

Effects of Froggy Mouth Appliance in Pediatric Patients with Atypical Swallowing: A Prospective Study

 ,
,  , ,
, , 

Abstract
1. Introduction
2. Materials and Methods
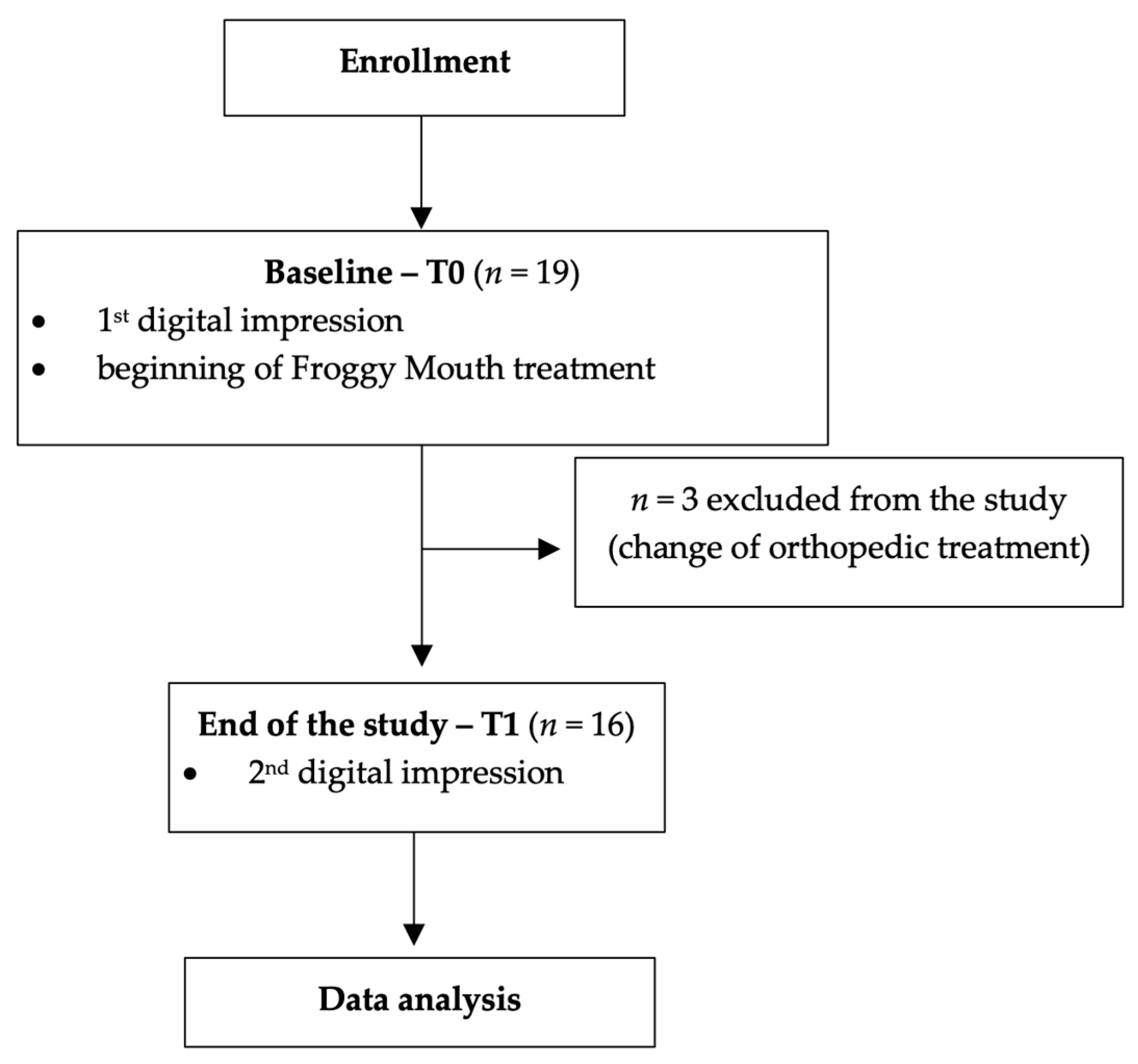
2.1. Study Design
2.2. Participants
- Age 5–12 years;
- No previous orthopedic and/or orthodontic treatment;
- No current orthodopedic and/or orthodontic treatment;
- Atypical swallowing diagnosed with lingual interposition between the dental arches during swallowing with contraction of the perioral muscles.
- Patients receiving speech therapy for atypical swallowing;
- Previous speech therapy for atypical swallowing.
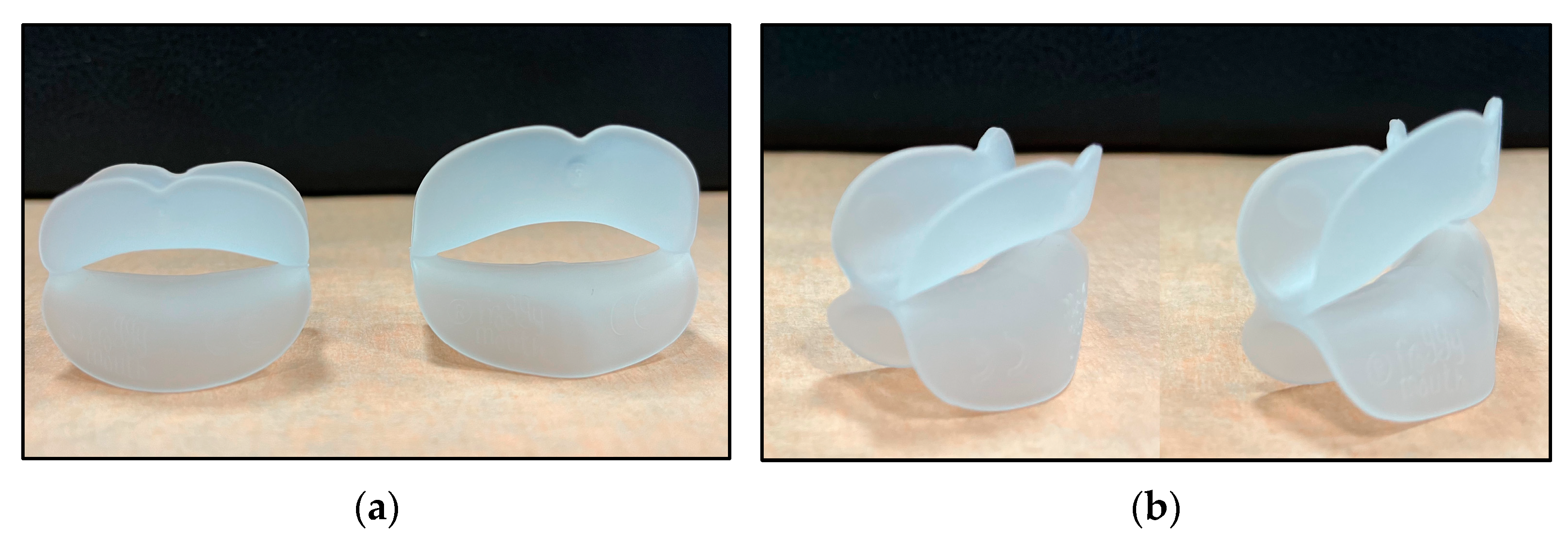
2.3. Interventions and Outcomes
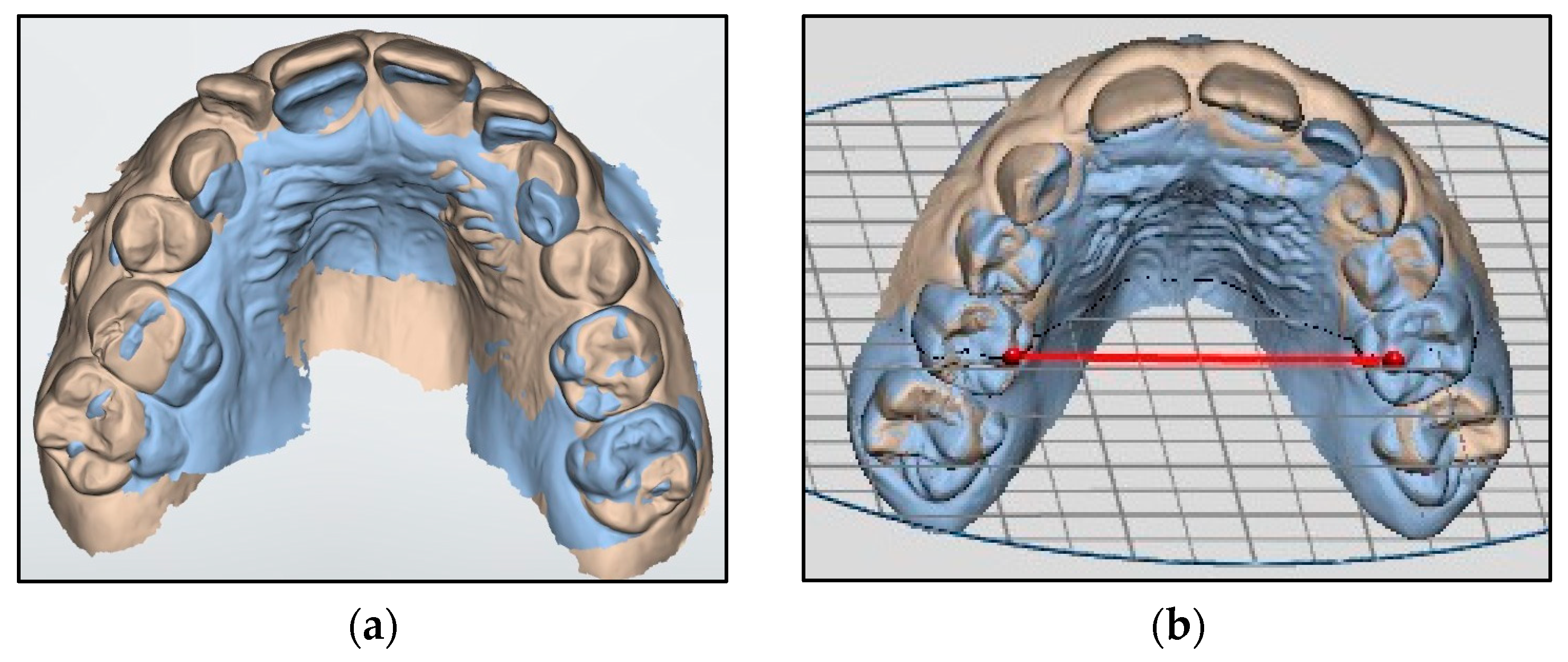
- Upper intercanine distance: distance between the edge of the cusps of the deciduous canines;
- Upper arch diameter (Figure 4a): distance between the mesio-palatal cusps of upper second deciduous molars;
- Upper arch width: distance between upper interincisal point and the point of intersection between the straight line passing from the furthest point from the crown of the second deciduous molars and the perpendicular line passing from the interincisal point;
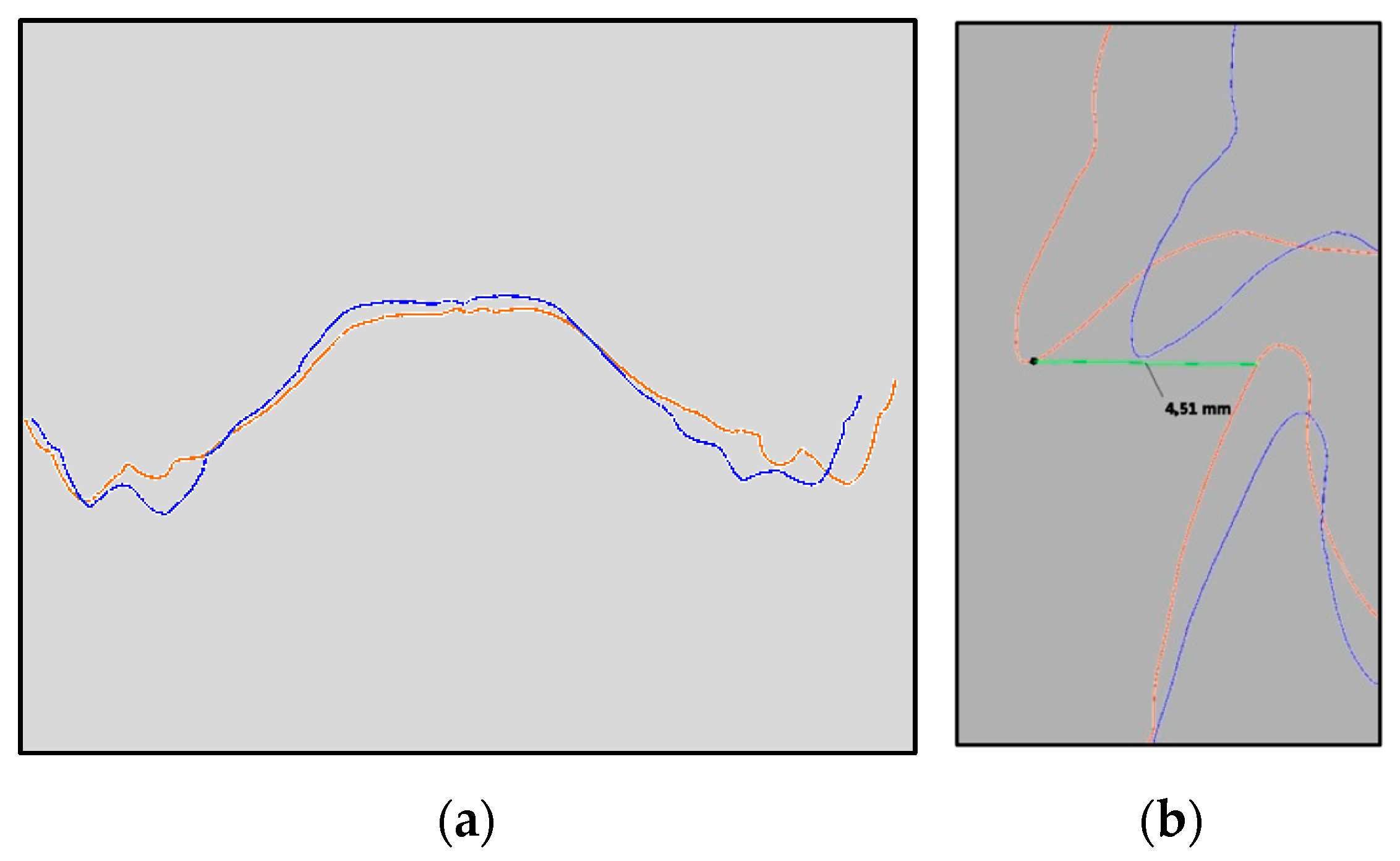
- Overbite: distance between the uppermost vertically erupted middle incisor and the corresponding incisal edge of the opposite mandibular tooth;
- Overjet (Figure 4b): distance between the most palatal point of the maxillary central incisors and the corresponding reference point on the vestibular surface of the mandibular incisor.
2.4. Sample Size
2.5. Statistical Analysis
3. Results
3.1. Demographic Data
3.2. Statistical Analysis Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Fellus, P. From digit-sucking-cum-deglutition to deglutition in dentate subjects. Orthod. Fr. 2016, 87, 89–90. [Google Scholar] [CrossRef] [PubMed]
- Fellus, P. Tongue disfunction and abnormal development. Orthod. Fr. 2006, 77, 105–112. [Google Scholar] [CrossRef]
- Begnoni, G.; Cadenas de Llano-Pérula, M.; Dellavia, C.; Willems, G. Cephalometric traits in children and adolescents with and without atypical swallowing: A retrospective study. Eur. J. Paediatr. Dent. 2020, 21, 46–52. [Google Scholar] [PubMed]
- Condò, R.; Costacurta, M.; Perugia, C.; Docimo, R. Atypical deglutition: Diagnosis and interceptive treatment. A clinical study. Eur. J. Paediatr. Dent. 2012, 13, 209–214. [Google Scholar] [PubMed]
- Maspero, C.; Prevedello, C.; Giannini, L.; Galbiati, G.; Farronato, G. Atypical swallowing: A review. Minerva Stomatol. 2014, 63, 217–227. [Google Scholar] [PubMed]
- Schmid, K.M.; Kugler, R.; Nalabothu, P.; Bosch, C.; Verna, C. The effect of pacifier sucking on orofacial structures: A systematic literature review. Prog. Orthod. 2018, 19, 8. [Google Scholar] [CrossRef] [PubMed]
- Caruso, S.; Nota, A.; Darvizeh, A.; Severino, M.; Gatto, R.; Tecco, S. Poor oral habits and malocclusions after usage of orthodontic pacifiers: An observational study on 3–5 years old children. BMC Pediatr. 2019, 19, 294. [Google Scholar] [CrossRef] [PubMed]
- Begnoni, G.; Dellavia, C.; Pellegrini, G.; Scarponi, L.; Schindler, A.; Pizzorni, N. The efficacy of myofunctional therapy in patients with atypical swallowing. Eur. Arch. Otorhinolaryngol. 2020, 277, 2501–2511. [Google Scholar] [CrossRef] [PubMed]
- Tecco, S.; Baldini, A.; Mummolo, S.; Marchetti, E.; Giuca, M.R.; Marzo, G.; Gherlone, E.F. Frenulectomy of the tongue and the influence of rehabilitation exercises on the sEMG activity of masticatory muscles. J. Electromyogr. Kinesiol. 2015, 25, 619–628. [Google Scholar] [CrossRef]
- Machado, A.J.; Crespo, A.N. Cephalometric evaluation of the airway space and hyoid bone in children with normal and atypical deglutition: Correlation study. Sao Paulo Med. J. 2012, 130, 236–241. [Google Scholar] [CrossRef]
- Martin-Harris, B. Clinical implications of respiratory-swallowing interactions. Curr. Opin. Otolaryngol. Head Neck Surg. 2008, 16, 194–199. [Google Scholar] [CrossRef]
- Hur, M.-S. Anatomical connections between the buccinator and the tendons of the temporalis. Ann. Anat. Anat. Anzeiger. 2017, 214, 63–66. [Google Scholar] [CrossRef] [PubMed]
- Jungbauer, R.; Koretsi, V.; Proff, P.; Rudzki, I.; Kirschneck, C. Twenty-year follow-up of functional treatment with a bionator appliance: A retrospective dental cast analysis. Angle Orthod. 2020, 90, 209–215. [Google Scholar] [CrossRef]
- Tecco, S.; Farronato, G.; Salini, V.; Di Meo, S.; Filippi, M.R.; Festa, F.; D’Attilio, M. Evaluation of cervical spine posture after functional therapy with FR-2: A longitudinal study. Cranio 2005, 23, 53–66. [Google Scholar] [CrossRef]
- Leite, J.S.; Matiussi, L.B.; Salem, A.C.; Provenzano, M.G.A.; Ramos, A.L. Effects of palatal crib and bonded spurs in early treatment of anterior open bite: A prospective randomized clinical study. Angle Orthod. 2016, 86, 734–739. [Google Scholar] [CrossRef] [PubMed]
- Giuca, M.R.; Pasini, M.; Pagano, A.; Mummolo, S.; Vanni, A. Longitudinal study on a rehabilitative model for correction of atypical swallowing. Eur. J. Paediatr. Dent. 2008, 9, 170–174. [Google Scholar]
- Bigenzahn, W.; Fischman, L.; Mayrhofer-Krammel, U. Myofunctional Therapy in Patients with Orofacial Dysfunctions Affecting Speech. Folia Phoniatr. Logop. 1992, 44, 238–244. [Google Scholar] [CrossRef] [PubMed]
- Di Vecchio, S.; Manzini, P.; Candida, E.; Gargari, M. Froggy mouth: A new myofunctional approach to atypical swallowing. Eur. J. Paediatr. Dent. 2019, 20, 33–37. [Google Scholar]
- Garg, H.; Khatria, H.; Kaldhari, K.; Singh, K.; Purwar, P.; Rukshana, R. Intermolar and Intercanine width Changes among Class I and Class II Malocclusions Following Orthodontic Treatment. Int. J. Clin. Pediatr. Dent. 2021, 14, S4–S9. [Google Scholar]
- Huo, B.; Che, X.; Li, X. Timing of early correction of mandibular hypoplasia in skeletal class II malocclusion: A review. J. Clin. Pediatr. Dent. 2023, 47, 11–20. [Google Scholar]
- Malmvind, D.; Golež, A.; Magnuson, A.; Ovsenik, M.; Bazargani, F. Three-dimensional assessment of palatal area changes after posterior crossbite correction with tooth-borne and tooth bone-borne rapid maxillary expansion. Angle Orthod. 2022, 92, 589–597. [Google Scholar] [CrossRef] [PubMed]
- Guinot, F.; Ferrer, M.; Díaz-González, L.; García, C.; Maura, I. Effects of Orthodontic Functional Appliances in Relation to Skeletal Maturation of Cervical Vertebrae In Class II Malocclusion. J. Clin. Pediatr. Dent. 2022, 46, 62–69. [Google Scholar] [CrossRef] [PubMed]
- Teixeira, E.C.; das Neves, B.M.; Castilho, T.; Silva Ramos, T.; Flaviana, A.; Carelli, J.; Kuchler, E.C.; Germano, F.N.; Alves Antunes, L.A.; Antunes, L.S. Evidence of Association between MTRR and TNF-α Gene Polymorphisms and Oral Health-Related Quality of Life in Children with Anterior Open Bite. J. Clin. Pediatr. Dent. 2022, 46, 249–258. [Google Scholar] [CrossRef] [PubMed]
- Proffit, W.R.; Fields, H.W., Jr.; Larson, B.E.; Sarver, D.M. Contemporary Orthodontics; Elsevier: Philadelphia, PA, USA, 2019; p. 130. [Google Scholar]
- Manzini, P.; Rosmarini, M.; Frati, E.; Severino, M.; Caruso, S. Tongue rehabilitation through the froggy mouth device: Case series. J. Biol. Regul. Homeost. Agents 2020, 34, 142–150. [Google Scholar] [PubMed]
- Quinzi, V.; Nota, A.; Caggiati, E.; Saccomanno, S.; Marzo, G.; Tecco, S. Short-Term Effects of a Myofunctional Appliance on Atypical Swallowing and Lip Strength: A Prospective Study. J. Clin. Med. 2020, 9, 2652. [Google Scholar] [CrossRef] [PubMed]
- Chen, J.; Xu, Y.; Guo, W. Combined orthopedic-orthodontic treatments of adolescent skeletal open-bite with severe molar-incisor hypomineralization: A case report and literature review. J. Clin. Pediatr. Dent. 2023, 47, 91–99. [Google Scholar]
- Cenzato, N.; Iannotti, L.; Maspero, C. Open bite and atypical swallowing: Orthodontic treatment, speech therapy or both? A literature review. Eur. J. Paediatr. Dent. 2021, 22, 286–290. [Google Scholar] [PubMed]
- Hoang, D.A.; Le, V.N.T.; Nguyen, T.M.; Jagomägi, T. Orofacial dysfunction screening examinations in children with sleep-disordered breathing symptoms. J. Clin. Pediatr. Dent. 2023, 47, 25–34. [Google Scholar]
- Sfondrini, M.F.; Pascadopoli, M.; Beccari, S.; Beccari, G.; Rizzi, C.; Gandini, P.; Scribante, A. Orthodontic Fixed Retainer and Unwanted Movements of Lower Anterior Teeth: A Case Report. Case Rep. Dent. 2022, 2022, 3100360. [Google Scholar]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Group | Time | Mean | SD | Min | Median | Max | SES | Significance |
|---|---|---|---|---|---|---|---|---|
| Upper intercanine distance | T0 | 31.86 | 2.54 | 27.60 | 32.25 | 36.18 | ||
| T1 | 32.78 | 2.19 | 27.70 | 32.83 | 35.66 | |||
| T1-T0 | 0.388 | 0.042 * | ||||||
| Upper arch diameter | T0 | 35.02 | 2.35 | 28.90 | 35.11 | 38.53 | ||
| T1 | 36.07 | 2.05 | 31.75 | 36.22 | 39.33 | |||
| T1-T0 | 0.476 | 0.016 * | ||||||
| Upper arch width | T0 | 30.25 | 3.62 | 24.62 | 29.27 | 40.00 | ||
| T1 | 31.96 | 3.35 | 28.04 | 31.58 | 42.00 | |||
| T1-T0 | 0.490 | 0.012 * | ||||||
| Overbite | T0 | 1.08 | 1.49 | −1.66 | 1.09 | 3.38 | ||
| T1 | 1.26 | 1.61 | −2.70 | 1.59 | 3.66 | |||
| T1-T0 | 0.116 | 0.433 | ||||||
| Overjet | T0 | 3.57 | 2.46 | −2.16 | 4.05 | 7.43 | ||
| T1 | 3.69 | 1.49 | 0.42 | 3.42 | 7.40 | |||
| T1-T0 | 0.048 | 0.769 |
| Variables | r |
|---|---|
| ∆ Upper intercanine distance~∆ Upper arch diameter | −0.0783 |
| ∆ Upper intercanine distance~∆ Upper arch width | 0.2382 |
| ∆ Upper arch diameter~∆ Upper arch width | −0.1578 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Scribante, A.; Pascadopoli, M.; Gallo, S.; Gandini, P.; Manzini, P.; Fadani, G.; Sfondrini, M.F. Effects of Froggy Mouth Appliance in Pediatric Patients with Atypical Swallowing: A Prospective Study. Dent. J. 2024, 12, 96. https://doi.org/10.3390/dj12040096
Scribante A, Pascadopoli M, Gallo S, Gandini P, Manzini P, Fadani G, Sfondrini MF. Effects of Froggy Mouth Appliance in Pediatric Patients with Atypical Swallowing: A Prospective Study. Dentistry Journal. 2024; 12(4):96. https://doi.org/10.3390/dj12040096
Chicago/Turabian StyleScribante, Andrea, Maurizio Pascadopoli, Simone Gallo, Paola Gandini, Pietro Manzini, Giulia Fadani, and Maria Francesca Sfondrini. 2024. "Effects of Froggy Mouth Appliance in Pediatric Patients with Atypical Swallowing: A Prospective Study" Dentistry Journal 12, no. 4: 96. https://doi.org/10.3390/dj12040096
APA StyleScribante, A., Pascadopoli, M., Gallo, S., Gandini, P., Manzini, P., Fadani, G., & Sfondrini, M. F. (2024). Effects of Froggy Mouth Appliance in Pediatric Patients with Atypical Swallowing: A Prospective Study. Dentistry Journal, 12(4), 96. https://doi.org/10.3390/dj12040096