
Clinical Effectiveness of Ion-Releasing Restorations versus Composite Restorations in Dental Restorations: Systematic Review and Meta-Analysis
 , , , , , and
, , , , , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Protocol
- -
- Population: Adults without systematic diseases who received dental restorations.
- -
- Intervention: Restoration with IRRs, which includes all GIC derivatives (RMGIC, HV–GIC, conventional and glass hybrid), polyacid-modified composites (compomer), giomer, and any material declared by the manufacturer to have the ability to release ions.
- -
- Comparison: Restoration with CR.
- -
- Outcomes: Secondary caries or erosion or abfraction, marginal discoloration, marginal adaptation, marginal or tooth integrity, color or translucency, surface texture or luster, surface staining, retention, wear, anatomical form, sensitivity, and state of periodontal tissues.
2.2. Focused Question (PICO)
2.3. Search and Selection of Studies
2.4. Data Extraction
2.5. Risk of Bias (RoB) Assessment
2.6. Analysis of Results
3. Results
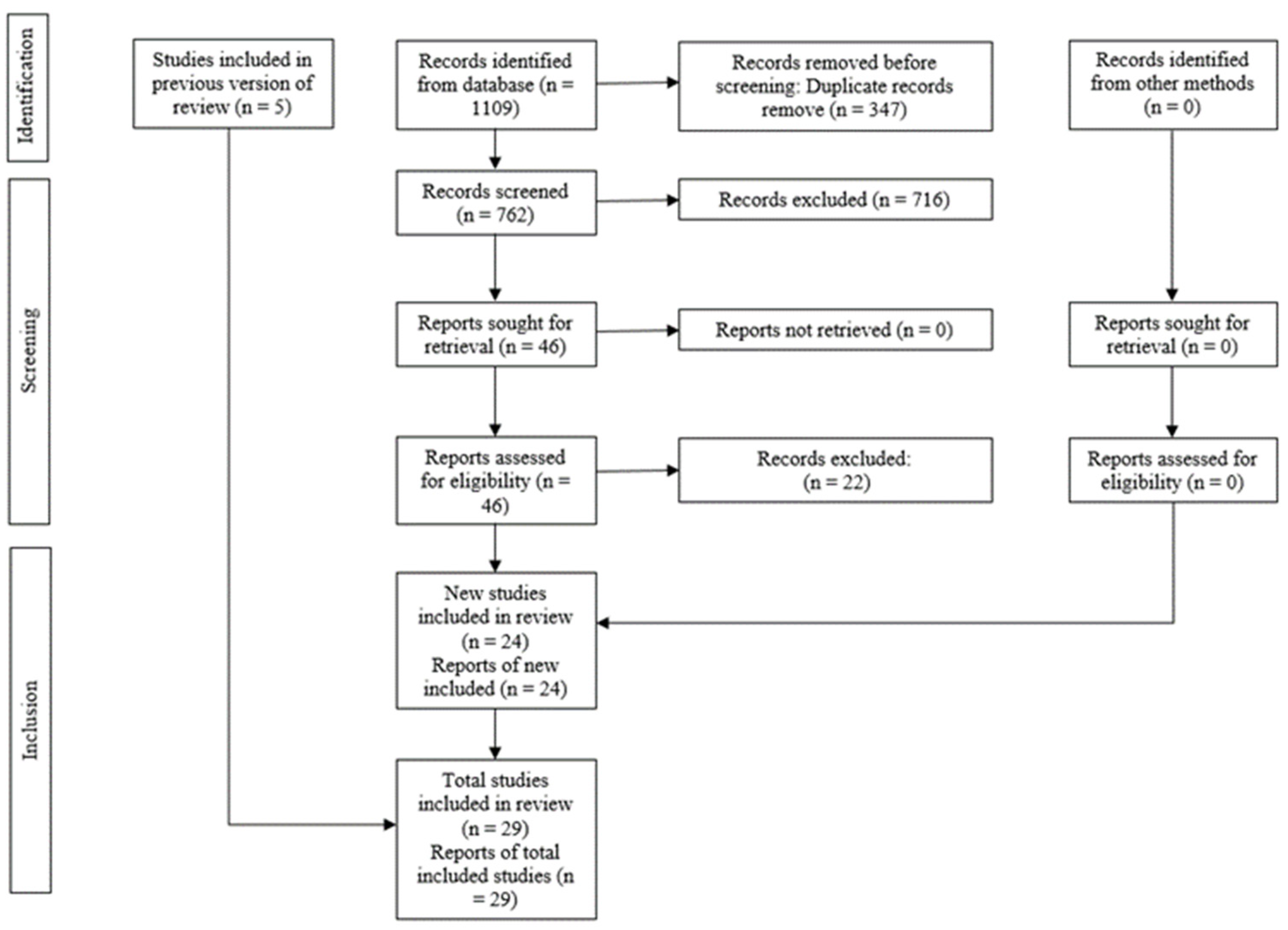
3.1. Selection of Studies
3.2. Characteristics of Included Studies
3.3. Risk of Bias Analysis of Studies
3.4. Synthesis of Results (Meta-Analysis)
3.5. Subgroup Synthesis
3.6. GRADE Analysis
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- Dobrzański, L.A.; Dobrzański, L.B.; Dobrzańska-Danikiewicz, A.D.; Dobrzańska, J. The Concept of Sustainable Development of Modern Dentistry. Processes 2020, 8, 1605. [Google Scholar] [CrossRef]
- Yadav, S.; Gangwar, S. A Critical Evaluation of Tribological Interaction for Restorative Materials in Dentistry. Int. J. Polym. Mater. Polym. Biomater. 2019, 68, 1005–1019. [Google Scholar] [CrossRef]
- Demarco, F.F.; Cenci, M.S.; Montagner, A.F.; de Lima, V.P.; Correa, M.B.; Moraes, R.R.; Opdam, N.J.M. Longevity of Composite Restorations Is Definitely Not Only about Materials. Dent. Mater. Off. Publ. Acad. Dent. Mater. 2023, 39, 1–12. [Google Scholar] [CrossRef] [PubMed]
- Kaur, G.; Kaushal, R.; Prabhakar, D. Esthetic Restorations and Smile Designing: A Review. Int. J. Health Sci. 2021, 5, 10–22. [Google Scholar] [CrossRef]
- Hatton, P.V.; Mulligan, S.; Martin, N. The Safety and Biocompatibility of Direct Aesthetic Restorative Materials. Br. Dent. J. 2022, 232, 611–614. [Google Scholar] [CrossRef] [PubMed]
- Tian, K.V.; Yang, B.; Yue, Y.; Bowron, D.T.; Mayers, J.; Donnan, R.S.; Dobó-Nagy, C.; Nicholson, J.W.; Fang, D.-C.; Greer, A.L.; et al. Atomic and Vibrational Origins of Mechanical Toughness in Bioactive Cement during Setting. Nat. Commun. 2015, 6, 8631. [Google Scholar] [CrossRef] [PubMed]
- Makanjuola, J.; Deb, S. Chemically Activated Glass-Ionomer Cements as Bioactive Materials in Dentistry: A Review. Prosthesis 2023, 5, 327–345. [Google Scholar] [CrossRef]
- Park, E.Y.; Kang, S. Current Aspects and Prospects of Glass Ionomer Cements for Clinical Dentistry. Yeungnam Univ. J. Med. 2020, 37, 169–178. [Google Scholar] [CrossRef] [PubMed]
- Saridena, U.S.N.G.; Sanka, G.S.S.J.; Alla, R.K.; Ramaraju, A.V.; Mc, S.S.; Mantena, S.R. An Overview of Advances in Glass Ionomer Cements. Int. J. Dent. Mater. 2022, 4, 89–94. [Google Scholar] [CrossRef]
- Kim, H.-J. Comparative Evaluation of Bond Strength and Microleakage of Three Ion-Releasing Restorative Materials at Various PH Levels. Appl. Sci. 2022, 12, 6796. [Google Scholar] [CrossRef]
- Sauro, S.; Makeeva, I.; Faus-Matoses, V.; Foschi, F.; Giovarruscio, M.; Maciel Pires, P.; Martins Moura, M.E.; Almeida Neves, A.; Faus-Llácer, V. Effects of Ions-Releasing Restorative Materials on the Dentine Bonding Longevity of Modern Universal Adhesives after Load-Cycle and Prolonged Artificial Saliva Aging. Materials 2019, 12, 722. [Google Scholar] [CrossRef] [PubMed]
- Aminoroaya, A.; Esmaeely Neisiany, R.; Nouri Khorasani, S.; Panahi, P.; Das, O.; Ramakrishna, S. A Review of Dental Composites: Methods of Characterizations. ACS Biomater. Sci. Eng. 2020, 6, 3713–3744. [Google Scholar] [CrossRef] [PubMed]
- Aminoroaya, A.; Neisiany, R.E.; Khorasani, S.N.; Panahi, P.; Das, O.; Madry, H.; Cucchiarini, M.; Ramakrishna, S. A Review of Dental Composites: Challenges, Chemistry Aspects, Filler Influences, and Future Insights. Compos. Part B Eng. 2021, 216, 108852. [Google Scholar] [CrossRef]
- Cho, K.; Rajan, G.; Farrar, P.; Prentice, L.; Prusty, B.G. Dental Resin Composites: A Review on Materials to Product Realizations. Compos. Part B Eng. 2022, 230, 109495. [Google Scholar] [CrossRef]
- Thalacker, C. Dental Adhesion with Resin Composites: A Review and Clinical Tips for Best Practice. Br. Dent. J. 2022, 232, 615–619. [Google Scholar] [CrossRef] [PubMed]
- Kumar, S.R.; Patnaik, A.; Bhat, I.K. Factors Influencing Mechanical and Wear Performance of Dental Composite: A Review. Mater. Werkst. 2020, 51, 96–108. [Google Scholar] [CrossRef]
- Simila, H.O.; Boccaccini, A.R. Sol-Gel Bioactive Glass Containing Biomaterials for Restorative Dentistry: A Review. Dent. Mater. Off. Publ. Acad. Dent. Mater. 2022, 38, 725–747. [Google Scholar] [CrossRef] [PubMed]
- Shearer, A.; Montazerian, M.; Sly, J.J.; Hill, R.G.; Mauro, J.C. Trends and Perspectives on the Commercialization of Bioactive Glasses. Acta Biomater. 2023, 160, 14–31. [Google Scholar] [CrossRef] [PubMed]
- Rokaya, D.; Srimaneepong, V.; Sapkota, J.; Qin, J.; Siraleartmukul, K.; Siriwongrungson, V. Polymeric Materials and Films in Dentistry: An Overview. J. Adv. Res. 2018, 14, 25–34. [Google Scholar] [CrossRef]
- Shamseer, L.; Moher, D.; Clarke, M.; Ghersi, D.; Liberati, A.; Petticrew, M.; Shekelle, P.; Stewart, L.A.; PRISMA-P Group. Preferred Reporting Items for Systematic Review and Meta-Analysis Protocols (PRISMA-P) 2015: Elaboration and Explanation. BMJ 2015, 350, g7647. [Google Scholar] [CrossRef]
- Booth, A.; Clarke, M.; Ghersi, D.; Moher, D.; Petticrew, M.; Stewart, L. An International Registry of Systematic-Review Protocols. Lancet Lond. Engl. 2011, 377, 108–109. [Google Scholar] [CrossRef] [PubMed]
- Gonçalves, R.S.; Scaffa, P.M.C.; Shinohara, M.S.; de Andrade Carvalho, P.R.M.; Buzalaf, M.A.R.; Fagundes, T.C. Two-Year Randomized Clinical Trial of Different Restorative Techniques in Non-Carious Cervical Lesions and MMP Activity in Gingival Crevicular Fluid. Clin. Oral Investig. 2022, 26, 1889–1902. [Google Scholar] [CrossRef] [PubMed]
- Shinohara, M.S.; Carvalho, P.R.M.d.A.; Neves Marcon, L.; Gonçalves, D.F.M.; Ramos, F.d.S.E.; Fagundes, T.C. Randomized Clinical Trial of Different Adhesion Strategies in Noncarious Cervical Lesion Restorations: 1-Year Follow-Up. Quintessence Int. Berl. Ger. 1985 2020, 51, 352–363. [Google Scholar] [CrossRef] [PubMed]
- Balkaya, H.; Arslan, S.; Pala, K. A Randomized, Prospective Clinical Study Evaluating Effectiveness of a Bulk-Fill Composite Resin, a Conventional Composite Resin and a Reinforced Glass Ionomer in Class II Cavities: One-Year Results. J. Appl. Oral Sci. 2019, 27, e20180678. [Google Scholar] [CrossRef] [PubMed]
- Çelik, E.U.; Tunac, A.T.; Yilmaz, F. A Randomized, Controlled, Split-Mouth Trial Evaluating the Clinical Performance of High-Viscosity Glass-Ionomer Restorations in Noncarious Cervical Lesions: Two-Year Results. J. Adhes. Dent. 2018, 20, 299–305. [Google Scholar] [PubMed]
- Brackett, M.G.; Dib, A.; Brackett, W.W.; Estrada, B.E.; Reyes, A.A. One-Year Clinical Performance of a Resin-Modified Glass Ionomer and a Resin Composite Restorative Material in Unprepared Class V Restorations. Oper. Dent. 2002, 27, 112–116. [Google Scholar] [PubMed]
- Folwaczny, M.; Loher, C.; Mehl, A.; Kunzelmann, K.H.; Hinkel, R. Tooth-Colored Filling Materials for the Restoration of Cervical Lesions: A 24-Month Follow-up Study. Oper. Dent. 2000, 25, 251–258. [Google Scholar]
- Koubi, S.; Raskin, A.; Bukiet, F.; Pignoly, C.; Toca, E.; Tassery, H. One-Year Clinical Evaluation of Two Resin Composites, Two Polymerization Methods, and a Resin-Modified Glass Lonomer in Non-Carious Cervical Lesions. J. Contemp. Dent. Pract. 2006, 7, 042–053. [Google Scholar]
- Gallo, J.R.; Burgess, J.O.; Ripps, A.H.; Walker, R.S.; Ireland, E.J.; Mercante, D.E.; Davidson, J.M. Three-Year Clinical Evaluation of a Compomer and a Resin Composite as Class V Filling Materials. Oper. Dent. 2005, 30, 275–281. [Google Scholar]
- Wucher, M.; Grobler, S.R.; Senekal, P.J.C. A 3-Year Clinical Evaluation of a Compomer, a Composite and a Compomer/Composite (Sandwich) in Class II Restorations. Am. J. Dent. 2002, 15, 274–278. [Google Scholar]
- Powell, L.V.; Johnson, G.H.; Gordon, G.E. Factors Associated with Clinical Success of Cervical Abrasion/Erosion Restorations. Oper. Dent. 1995, 20, 7–13. [Google Scholar] [PubMed]
- Smales, R.J.; Gerke, D.C.; White, I.L. Clinical Evaluation of Occlusal Glass Ionomer, Resin, and Amalgam Restorations. J. Dent. 1990, 18, 243–249. [Google Scholar] [CrossRef] [PubMed]
- Burgess, J.O.; Gallo, J.R.; Ripps, A.H.; Walker, R.S.; Ireland, E.J. Clinical Evaluation of Four Class 5 Restorative Materials: 3-Year Recall. Am. J. Dent. 2004, 17, 147–150. [Google Scholar] [PubMed]
- Neo, J.; Chew, C.L. Direct Tooth-Colored Materials for Noncarious Lesions: A 3-Year Clinical Report. Quintessence Int. Berl. Ger. 1985 1996, 27, 183–188. [Google Scholar]
- van Dijken, J.W. 3-Year Clinical Evaluation of a Compomer, a Resin-Modified Glass Ionomer and a Resin Composite in Class III Restorations. Am. J. Dent. 1996, 9, 195–198. [Google Scholar] [PubMed]
- Wilkie, R.; Lidums, A.; Smales, R. Class II Glass Ionomer Cermet Tunnel, Resin Sandwich and Amalgam Restorations over 2 Years. Am. J. Dent. 1993, 6, 181–184. [Google Scholar] [PubMed]
- Lidums, A.; Wilkie, R.; Smales, R. Occlusal Glass Ionomer Cermet, Resin Sandwich and Amalgam Restorations: A 2-Year Clinical Study. Am. J. Dent. 1993, 6, 185–188. [Google Scholar] [PubMed]
- Kaurich, M.; Kawakami, K.; Perez, P.; Munn, T.; Hasse, A.L.; Garrett, N.R. A Clinical Comparison of a Glass Ionomer Cement and a Microfilled Composite Resin in Restoring Root Caries: Two-Year Results. Gen. Dent. 1991, 39, 346–349. [Google Scholar] [PubMed]
- Osborne, J.W.; Berry, T.G. 3-Year Clinical Evaluation of Glass Ionomer Cements as Class III Restorations. Am. J. Dent. 1990, 3, 40–43. [Google Scholar]
- Gupta, R.; Patel, A.; Pradnya, N.; Manoj, C.; Rutuja, R.; Meghna, D. Comparative Evaluation of Postoperative Sensitivity Using Three Different Tooth-Colored Restorative Materials in Non-Carious Cervical Lesions: A Split-Mouth Design In Vivo Study. Cureus 2022, 14, e27861. [Google Scholar] [CrossRef]
- Isler, S.C.; Ozcan, G.; Ozcan, M.; Omurlu, H. Clinical Evaluation of Combined Surgical/ Restorative Treatment of Gingival Recession-Type Defects Using Different Restorative Materials: A Randomized Clinical Trial. J. Dent. Sci. 2018, 13, 20–29. [Google Scholar] [CrossRef]
- Van Dijken, J.W.V.; Pallesen, U. A 7-Year Randomized Prospective Study of a One-Step Self-Etching Adhesive in Non-Carious Cervical Lesions. the Effect of Curing Modes and Restorative Material. J. Dent. 2012, 40, 1060–1067. [Google Scholar] [CrossRef]
- Burrow, M.F.; Tyas, M.J. Clinical Evaluation of Three Adhesive Systems for the Restoration of Non-Carious Cervical Lesions. Oper. Dent. 2007, 32, 11–15. [Google Scholar] [CrossRef]
- Albelasy, E.H.; Hamama, H.H.; Chew, H.P.; Montasser, M.; Mahmoud, S.H. Clinical Performance of Two Ion-Releasing Bulk-Fill Composites in Class I and Class II Restorations: A Two-Year Evaluation. J. Esthet. Restor. Dent. Off. Publ. Am. Acad. Esthet. Dent. Al 2024, 36, 723–736. [Google Scholar] [CrossRef]
- Ballal, N.V.; Jalan, P.; Rai, N.; Al-Haj Husain, N.; Özcan, M. Evaluation of New Alkasite Based Restorative Material for Restoring Non- Carious Cervical Lesions- Randomized Controlled Clinical Trial. Eur. J. Prosthodont. Restor. Dent. 2023, 31, 72–77. [Google Scholar] [CrossRef]
- Saghir, A.; Rehman, T.; Irum, B.; Afreen, Z.; Khan, F.N. 12 Month’s Assessment of Clinical Efficacy of Resin Modified Glass Ionomer Cement and Flowable Composites in Restoration of Non-Carious Cervical Lesions, A Randomized Clinical Trial. J. Ayub Med. Coll. Abbottabad-Pak. 2023, 35, 7–10. [Google Scholar] [CrossRef] [PubMed]
- Wafaie, R.A.; Ibrahim Ali, A.; El-Negoly, S.A.E.-R.; Mahmoud, S.H. Five-Year Randomized Clinical Trial to Evaluate the Clinical Performance of High-Viscosity Glass Ionomer Restorative Systems in Small Class II Restorations. J. Esthet. Restor. Dent. 2023, 35, 538–555. [Google Scholar] [CrossRef]
- Toz-Akalin, T.; Öztürk-Bozkurt, F.; Kusdemir, M.; Özsoy, A.; Yüzbaşıoğlu, E.; Özcan, M. Clinical Evaluation of Low-Shrinkage Bioactive Material Giomer Versus Nanohybrid Resin Composite Restorations: A Two-Year Prospective Controlled Clinical Trial. Oper. Dent. 2023, 48, 10–20. [Google Scholar] [CrossRef] [PubMed]
- Gonçalves, D.F.M.; Shinohara, M.S.; Carvalho, P.R.M.d.A.; Ramos, F.d.S.E.S.; Oliveira, L.d.C.; Omoto, É.M.; Fagundes, T.C. Three-Year Evaluation of Different Adhesion Strategies in Non-Carious Cervical Lesion Restorations: A Randomized Clinical Trial. J. Appl. Oral Sci. Rev. FOB 2021, 29, e20210192. [Google Scholar] [CrossRef] [PubMed]
- Schwendicke, F.; Müller, A.; Seifert, T.; Jeggle-Engbert, L.-M.; Paris, S.; Göstemeyer, G. Glass Hybrid versus Composite for Non-Carious Cervical Lesions: Survival, Restoration Quality and Costs in Randomized Controlled Trial after 3 Years. J. Dent. 2021, 110, 103689. [Google Scholar] [CrossRef] [PubMed]
- Koc Vural, U.; Kerimova, L.; Kiremitci, A. Clinical Comparison of a Micro-Hybride Resin-Based Composite and Resin Modified Glass Ionomer in the Treatment of Cervical Caries Lesions: 36-Month, Split-Mouth, Randomized Clinical Trial. Odontology 2021, 109, 376–384. [Google Scholar] [CrossRef]
- Balkaya, H.; Arslan, S. A Two-Year Clinical Comparison of Three Different Restorative Materials in Class II Cavities. Oper. Dent. 2020, 45, E32–E42. [Google Scholar] [CrossRef]
- Miletić, I.; Baraba, A.; Basso, M.; Pulcini, M.G.; Marković, D.; Perić, T.; Ozkaya, C.A.; Turkun, L.S. Clinical Performance of a Glass-Hybrid System Compared with a Resin Composite in the Posterior Region: Results of a 2-Year Multicenter Study. J. Adhes. Dent. 2020, 22, 235–247. [Google Scholar] [CrossRef]
- Celik, E.U.; Tunac, A.T.; Yilmaz, F. Three-Year Clinical Evaluation of High-Viscosity Glass Ionomer Restorations in Non-Carious Cervical Lesions: A Randomised Controlled Split-Mouth Clinical Trial. Clin. Oral Investig. 2019, 23, 1473–1480. [Google Scholar] [CrossRef]
- van Dijken, J.W.V.; Pallesen, U.; Benetti, A. A Randomized Controlled Evaluation of Posterior Resin Restorations of an Altered Resin Modified Glass-Ionomer Cement with Claimed Bioactivity. Dent. Mater. Off. Publ. Acad. Dent. Mater. 2019, 35, 335–343. [Google Scholar] [CrossRef]
- Jassal, M.; Mittal, S.; Tewari, S. Clinical Effectiveness of a Resin-Modified Glass Ionomer Cement and a Mild One-Step Self-Etch Adhesive Applied Actively and Passively in Noncarious Cervical Lesions: An 18-Month Clinical Trial. Oper. Dent. 2018, 43, 581–592. [Google Scholar] [CrossRef]
- Hussainy, S.N.; Nasim, I.; Thomas, T.; Ranjan, M. Clinical Performance of Resin-Modified Glass Ionomer Cement, Flowable Composite, and Polyacid-Modified Resin Composite in Noncarious Cervical Lesions: One-Year Follow-Up. J. Conserv. Dent. JCD 2018, 21, 510–515. [Google Scholar] [CrossRef]
- Popescu, S.M.; Ţuculină, M.J.; Manolea, H.O.; Mercuţ, R.; Scrieciu, M. Randomized Clinical Trial of Adhesive Restorations in Non Carious Cervical Lesions. Key Eng. Mater. 2016, 695, 3–11. [Google Scholar] [CrossRef]
- Fagundes, T.C.; Barata, T.J.E.; Bresciani, E.; Santiago, S.; Franco, E.B.; Lauris, J.R.P.; Navarro, M.F. Seven-Year Clinical Performance of Resin Composite versus Resin-Modified Glass Ionomer Restorations in Noncarious Cervical Lesions. Oper. Dent. 2014, 39, 578–587. [Google Scholar] [CrossRef] [PubMed]
- de Oliveira, F.G.; Machado, L.S.; Rocha, E.P.; de Alexandre, R.S.; Fraga Briso, A.L.; Mazza Sundefeld, M.L.M.; Sundfeld, R.H. Clinical Evaluation of a Composite Resin and a Resin-Modified Glass-Ionomer Cement in Non-Carious Cervical Lesions: One-Year Results. Int. J. Clin. Dent. 2012, 5, 155–166. [Google Scholar]
- Perdigão, J.; Dutra-Corrêa, M.; Saraceni, S.; Ciaramicoli, M.; Kiyan, V. Randomized Clinical Trial of Two Resin-Modified Glass Ionomer Materials: 1-Year Results. Oper. Dent. 2012, 37, 591–601. [Google Scholar] [CrossRef] [PubMed]
- Adeleke, A.; Oginni, A. Clinical Evaluation of Resin Composite and Resin-Modified Glass Ionomer Cement in Non-Carious Cervical Lesions. J. West Afr. Coll. Surg. 2012, 2, 21–37. [Google Scholar] [PubMed]
- Santiago, S.L.; Passos, V.F.; Vieira, A.H.M.; Navarro, M.F.d.L.; Lauris, J.R.P.; Franco, E.B. Two-Year Clinical Evaluation of Resinous Restorative Systems in Non-Carious Cervical Lesions. Braz. Dent. J. 2010, 21, 229–234. [Google Scholar] [CrossRef] [PubMed]
- Türkün, L.; Uzer Çelik, E. Noncarious Class V Lesions Restored with a Polyacid Modified Resin Composite and a Nanocomposite: A Two-Year Clinical Trial. J. Adhes. Dent. 2008, 10, 399–405. [Google Scholar] [PubMed]
- Pollington, S.; van Noort, R. A Clinical Evaluation of a Resin Composite and a Compomer in Non-Carious Class V Lesions. A 3-Year Follow-Up. Am. J. Dent. 2008, 21, 49–52. [Google Scholar] [PubMed]
- Franco, E.B.; Benetti, A.R.; Ishikiriama, S.K.; Santiago, S.L.; Lauris, J.R.P.; Jorge, M.F.F.; Navarro, M.F. de L. 5-Year Clinical Performance of Resin Composite versus Resin Modified Glass Ionomer Restorative System in Non-Carious Cervical Lesions. Oper. Dent. 2006, 31, 403–408. [Google Scholar] [CrossRef] [PubMed]
- Onal, B.; Pamir, T. The Two-Year Clinical Performance of Esthetic Restorative Materials in Noncarious Cervical Lesions. J. Am. Dent. Assoc. 1939 2005, 136, 1547–1555. [Google Scholar] [CrossRef] [PubMed]
- Brackett, W.W.; Dib, A.; Brackett, M.G.; Reyes, A.A.; Estrada, B.E. Two-Year Clinical Performance of Class V Resin-Modified Glass-Lonomer and Resin Composite Restorations. Oper. Dent. 2003, 28, 477–481. [Google Scholar] [PubMed]
- Ozgünaltay, G.; Onen, A. Three-Year Clinical Evaluation of a Resin Modified Glass-Ionomer Cement and a Composite Resin in Non-Carious Class V Lesions. J. Oral Rehabil. 2002, 29, 1037–1041. [Google Scholar] [CrossRef]
- Folwaczny, M.; Loher, C.; Mehl, A.; Kunzelmann, K.H.; Hickel, R. Class V Lesions Restored with Four Different Tooth-Colored Materials--3-Year Results. Clin. Oral Investig. 2001, 5, 31–39. [Google Scholar] [CrossRef]
- Federlin, M.; Thonemann, B.; Schmalz, G.; Urlinger, T. Clinical Evaluation of Different Adhesive Systems for Restoring Teeth with Erosion Lesions. Clin. Oral Investig. 1998, 2, 58–66. [Google Scholar] [CrossRef] [PubMed]
- Matis, B.A.; Cochran, M.; Carlson, T. Longevity of Glass-Ionomer Restorative Materials: Results of a 10-Year Evaluation. Quintessence Int. 1996, 27, 373–382. [Google Scholar] [PubMed]
- Balhaddad, A.A.; Kansara, A.A.; Hidan, D.; Weir, M.D.; Xu, H.H.K.; Melo, M.A.S. Toward Dental Caries: Exploring Nanoparticle-Based Platforms and Calcium Phosphate Compounds for Dental Restorative Materials. Bioact. Mater. 2019, 4, 43–55. [Google Scholar] [CrossRef] [PubMed]
- Pinto, N.S.; Jorge, G.R.; Vasconcelos, J.; Probst, L.F.; De-Carli, A.D.; Freire, A. Clinical Efficacy of Bioactive Restorative Materials in Controlling Secondary Caries: A Systematic Review and Network Meta-Analysis. BMC Oral Health 2023, 23, 394. [Google Scholar] [CrossRef] [PubMed]
- Albelasy, E.H.; Hamama, H.H.; Chew, H.P.; Montaser, M.; Mahmoud, S.H. Secondary Caries and Marginal Adaptation of Ion-Releasing versus Resin Composite Restorations: A Systematic Review and Meta-Analysis of Randomized Clinical Trials. Sci. Rep. 2022, 12, 19244. [Google Scholar] [CrossRef] [PubMed]
- Nedeljkovic, I.; De Munck, J.; Vanloy, A.; Declerck, D.; Lambrechts, P.; Peumans, M.; Teughels, W.; Van Meerbeek, B.; Van Landuyt, K.L. Secondary Caries: Prevalence, Characteristics, and Approach. Clin. Oral Investig. 2020, 24, 683–691. [Google Scholar] [CrossRef] [PubMed]
- Bezerra, I.M.; Brito, A.C.M.; de Sousa, S.A.; Santiago, B.M.; Cavalcanti, Y.W.; de Almeida, L.D.F.D. Glass Ionomer Cements Compared with Composite Resin in Restoration of Noncarious Cervical Lesions: A Systematic Review and Meta-Analysis. Heliyon 2020, 6, e03969. [Google Scholar] [CrossRef] [PubMed]
- Ge, K.; Quock, R.; Chu, C.; Yu, O. The Preventive Effect of Glass Ionomer Cement Restorations on Secondary Caries Formation: A Systematic Review and Meta-Analysis. Dent. Mater. 2023, 39, e1–e17. [Google Scholar] [CrossRef] [PubMed]
- Kharma, K.; Zogheib, T.; Mehanna, C. Clinical Evaluation of Microhybrid Composite and Glass Ionomer Restorative Material in Permanent Teeth. J. Contemp. Dent. Pract. 2013, 19, 226–232. [Google Scholar] [CrossRef]
- Oz, F.D.; Meral, E.; Ergin, E.; Gurgan, S. One-Year Evaluation of a New Restorative Glass Ionomer Cement for the Restoration of Non-Carious Cervical Lesions in Patients with Systemic Diseases: A Randomized, Clinical Trial. J. Appl. Oral Sci. 2020, 28, e20200311. [Google Scholar] [CrossRef]
- Aydın, N.; Topçu, F.-T.; Karaoğlanoğlu, S.; Oktay, E.-A.; Erdemir, U. Effect of Finishing and Polishing Systems on the Surface Roughness and Color Change of Composite Resins. J. Clin. Exp. Dent. 2021, 13, e446–e454. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
| Database | Search Strategy | Number of Study |
|---|---|---|
| Pubmed | ((“ion releasing”) OR (“bioactive resin composite”) OR (“glass ionomer cement”) OR (“high viscosity glass ionomer”) OR (“resin modified glass ionomer”) OR (“glass hybrid”) OR (“polyacid-modified composite”) OR (“compomer”)) AND ((“resin composite”) OR (“composite resin”)) AND ((“randomized clinical trial”) OR (“clinical trial”)) | 174 |
| Cochrane Library | #1 MeSH descriptor: [Glass Ionomer Cements] explode all trees #2 MeSH descriptor: [Compomers] explode all trees #3 (“ion releasing”) OR (“bioactive resin composite”) OR (“glass ionomer cement”) OR (“high viscosity glass ionomer”) OR (“resin modified glass ionomer”) OR (“glass hybrid”) OR (“polyacid-modified composite”) OR (“compomer”) (Word variations have been searched) #4 #1 OR #2 OR #3 #5 MeSH descriptor: [Composite Resins] explode all trees #6 (“Composite resin”) OR (“Resin composite”) (Word variations have been searched) #7 #5 OR #6 #8 MeSH descriptor: [Clinical Trial] explode all trees #9 (“randomized clinical trial”) OR (“clinical trial”) (Word variations have been searched) #10 #8 OR #9 #11 #4 AND #7 AND #10 | 183 |
| Scielo | ((“ion releasing”) OR (“bioactive resin composite”) OR (“glass ionomer cement”) OR (“high viscosity glass ionomer”) OR (“resin modified glass ionomer”) OR (“glass hybrid”) OR (“polyacid-modified composite”) OR (“compomer”)) AND ((“resin composite”) OR (“composite resin”)) AND ((“randomized clinical trial”) OR (“clinical trial”)) | 3 |
| Scopus | (TITLE-ABS-KEY ((“ion releasing”) OR (“bioactive resin composite”) OR (“glass ionomer cement”) OR (“high-viscosity glass ionomer”) OR (“resin-modified glass ionomer”) OR (“glass hybrid”) OR (“polyacid-modified composite”) OR (“compomer”)) AND TITLE-ABS-KEY (((“resin composite”) OR (“composite resin”))) AND TITLE-ABS-KEY ((“randomized clinical trial”) OR (“clinical trial”))) AND (LIMIT-TO (DOCTYPE, “ar”)) | 494 |
| Web of Science | (TS = (“ion releasing”) OR TS = (“bioactive resin composite”) OR TS = (“glass ionomer cement”) OR TS = (“high viscosity glass ionomer”) OR TS = (“resin modified glass ionomer”) OR TS = (“glass hybrid”) OR TS = (“polyacid-modified composite”) OR TS = (“compomer”)) AND (TS = (“resin composite”) OR TS = (“composite resin”)) AND (TS = (“randomized clinical trial”) OR TS = (“clinical trial”)) | 80 |
| Google Scholar | allintitle: “ion releasing” OR “bioactive resin composite” OR “glass ionomer cement” OR “high viscosity glass ionomer” OR “resin modified glass ionomer” OR “glass hybrid” OR “polyacid modified composite” OR “compomer” OR “resin composite” OR “composite resin” “clinical trial”-“systematic review”-“in vitro”-“review” | 156 |
| Open Gray | ((“ion releasing”) OR (“bioactive resin composite”) OR (“glass ionomer cement”) OR (“high viscosity glass ionomer”) OR (“resin modified glass ionomer”) OR (“glass hybrid”) OR (“polyacid-modified composite”) OR (“compomer”)) AND ((“resin composite”) OR (“composite resin”)) AND ((“randomized clinical trial”) OR (“clinical trial”)) | 0 |
| Proquest | (“ion releasing” OR “bioactive resin composite” OR “glass ionomer cement” OR “high viscosity glass ionomer” OR “resin modified glass ionomer” OR “glass hybrid” OR “polyacid-modified composite” OR “compomer”) AND (“resin composite” OR “composite resin”) AND (“randomized clinical trial” OR “clinical trial”) NOT (“systematic review” OR “in vitro” OR “review”) | 19 |
| Author | Reason for Exclusion |
|---|---|
| Gonçalves et al. [22] | Study with data reported in another publication with different follow-up period |
| Shinohara et al. [23] | |
| Balkaya et al. [24] | |
| Çelik et al. [25] | |
| Brackett et al. [26] | |
| Folwaczny et al. [27] | |
| Koubi et al. [28] | Non-randomized clinical trials |
| Gallo et al. [29] | |
| Wucher et al. [30] | |
| Powell et al. [31] | |
| Smales et al. [32] | |
| Burgess et al. [33] | The full text was not found |
| Neo et al. [34] | |
| van Dijken et al. [35] | |
| Wilkie et al. [36] | |
| Lidums et al. [37] | |
| Kaurich et al. [38] | |
| Osborne et al. [39] | |
| Gupta et al. [40] | Studies with different evaluation criteria |
| Isler et al. [41] | |
| van Dijken et al. [42] | |
| Burrow et al. [43] |
| Authors | Year | Study Design | Country | Number of Patients (Male/Female) | Average Age (Range) | Follow-Up | Evaluation Criteria | Groups | Number of Patients per Group | Number of Teeth per Group | Class (Black) |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Albelasy et al. [44] | 2024 | RCT cross-over | Egypt | 32 (10/22) | 29.4 ± 8 (>18) | 2 years | FDI | IRC | 32 | 32 | I and II |
| IRC | 32 | 32 | |||||||||
| CR | 32 | 32 | |||||||||
| Ballal et al. [45] | 2023 | RCT cross-over | India | 40 | (18–60) | 1 year | USPHS | RMGIC | 40 | 40 | V |
| CR | 40 | 40 | |||||||||
| Saghir et al. [46] | 2023 | RCT cross-over | Pakistan | 30 | (30–60) | 1 year | USPHS | RMGIC | 30 | 30 | V |
| FCR | 30 | 30 | |||||||||
| Wafaie et al. [47] | 2023 | RCT cross-over | Egypt | 40 (26/14) | 25 (20–40) | 5 years | FDI | HVGIC | 40 | 40 | II |
| HVGIC | 40 | 40 | |||||||||
| HVGIC | 40 | 40 | |||||||||
| CR | 40 | 40 | |||||||||
| Toz-Akalin et al. [48] | 2023 | RCT cross-over | Turkey | 35 (18/17) | 29 ± 9 (18–47) | 2 years | FDI | G | 35 | 35 | I and II |
| CR | 35 | 35 | |||||||||
| Gonçalves et al. [49] | 2021 | RCT cross-over | Brazil | 50 (34/16) | 61 (38–92) | 3 years | USPHS | RMGIC | 50 | 50 | V |
| RMGIC + EDTA | 50 | 50 | |||||||||
| CR | 50 | 50 | |||||||||
| CR + SE | 50 | 50 | |||||||||
| Schwendicke et al. [50] | 2021 | RCT parallel | Germany | 88 (45/43) | 62.2 ± 5.7 (50–70) | 3 years | FDI | HVGIC | 43 | 81 | V |
| CR | 45 | 88 | |||||||||
| Koc Vural et al. [51] | 2021 | RCT cross-over | Turkey | 33 (10/23) | 52.69 ± 9.7 (37–89) | 3 years | USPHS | RMGIC | 33 | 55 | V |
| CR | 33 | 55 | |||||||||
| Balkaya et al. [52] | 2020 | RCT cross-over | Turkey | 54 (23/31) | 22 (20–32) | 2 years | USPHS | HVGIC | 54 | 34 | II |
| CR | 54 | 37 | |||||||||
| CR | 54 | 38 | |||||||||
| Miletić et al. [53] | 2020 | RCT cross-over | Croatia, Italy, Turkey and Serbia | 180 (64/116) | (>18) | 2 years | FDI | GH | 180 | 180 | II |
| CR | 180 | 180 | |||||||||
| Celik et al. [54] | 2019 | RCT cross-over | Turkey | 22 (11/11) | 47.8 (34–63) | 3 years | FDI | HVGIC | 22 | 67 | V |
| CR | 22 | 67 | |||||||||
| van Dijken et al. [55] | 2019 | RCT cross-over | Sweeden | 67 (38/29) | 58.3 (37–86) | 1 year | USPHS | RMGIC | 67 | 82 | I and II |
| CR | 67 | 82 | |||||||||
| Jassal et al. [56] | 2018 | RCT cross-over | India | 56 (44/12) | 54 (>18) | 1.5 years | FDI | RMGIC | 56 | 98 | V |
| CR + P-SEA | 56 | 98 | |||||||||
| CR + A-SEA | 56 | 98 | |||||||||
| Hussainy et al. [57] | 2018 | RCT cross-over | India | NR | (18–65) | 1 year | USPHS | RMGIC | NR | 33 | V |
| PMRC | NR | 34 | |||||||||
| CR | NR | 34 | |||||||||
| Popescu et al. [58] | 2016 | RCT cross-over | Romania | 45 | (25–65) | 2 years | USPHS | RMGIC | 45 | 73 | V |
| CR | 45 | 74 | |||||||||
| RMGIC + CR | 45 | 73 | |||||||||
| Fagundes et al. [59] | 2014 | RCT cross-over | Brazil | 30 | (18–50) | 7 years | USPHS | RMGIC | 30 | 35 | V |
| CR | 30 | 35 | |||||||||
| de Oliveira et al. [60] | 2012 | RCT cross-over | Brazil | 10 (3/7) | (36–55) | 1 year | USPHS | RMGIC | 10 | 40 | V |
| RMGIC + AS | 10 | 43 | |||||||||
| CR | 10 | 41 | |||||||||
| Perdigão et al. [61] | 2012 | RCT cross-over | Brazil | 33 | 48.7 (30–79) | 1 year | USPHS | RMGIC | 33 | 31 | V |
| RMGIC | 33 | 30 | |||||||||
| CR | 33 | 31 | |||||||||
| Adeleke et al. [62] | 2012 | RCT cross-over | Nigeria | 44 (32/12) | 52 ± 12 (25–74) | 1 year | USPHS | RMGIC | 44 | 170 | V |
| CR | 44 | 168 | |||||||||
| Santiago et al. [63] | 2010 | RCT cross-over | Brazil | 30 | (18–50) | 2 years | USPHS | RMGIC | 30 | 35 | V |
| CR | 30 | 35 | |||||||||
| Türkün et al. [64] | 2008 | RCT cross-over | Turkey | 24 (12/12) | 44 (25–54) | 2 years | USPHS | PMRC | 24 | 50 | V |
| CR | 24 | 50 | |||||||||
| Pollington et al. [65] | 2008 | RCT cross-over | United Kingdom | 30 | 54 | 3 years | USPHS | Compomer | 30 | 30 | V |
| CR | 30 | 30 | |||||||||
| Franco et al. [66] | 2006 | RCT cross-over | Brazil | 30 | (18–50) | 5 years | USPHS | RMGIC | 30 | 35 | V |
| CR | 30 | 35 | |||||||||
| Onal et al. [67] | 2005 | RCT cross-over | Turkey | 30 | (27–64) | 2 years | USPHS | RMGIC | 30 | 24 | V |
| PMRC | 30 | 38 | |||||||||
| PMRC | 30 | 46 | |||||||||
| CR | 30 | 22 | |||||||||
| Brackett et al. [68] | 2003 | RCT cross-over | Mexico | 24 | 47 (28–73) | 2 years | USPHS | RMGIC | 24 | 37 | V |
| CR | 24 | 37 | |||||||||
| Ozgünaltay et al. [69] | 2002 | RCT cross-over | Turkey | 24 | (40–65) | 3 years | USPHS | RMGIC | 24 | 50 | V |
| CR | 24 | 50 | |||||||||
| Folwaczny et al. [70] | 2001 | RCT cross-over | Germany | 37 | (26–67) | 3 years | USPHS | RMGIC | 37 | 51 | V |
| RMGIC | 37 | 31 | |||||||||
| CR | 37 | 36 | |||||||||
| PMRC | 37 | 79 | |||||||||
| Federlin et al. [71] | 1998 | RCT cross-over | Germany | 11 (5/6) | (30–77) | 1 year | USPHS | RMGIC | 11 | 16 | V |
| PMRC | 11 | 16 | |||||||||
| CR | 11 | 16 | |||||||||
| Matis et al. [72] | 1996 | RCT cross-over | United State | 30 (18/12) | 58 (29–76) | 10 years | USPHS | GIC-IF | 30 | 30 | V |
| GIC-DF | 30 | 30 | |||||||||
| GIC | 30 | 30 | |||||||||
| CR | 30 | 30 |
| Authors | Year | Groups | Absence of Secondary Caries, Erosion or Abfraction | Absence of Marginal Discoloration | Adequate Marginal Adaptation | Adequate Marginal or Tooth Integrity | Adequate Color or Translucency | Proper Surface Texture or Luster | Proper Surface Staining | Retention | Absence of Wear | Proper Anatomic Form | Absence of Sensibility | Adequate Periodontal Tissue |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Albelasy et al. [44] | 2024 | IRC | 6 m: 31/31 1 y: 29/29 2 y: 27/27 | 6 m: 31/31 1 y: 29/29 2 y: 27/27 | 6 m: 31/31 1 y: 29/29 2 y: 27/27 | 6 m: 31/31 1 y: 29/29 2 y: 27/27 | NR | NR | NR | 6 m: 31/31 1 y: 29/29 2 y: 27/27 | NR | NR | 6 m: 31/31 1 y: 29/29 2 y: 27/27 | NR |
| IRC | 6 m: 31/31 1 y: 29/29 2 y: 27/27 | 6 m: 31/31 1 y: 29/29 2 y: 27/27 | 6 m: 31/31 1 y: 29/29 2 y: 27/27 | 6 m: 31/31 1 y: 29/29 2 y: 27/27 | NR | NR | NR | 6 m: 31/31 1 y: 29/29 2 y: 26/27 | NR | NR | 6 m: 31/31 1 y: 29/29 2 y: 27/27 | NR | ||
| CR | 6 m: 31/31 1 y: 29/29 2 y: 27/27 | 6 m: 31/31 1 y: 29/29 2 y: 27/27 | 6 m: 31/31 1 y: 29/29 2 y: 27/27 | 6 m: 31/31 1 y: 29/29 2 y: 27/27 | NR | NR | NR | 6 m: 31/31 1 y: 29/29 2 y: 27/27 | NR | NR | 6 m: 31/31 1 y: 29/29 2 y: 27/27 | NR | ||
| Ballal et al. [45] | 2023 | RMGIC | 1 m: 40/40 6 m: 40/40 1 y: 40/40 | 1 m: 39/40 6 m: 32/40 1 y: 24/40 | NR | 1 m: 39/40 6 m: 29/40 1 y: 23/40 | NR | NR | NR | 1 m: 39/40 6 m: 32/40 1 y: 24/40 | NR | 1 m: 39/40 6 m: 30/40 1 y: 22/40 | NR | NR |
| CR | 1 m: 40/40 6 m: 40/40 1 y: 40/40 | 1 m: 40/40 6 m: 39/40 1 y: 33/40 | NR | 1 m: 40/40 6 m: 39/40 1 y: 31/40 | NR | NR | NR | 1 m: 40/40 6 m: 39/40 1 y: 33/40 | NR | 1 m: 40/40 6 m: 39/40 1 y: 32/40 | NR | NR | ||
| Saghir et al. [46] | 2023 | RMGIC | NR | NR | 1 y: 23/30 | NR | NR | 1 y: 25/30 | NR | 1 y: 28/30 | NR | NR | NR | NR |
| FCR | NR | NR | 1 y: 21/30 | NR | NR | 1 y: 18/30 | NR | 1 y: 19/30 | NR | NR | NR | NR | ||
| Wafaie et al. [47] | 2023 | HVGIC | 1 y: 40/40 3 y: 38/38 5 y: 38/38 | 1 y: 40/40 3 y: 38/38 5 y: 38/38 | 1 y: 40/40 3 y: 38/38 5 y: 38/38 | 1 y: 40/40 3 y: 38/38 5 y: 38/38 | 1 y: 40/40 3 y: 38/38 5 y: 38/38 | 1 y: 40/40 3 y: 38/38 5 y: 38/38 | 1 y: 40/40 3 y: 38/38 5 y: 38/38 | 1 y: 40/40 3 y: 38/39 5 y: 38/38 | 1 y: 40/40 3 y: 38/38 5 y: 38/38 | 1 y: 40/40 3 y: 38/38 5 y: 38/38 | 1 y: 40/40 3 y: 38/38 5 y: 38/38 | 1 y: 40/40 3 y: 38/38 5 y: 38/38 |
| HVGIC | 1 y: 40/40 3 y: 39/39 5 y: 37/37 | 1 y: 40/40 3 y: 39/39 5 y: 37/37 | 1 y: 40/40 3 y: 39/39 5 y: 37/37 | 1 y: 40/40 3 y: 39/39 5 y: 39/39 | 1 y: 40/40 3 y: 39/39 5 y: 37/37 | 1 y: 40/40 3 y: 39/39 5 y: 37/37 | 1 y: 40/40 3 y: 39/39 5 y: 37/37 | 1 y: 40/40 3 y: 39/39 5 y: 37/39 | 1 y: 40/40 3 y: 39/39 5 y: 37/37 | 1 y: 40/40 3 y: 39/39 5 y: 37/37 | 1 y: 40/40 3 y: 39/39 5 y: 39/39 | 1 y: 40/40 3 y: 39/39 5 y: 39/39 | ||
| HVGIC | 1 y: 40/40 3 y: 38/38 5 y: 38/38 | 1 y: 40/40 3 y: 38/38 5 y: 38/38 | 1 y: 40/40 3 y: 38/38 5 y: 37/38 | 1 y: 40/40 3 y: 39/39 5 y: 38/38 | 1 y: 40/40 3 y: 38/38 5 y: 38/38 | 1 y: 40/40 3 y: 38/38 5 y: 38/38 | 1 y: 40/40 3 y: 38/38 5 y: 38/38 | 1 y: 40/40 3 y: 38/39 5 y: 38/38 | 1 y: 40/40 3 y: 38/38 5 y: 38/38 | 1 y: 40/40 3 y: 38/38 5 y: 37/38 | 1 y: 40/40 3 y: 39/39 5 y: 38/38 | 1 y: 40/40 3 y: 39/39 5 y: 38/38 | ||
| CR | 1 y: 40/40 3 y: 39/39 5 y: 39/39 | 1 y: 40/40 3 y: 39/39 5 y: 39/39 | 1 y: 40/40 3 y: 39/39 5 y: 39/39 | 1 y: 40/40 3 y: 39/39 5 y: 39/39 | 1 y: 40/40 3 y: 39/39 5 y: 39/39 | 1 y: 40/40 3 y: 39/39 5 y: 39/39 | 1 y: 40/40 3 y: 39/39 5 y: 39/39 | 1 y: 40/40 3 y: 39/39 5 y: 39/39 | 1 y: 40/40 3 y: 39/39 5 y: 39/39 | 1 y: 40/40 3 y: 39/39 5 y: 39/39 | 1 y: 40/40 3 y: 39/39 5 y: 39/39 | 1 y: 40/40 3 y: 39/39 5 y: 39/39 | ||
| Toz-Akalin et al. [48] | 2023 | G | 2 y: 28/28 | 2 y: 28/28 | 2 y: 28/28 | 2 y: 28/28 | 2 y: 28/28 | 2 y: 28/28 | 2 y: 28/29 | 2 y: 28/28 | NR | 2 y: 28/28 | NR | |
| CR | 2 y: 29/29 | 2 y: 29/29 | 2 y: 29/29 | 2 y: 29/29 | 2 y: 29/29 | 2 y: 29/29 | 2 y: 29/29 | 2 y: 29/29 | NR | 2 y: 29/29 | NR | |||
| Gonçalves et al. [49] | 2021 | RMGIC | 1 y: 48/48 2 y: 47/47 3 y: 42/42 | 1 y: 45/48 2 y: 42/47 3 y: 29/42 | NR | 1 y: 44/48 2 y: 38/47 3 y: 30/42 | 1 y: 33/48 2 y: 33/47 3 y: 27/42 | 1 y: 47/48 2 y: 43/47 3 y: 34/42 | 1 y: 48/48 2 y: 46/47 3 y: 40/42 | 1 y: 48/49 2 y: 47/48 3 y: 42/43 | 1 y: 48/48 2 y: 46/47 3 y: 39/42 | 1 y: 46/48 2 y: 45/47 3 y: 40/42 | NR | 1 y: 48/48 2 y: 47/47 3 y: 42/42 |
| RMGIC + EDTA | 1 y: 49/49 2 y: 47/47 3 y: 40/40 | 1 y: 48/49 2 y: 41/47 3 y: 30/40 | NR | 1 y: 44/49 2 y: 37/47 3 y: 30/40 | 1 y: 38/49 2 y: 35/47 3 y: 32/40 | 1 y: 47/49 2 y: 42/47 3 y: 32/40 | 1 y: 49/49 2 y: 47/47 3 y: 40/40 | 1 y: 49/49 2 y: 47/48 3 y: 40/42 | 1 y: 49/49 2 y: 47/47 3 y: 38/40 | 1 y: 46/49 2 y: 44/47 3 y: 38/40 | NR | 1 y: 49/49 2 y: 47/47 3 y: 40/40 | ||
| CR | 1 y: 47/47 2 y: 44/44 3 y: 37/37 | 1 y: 41/47 2 y: 35/44 3 y: 25/37 | NR | 1 y: 38/47 2 y: 35/44 3 y: 25/37 | 1 y: 36/47 2 y: 36/44 3 y: 29/37 | 1 y: 45/47 2 y: 43/44 3 y: 35/37 | 1 y: 45/47 2 y: 43/44 3 y: 35/37 | 1 y: 47/49 2 y: 44/48 3 y: 37/42 | 1 y: 47/47 2 y: 44/44 3 y: 36/37 | 1 y: 46/47 2 y: 43/44 3 y: 36/37 | NR | 1 y: 46/47 2 y: 43/44 3 y: 36/37 | ||
| CR + SE | 1 y: 48/48 2 y: 47/47 3 y: 41/41 | 1 y: 43/48 2 y: 37/47 3 y: 25/41 | NR | 1 y: 43/48 2 y: 40/47 3 y: 30/41 | 1 y: 38/48 2 y: 38/47 3 y: 32/41 | 1 y: 43/48 2 y: 43/47 3 y: 36/41 | 1 y: 47/48 2 y: 45/47 3 y: 39/41 | 1 y: 48/49 2 y: 47/48 3 y: 41/42 | 1 y: 48/48 2 y: 46/47 3 y: 38/41 | 1 y: 48/48 2 y: 47/47 3 y: 41/41 | NR | 1 y: 48/48 2 y: 47/47 3 y: 41/41 | ||
| Schwendicke et al. [50] | 2021 | HVGIC | 1.5 y: 67/67 3y: 41/41 | 1.5 y: 67/67 3y: 41/41 | 1.5 y: 65/67 3y: 40/41 | NR | 1.5 y: 67/67 3y: 41/41 | 1.5 y: 67/67 3y: 41/41 | 1.5 y: 67/67 3y: 41/41 | 1.5 y: 64/77 3y: 39/41 | 1.5 y: 67/67 3y: 41/41 | 1.5 y: 66/67 3y: 41/41 | 1.5 y: 67/67 3y: 41/41 | NR |
| CR | 1.5 y: 70/70 3y: 49/49 | 1.5 y: 70/70 3y: 49/49 | 1.5 y: 70/70 3y: 49/49 | NR | 1.5 y: 70/70 3y: 49/49 | 1.5 y: 70/70 3y: 49/49 | 1.5 y: 70/70 3y: 49/49 | 1.5 y: 70/77 3y: 49/49 | 1.5 y: 70/70 3y: 49/49 | 1.5 y: 70/70 3y: 49/49 | 1.5 y: 70/70 3y: 49/49 | NR | ||
| Koc Vural et al. [51] | 2021 | RMGIC | 6 m: 54/54 1 y: 52/52 1.5 y: 48/48 2 y: 47/47 3 y: 47/47 | 6 m: 53/54 1 y: 51/52 1.5 y: 33/48 2 y: 31/47 3 y: 31/47 | 6 m: 54/54 1 y: 52/52 1.5 y: 48/48 2 y: 47/47 3 y: 47/47 | NR | NR | NR | NR | 6 m: 54/55 1 y: 52/53 1.5 y: 48/51 2 y: 47/51 3 y: 47/51 | NR | NR | 6 m: 54/54 1 y: 52/52 1.5 y: 48/48 2 y: 47/47 3 y: 47/47 | NR |
| CR | 6 m: 55/55 1 y: 52/52 1.5 y: 43/43 2 y: 43/43 3 y: 43/43 | 6 m: 55/55 1 y: 52/52 1.5 y: 40/43 2 y: 40/43 3 y: 40/43 | 6 m: 55/55 1 y: 52/52 1.5 y: 43/43 2 y: 43/43 3 y: 43/43 | NR | NR | NR | NR | 6 m: 55/55 1 y: 52/53 1.5 y: 43/51 2 y: 43/51 3 y: 43/51 | NR | NR | 6 m: 55/55 1 y: 52/52 1.5 y: 43/43 2 y: 43/43 3 y: 43/43 | NR | ||
| Balkaya et al. [52] | 2020 | HVGIC | 1 y: 32/32 2 y: 21/21 | 1 y: 32/32 2 y: 20/21 | 1 y: 30/32 2 y: 20/21 | NR | 1 y: 6/32 2 y: 15/21 | 1 y: 31/32 2 y: 19/21 | NR | 1 y: 24/32 2 y: 15/21 | NR | 1 y: 30/32 2 y: 20/21 | 1 y: 32/32 2 y: 21/21 | NR |
| CR | 1 y: 35/35 2 y: 32/32 | 1 y: 35/35 2 y: 32/32 | 1 y: 35/35 2 y: 32/32 | NR | 1 y: 35/35 2 y: 32/32 | 1 y: 35/35 2 y: 32/32 | NR | 1 y: 35/35 2 y: 32/32 | NR | 1 y: 35/35 2 y: 32/32 | 1 y: 35/35 2 y: 32/32 | NR | ||
| CR | 1 y: 36/36 2 y: 31/31 | 1 y: 36/36 2 y: 31/31 | 1 y: 36/36 2 y: 31/31 | NR | 1 y: 36/36 2 y: 31/31 | 1 y: 36/36 2 y: 31/31 | NR | 1 y: 36/36 2 y: 31/31 | NR | 1 y: 36/36 2 y: 31/31 | 1 y: 36/36 2 y: 31/31 | NR | ||
| Miletić et al. [53] | 2020 | GH | 1 y: 162/162 2 y: 143/143 | 1 y: 161/161 2 y: 142/142 | 1 y: 161/161 2 y: 142/142 | 1 y: 162/162 2 y: 143/143 | NR | NR | 1 y: 162/162 2 y: 143/143 | 1 y: 162/162 2 y: 143/143 | 1 y: 162/162 2 y: 143/143 | 1 y: 162/162 2 y: 143/143 | 1 y: 162/162 2 y: 143/143 | 1 y: 162/162 2 y: 144/144 |
| CR | 1 y: 162/162 2 y: 143/143 | 1 y: 161/161 2 y: 142/142 | 1 y: 161/161 2 y: 142/142 | 1 y: 162/162 2 y: 143/143 | NR | NR | 1 y: 162/162 2 y: 143/143 | 1 y: 161/162 2 y: 141/143 | 1 y: 162/162 2 y: 143/143 | 1 y: 162/162 2 y: 143/143 | 1 y: 162/162 2 y: 143/143 | 1 y: 162/162 2 y: 144/144 | ||
| Celik et al. [54] | 2019 | HVGIC | 6 m: 66/66 1 y: 63/63 2 y: 52/52 3 y: 47/47 | 6 m: 66/66 1 y: 63/63 2 y: 52/52 3 y: 47/47 | 6 m: 66/66 1 y: 63/63 2 y: 52/52 3 y: 47/47 | 6 m: 66/66 1 y: 63/63 2 y: 52/52 3 y: 47/47 | 6 m: 66/66 1 y: 63/63 2 y: 52/52 3 y: 47/47 | 6 m: 66/66 1 y: 63/63 2 y: 52/52 3 y: 47/47 | 6 m: 66/66 1 y: 63/63 2 y: 52/52 3 y: 47/47 | 6 m: 66/66 1 y: 63/63 2 y: 52/53 3 y: 47/49 | 6 m: 66/66 1 y: 63/63 2 y: 52/52 3 y: 47/47 | 6 m: 66/66 1 y: 63/63 2 y: 52/52 3 y: 47/47 | 6 m: 66/66 1 y: 63/63 2 y: 52/52 3 y: 47/47 | 6 m: 66/66 1 y: 63/63 2 y: 52/52 3 y: 47/47 |
| CR | 6 m: 67/67 1 y: 67/67 2 y: 57/57 3 y: 54/54 | 6 m: 67/67 1 y: 67/67 2 y: 57/57 3 y: 54/54 | 6 m: 67/67 1 y: 67/67 2 y: 57/57 3 y: 54/54 | 6 m: 67/67 1 y: 67/67 2 y: 57/57 3 y: 54/54 | 6 m: 67/67 1 y: 67/67 2 y: 57/57 3 y: 54/54 | 6 m: 67/67 1 y: 67/67 2 y: 57/57 3 y: 54/54 | 6 m: 67/67 1 y: 67/67 2 y: 57/57 3 y: 54/54 | 6 m: 67/67 1 y: 67/67 2 y: 57/57 3 y: 54/54 | 6 m: 67/67 1 y: 67/67 2 y: 57/57 3 y: 54/54 | 6 m: 67/67 1 y: 67/67 2 y: 57/57 3 y: 54/54 | 6 m: 67/67 1 y: 67/67 2 y: 57/57 3 y: 54/54 | 6 m: 67/67 1 y: 67/67 2 y: 55/57 3 y: 52/54 | ||
| van Dijken et al. [55] | 2019 | RMGIC | 1 y: 3/82 | 1 y: 82/82 | 1 y: 74/82 | NR | 1 y: 77/82 | 1 y: 82/82 | NR | 1 y: 62/82 | NR | 1 y: 74/82 | NR | NR |
| CR | 1 y: 82/82 | 2 y: 82/82 | 2 y: 81/82 | NR | 2 y: 82/82 | 2 y: 82/82 | NR | 2 y: 80/82 | NR | 2 y: 81/82 | NR | NR | ||
| Jassal et al. [56] | 2018 | RMGIC | 6 m: 95/95 1 y: 90/90 1.5 y: 90/90 | 6 m: 95/95 1 y: 90/90 1.5 y: 90/90 | 6 m: 95/95 1 y: 90/90 1.5 y: 90/90 | NR | NR | NR | NR | 6 m: 95/98 1 y: 90/98 1.5 y: 90/98 | NR | NR | 6 m: 95/95 1 y: 90/90 1.5 y: 90/90 | NR |
| CR + P-SEA | 6 m: 93/93 1 y: 88/88 1.5 y: 86/86 | 6 m: 92/93 1 y: 87/88 1.5 y: 85/86 | 6 m: 92/93 1 y: 87/88 1.5 y: 85/86 | NR | NR | NR | NR | 6 m: 93/98 1 y: 88/98 1.5 y: 86/98 | NR | NR | 6 m: 93/93 1 y: 88/88 1.5 y: 86/86 | NR | ||
| CR + A-SEA | 6 m: 96/96 1 y: 93/93 1.5 y: 92/92 | 6 m: 96/96 1 y: 93/93 1.5 y: 92/92 | 6 m: 96/96 1 y: 93/93 1.5 y: 92/92 | NR | NR | NR | NR | 6 m: 96/98 1 y: 93/98 1.5 y: 92/98 | NR | NR | 6 m: 96/96 1 y: 93/93 1.5 y: 92/92 | NR | ||
| Hussainy et al. [57] | 2018 | RMGIC | NR | 6 m: 33/33 1 y: 32/33 | 6 m: 33/33 1 y: 32/33 | NR | 6 m: 33/33 1 y: 32/33 | 6 m: 33/33 1 y: 32/33 | NR | 6 m: 33/33 1 y: 32/33 | NR | NR | 6 m: 33/33 1 y: 32/33 | NR |
| PMRC | NR | 6 m: 33/34 1 y: 33/34 | 6 m: 33/34 1 y: 33/34 | NR | 6 m: 33/34 1 y: 33/34 | 6 m: 33/34 1 y: 33/34 | NR | 6 m: 33/34 1 y: 33/34 | NR | NR | 6 m: 33/34 1 y: 33/34 | NR | ||
| CR | NR | 6 m: 32/34 1 y: 32/34 | 6 m: 32/34 1 y: 32/34 | NR | 6 m: 32/34 1 y: 32/34 | 6 m: 32/34 1 y: 32/34 | NR | 6 m: 32/34 1 y: 32/34 | NR | NR | 6 m: 32/34 1 y: 32/34 | NR | ||
| Popescu et al. [58] | 2016 | RMGIC | 6 m: 73/73 1 y: 57/57 1.5 y: 57/57 2 y: 57/57 | 6 m: 73/73 1 y: 49/57 1.5 y: 38/57 2 y: 32/57 | 6 m: 73/73 1 y: 49/57 1.5 y: 39/57 2 y: 32/57 | NR | 6 m: 41/73 1 y: 32/57 1.5 y: 32/57 2 y: 50/57 | NR | NR | 6 m: 73/73 1 y: 57/57 1.5 y: 57/57 2 y: 54/57 | NR | 6 m: 73/73 1 y: 57/57 1.5 y: 57/57 2 y: 57/57 | NR | NR |
| CR | 6 m: 74/74 1 y: 58/58 1.5 y: 57/57 2 y: 53/53 | 6 m: 74/74 1 y: 52/58 1.5 y: 37/57 2 y: 31/53 | 6 m: 74/74 1 y: 52/58 1.5 y: 39/57 2 y: 30/53 | NR | 6 m: 74/74 1 y: 57/58 1.5 y: 51/57 2 y: 44/53 | NR | NR | 6 m: 74/74 1 y: 58/58 1.5 y: 57/58 2 y: 53/57 | NR | 6 m: 74/74 1 y: 58/58 1.5 y: 57/57 2 y: 53/53 | NR | NR | ||
| RMGIC + CR | 6 m: 73/73 1 y: 57/57 1.5 y: 54/54 2 y: 48/48 | 6 m: 73/73 1 y: 54/57 1.5 y: 39/54 2 y: 30/48 | 6 m: 73/73 1 y: 54/57 1.5 y: 38/54 2 y: 28/48 | NR | 6 m: 73/73 1 y: 55/57 1.5 y: 45/54 2 y: 37/48 | NR | NR | 6 m: 73/73 1 y: 57/57 1.5 y: 54/57 2 y: 48/57 | NR | 6 m: 73/73 1 y: 57/57 1.5 y: 54/54 2 y: 48/48 | NR | NR | ||
| Fagundes et al. [59] | 2014 | RMGIC | 6 m: 34/34 1 y: 35/35 2 y: 33/33 5 y: 27/27 7 y: 23/23 | 6 m: 34/34 1 y: 35/35 2 y: 33/33 5 y: 27/27 7 y: 23/23 | NR | 6 m: 34/34 1 y: 35/35 2 y: 33/33 5 y: 23/27 7 y: 20/23 | NR | NR | NR | 6 m: 34/34 1 y: 35/35 2 y: 33/33 5 y: 27/28 7 y: 23/26 | NR | 6 m: 34/34 1 y: 35/35 2 y: 33/33 5 y: 23/27 7 y: 21/23 | NR | NR |
| CR | 6 m: 30/30 1 y: 30/30 2 y: 26/26 5 y: 15/17 7 y: 12/13 | 6 m: 30/30 1 y: 30/30 2 y: 26/26 5 y: 17/17 7 y: 13/13 | NR | 6 m: 30/30 1 y: 30/30 2 y: 26/26 5 y: 13/17 7 y: 9/13 | NR | NR | NR | 6 m: 30/34 1 y: 30/35 2 y: 26/33 5 y: 17/27 7 y: 13/25 | NR | 6 m: 29/30 1 y: 29/30 2 y: 25/26 5 y: 15/17 7 y: 12/13 | NR | NR | ||
| de Oliveira et al. [60] | 2012 | RMGIC | 1 y: 38/38 | 1 y: 38/38 | 1 y: 38/38 | NR | 1 y: 38/38 | NR | NR | 1 y: 38/40 | NR | 1 y: 38/38 | NR | NR |
| RMGIC + AS | 1 y: 43/43 | 1 y: 43/43 | 1 y: 43/43 | NR | 1 y: 43/43 | NR | NR | 1 y: 43/43 | NR | 1 y: 43/43 | NR | NR | ||
| CR | 1 y: 41/41 | 1 y: 41/41 | 1 y: 41/41 | NR | 1 y: 41/41 | NR | NR | 1 y: 41/41 | NR | 1 y: 41/41 | NR | NR | ||
| Perdigão et al. [61] | 2012 | RMGIC | 6 m: 28/28 1 y: 26/26 | 6 m: 28/28 1 y: 25/26 | 6 m: 26/28 1 y: 26/26 | NR | 6 m: 28/28 1 y: 26/26 | 6 m: 16/28 1 y: 11/26 | NR | 6 m: 28/28 1 y: 26/26 | 6 m: 28/28 1 y: 26/26 | NR | 6 m: 28/28 1 y: 25/26 | NR |
| N-RMGIC | 6 m: 27/27 1 y: 25/25 | 6 m: 26/27 1 y: 15/25 | 6 m: 21/27 1 y: 17/25 | NR | 6 m: 16/27 1 y: 15/25 | 6 m: 24/27 1 y: 23/25 | NR | 6 m: 27/27 1 y: 25/25 | 6 m: 26/27 1 y: 24/25 | NR | 6 m: 27/27 1 y: 24/25 | NR | ||
| CR | 6 m: 27/29 1 y: 25/27 | 6 m: 25/29 1 y: 22/27 | 6 m: 23/29 1 y: 23/27 | NR | 6 m: 25/29 1 y: 22/27 | 6 m: 26/29 1 y: 25/27 | NR | 6 m: 27/29 1 y: 25/27 | 6 m: 27/29 1 y: 25/27 | NR | 6 m: 27/29 1 y: 24/27 | NR | ||
| Adeleke et al. [62] | 2012 | RMGIC | 6 m: 154/154 1 y: 117/117 | 6 m: 136/136 1 y: 130/131 | 6 m: 136/136 1 y: 131/131 | NR | NR | NR | NR | 6 m: 136/148 1 y: 131/144 | 6 m: 136/136 1 y: 131/131 | NR | 6 m: 136/136 1 y: 131/131 | NR |
| CR | 6 m: 86/86 1 y: 72/72 | 6 m: 115/115 1 y: 105/106 | 6 m: 115/115 1 y: 105/106 | NR | NR | NR | NR | 6 m: 115/147 1 y: 106/143 | 6 m: 115/115 1 y: 106/106 | NR | 6 m: 115/115 1 y: 106/106 | NR | ||
| Santiago et al. [63] | 2010 | RMGIC | 6 m: 35/35 1 y: 35/35 2 y: 33/33 | 6 m: 35/35 1 y: 35/35 2 y: 33/33 | NR | 6 m: 35/35 1 y: 35/35 2 y: 33/33 | NR | NR | NR | 6 m: 35/35 1 y: 35/35 2 y: 33/33 | NR | 6 m: 35/35 1 y: 35/35 2 y: 33/33 | NR | NR |
| CR | 6 m: 31/31 1 y: 30/30 2 y: 26/26 | 6 m: 31/31 1 y: 30/30 2 y: 26/26 | NR | 6 m: 31/31 1 y: 30/30 2 y: 26/26 | NR | NR | NR | 6 m: 31/35 1 y: 30/35 2 y: 26/33 | NR | 6 m: 31/31 1 y: 29/30 2 y: 25/26 | NR | NR | ||
| Türkün et al. [64] | 2008 | PMRC | 6 m: 50/50 1 y: 50/50 2 y: 50/50 | 6 m: 50/50 1 y: 50/50 2 y: 50/50 | 6 m: 50/50 1 y: 50/50 2 y: 50/50 | NR | 6 m: 50/50 1 y: 50/50 2 y: 50/50 | 6 m: 50/50 1 y: 50/50 2 y: 50/50 | NR | 6 m: 50/50 1 y: 50/50 2 y: 48/50 | NR | NR | 6 m: 50/50 1 y: 50/50 2 y: 50/50 | 6 m: 50/50 1 y: 50/50 2 y: 50/50 |
| CR | 6 m: 50/50 1 y: 50/50 2 y: 50/50 | 6 m: 50/50 1 y: 50/50 2 y: 50/50 | 6 m: 50/50 1 y: 50/50 2 y: 50/50 | NR | 6 m: 48/50 1 y: 48/50 2 y: 47/50 | 6 m: 50/50 1 y: 50/50 2 y: 50/50 | NR | 6 m: 50/50 1 y: 50/50 2 y: 50/50 | NR | NR | 6 m: 50/50 1 y: 50/50 2 y: 50/50 | 6 m: 50/50 1 y: 50/50 2 y: 50/50 | ||
| Pollington et al. [65] | 2008 | C | 6 m: 30/30 1 y: 30/30 3 y: 30/30 | 6 m: 29/30 1 y: 28/30 3 y: 28/30 | 6 m: 26/30 1 y: 25/30 3 y: 24/30 | NR | NR | NR | NR | 6 m: 28/30 1 y: 27/30 3 y: 26/30 | NR | 6 m: 27/30 1 y: 27/30 3 y: 27/30 | NR | NR |
| CR | 6 m: 30/30 1 y: 30/30 3 y: 30/30 | 6 m: 29/30 1 y: 29/30 3 y: 28/30 | 6 m: 28/30 1 y: 27/30 3 y: 25/30 | NR | NR | NR | NR | 6 m: 28/30 1 y: 28/30 3 y: 26/30 | NR | 6 m: 30/30 1 y: 29/30 3 y: 29/30 | NR | NR | ||
| Franco et al. [66] | 2006 | RMGIC | 1 y: 35/35 2 y: 33/33 5 y: 27/27 | 1 y: 35/35 2 y: 33/33 5 y: 27/27 | NR | 1 y: 35/35 2 y: 33/33 5 y: 23/27 | NR | NR | NR | 1 y: 35/35 2 y: 33/33 5 y: 27/28 | NR | 1 y: 35/35 2 y: 33/33 5 y: 23/27 | NR | NR |
| CR | 1 y: 30/30 2 y: 26/26 5 y: 15/17 | 1 y: 30/30 2 y: 26/26 5 y: 17/17 | NR | 1 y: 30/30 2 y: 26/26 5 y: 13/17 | NR | NR | NR | 1 y: 30/35 2 y: 26/33 5 y: 27/33 | NR | 1 y: 29/30 2 y: 25/26 5 y: 15/17 | NR | NR | ||
| Onal et al. [67] | 2005 | RMGIC | 1 y: 24/24 2 y: 24/24 | 1 y: 24/24 2 y: 24/24 | NR | 1 y: 24/24 2 y: 24/24 | 1 y: 24/24 2 y: 24/24 | 1 y: 24/24 2 y: 24/24 | NR | 1 y: 24/24 2 y: 24/24 | NR | 1 y: 24/24 2 y: 24/24 | NR | NR |
| PMRC | 1 y: 32/32 2 y: 21/21 | 1 y: 32/32 2 y: 21/21 | NR | 1 y: 32/32 2 y: 21/21 | 1 y: 32/32 2 y: 21/21 | 1 y: 32/32 2 y: 21/21 | NR | 1 y: 32/38 2 y: 21/32 | NR | 1 y: 32/32 2 y: 21/21 | NR | NR | ||
| PMRC | 1 y: 38/38 2 y: 26/26 | 1 y: 38/38 2 y: 26/26 | NR | 1 y: 38/38 2 y: 26/26 | 1 y: 38/38 2 y: 26/26 | 1 y: 38/38 2 y: 26/26 | NR | 1 y: 38/46 2 y: 26/38 | NR | 1 y: 38/38 2 y: 26/26 | NR | NR | ||
| CR | 1 y: 18/18 2 y: 13/13 | 1 y: 18/18 2 y: 13/13 | NR | 1 y: 18/18 2 y: 13/13 | 1 y: 18/18 2 y: 13/13 | 1 y: 18/18 2 y: 13/13 | NR | 1 y: 18/22 2 y: 13/18 | NR | 1 y: 18/18 2 y: 13/13 | NR | NR | ||
| Brackett et al. [68] | 2003 | RMGIC | 6 m: 31/31 1 y: 30/30 1.5 y: 30/30 2 y: 26/26 | 6 m: 31/31 1 y: 30/30 1.5 y: 30/30 2 y: 26/26 | 6 m: 31/31 1 y: 30/30 1.5 y: 30/30 2 y: 26/26 | NR | 6 m: 31/31 1 y: 30/30 1.5 y: 30/30 2 y: 26/26 | 6 m: 31/31 1 y: 30/30 1.5 y: 30/30 2 y: 26/26 | NR | 6 m: 31/32 1 y: 30/31 1.5 y: 30/31 2 y: 26/27 | NR | 6 m: 31/31 1 y: 30/30 1.5 y: 30/30 2 y: 26/26 | NR | NR |
| CR | 6 m: 28/28 1 y: 26/26 1.5 y: 26/26 2 y: 22/22 | 6 m: 28/28 1 y: 26/26 1.5 y: 26/26 2 y: 22/22 | 6 m: 28/28 1 y: 26/26 1.5 y: 26/26 2 y: 22/22 | NR | 6 m: 28/28 1 y: 26/26 1.5 y: 26/26 2 y: 22/22 | 6 m: 28/28 1 y: 26/26 1.5 y: 26/26 2 y: 22/22 | NR | 6 m: 28/32 1 y: 26/31 1.5 y: 26/31 2 y: 22/27 | NR | 6 m: 28/28 1 y: 26/26 1.5 y: 26/26 2 y: 22/22 | NR | NR | ||
| Ozgünaltay et al. [69] | 2002 | RMGIC | 6 m: 48/48 1 y: 48/48 2 y: 44/44 3 y: 44/44 | 6 m: 48/48 1 y: 48/48 2 y: 44/44 3 y: 44/44 | 6 m: 48/48 1 y: 48/48 2 y: 44/44 3 y: 44/44 | NR | 6 m: 48/48 1 y: 48/48 2 y: 44/44 3 y: 44/44 | NR | NR | 6 m: 48/48 1 y: 48/48 2 y: 44/45 3 y: 44/45 | NR | 6 m: 48/48 1 y: 48/48 2 y: 44/44 3 y: 44/44 | NR | NR |
| CR | 6 m: 45/45 1 y: 45/45 2 y: 40/40 3 y: 40/40 | 6 m: 45/45 1 y: 45/45 2 y: 40/40 3 y: 40/40 | 6 m: 45/45 1 y: 45/45 2 y: 40/40 3 y: 40/40 | NR | 6 m: 45/45 1 y: 45/45 2 y: 40/40 3 y: 40/40 | NR | NR | 6 m: 45/45 1 y: 45/45 2 y: 40/42 3 y: 40/42 | NR | 6 m: 45/45 1 y: 45/45 2 y: 40/40 3 y: 40/40 | NR | NR | ||
| Folwaczny et al. [70] | 2001 | RMGIC | NR | 3 y: 28/31 | NR | 3 y: 24/31 | 3 y: 31/31 | 3 y: 31/31 | NR | 3 y: 31/33 | NR | 3 y: 29/31 | NR | NR |
| RMGIC | NR | 3 y: 19/23 | NR | 3 y: 17/23 | 3 y: 23/23 | 3 y: 23/23 | NR | 3 y: 23/26 | NR | 3 y: 14/23 | NR | NR | ||
| CR | NR | 3 y: 20/22 | NR | 3 y: 20/22 | 3 y: 22/22 | 3 y: 22/22 | NR | 3 y: 22/23 | NR | 3 y: 22/22 | NR | NR | ||
| PMRC | NR | 3 y: 40/43 | NR | 3 y: 36/43 | 3 y: 43/43 | 3 y: 43/43 | NR | 3 y: 43/48 | NR | 3 y: 40/43 | NR | NR | ||
| Federlin et al. [71] | 1998 | RMGIC | 1 y: 15/15 | 1 y: 15/15 | NR | 1 y: 15/15 | 1 y: 15/15 | 1 y: 15/15 | NR | NR | NR | 1 y: 15/15 | NR | NR |
| PMRC | 1 y: 15/15 | 1 y: 15/15 | NR | 1 y: 15/15 | 1 y: 15/15 | 1 y: 15/15 | NR | NR | NR | 1 y: 15/15 | NR | NR | ||
| CR | 1 y: 15/15 | 1 y: 15/15 | NR | 1 y: 15/15 | 1 y: 15/15 | 1 y: 15/15 | NR | NR | NR | 1 y: 15/15 | NR | NR | ||
| Matis et al. [72] | 1996 | GIC-IF | 10 y: 15/15 | 10 y: 15/15 | 10 y: 13/15 | NR | NR | 10 y: 15/15 | 10 y: 14/15 | 6 m: 29/29 1 y: 29/29 3 y: 27/30 5 y: 27/30 10 y: 15/18 | 10 y: 14/15 | 10 y: 13/15 | NR | NR |
| GIC-DF | 10 y: 14/14 | 10 y: 14/14 | 10 y: 12/14 | NR | NR | 10 y: 14/14 | 10 y: 14/14 | 6 m: 29/29 1 y: 29/29 3 y: 29/30 5 y: 28/30 10 y: 14/18 | 10 y: 12/14 | 10 y: 14/14 | NR | NR | ||
| GIC | 10 y: 12/12 | 10 y: 12/12 | 10 y: 10/12 | NR | NR | 10 y: 12/12 | 10 y: 11/12 | 6 m: 28/29 1 y: 28/29 3 y: 28/30 5 y: 28/30 10 y: 12/18 | 10 y: 9/12 | 10 y: 8/12 | NR | NR | ||
| CR | 10 y: 3/3 | 10 y: 3/3 | 10 y: 2/3 | NR | NR | 10 y: 3/3 | 10 y: 3/3 | 6 m: 22/29 1 y: 20/29 3 y: 15/30 5 y: 13/30 10 y: 3/18 | 10 y: 3/3 | 10 y: 3/3 | NR | NR |
| Certainty Assessment | N° of Patients | Effect | Certainty | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| N° of Studies | Study Design | Risk of Bias | Inconsistency | Indirectness | Imprecision | Other Considerations | IRR | CR | Relative (95% CI) | Absolute (95% CI) | |
| Absence of secondary caries or erosion or abfraction (follow-up: range 1 year to 10 years) | |||||||||||
| 26 | randomized trials | not serious | serious | not serious | not serious | none | 1088/1167 (93.2%) | 1083/1089 (99.4%) | RR 1.00 (0.97 to 1.04) | 0 fewer per 1000 (from 30 fewer to 40 more) | ⨁⨁⨁◯ Moderate |
| Absence of marginal discoloration (follow-up: range 1 year to 10 years) | |||||||||||
| 27 | randomized trials | not serious | not serious | not serious | not serious | none | 1128/1208 (93.4%) | 1093/1149 (95.1%) | RR 1.00 (0.99 to 1.01) | 0 fewer per 1000 (from 10 fewer to 10 more) | ⨁⨁⨁⨁ High |
| Adequate marginal adaptation (follow-up: range 1 year to 10 years) | |||||||||||
| 21 | randomized trials | not serious | not serious | not serious | not serious | none | 988/1039 (95.1%) | 979/1025 (95.5%) | RR 1.00 (0.99 to 1.01) | 0 fewer per 1000 (from 10 fewer to 10 more) | ⨁⨁⨁⨁ High |
| Adequate marginal or tooth integrity (follow-up: range 1 year to 5 years) | |||||||||||
| 13 | randomized trials | not serious | not serious | not serious | not serious | none | 468/511 (91.6%) | 442/475 (93.1%) | RR 1.00 (0.99 to 1.01) | 0 fewer per 1000 (from 9 fewer to 9 more) | ⨁⨁⨁⨁ High |
| Adequate color or translucency (follow-up: range 1 year to 5 years) | |||||||||||
| 17 | randomized trials | not serious | not serious | not serious | not serious | None | 600/634 (94.6%) | 612/639 (95.8%) | RR 1.00 (0.98 to 1.02) | 0 more per 1000 (from 19 fewer to 19 more) | ⨁⨁⨁⨁ High |
| Proper surface texture or luster (follow-up: range 1 year to 10 years) | |||||||||||
| 16 | randomized trials | not serious | serious | not serious | not serious | none | 506/537 (94.2%) | 520/538 (96.7%) | RR 0.99 (0.97 to 1.02) | 10 fewer per 1000 (from 29 fewer to 19 more) | ⨁⨁⨁◯ Moderate |
| Proper surface staining (follow-up: range 2 years to 10 years) | |||||||||||
| 7 | randomized trials | not serious | not serious | not serious | not serious | none | 347/350 (99.1%) | 352/354 (99.4%) | RR 1.00 (0.99 to 1.01) | 0 fewer per 1000 (from 10 fewer to 10 more) | ⨁⨁⨁⨁ High |
| Retention (follow-up: range 1 year to 10 years) | |||||||||||
| 28 | randomized trials | not serious | serious | not serious | not serious | none | 1195/1300 (91.9%) | 1174/1317 (89.1%) | RR 1.02 (0.98 to 1.06) | 9 more per 1000 (from 18 fewer to 53 more) | ⨁⨁⨁◯ Moderate |
| Absence of wear (follow-up: range 1 year to 10 years) | |||||||||||
| 9 | randomized trials | not serious | not serious | not serious | not serious | none | 501/507 (98.8%) | 484/487 (99.4%) | RR 1.00 (0.99 to 1.01) | 0 fewer per 1000 (from 10 fewer to 10 more) | ⨁⨁⨁⨁ High |
| Proper anatomic form (follow-up: range 1 year to 10 years) | |||||||||||
| 20 | randomized trials | not serious | serious | not serious | not serious | none | 752/805 (93.4%) | 756/771 (98.1%) | RR 0.98 (0.95 to 1.01) | 20 fewer per 1000 (from 49 fewer to 10 more) | ⨁⨁⨁◯ Moderate |
| Absence of sensibility (follow-up: range 1 years to 5 years) | |||||||||||
| 13 | randomized trials | not serious | not serious | not serious | not serious | none | 721/723 (99.7%) | 720/725 (99.3%) | RR 1.00 (0.99 to 1.01) | 0 fewer per 1000 (from 10 fewer to 10 more) | ⨁⨁⨁⨁ High |
| Adequate periodontal tissue (follow-up: range 2 years to 5 years) | |||||||||||
| 5 | randomized trials | not serious | not serious | not serious | not serious | none | 322/322 (100.0%) | 321/324 (99.1%) | RR 1.00 (0.99 to 1.01) | 0 more per 1000 (from 10 fewer to 10 more) | ⨁⨁⨁⨁ High |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Arbildo-Vega, H.I.; Cruzado-Oliva, F.H.; Coronel-Zubiate, F.T.; Luján-Valencia, S.A.; Meza-Málaga, J.M.; Aguirre-Ipenza, R.; Echevarria-Goche, A.; Luján-Urviola, E.; Castillo-Cornock, T.B.; Serquen-Olano, K.; et al. Clinical Effectiveness of Ion-Releasing Restorations versus Composite Restorations in Dental Restorations: Systematic Review and Meta-Analysis. Dent. J. 2024, 12, 158. https://doi.org/10.3390/dj12060158
Arbildo-Vega HI, Cruzado-Oliva FH, Coronel-Zubiate FT, Luján-Valencia SA, Meza-Málaga JM, Aguirre-Ipenza R, Echevarria-Goche A, Luján-Urviola E, Castillo-Cornock TB, Serquen-Olano K, et al. Clinical Effectiveness of Ion-Releasing Restorations versus Composite Restorations in Dental Restorations: Systematic Review and Meta-Analysis. Dentistry Journal. 2024; 12(6):158. https://doi.org/10.3390/dj12060158
Chicago/Turabian StyleArbildo-Vega, Heber Isac, Fredy Hugo Cruzado-Oliva, Franz Tito Coronel-Zubiate, Sara Antonieta Luján-Valencia, Joan Manuel Meza-Málaga, Rubén Aguirre-Ipenza, Adriana Echevarria-Goche, Eduardo Luján-Urviola, Tania Belú Castillo-Cornock, Katherine Serquen-Olano, and et al. 2024. "Clinical Effectiveness of Ion-Releasing Restorations versus Composite Restorations in Dental Restorations: Systematic Review and Meta-Analysis" Dentistry Journal 12, no. 6: 158. https://doi.org/10.3390/dj12060158