
The Efficacy of the RME II System Compared with a Herbst Appliance in the Treatment of Class II Skeletal Malocclusion in Growing Patients: A Retrospective Study

 , , , , , , and
, , , , , , and 
Abstract
:1. Introduction
2. Material and Methods
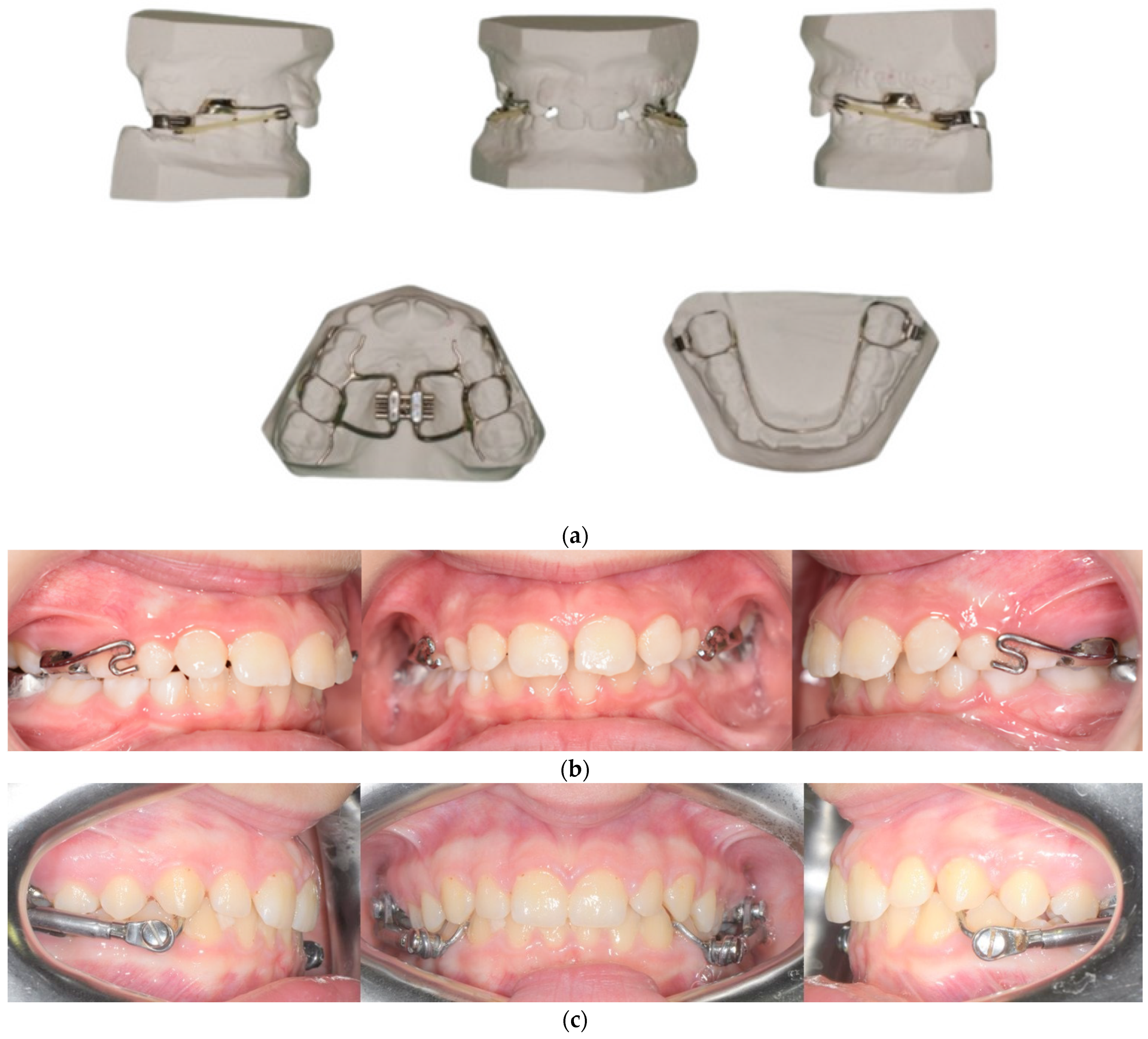
2.1. Group R
2.2. Group H
2.3. Group C
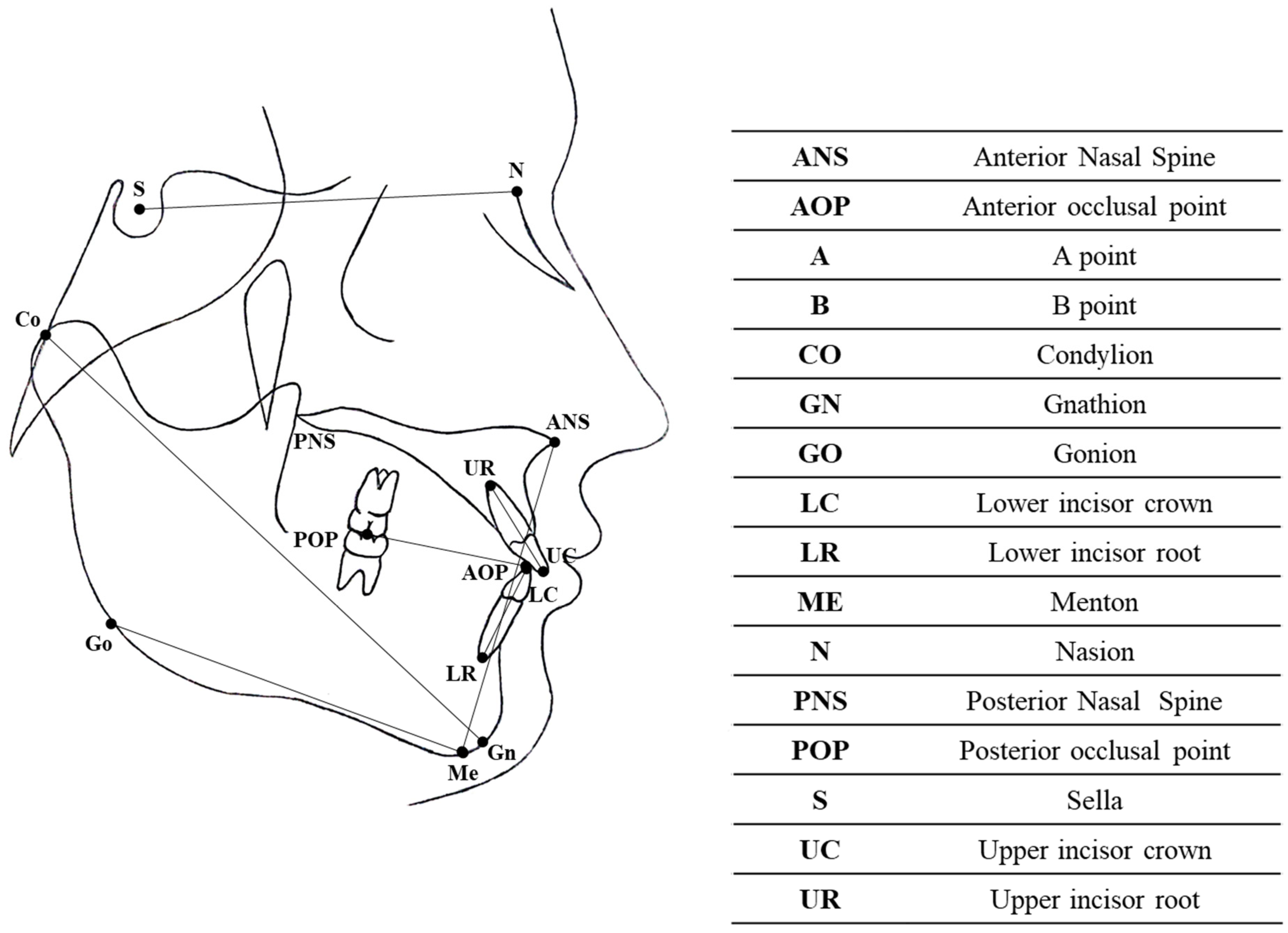
2.4. Cephalometric Analysis
2.5. Statistical Analysis
3. Results
- Patients treated with the RME II System showed a decreased lower incisor inclination, decreased occlusal plane inclination, a greater reduction in the ANB angle and LFH, and decreased mandibular length compared with patients treated with the Herbst appliance;
- Patients treated with the RME II System showed an increased mandibular length, reduced overjet and overbite, a smaller divergence angle and LFH, and a greater occlusal plane inclination compared with the control group;
- Patients treated with the Herbst appliance showed a greater occlusal plane inclination and SN-PP angle, increased lower incisor proclination, and a reduction in overjet, overbite, and upper incisor inclination compared with the control group.
4. Discussion
Limitations of the Study
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Angle, E.H. Classification of malocclusion. Dent. Cosmos 1899, 41, 350–357. [Google Scholar]
- dos Santos, R.R.; Nayme, J.G.; Garbin, A.J.; Saliba, N.; Garbin, C.A.; Moimaz, S.A. Prevalence of malocclusion and related oral habits in 5- to 6-year-old children. Oral. Health Prev. Dent. 2012, 10, 311–318. [Google Scholar] [PubMed]
- Aggarwal, P.; Kharbanda, O.P.; Mathur, R.; Duggal, R.; Parkash, H. Muscle response to the twin-block appliance: An electromyographic study of the masseter and anterior temporal muscles. Am. J. Orthod. Dentofac. Orthop. 1999, 116, 405–414. [Google Scholar] [CrossRef] [PubMed]
- Barton, S.; Cook, P.A. Predicting functional appliance treatment outcome in Class II malocclusions—A review. Am. J. Orthod. Dentofac. Orthop. 1997, 112, 282–286. [Google Scholar] [CrossRef] [PubMed]
- Baccetti, T.; Franchi, L.; McNamara, J.A., Jr. An improved version of the cervical vertebral maturation (CVM) method for the assessment of mandibular growth. Angle Orthod. 2002, 72, 316–323. [Google Scholar] [CrossRef] [PubMed]
- Perinetti, G.; Primozic, J.; Franchi, L.; Contardo, L. Treatment Effects of Removable Functional Appliances in Pre-Pubertal and Pubertal Class II Patients: A Systematic Review and Meta-Analysis of Controlled Studies. PLoS ONE 2015, 10, e0141198. [Google Scholar] [CrossRef] [PubMed]
- Arens, R.; Marcus, C.L. Pathophysiology of upper airway obstruction: A developmental perspective. Sleep 2004, 27, 997–1019. [Google Scholar] [CrossRef] [PubMed]
- Claudino, L.V.; Mattos, C.T.; Ruellas, A.C.; Sant’ Anna, E.F. Pharyngeal airway characterization in adolescents related to facial skeletal pattern: A preliminary study. Am. J. Orthod. Dentofac. Orthop. 2013, 143, 799–809. [Google Scholar] [CrossRef]
- Shete, C.S.; Bhad, W.A. Three-dimensional upper airway changes with mandibular advancement device in patients with obstructive sleep apnea. Am. J. Orthod. Dentofac. Orthop. 2017, 151, 941–948. [Google Scholar] [CrossRef]
- Xiang, M.; Hu, B.; Liu, Y.; Sun, J.; Song, J. Changes in airway dimensions following functional appliances in growing patients with skeletal class II malocclusion: A systematic review and meta-analysis. Int. J. Pediatr. Otorhinolaryngol. 2017, 97, 170–180. [Google Scholar] [CrossRef]
- Graber, T.M. The “three M’s”: Muscles, malformation, and malocclusion. Am. J. Orthod. 1963, 49, 418–450. [Google Scholar] [CrossRef]
- Riolo, M.L.; Brandt, D.; TenHave, T.R. Associations between occlusal characteristics and signs and symptoms of TMJ dysfunction in children and young adults. Am. J. Orthod. Dentofac. Orthop. 1987, 92, 467–477. [Google Scholar] [CrossRef] [PubMed]
- Seligman, D.A.; Pullinger, A.G. The role of functional occlusal relationships in temporomandibular disorders: A review. J. Craniomandib. Disord. 1991, 5, 265–279. [Google Scholar]
- Fichera, G.; Ronsivalle, V.; Santonocito, S.; Aboulazm, K.S.; Isola, G.; Leonardi, R.; Palazzo, G. Class II Skeletal Malocclusion and Prevalence of Temporomandibular Disorders. An Epidemiological Pilot Study on Growing Subjects. J. Funct. Morphol. Kinesiol. 2021, 6, 63. [Google Scholar] [CrossRef]
- Pancherz, H.; Anehus-Pancherz, M. The headgear effect of the Herbst appliance: A cephalometric long-term study. Am. J. Orthod. Dentofac. Orthop. 1993, 103, 510–520. [Google Scholar] [CrossRef] [PubMed]
- von Elm, E.; Altman, D.G.; Egger, M.; Pocock, S.J.; Gotzsche, P.C.; Vandenbroucke, J.P.; Initiative, S. The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) Statement: Guidelines for reporting observational studies. Int. J. Surg. 2014, 12, 1495–1499. [Google Scholar] [CrossRef]
- Cohen, J. Statistical Power Analysis. Curr. Dir. Psychol. Sci. 1992, 1, 98–101. [Google Scholar] [CrossRef]
- Houston, W.J. The analysis of errors in orthodontic measurements. Am. J. Orthod. 1983, 83, 382–390. [Google Scholar] [CrossRef] [PubMed]
- Dahlberg, G. Statistical Methods for Medical and Biological Students; G. Allen & Unwin Limited: Sydney, Australia, 1940. [Google Scholar]
- Pancherz, H. Treatment of class II malocclusions by jumping the bite with the Herbst appliance. A cephalometric investigation. Am. J. Orthod. 1979, 76, 423–442. [Google Scholar] [CrossRef]
- Pancherz, H. The Herbst appliance--its biologic effects and clinical use. Am. J. Orthod. 1985, 87, 1–20. [Google Scholar] [CrossRef]
- Konik, M.; Pancherz, H.; Hansen, K. The mechanism of Class II correction in late Herbst treatment. Am. J. Orthod. Dentofac. Orthop. 1997, 112, 87–91. [Google Scholar] [CrossRef] [PubMed]
- Franchi, L.; Baccetti, T.; McNamara, J.A., Jr. Treatment and posttreatment effects of acrylic splint Herbst appliance therapy. Am. J. Orthod. Dentofac. Orthop. 1999, 115, 429–438. [Google Scholar] [CrossRef]
- Bock, N.C.; von Bremen, J.; Ruf, S. Stability of Class II fixed functional appliance therapy--a systematic review and meta-analysis. Eur. J. Orthod. 2016, 38, 129–139. [Google Scholar] [CrossRef] [PubMed]
- Barnett, G.A.; Higgins, D.W.; Major, P.W.; Flores-Mir, C. Immediate skeletal and dentoalveolar effects of the crown- or banded type Herbst appliance on Class II division 1 malocclusion. Angle Orthod. 2008, 78, 361–369. [Google Scholar] [CrossRef] [PubMed]
- D’Anto, V.; Bucci, R.; Franchi, L.; Rongo, R.; Michelotti, A.; Martina, R. Class II functional orthopaedic treatment: A systematic review of systematic reviews. J. Oral. Rehabil. 2015, 42, 624–642. [Google Scholar] [CrossRef] [PubMed]
- Pancherz, H. Vertical dentofacial changes during Herbst appliance treatment. A cephalometric investigation. Swed. Dent. J. Suppl. 1982, 15, 189–196. [Google Scholar] [PubMed]
- Aiello, D.; Finamore, A.; Scribante, A.; Figliuzzi, M.M.; Paduano, S. The Use of TADs in the Mandibular Arch to Prevent Proclination of the Lower Incisors during the Use of the Mini Scope Herbst Appliance. Case Rep. Dent. 2022, 2022, 9144900. [Google Scholar] [CrossRef] [PubMed]
- Al-Dboush, R.; Soltan, R.; Rao, J.; El-Bialy, T. Skeletal and dental effects of Herbst appliance anchored with temporary anchorage devices: A systematic review with meta-analysis. Orthod. Craniofac. Res. 2022, 25, 31–48. [Google Scholar] [CrossRef] [PubMed]
- Manni, A.; Pasini, M.; Mauro, C. Comparison between Herbst appliances with or without miniscrew anchorage. Dent. Res. J. 2012, 9, S216–S221. [Google Scholar] [CrossRef]
- Sidhu, M.S.; Kharbanda, O.P.; Sidhu, S.S. Cephalometric analysis of changes produced by a modified Herbst appliance in the treatment of Class II division 1 malocclusion. Br. J. Orthod. 1995, 22, 1–12. [Google Scholar] [CrossRef]
- Flores-Mir, C.; Ayeh, A.; Goswani, A.; Charkhandeh, S. Skeletal and dental changes in Class II division 1 malocclusions treated with splint-type Herbst appliances. A systematic review. Angle Orthod. 2007, 77, 376–381. [Google Scholar] [CrossRef] [PubMed]
- Mutinelli, S.; Manfredi, M.; Guiducci, A.; Denotti, G.; Cozzani, M. Anchorage onto deciduous teeth: Effectiveness of early rapid maxillary expansion in increasing dental arch dimension and improving anterior crowding. Prog. Orthod. 2015, 16, 22. [Google Scholar] [CrossRef] [PubMed]
- Brunetto, M.; Andriani Jda, S.; Ribeiro, G.L.; Locks, A.; Correa, M.; Correa, L.R. Three-dimensional assessment of buccal alveolar bone after rapid and slow maxillary expansion: A clinical trial study. Am. J. Orthod. Dentofac. Orthop. 2013, 143, 633–644. [Google Scholar] [CrossRef] [PubMed]
- Perinetti, G.; Contardo, L. Reliability of Growth Indicators and Efficiency of Functional Treatment for Skeletal Class II Malocclusion: Current Evidence and Controversies. Biomed. Res. Int. 2017, 2017, 1367691. [Google Scholar] [CrossRef] [PubMed]
- Kirschneck, C.; Proff, P.; Lux, C. Ideal treatment timing of orthodontic anomalies-a German clinical S3 practice guideline. J. Orofac. Orthop. 2022, 83, 225–232. [Google Scholar] [CrossRef]
- Baratieri, C.; Alves, M., Jr.; Bolognese, A.M.; Nojima, M.C.; Nojima, L.I. Changes in skeletal and dental relationship in Class II Division I malocclusion after rapid maxillary expansion: A prospective study. Dental Press. J. Orthod. 2014, 19, 75–81. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
| Inclusion Criteria | Exclusion Criteria |
|---|---|
| Complete eruption of permanent incisors and first permanent molars | Mono- or bilateral crossbite |
| Age between 9 and 13 years | Patients with complete permanent teeth |
| Class II division 1 malocclusion | Early loss of second deciduous molars |
| Lateral cephalogram performed with the same cephalostat | Skeletal malformations and destructive caries |
| Skeletal age between CS2 and CS3 according to the cervical vertebral maturation method | Previous cervical trauma |
| Absence of temporomandibular joint disorders | Patients with previous orthodontic treatment |
| No maxillofacial or airway surgery |
| Measurement | Description |
|---|---|
| Skeletal measurements | |
| SN-MP | Angle between the sella–nasion (SN) line and the mandibular plane (MP) |
| SN-PO | Angle between the sella–nasion (SN) line and the occlusal plane (APO–PPO) |
| ANB | Angle between the N–A line and N–B line |
| AR-GO-ME | Gonial angle: the angle between the AR point and the mandibular plane (MP) |
| UPPER GONIAL ANGLE (AR-GO-N) | Angle between the N–AR line and the AR–GO line |
| LOWER GONIAL ANGLE (N-GO-ME) | Angle between the gonion–nasion (GO–N) line and the gonion–menton (GO–ME) line |
| SN-PP | Angle between the sella–nasion (SN) line and the maxillary plane (ANS–PNS) |
| LFH (lower face height) | Distance between the anterior nasal spine (ANS) and the menton (ME) |
| MANDIBULAR LENGTH (CO-GN) | Distance between the condylion and the gnathion |
| Dental measurements | |
| 1+SN | Angle between the upper incisor and the sella–nasion line |
| IMPA | Angle between the lower incisor and the mandibular plane (GO–ME) |
| OVERJET | Horizontal distance between the incisal border of the upper and lower incisors |
| OVERBITE | Vertical distance between the incisal border of the upper and lower incisors |
| Group R | Group H | Group C | |||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| T0 | T1 | P | T0 | T1 | P | T0 | T1 | P | |||||||
| Mean | Std Dev. | Mean | Std Dev. | Mean | Std Dev. | Mean | Std Dev. | Mean | Std Dev. | Mean | Std Dev. | ||||
| SN-PO | 19.90 | 4.21 | 19.26 | 4.63 | 0.18 | 14.36 | 4.43 | 17.32 | 8.01 | 0.264 | 15.98 | 3.24 | 12.07 | 4.02 | 0.001 |
| SN-MP | 35.21 | 4.70 | 32.67 | 4.81 | 0.001 | 34.03 | 3.30 | 32.81 | 5.79 | 0.041 | 34.61 | 3.76 | 33.76 | 3.95 | 0.05 |
| AR-GO-ME | 124.5 | 6.41 | 124.3 | 7.43 | 0.264 | 132.9 | 7.91 | 131.5 | 7.04 | 0.431 | 134.7 | 6.06 | 132.6 | 5.55 | 0.614 |
| AR-GO-N | 51.62 | 3.40 | 51.75 | 4.70 | 0.362 | 58.41 | 3.91 | 56.82 | 5.23 | 0.752 | 58.88 | 2.83 | 57.89 | 3.96 | 0.158 |
| N-GO-ME | 72.85 | 4.84 | 72.36 | 4.48 | 0.451 | 74.9 | 4.95 | 74.62 | 4.50 | 0.461 | 75.81 | 4.60 | 74.75 | 3.85 | 0.219 |
| SN-PP | 9.08 | 4.16 | 9.43 | 4.94 | 0.753 | 6.155 | 3.45 | 7.533 | 4.21 | 0.513 | 7.046 | 4.02 | 6.26 | 5.14 | 0.482 |
| LFH | 67.42 | 6.21 | 67.13 | 4.91 | 0.396 | 58.06 | 5.87 | 59.52 | 4.82 | 0.271 | 69.11 | 9.24 | 68 | 8.80 | 0.372 |
| CO-GN | 110.3 | 4.79 | 115.8 | 4.89 | 0.001 | 96.72 | 8.72 | 101.6 | 7.28 | 0.001 | 118.9 | 12.6 | 118.4 | 13.93 | 0.004 |
| 1+SN | 105.5 | 9.28 | 103.4 | 5.11 | 0.031 | 110 | 7.67 | 107.3 | 6.36 | 0.003 | 107 | 4.78 | 105.9 | 5.78 | 0.001 |
| IMPA | 95.07 | 6.67 | 94.74 | 6.89 | 0.863 | 94.79 | 3.95 | 100.9 | 3.42 | 0.004 | 90.85 | 6.43 | 91.18 | 7.18 | 0.354 |
| Overbite | 1.31 | 1.67 | 2.97 | 1.35 | 0.001 | 3.66 | 1.98 | 2.850 | 1.75 | 0.006 | 3.37 | 3.16 | 3.72 | 1.40 | 0.002 |
| Overjet | 6.89 | 1.96 | 4.34 | 1.24 | 0.001 | 7.66 | 1.90 | 4.09 | 1.05 | 0.02 | 6.31 | 2.55 | 2.7 | 2.51 | 0.005 |
| ANB | 5.61 | 1.43 | 2.39 | 0.85 | 0.002 | 6.22 | 1.72 | 4.51 | 1.47 | 0.001 | 7.61 | 2.50 | 6.60 | 2.09 | 0.05 |
| Sum of Squares | df | Mean Square | F | Sig. | ||
|---|---|---|---|---|---|---|
| SN-PO | Between groups | 612.614 | 2 | 306.307 | 21.694 | 0.001 * |
| Within groups | 1228.396 | 87 | 14.119 | |||
| Total | 1841.010 | 89 | ||||
| SN-MP | Between groups | 49.653 | 2 | 24.827 | 3.940 | 0.023 * |
| Within groups | 548.180 | 87 | 6.301 | |||
| Total | 597.833 | 89 | ||||
| AR-GO-ME | Between groups | 85.784 | 2 | 42.892 | 1.521 | 0.224 |
| Within groups | 2453.685 | 87 | 28.203 | |||
| Total | 2539.469 | 89 | ||||
| AR-GO-N | Between groups | 28.064 | 2 | 14.032 | 1.143 | 0.323 |
| Within groups | 1067.697 | 87 | 12.272 | |||
| Total | 1095.761 | 89 | ||||
| N-GO-ME | Between groups | 9.438 | 2 | 4.719 | 0.414 | 0.662 |
| Within groups | 990.522 | 87 | 11.385 | |||
| Total | 999.960 | 89 | ||||
| SN-PP | Between groups | 57.155 | 2 | 28.578 | 4.273 | 0.017 * |
| Within groups | 581.825 | 87 | 6.688 | |||
| Total | 638.980 | 89 | ||||
| LOWER FACE HEIGHT | Between groups | 487.326 | 2 | 243.663 | 18.481 | 0.001 * |
| Within groups | 1147.030 | 87 | 13.184 | |||
| Total | 1634.355 | 89 | ||||
| CO-GN | Between groups | 344.719 | 2 | 172.359 | 4.429 | 0.015 * |
| Within groups | 3386.049 | 87 | 38.920 | |||
| Total | 3730.767 | 89 | ||||
| 1+SN | Between groups | 257.450 | 2 | 128.725 | 3.431 | 0.037 * |
| Within groups | 3264.500 | 87 | 37.523 | |||
| Total | 3521.950 | 89 | ||||
| IMPA | Between groups | 743.330 | 2 | 371.665 | 21.883 | 0.001 * |
| Within groups | 1477.603 | 87 | 16.984 | |||
| Total | 2220.934 | 89 | ||||
| OVERBITE | Between groups | 71.946 | 2 | 35.973 | 6.850 | 0.002 * |
| Within groups | 456.915 | 87 | 5.252 | |||
| Total | 528.861 | 89 | ||||
| OVERJET | Between groups | 377.546 | 2 | 188.773 | 39.320 | 0.001 * |
| Within groups | 417.678 | 87 | 4.801 | |||
| Total | 795.224 | 89 | ||||
| ANB | Between groups | 72.458 | 2 | 36.229 | 21.511 | 0.001 * |
| Within groups | 146.526 | 87 | 1.684 | |||
| Total | 218.984 | 89 | ||||
| Dependent Variable | (I) GROUP | (J) GROUP | Mean Difference (I − J) | Std Error | Sig. | 95% Confidence Interval | |
|---|---|---|---|---|---|---|---|
| Lower Bound | Upper Bound | ||||||
| SN-PO | C | R | −2.77 * | 0.970 | 0.015 | −5.088 | −0.461 |
| C | H | −6.37 * | 0.970 | 0.000 | −8.686 | −4.059 | |
| R | H | −3.59 * | 0.970 | 0.001 | −5.911 | −1.284 | |
| SN-MP | C | R | 1.81 * | 0.648 | 0.017 | 0.269 | 3.360 |
| C | H | 0.79 | 0.648 | 0.438 | −0.747 | 2.343 | |
| R | H | −1.01 | 0.648 | 0.264 | −2.562 | 0.528 | |
| AR-GO-ME | C | R | −2.22 | 1.371 | 0.243 | −5.490 | 1.050 |
| C | H | −1.88 | 1.371 | 0.360 | −5.150 | 1.390 | |
| R | H | 0.34 | 1.371 | 0.967 | −2.930 | 3.610 | |
| AR-GO-N | C | R | −1.12 | 0.904 | 0.434 | −3.277 | 1.037 |
| C | H | 0.12 | 0.904 | 0.990 | −2.037 | 2.277 | |
| R | H | 1.24 | 0.904 | 0.361 | −0.917 | 3.397 | |
| N-GO-ME | C | R | −0.55 | 0.871 | 0.803 | −2.627 | 1.527 |
| C | H | −0.77 | 0.871 | 0.652 | −2.847 | 1.307 | |
| R | H | −0.22 | 0.871 | 0.965 | −2.297 | 1.857 | |
| SN-PP | C | R | −0.92 | 0.667 | 0.356 | −2.513 | 0.671 |
| C | H | −1.95 * | 0.667 | 0.012 | −3.543 | −0.358 | |
| R | H | −1.03 | 0.667 | 0.276 | −2.622 | 0.562 | |
| LOWER FACE HEIGHT | C | R | 5.46 * | 0.937 | 0.000 | 3.231 | 7.702 |
| C | H | 1.33 | 0.937 | 0.332 | −0.898 | 3.572 | |
| R | H | −4.13 * | 0.937 | 0.000 | −6.365 | −1.894 | |
| CO-GN | C | R | −2.33 * | 1.610 | 0.023 | 0.494 | 8.175 |
| C | H | 0.39 | 1.610 | 0.967 | −3.445 | 4.235 | |
| R | H | −3.94 * | 1.610 | 0.043 | −7.780 | −0.099 | |
| 1+SN | C | R | 3.25 | 1.581 | 0.105 | −0.521 | 7.021 |
| C | H | 3.85 * | 1.581 | 0.044 | 0.078 | 7.621 | |
| R | H | 0.60 | 1.581 | 0.924 | −3.171 | 4.371 | |
| IMPA | C | R | 0.66 | 1.064 | 0.809 | −1.876 | 3.198 |
| C | H | −5.73 * | 1.064 | 0.000 | −8.276 | −3.201 | |
| R | H | −6.40 * | 1.064 | 0.000 | −8.937 | −3.862 | |
| OVERBITE | C | R | 1.11 | 0.591 | 0.152 | −0.301 | 2.521 |
| C | H | 2.19 * | 0.591 | 0.001 | 0.779 | 3.601 | |
| R | H | 1.08 | 0.591 | 0.167 | −0.331 | 2.491 | |
| OVERJET | C | R | 3.59 * | 0.565 | 0.000 | 2.241 | 4.939 |
| C | H | 4.83 * | 0.565 | 0.000 | 3.481 | 6.179 | |
| R | H | 1.24 | 0.565 | 0.078 | −0.109 | 2.589 | |
| ANB | C | R | 2.15 * | 0.335 | 0.000 | 1.351 | 2.949 |
| C | H | 0.68 | 0.335 | 0.111 | −0.119 | 1.479 | |
| R | H | −1.47 * | 0.335 | 0.000 | −2.269 | −0.671 | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ciavarella, D.; Lorusso, M.; Fanelli, C.; Ferrara, D.; Esposito, R.; Laurenziello, M.; Esperouz, F.; Lo Russo, L.; Tepedino, M. The Efficacy of the RME II System Compared with a Herbst Appliance in the Treatment of Class II Skeletal Malocclusion in Growing Patients: A Retrospective Study. Dent. J. 2024, 12, 254. https://doi.org/10.3390/dj12080254
Ciavarella D, Lorusso M, Fanelli C, Ferrara D, Esposito R, Laurenziello M, Esperouz F, Lo Russo L, Tepedino M. The Efficacy of the RME II System Compared with a Herbst Appliance in the Treatment of Class II Skeletal Malocclusion in Growing Patients: A Retrospective Study. Dentistry Journal. 2024; 12(8):254. https://doi.org/10.3390/dj12080254
Chicago/Turabian StyleCiavarella, Domenico, Mauro Lorusso, Carlotta Fanelli, Donatella Ferrara, Rosa Esposito, Michele Laurenziello, Fariba Esperouz, Lucio Lo Russo, and Michele Tepedino. 2024. "The Efficacy of the RME II System Compared with a Herbst Appliance in the Treatment of Class II Skeletal Malocclusion in Growing Patients: A Retrospective Study" Dentistry Journal 12, no. 8: 254. https://doi.org/10.3390/dj12080254