
Evaluating the Effectiveness of a Virtual Simulation Platform for Apexification Learning



Abstract
:
1. Introduction
2. Materials and Methods
2.1. Basics of Apexification Learning Using the Simulated Virtual Platform
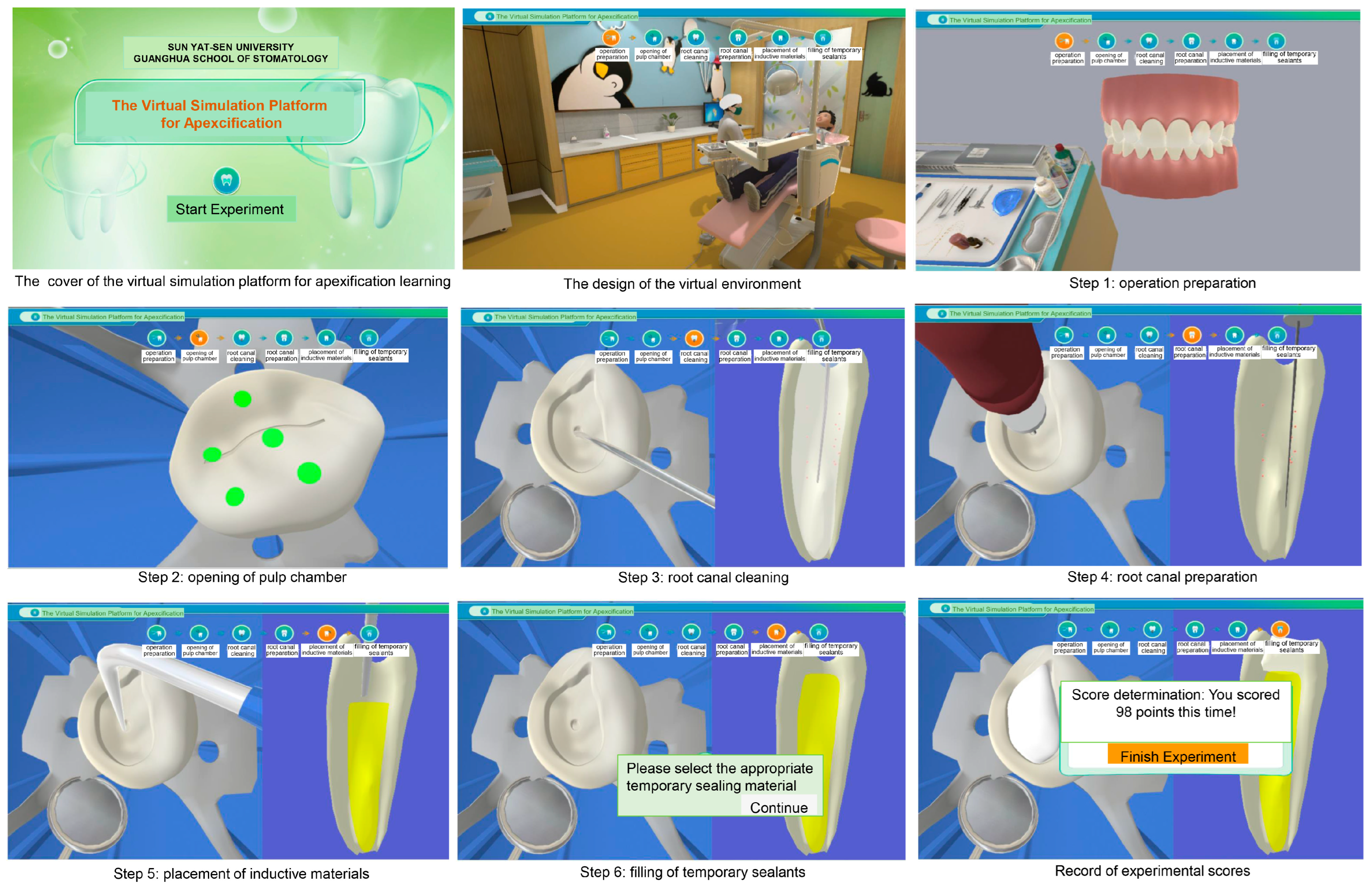
2.1.1. General Information about the Virtual Simulation Learning Platform
2.1.2. Details about the Simulated Virtual Learning Platform
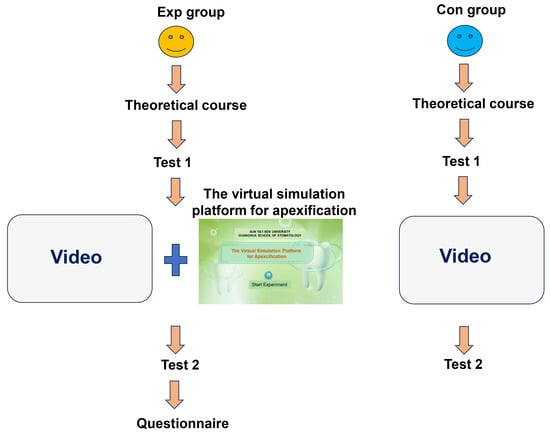
2.2. Study Procedure
2.3. Statistical Analysis
3. Results
3.1. Score Comparison between the Con and Exp Groups
3.2. Score Comparison in the Con and Exp Groups Separately
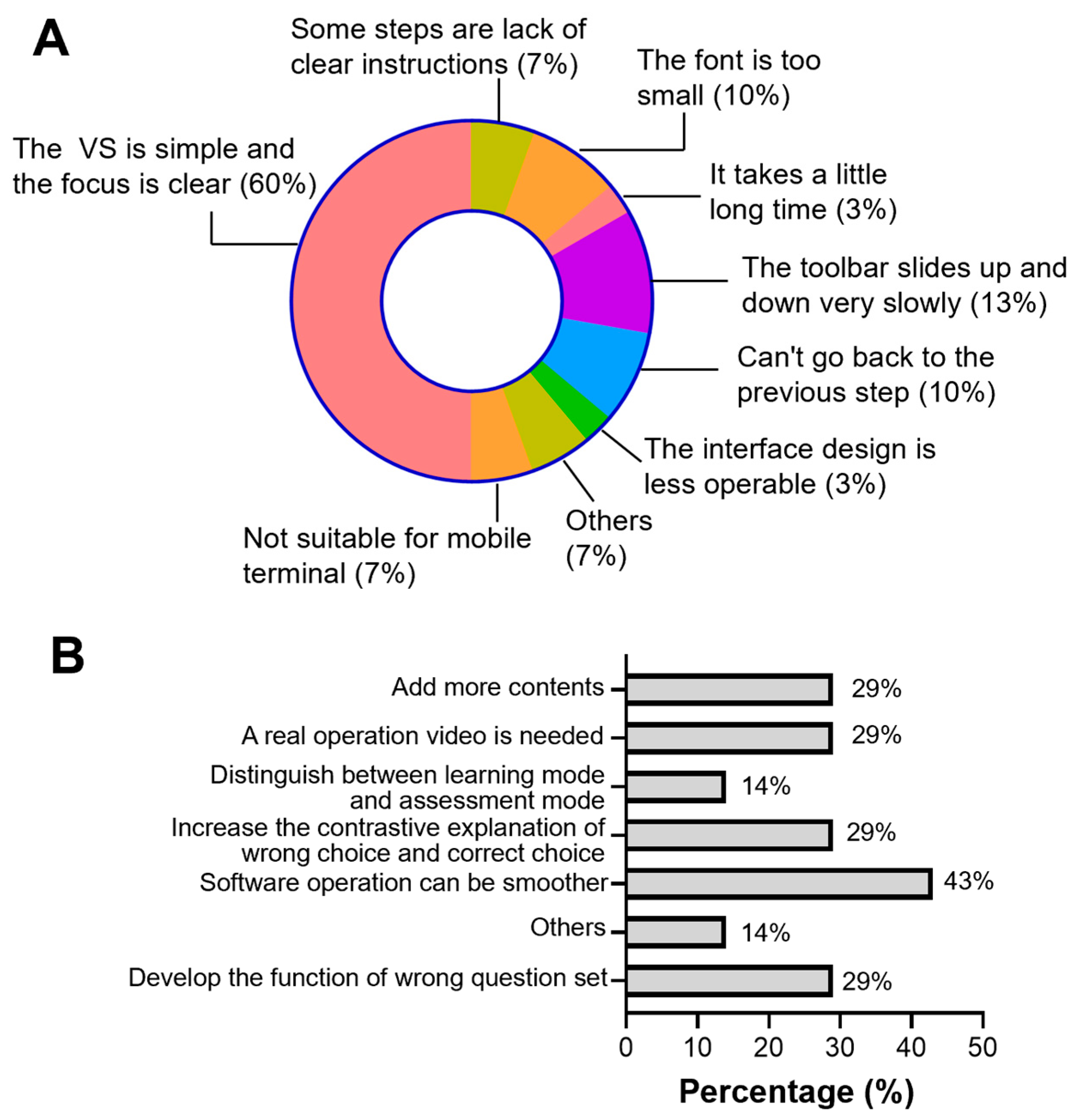
3.3. Exp Group’s Responses to the Questionnaire
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A
- Choose the appropriate examination method for the affected tooth ( )
- X-ray machine or X-ray image
- Dental pulp vitality tester
- Dental pulp sensory temperature tester
- Percussion
Explanations:- A:
- Correct answer! Children and adolescents with traumatic teeth need to undergo X-ray examination to examine the degree of root development, periodontal ligament damage, and the presence of lesions around the apex. Imaging examination is an important basis for diagnosing young permanent teeth with periapical disease.
- B:
- Wrong answer! The development of the apical foramen of young permanent teeth is not complete, and the accuracy of pulp electrical vitality test is relatively low. In addition, the credibility of the response from children is relatively low. At the same time, there may be “pulp shock” in injured teeth. Therefore, clinical practice does not advocate using pulp electrical vitality test results to determine pulp status.
- C:
- Correct answer! Although the development of apical foramen in young permanent teeth is not yet complete, pulp vitality tests conducted in combination with medical history, intraoral examination, and X-ray examination can be used as a reference to determine the status of pulp.
- D:
- Correct answer! The status of the periapical periodontal ligament can be determined through percussion examination.
- Facing the injured teeth, the doctor asked the child to take a dental X-ray, which showed that the apical foramen with large diameter was not closed, and there were shadows in the apical area. At this time, what is the most appropriate treatment method? ( )
- Pulpotomy
- Direct pulp capping
- Apexification
- Root canal therapy
Explanations:- A:
- Wrong answer! Based on clinical manifestations and examination results, the pulp of the affected tooth has necrotized and pulp preservation treatment cannot be chosen.
- B:
- Wrong answer! Based on clinical manifestations and examination results, the pulp of the affected tooth has necrotized and pulp preservation treatment cannot be chosen.
- C:
- Correct answer! Apexification is a classic operation for treating young permanent tooth with pulp and periapical disease. It is a method of preserving the apical pulp or depositing hard tissue around the apex with drugs such as calcium hydroxide on the basis of controlling infection, so as to promote the continued development of the root and the formation of the apex.
- D:
- Wrong answer!
- Please perform moisture isolation operation, click ( ) to continueA. Rubber dam B. Cotton rollExplanations:
- A:
- Correct answer! Rubber dams have a good moisture isolation effect and effectively reduce the possibility of pollution. Moreover, rubber dams increase operational safety and facilitate clear surgical field.
- B:
- Wrong answer! The moisture isolation effect of cotton rolls is poor, and they need to be constantly replaced, which is not conducive to aseptic treatment.
- Open the pulp chamber along the puncture site to prepare the channel. Please select a tool ( )A. Fast dental handpiece B. Slow dental handpieceExplanations:
- A:
- Correct answer! The fast dental handpiece can efficiently remove the wall detritus and most of the bottom detritus, and prepare the necessary cave shape.
- B:
- Wrong answer!
- Please choose the appropriate bur for opening of the pulp chamber ( )A. Fissure bur B. Round bur C. Inverted burExplanations:
- A:
- Wrong answer!
- B:
- Correct answer! The fissure bur can open the pulp and prepare a straight-line channel, and the round bur can lift and remove the top of the pulp chamber.
- C:
- Wrong answer!
- Choose the appropriate root canal irrigation solution ( )A. Saline+3% hydrogen peroxide B. 5.25% sodium hypochloriteC. 17% EDTA solution D. 7.5% povidone iodineExplanations:
- A:
- Correct answer! Adequate irrigation and effective control of inflammation are important steps in apexification.
- B:
- Wrong answer! Excessive concentration of sodium hypochlorite has a certain toxic effect, which can stimulate and damage the periapical tissue.
- C:
- Wrong answer! EDTA solution needs to be combined with sodium hypochlorite to achieve good cleaning effect.
- D:
- Wrong answer! 7.5% povidone iodine can easily cause tooth discoloration.
- Select nickel-titanium (NiTi) instruments with appropriate taper for root canal cleaning and preparation ( )A. #8 NiTi file B. #15 NiTi file C. #30 NiTi fileExplanations:
- A:
- Wrong answer! The root canal of young permanent teeth is relatively large, and NiTi files with too small taper cannot effectively clean and prepare the root canal, and are prone to extending beyond the apical foramen.
- B:
- Wrong answer! The root canal of young permanent teeth is relatively large, and NiTi files with too small taper cannot effectively clean and prepare the root canal, and are prone to extending beyond the apical foramen.
- C:
- Correct answer! Young permanent teeth have larger root canals, and the selection of large taper NiTi files can effectively clean and prepare the root canal.
- Select appropriate materials for apexification ( )A. Vitapex or Metapex B. Gutta-percha C. Light cured calcium hydroxideD. Handmade calcium hydroxideExplanations:
- A:
- Correct answer! Vitapex or Metapex is a manufactured calcium hydroxide oil-based product with a certain viscosity, which is easy to place at the root apex, slows down the rate of calcium hydroxide decomposition, plays a sustained antibacterial role, and promotes sealing of root apex.
- B:
- Wrong answer! Gutta-percha is a non-absorbable root filling material and cannot be used when the apical foramen of young permanent teeth is not closed.
- C:
- Wrong answer! Light curing calcium hydroxide cannot be used for root canal disinfection.
- D:
- Wrong answer! The disinfection effect of handmade calcium hydroxide only lasts for about 2 weeks. Frequent dressing changes will increase the stimulation of the affected root apex, and repeated opening of the pulp cavity will also increase the risk of reinfection. Moreover, handmade calcium hydroxide is difficult to fill the root apex tightly.
- Please select the appropriate temporary sealing material ( )A. Zinc oxide (ZOE) B. Glass ionomerExplanations:
- A:
- Wrong answer! ZOE has a good sealing effect within 1 week, and the coronal leakage will increase with the extension of the temporary sealing time. It is suitable for short-term treatment, and it is not recommended for treatment requiring temporary sealing for more than 2 weeks. Moreover, eugenol can affect the polymerization of the resin, and manual modulation may lead to unstable performance.
- B:
- Correct answer! Glass ionomers have good edge sealing properties, reduce micro leakage, and release fluoride ions that can induce partial softened dentin remineralization, which is suitable for treatment with a long observation period such as apexification and pulpotomy.
- After completing apexification, please choose the right time for shape repair ( )A. After apexification B. After apical closureExplanations:
- A:
- Correct answer! After the child has no conscious symptoms, the appearance repair of teeth as soon as possible can restore the aesthetic and chewing function in time, and maintain the gap.
- B:
- Wrong answer! Long-term dental defects will reduce the aesthetic and chewing function of children, lead to psychological disorders, and may cause loss of space.
- The appropriate timing for permanent root canal treatment of affected teeth after apexification is ( )A. When the root apex of the affected tooth is closed B. The patient is 12 years oldC. The patient is 18 years oldExplanations:
- A:
- Correct answer! When the apical foramen of the affected tooth is closed or the apical barrier is formed, permanent root canal treatment can be performed.
- B:
- Wrong answer! There are significant individual differences in the degree of tooth development, especially in the development of traumatic teeth. It is impossible to determine the treatment time of affected teeth based on age alone.
- C:
- Wrong answer! There are significant individual differences in the degree of tooth development, especially in the development of traumatic teeth. It is impossible to determine the treatment time of affected teeth based on age alone.
Appendix B
- Apexification is suitable for ( )
- Deciduous teeth
- Permanent teeth with fully developed tooth roots
- Young permanent teeth with pulp necrosis or concurrent periapical inflammation
- Which of the following is not a success criterion for apexification? ( )
- The root apex continues to develop, the root canal becomes narrow, and the root apex is closed.
- The root canal has no change but the root apex is closed.
- There is a trace of colored liquid discharged from the root canal.
- No development was observed, and hard tissue barrier formation was detected in the root canal.
- A calcification barrier is formed at 1/3 of the root end.
- What is the incorrect description about apexification? ( )
- The infected material in the root canal is removed and induced by drugs to promote root development and apical closure.
- Calcium hydroxide preparations are commonly used inducers.
- It is suitable for young permanent teeth with severe pulp lesions or concurrent periodontitis before the root development is complete.
- It is suitable for the tooth with residual living pulp at the root end, or the dental papilla has not been damaged.
- Successful apexification means that the root continues to develop and the apex is formed.
- A 7 years old boy had spontaneous pain in the first lower right permanent molar. He was unable to sleep for the past two days. Examination revealed deep caries and exposed pulp on the occlusal surface. Discomfort during probing (+) and percussion. No redness or swelling in the gums. What treatment should be taken? ( )
- Root canal treatment
- Pulp mummification
- Apexification
- Filling after oral anti-inflammatory medication
- Direct pulp capping
- 5.
- What is the incorrect statement about the operation steps of apexification? ( )
- Teeth with acute symptoms should first undergo emergency treatment, open the root canal, and continue treatment after the acute inflammations disappear.
- The root canal preparation was mainly mechanical preparation, supplemented by chemical preparation.
- X-rays are routinely taken before treatment.
- The position and size of pulp opening should be such that the instrument enters the root canal in a straight line as much as possible.
- 6.
- When performing apexification, the stopping point of the operation should be located at ( ).A. The end of the root tip B. 1 mm above the end of the root tipC. 0.5 mm above the end of the root tip D. 2 mm above the end of the root tip
- 7.
- The commonly used irrigation solution for root canal preparation during apexification does not include ( )A. 17%EDTA B. 3% hydrogen peroxideC. physiological saline D. 1.5% sodium hypochlorite
- 8.
- Which of the following drugs should not be used as root canal disinfectants during apexification? ( )A. Pomegranate oil B. Glutaraldehyde C. Camphor phenol D. Antibiotic paste
- 9.
- The statement about calcium hydroxide as apexification inducer is incorrect ( )
- The induction effect of calcium hydroxide originates from its strong alkalinity and the combined effect of calcium ions.
- Calcium hydroxide is currently the preferred drug for apexification.
- Calcium hydroxide water paste is easy to fill the root apex tightly.
- Calcium hydroxide is a paste that is easily absorbed by inflammatory tissues.
- 10.
- Which of the following statements is incorrect during apexification re-examination? ( )
- Check if the filling material is intact.
- Replace calcium hydroxide every time when the re-examination is conducted.
- X-ray examination should be taken.
- Observe the periapical condition and apical formation status.
- 11.
- The tissues on which apexification depends do not include ( )A. Periodontal ligament B. Epithelial root sheathC. Residual living pulp at the apex D. Dental papilla at the apex
- 12.
- Which of the following is NOT a disadvantage of apexification compared with apical barrier surgery? ( )A. Longer treatment cycle B. Significantly lower success rateC. Increased risk of root fracture D. Higher risk of reinfection in the root canal
Appendix C
- Female, 8 years old, presents 1 week after anterior tooth trauma. Right upper central incisor crown fracture 2/3, subgingival 1 mm on the mesial side. There is no pain during probing at the exposed pulp, and percussion (+). The tooth shows dark red bleeding and degree I looseness. X-ray shows no root fracture, and the root apex appears as a trumpet shaped opening. Which is the appropriate treatment method choice? ( )
- Calcium hydroxide pulpotomy
- Formaldehyde cresol pulpotomy
- Apexification
- Root canal therapy
- How often should follow-up be conducted after apexification? ( )A. 1–3 months B. 3–6 months C. 9–12 months D. 6–9 months E. 12 months
- What is the correct timing for permanent root canal filling after apexification? ( )A. 12 years old B. When the apical calcification barrier begins to formC. When the apical calcification barrier forms D. When there is calcified tissue deposition
- Which of the following is considered as ineffective treatment according to the evaluation criteria for apexification? ( )
- Failure to extend the tooth root or no reduction or disappearance of periapical lesions
- Periapical lesions disappear, roots elongate, root canal shrink, apical formation or root closure occurs
- Periapical lesions disappear, roots elongate, incomplete or highly irregular apical formation
- 5.
- When performing apexification, the method to determine the working length of the root canal is ( )A. Root canal length measuring instrument B. Referring to the preoperative X-rayC. Determining the location of apical stenosis by hand feeling
- 6.
- Which of the following statements is incorrect during root canal preparation for apexification? ( )
- Whether it is mechanical preparation or chemical flushing, attention should be paid to avoiding damage to the apical dental papilla or epithelial root sheath.
- Due to the large size of the apical foramen of young permanent teeth, the root canal instruments can be slightly extended beyond the apical foramen during mechanical preparation.
- Be careful not to apply pressure during rinsing to avoid pushing infectious substances out of the root apex.
- When performing root canal preparation, the movements should be as gentle as possible.
- 7.
- The material that is not suitable for apexification is ( )A. Vitapex B. Metapex C. Photocured calcium hydroxide D. MTA
- 8.
- The appropriate timing for shape restoration after completing apexification is ( )A. After completing apexification B. After apical closureC. Formation of apical calcification barrier D. After root canal treatment
- 9.
- Which of the following is a possible treatment option after failure of apexification? ( )A. Apical barrier B. revascularization C. pulpotomy
- 10.
- On X-rays, a calcified barrier can be seen at one-third of the root apex. According to Frank classification, which type of root development after apexification is this? ( )A. A-type B. B-type C. C-type D. D-type
- 11.
- What is the wrong statement about the function of epithelial root sheath in apexification? ( )
- Epithelial root sheath can prevent periodontal ligament cells from growing into the root canal.
- There are a large number of undifferentiated mesenchymal cells in the epithelial root sheath, which can further differentiate into hard tissue.
- If the Hertwig epithelial root sheath is completely destroyed, it will lead to the cessation of normal tooth root development and also indicates the end of hard tissue deposition in the apical area of the root.
- During treatment, it is important to preserve the activity of the epithelial root sheath as much as possible.
- 12.
- Which of the following is not a factor in determining the overall duration of apexification? ( )A. Frequency of dressing change B. Degree of periapical inflammationC. patient’s physical condition D. The original length of the root of the tooth
References
- Umoren, R.A.; Schmölzer, G.M. Virtual simulations for neonatal education. Semin. Perinatol. 2023, 47, 151826. [Google Scholar] [CrossRef]
- Xu, X.; Allen, W.; Miao, Z.; Yao, J.; Sha, L.; Chen, Y. Exploration of an interactive “Virtual and Actual Combined” teaching mode in medical developmental biology. Biochem. Mol. Biol. Educ. 2018, 46, 585–591. [Google Scholar] [CrossRef]
- Wang, Q.; Li, C.; Xie, Z.; Bu, Z.; Shi, L.; Wang, C.; Jiang, F. The development and application of virtual reality animation simulation technology: Take gastroscopy simulation system as an example. Pathol. Oncol. Res. 2020, 26, 765–769. [Google Scholar] [CrossRef]
- Wang, K.; Zhang, L.; Ye, L. A nationwide survey of online teaching strategies in dental education in China. J. Dent. Educ. 2021, 85, 128–134. [Google Scholar] [CrossRef]
- Quiroga, M.D.M.; Choate, J.K. A virtual experiment improved students’ understanding of physiological experimental processes ahead of a live inquiry-based practical class. Adv. Physiol. Educ. 2019, 43, 495–503. [Google Scholar] [CrossRef]
- Lu, J.; Zhang, L.; Ye, L. Construction and application of dental virtual reality simulation teaching system in China: Necessity and strategies. Eur. J. Dent. Educ. 2023. Epub ahead of print. [Google Scholar] [CrossRef]
- Chen, Y.; Deng, J.; Li, B.; Yang, Y.; He, Z.; Ye, L.; Zhang, L.; Ren, Q.; Zheng, Q. Curriculum setting and students’ feedback of pre-clinical training in different dental schools in China-A national-wide survey. Eur. J. Dent. Educ. 2022, 26, 28–35. [Google Scholar] [CrossRef] [PubMed]
- Murbay, S.; Neelakantan, P.; Chang, J.W.W.; Yeung, S. Evaluation of the introduction of a dental virtual simulator on the performance of undergraduate dental students in the pre-clinical operative dentistry course. Eur. J. Dent. Educ. 2020, 24, 5–16. [Google Scholar] [CrossRef]
- Zhang, B.; Li, S.; Gao, S.; Hou, M.; Chen, H.; He, L.; Li, Y.; Guo, Y.; Wang, E.; Cao, R.; et al. Virtual versus jaw simulation in oral implant education: A randomized controlled trial. BMC Med. Educ. 2020, 20, 272. [Google Scholar] [CrossRef] [PubMed]
- Li, Y.; Ye, H.; Ye, F.; Liu, Y.; Lv, L.; Zhang, P.; Zhang, X.; Zhou, Y. The current situation and future prospects of simulators in dental education. J. Med. Internet Res. 2021, 23, e23635. [Google Scholar] [CrossRef] [PubMed]
- Zafar, S.; Lai, Y.; Sexton, C.; Siddiqi, A. Virtual Reality as a novel educational tool in pre-clinical paediatric dentistry training: Students’ perceptions. Int. J. Paediatr. Dent. 2020, 30, 791–797. [Google Scholar] [CrossRef]
- Zafar, S.; Siddiqi, A.; Yasir, M.; Zachar, J.J. Pedagogical development in local anaesthetic training in paediatric dentistry using virtual reality simulator. Eur. Arch. Paediatr. Dent. 2021, 22, 667–674. [Google Scholar] [CrossRef]
- Lu, J.; Yang, X.; Zhao, W.; Lin, J. Effect analysis of a virtual simulation experimental platform in teaching pulpotomy. BMC Med. Educ. 2022, 22, 760. [Google Scholar] [CrossRef]
- Philip, N.; Ali, K.; Duggal, M.; Daas, H.; Nazzal, H. Effectiveness and student perceptions of haptic virtual reality simulation training as an instructional tool in pre-clinical paediatric dentistry: A pilot pedagogical study. Int. J. Environ. Res. Public. Health 2023, 20, 4226. [Google Scholar] [CrossRef] [PubMed]
- Guerrero, F.; Mendoza, A.; Ribas, D.; Aspiazu, K. Apexification: A systematic review. J. Conserv. Dent. 2018, 21, 462–465. [Google Scholar] [CrossRef]
- Lu, H.; Lu, J.; Guo, J.; Zeng, B.; Zeng, Q.; Zhao, W.; Lin, J. Radiographic outcomes and prognostic factors in nonvital immature permanent teeth after apexification with modified calcium hydroxide paste: A retrospective study. Clin. Oral. Investig. 2022, 26, 5079–5088. [Google Scholar] [CrossRef] [PubMed]
- Shaik, I.; Dasari, B.; Kolichala, R.; Doos, M.; Qadri, F.; Arokiyasamy, J.L.; Tiwari, R.V.C. Comparison of the success rate of mineral trioxide aggregate, endosequence bioceramic root repair material, and calcium hydroxide for apexification of immature permanent teeth: Systematic review and meta-analysis. J. Pharm. Bioallied Sci. 2021, 13, S43–S47. [Google Scholar] [CrossRef] [PubMed]
- Naved, N.; Umer, F.; Khowaja, A.R. Cost-Effectiveness analysis of regenerative endodontics versus MTA apexification. JDR Clin. Trans. Res. 2023. Epub ahead of print. [Google Scholar] [CrossRef]
- Shabahang, S. Treatment options: Apexogenesis and apexification. J. Endod. 2013, 39, S26–S29. [Google Scholar] [CrossRef]
- American Academy of Pediatric Dentistry. Guideline on pulp therapy for primary and immature permanent teeth. Pediatr. Dent. 2016, 38, 280–288. [Google Scholar]
- Al Khasawnah, Q.; Hassan, F.; Malhan, D.; Engelhardt, M.; Daghma, D.E.S.; Obidat, D.; Lips, K.S.; El Khassawna, T.; Heiss, C. Nonsurgical clinical management of periapical lesions using calcium hydroxide-iodoform-silicon-oil paste. Biomed. Res. Int. 2018, 2018, 8198795. [Google Scholar] [CrossRef]
- Damle, S.G.; Bhattal, H.; Loomba, A. Apexification of anterior teeth: A comparative evaluation of mineral trioxide aggregate and calcium hydroxide paste. J. Clin. Pediatr. Dent. 2012, 36, 263–268. [Google Scholar] [CrossRef] [PubMed]
- Lin, J.C.; Lu, J.X.; Zeng, Q.; Zhao, W.; Li, W.Q.; Ling, J.Q. Comparison of mineral trioxide aggregate and calcium hydroxide for apexification of immature permanent teeth: A systematic review and meta-analysis. J. Formos. Med. Assoc. 2016, 115, 523–530. [Google Scholar] [CrossRef] [PubMed]
- Lee, L.W.; Hsieh, S.C.; Lin, Y.H.; Huang, C.F.; Hsiao, S.H.; Hung, W.C. Comparison of clinical outcomes for 40 necrotic immature permanent incisors treated with calcium hydroxide or mineral trioxide aggregate apexification/apexogenesis. J. Formos. Med. Assoc. 2015, 114, 139–146. [Google Scholar] [CrossRef] [PubMed]
- de Boer, I.R.; Lagerweij, M.D.; Wesselink, P.R.; Vervoorn, J.M. The effect of variations in force feedback in a virtual reality environment on the performance and satisfaction of dental students. Simul. Healthc. 2019, 14, 169–174. [Google Scholar] [CrossRef] [PubMed]
- Kenny, K.P.; Alkazme, A.M.; Day, P.F. The effect of viewing video clips of paediatric local anaesthetic administration on the confidence of undergraduate dental students. Eur. J. Dent. Educ. 2018, 22, e57–e62. [Google Scholar] [CrossRef] [PubMed]
- Gallardo, N.E.; Caleya, A.M.; Sánchez, M.E.; Feijóo, G. Learning of paediatric dentistry with the flipped classroom model. Eur. J. Dent. Educ. 2022, 26, 302–309. [Google Scholar] [CrossRef]
- Gallardo-López, N.E.; Sánchez-Sánchez, M.E.; Feijóo-Garcia, G.; Caleya, A.M. Edpuzzle versus Moodle: Learning tools in pediatric dentistry practice: A study pilot. Healthcare 2022, 10, 2548. [Google Scholar] [CrossRef]
- Lechermeier, J.; Fassnacht, M. How do performance feedback characteristics influence recipients’ reactions? A state-of-the-art review on feedback source, timing, and valence effects. Manag. Rev. Q. 2018, 68, 145–193. [Google Scholar] [CrossRef]
- Farra, S.L.; Gneuhs, M.; Hodgson, E.; Kawosa, B.; Miller, E.T.; Simon, A.; Timm, N.; Hausfeld, J. Comparative cost of virtual reality training and live exercises for training hospital workers for evacuation. Comput. Inform. Nurs. 2019, 37, 446–454. [Google Scholar] [CrossRef]
- Wang, D.; Li, T.; Zhang, Y.; Hou, J. Survey on multisensory feedback virtual reality dental training systems. Eur. J. Dent. Educ. 2016, 20, 248–260. [Google Scholar] [CrossRef] [PubMed]
- Koolivand, H.; Shooreshi, M.M.; Safari-Faramani, R.; Borji, M.; Mansoory, M.S.; Moradpoor, H.; Bahrami, M.; Azizi, S.M. Comparison of the effectiveness of virtual reality-based education and conventional teaching methods in dental education: A systematic review. BMC Med. Educ. 2024, 24, 8. [Google Scholar] [CrossRef] [PubMed]
- Liebermann, A.; Erdelt, K. Virtual education: Dental morphologies in a virtual teaching environment. J. Dent. Educ. 2020, 84, 1143–1150. [Google Scholar] [CrossRef] [PubMed]
- Nassar, H.M.; Tekian, A. Computer simulation and virtual reality in undergraduate operative and restorative dental education: A critical review. J. Dent. Educ. 2020, 84, 812–829. [Google Scholar] [CrossRef]
- Vincent, M.; Joseph, D.; Amory, C.; Paoli, N.; Ambrosini, P.; Mortier, É.; Tran, N. Contribution of Haptic Simulation to Analogic Training Environment in Restorative Dentistry. J. Dent. Educ. 2020, 84, 367–376. [Google Scholar] [CrossRef]
- Mon-Williams, M.A.; Mushtaq, F.; Wilkie, R.M.; Khambay, B.; Keeling, A.; Manogue, M. A three dimensional view of stereopsis in dentistry. Br. Dent. J. 2015, 219, 479–480. [Google Scholar] [CrossRef]
- Quinn, F.; Keogh, P.; McDonald, A.; Hussey, D. A study comparing the effectiveness of conventional training and virtual reality simulation in the skills acquisition of junior dental students. Eur. J. Dent. Educ. 2003, 7, 164–169. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| ST1 | Exp Group (n = 52) | Con Group (n = 47) | p-Value |
|---|---|---|---|
| Total points | 9.0 (9.0, 10.0) | 9.0 (9.0, 10.0) | 0.594 |
| Part A | 3.0 (3.0, 4.0) | 3.0 (3.0, 4.0) | 0.968 |
| Part B | 3.0 (3.0, 4.0) | 3.0 (2.0, 3.0) | 0.146 |
| Part C | 3.0 (2.0, 4.0) | 3.0 (3.0, 4.0) | 0.499 |
| ST2 | Exp Group (n = 52) | Con Group (n = 47) | p-Value |
|---|---|---|---|
| Total points | 11.0 (10.0, 11.0) | 10.0 (9.0, 11.0) | <0.001 *** |
| Part A | 3.5 (3.0, 4.0) | 4.0 (3.0, 4.0) | 0.470 |
| Part B | 4.0 (4.0, 4.0) | 3.0 (2.0, 3.0) | <0.001 *** |
| Part C | 4.0 (3.0, 4.0) | 4.0 (3.0, 4.0) | 0.802 |
| Variable | ST1 | ST2 | p-Value |
|---|---|---|---|
| Total points | 9.0 (9.0, 10.0) | 10.0 (9.0, 11.0) | 0.014 * |
| Part A | 3.0 (3.0, 4.0) | 4.0 (3.0, 4.0) | 0.440 |
| Part B | 3.0 (2.0, 3.0) | 3.0 (2.0, 3.0) | 0.393 |
| Part C | 3.0 (3.0, 4.0) | 4.0 (3.0, 4.0) | <0.001 *** |
| Variable | ST1 | ST2 | p-Value |
|---|---|---|---|
| Total points | 9.0 (9.0, 10.0) | 11.0 (10.0, 11.0) | <0.001 *** |
| Part A | 3.0 (3.0, 4.0) | 3.5 (3.0, 4.0) | 0.986 |
| Part B | 3.0 (3.0, 4.0) | 4.0 (4.0, 4.0) | <0.001 *** |
| Part C | 3.0 (2.0, 4.0) | 4.0 (3.0, 4.0) | <0.001 *** |
| Questions | Strongly Agree | Partially Agree | Disagree |
|---|---|---|---|
| I understand the apexification better with the help of the vs. learning platform. | 63.46% | 36.54% | 0% |
| I master the key points and difficulties of apexification technique better with the help of the vs. learning platform. | 63.46% | 34.62% | 1.92% |
| I have become familiar with the process of apexification with the help of the vs. learning platform. | 80.77% | 19.23% | 0% |
| The vs. learning platform enhanced my enthusiasm to study apexification. | 42.31% | 51.92% | 5.77% |
| The vs. learning platform is easy to operate. | 57.69% | 28.85% | 13.46% |
| I like the vs. learning platform very much. | 42.31% | 51.92% | 5.77% |
| The vs. learning platform is inconvenient and a waste of time. | 7.69% | 26.92% | 65.38% |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ma, L.; Lai, H.; Zhao, W. Evaluating the Effectiveness of a Virtual Simulation Platform for Apexification Learning. Dent. J. 2024, 12, 27. https://doi.org/10.3390/dj12020027
Ma L, Lai H, Zhao W. Evaluating the Effectiveness of a Virtual Simulation Platform for Apexification Learning. Dentistry Journal. 2024; 12(2):27. https://doi.org/10.3390/dj12020027
Chicago/Turabian StyleMa, Lan, Hongbin Lai, and Wei Zhao. 2024. "Evaluating the Effectiveness of a Virtual Simulation Platform for Apexification Learning" Dentistry Journal 12, no. 2: 27. https://doi.org/10.3390/dj12020027
APA StyleMa, L., Lai, H., & Zhao, W. (2024). Evaluating the Effectiveness of a Virtual Simulation Platform for Apexification Learning. Dentistry Journal, 12(2), 27. https://doi.org/10.3390/dj12020027