 57. [Google Scholar] [CrossRef]
- Greenstein, G.; Caton, J.; Polson, A.M. Histologic Characteristics Associated With Bleeding After Probing and Visual Signs of Inflammation. J. Periodontol. 1981, 52, 420–425. [Google Scholar] [CrossRef]
- Trombelli, L.; Farina, R.; Silva, C.; Tatakis, D. Peri-implant diseases and conditions: Consensus report of workgroup 4 of the 2017 World Workshop on the Classification of Periodontal and Peri-Implant Diseases and Conditions. Br. Dent. J. 2018, 225, 141. [Google Scholar] [CrossRef]
- Milgrom, P. Quality control of end results: Identifying avoidable adverse events in dentistry. J. Am. Dent. Assoc. 1975, 90, 1282–1290. [Google Scholar] [CrossRef] [PubMed]
- Jacobs, R.; Fontenele, R.C.; Lahoud, P.; Shujaat, S.; Bornstein, M.M. Radiographic diagnosis of periodontal diseases—Current evidence versus innovations. Periodontol. 2000 2024, 95, 51–69. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Examination | Parameters | Healthy (n) | Early Periodontitis (n) | Total (n) |
|---|---|---|---|---|
| Clinical Examination | Bleeding on probing (BoP) | 1 (2.5%) | 39 (97.5%) | 40 |
| Pocket depth (PD) | 37 (92.5%) | 3 (7.5%) | 40 | |
| Periapical Radiograph Examination | Irregularity of alveolar crest | 16 (40%) | 24 (60%) | 40 |
| Periodontal ligament width (PDL) | 16 (40%) | 24 (60%) | 40 |
| Diagnose Decision | Bleeding on Probing (BoP) | p-Value | |
|---|---|---|---|
| No BoP | There is BoP | ||
| Healthy (n = 37) | 1 (2.7%) | 36 (97.3%) | 1.000 * |
| Early Periodontitis (n = 3) | 0 (0.0%) | 3 (100%) | |
| Diagnose Decision | Pocket Depth (PD) | p-Value | |
|---|---|---|---|
| No PD | There is PD | ||
| Healthy (n = 37) | 37 (100%) | 0 (0.0%) | 0.000 * |
| Early Periodontitis (n = 3) | 0 (0.0%) | 3 (100%) | |
| Diagnose Decision | Irregularity of Alveolar Crest | p-Value | |
|---|---|---|---|
| No Irregularity | There Is Irregularity | ||
| Healthy (n = 37) | 15 (40.5%) | 22 (59.5%) | 1.000 * |
| Early Periodontitis (n = 3) | 1 (33.3%) | 2 (66.7%) | |
| Diagnose Decision | Periodontal Ligament Width (PLW) | p-Value | |
|---|---|---|---|
| No PLW | There Is PLW | ||
| Healthy (n = 37) | 15 (40.5%) | 22 (59.5%) | 1.000 * |
| Early Periodontitis (n = 3) | 1 (33.3%) | 2 (66.7%) | |
| Bleeding on Probing (BoP) | Irregularity of Alveolar Crest | p-Value | |
|---|---|---|---|
| No Irregularity | There Is Irregularity | ||
| Healthy/BoP (–) (n = 1) | 1 (100%) | 0 (0.0%) | 0.400 * |
| Early Periodontitis/ BoP (+) (n = 39) | 15 (38.5%) | 24 (61.5%) | |
| Bleeding on Probing = (BoP) | Periodontal Ligament Width (PLW) | p-Value | |
|---|---|---|---|
| No PLW | There Is PLW | ||
| Healthy/BoP (–) (n = 1) | 1 (100%) | 0 (0.0%) | 0.400 * |
| Early Periodontitis/ BoP (+) (n = 39) | 15 (38.5%) | 24 (61.5%) | |
| Pocket Depth | Irregularity of Alveolar Crest | p-Value | |
|---|---|---|---|
| No Irregularity | There Is Irregularity | ||
| Healthy/PD (–) (n = 37) | 15 (40.5%) | 22 (59.5%) | 1.000 * |
| Early Periodontitis/ PD (+) (n = 3) | 1 (33.3%) | 2 (66.7%) | |
| Pocket Depth (PD) | Periodontal Ligament Width (PLW) | p-Value | |
|---|---|---|---|
| No PLW | There Is PLW | ||
| Healthy/PD (–) (n = 37) | 15 (40.5%) | 22 (59.5%) | 1.000 * |
| Early Periodontitis/ PD (+) (i = 3) | 1 (33.3%) | 2 (66.7%) | |
| Periodontal Ligament Width (PLW) | Irregularity of Alveolar Crest | p-Value | |
|---|---|---|---|
| No Irregularity | There Is Irregularity | ||
| Healthy/PLW (–) (n = 16) | 16 (100%) | 0 (0.0%) | 0.000 * |
| Early Periodontitis/ PLW (+) (n = 24) | 0 (0.0%) | 24 (100%) | |
| Parameter | Diagnose Decision | |
|---|---|---|
| Correlation Coefficient (r) | Sig (2-Tailed) | |
| Bleeding on probing | 0.95 | 0.553 |
| Pocket depth | 1.000 | 0.000 * |
| Irregularity | 0.39 | 0.809 |
| Periodontal ligament width | 0.39 | 0.809 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Fidyawati, D.; Masulili, S.L.C.; Iskandar, H.B.; Suhartanto, H.; Kiswanjaya, B.; Li, X. Clinical and Radiographic Parameters for Early Periodontitis Diagnosis: A Comparative Study. Dent. J. 2024, 12, 407. https://doi.org/10.3390/dj12120407
Fidyawati D, Masulili SLC, Iskandar HB, Suhartanto H, Kiswanjaya B, Li X. Clinical and Radiographic Parameters for Early Periodontitis Diagnosis: A Comparative Study. Dentistry Journal. 2024; 12(12):407. https://doi.org/10.3390/dj12120407
Chicago/Turabian StyleFidyawati, Desy, Sri Lelyati C. Masulili, Hanna Bachtiar Iskandar, Heru Suhartanto, Bramma Kiswanjaya, and Xue Li. 2024. "Clinical and Radiographic Parameters for Early Periodontitis Diagnosis: A Comparative Study" Dentistry Journal 12, no. 12: 407. https://doi.org/10.3390/dj12120407
APA StyleFidyawati, D., Masulili, S. L. C., Iskandar, H. B., Suhartanto, H., Kiswanjaya, B., & Li, X. (2024). Clinical and Radiographic Parameters for Early Periodontitis Diagnosis: A Comparative Study. Dentistry Journal, 12(12), 407. https://doi.org/10.3390/dj12120407